
Abstract

Keywords
Case report
A 31-year-old man, a native of Bihar, India presented with an asymptomatic erythematous nodule on the left bulbar conjunctiva (Figure 1a) which was progressing gradually for the past ten months. He also complained of painless, progressive erythematous swelling and induration in the right hand (Figure 1b) for the same duration. The appearance of eye and hand lesions was preceded by a history of intermittent fever. There was a positive family history of Kala-azar in a sibling 10 years previously.
(a) Clinical photograph of the patient showing nodule on the conjunctiva of the left eye and (b) lesions of cutaneous leishmaniasis on the right hand; (c) histopathology slide with haematoxylin and eosin stain of the conjunctival biopsy showing Leishmania donovani (LD) bodies in 40 × magnification (indicated by arrow); (d) periodic acid Schiff (PAS) stain showing LD bodies in 40 × magnification (indicated by arrow).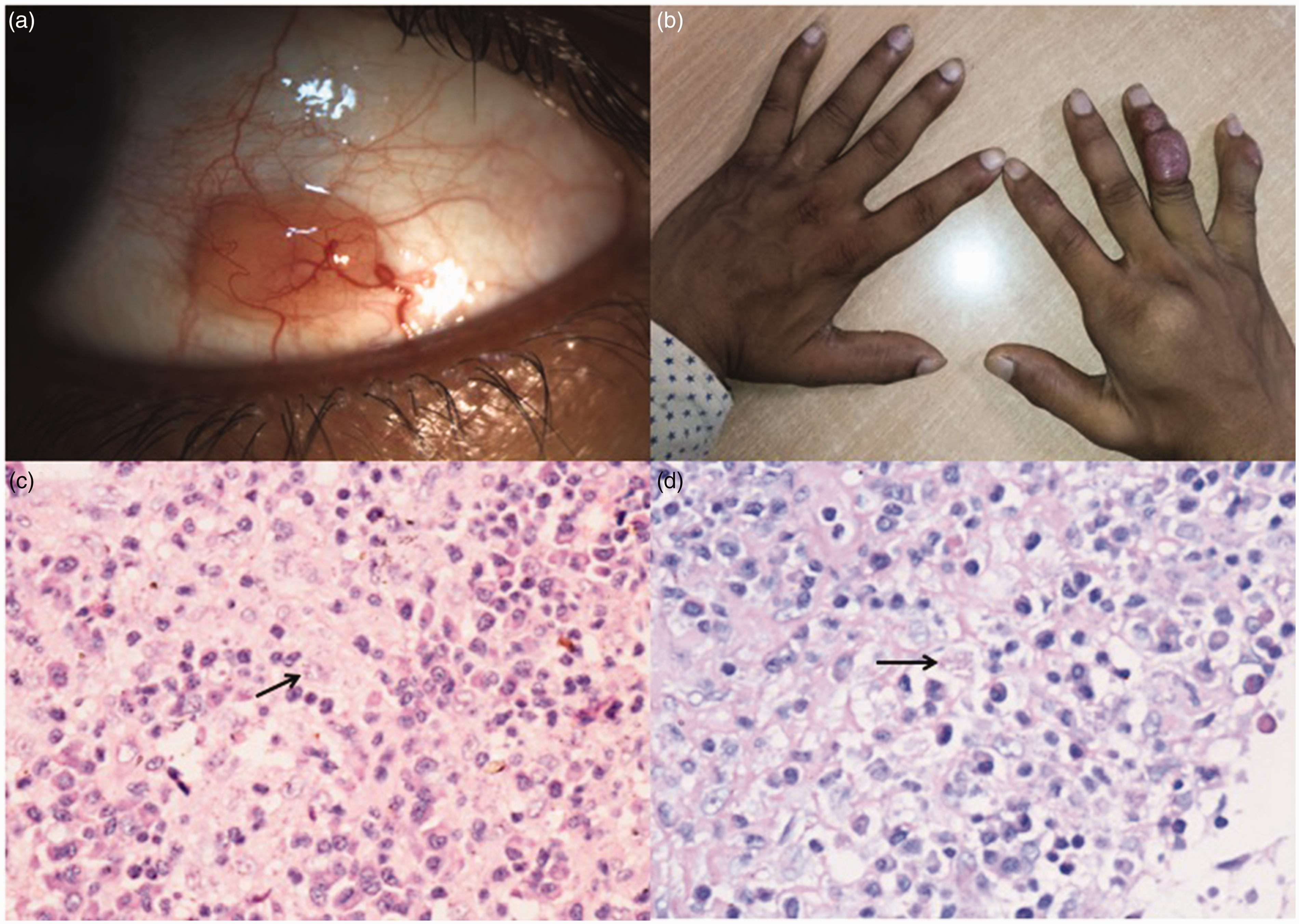
Visual acuity in both eyes was 20/20; the anterior segment, intra-ocular pressure and fundal examination were within normal limits. The temporal bulbar conjunctiva in the left eye showed an elevated, erythematous nodule measuring 6 × 3 mm, with a prominent feeder vessel, and surrounding mild conjunctival congestion. On general physical examination, there were ulcerated indurated nodules on the dorsal surface of the fingers of the right hand. There was no associated lymphadenopathy or hepato-splenomegaly.
A biopsy was obtained from the cutaneous lesions on his hands, revealing diffuse infiltration of the dermis by sheets of histiocytes containing amastigote forms of leishmania (LD bodies) which were highlighted by Giemsa stain, suggestive of cutaneous leishmaniasis.
A subsequent excision biopsy of the conjunctival lesion showed LD bodies (Figure 1c and 1d) in the histiocytic cells along with inflammatory lymphomononuclear cell infiltration, which confirmed the diagnosis of muco-cutaneous leishmaniasis.
The patient was started on systemic liposomal amphotericin B and a total cumulative dose of 21 mg/kg was given. At six-month follow up, the skin lesions were completely resolved and there was no recurrence of the conjunctival lesion.
Discussion
Leishmaniasis is endemic in over 60 countries worldwide and still poses a significant health burden in many middle and low-income countries. It is caused by the leishmania protozoa, which is transmitted by the bite of an infected female phlebotomine sandfly. There are three disease patterns identified: visceral; cutaneous; and mucocutaneous leishmaniasis. Mucocutaneous leishmaniasis is typically known to be endemic in South America. 1 Clinically, it begins as a small, well-demarcated papule at the inoculation site which enlarges into a nodule or plaque and eventually becomes ulcerated or verrucous. After cutaneous involvement, mucosal or mucocutaneous metastatic lesions may complicate the clinical picture, which may be due to lymphatic or hematogenous diffusion of the parasite. 2
Ocular leishmaniasis presents with several diagnostic and therapeutic challenges, owing to its uncommon nature and varied presentation. The eyelid is the most common site of ocular involvement. 3 Conjunctival lesions may occur as a contiguous dissemination from lid margin or in the setting of a disseminated leishmaniasis in an immune-compromised host. 4 To the best of our knowledge, only two other cases of independent conjunctival involvement have been reported, both of which were from Iran.4,5
Our case highlights the importance of a thorough history and examination in patients presenting with symptoms of leishmaniasis. It also emphasises the possibility of unusual local and systemic manifestations in non-endemic areas. A high degree of suspicion is essential for ruling out underlying infectious causes in cases with conjunctival lesions. Timely diagnosis and treatment can prevent permanent structural and functional impairment caused by damage to other ocular structures.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.