
Abstract
Acquired heart diseases (AHD) cause significant morbidity and mortality in children. There are limited studies on their burden in children. We conducted a retrospective study of 85 consecutive children diagnosed with AHD using clinical evaluation and echocardiography at Medical College, Kanpur, India to determine the aetiology and outcome of AHD in children. We found rheumatic heart disease (RHD) in one-third, cardiomyopathies or myocarditis combined in a further third and the remaining third were other causes, including pericardial diseases and metabolic or genetic disorders. These latter diseases were frequently misdiagnosed, causing significant morbidity and mortality. Hence, in children of all age groups presenting with unexplained shock, dyspnoea, hepatomegaly and ascites, cardiac status should be carefully and critically evaluated so that non-rheumatic AHD may not be missed.
Introduction
Apart from rheumatic heart disease (RHD), acquired heart diseases (AHD) in children include primary myocardial diseases such as dilated cardiomyopathy (DCM), restrictive and other cardiomyopathies, myocarditis, pericardial diseases, endocarditis, arrhythmias and rare disorders such as primary pulmonary hypertension (PH). Cardiac involvement is obviously a consequence of severe derangements including anaemia, hypertension, renal disease or thyroid disease, but is also seen in many other infections such as diphtheria, mumps, dengue and malaria, as well as generalised sepsis and tuberculosis, and also in several metabolic or genetic diseases including mucopolysaccharidoses, dermatomyositis, muscular dystrophies and lupus. 1
To date, RHD was considered the predominant cause of AHD in children in low- and middle-income countries2–4 and less attention was paid to other causes. With the advent of echocardiography, an increasing number of cases of AHD due to other causes are being recognised in children. 5 Limited studies on the burden of non-rheumatic AHD in children exist.6–10
Patients and methods
Our retrospective study was conducted at the Paediatric Department of GSVM Medical College Kanpur, India, between August 2016 and September 2018, with the objective of determining the clinical profile, aetiology and outcome of AHD in children. Approval for the study was obtained from the Institutional Ethics Committee (approval number 175/2018). All children aged 2 months to 16 years seen in the outpatient unit or admitted with a presumptive diagnosis of AHD were included in the study. Data on age, gender, symptoms, examination findings, investigations, diagnosis, disease course, treatment received and outcome were obtained from the case sheets and entered in a predesigned proforma. Children with cardiac symptoms directly due to anaemia and those who died before confirmation of the diagnosis by echocardiography were excluded from the study. Transthoracic echocardiography was performed on all patients using a GE Vivid-T8 echocardiography machine, which has the facility for giving two-dimensional (2D), M-mode and colour flow Doppler imaging. A single cardiologist performed the echocardiograms on all the patients.
Data were collected and analysed using SPSS version 20. Quantitative data were expressed as mean and standard deviations while categorical variables were expressed as frequencies and percentages.
Results
Types of acquired heart disease in children.

RCMP, restrictive cardiomyopathy; ARVD, arrhythmogenic right ventricular dysplasia; PSVT, paroxysmal supraventricular tachycardia; MPS, mucopolysaccharidoses.
Distribution of acquired heart disease cases by age and gender.

Outcome of different acquired heart diseases.
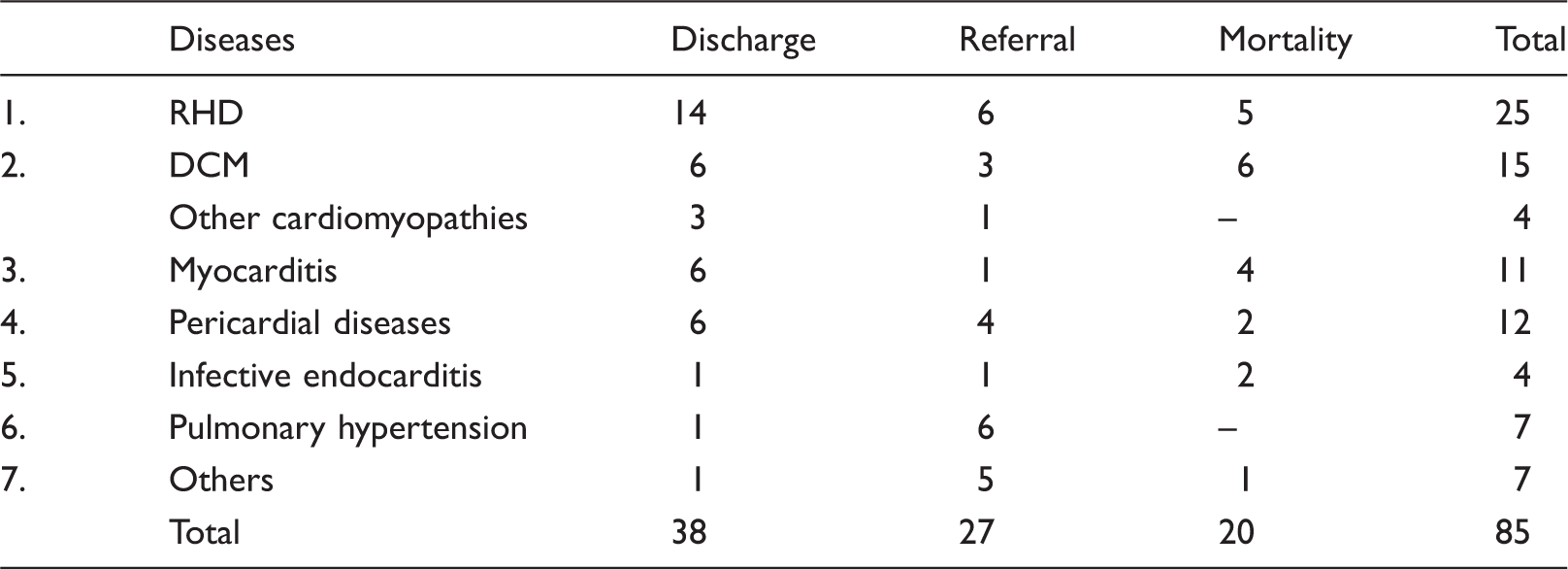
Infective endocarditis was associated with prolonged hospital stay and an overall mortality of 50%; one such case had acute Staphylococcus aureus endocarditis involving normal valves without any predisposing cardiac lesion with a fulminating course with CCF, arthritis, thyroiditis and embolic stroke.
One patient who presented with unexplained ascites and was previously misdiagnosed and treated as liver cirrhosis was found to have primary pulmonary hypertension (PH) on careful clinical examination and Doppler.
PH secondary to alveolar hypoxia was documented in a toddler with achondroplasia and obstructive sleep apnoea and a child with thalassemia intermedia.
Another patient who presented in cardiogenic shock was found to have narrow QRS tachycardia (SVT degenerating into atrial fibrillation) with a ventricular rate of 350/min. She was referred for cardioversion but died.
Metabolic causes (Hurler's and Hunter's) were identified in two patients and one patient, respectively, presenting with heart failure. They were earlier misdiagnosed as RHD.
Mitral valve prolapse was found in a child with dysmorphic facies, blue sclera and dyspnoea on exertion.
Discussion
Recent studies have also shown that the incidence of DCM and myocarditis is increasing.11,12 With wider availability and application of echocardiography, much greater accuracy of diagnosis is possible. Thus, a high index of suspicion is required in the diagnosis of AHDs other than RHD. Owing to non-specific symptoms, the assumption of RHD is no longer justified.
Conclusion
In our study of AHD in children, although the incidence of RHD was most common, a substantial proportion of cases of AHD other than RHD (namely cardiomyopathies, myocarditis, pericardial diseases, PH and metabolic/genetic disorders) were also encountered; the incidence of which was comparable to that of RHD. Due to the absence of significant cardiac murmurs, many of them often remain undiagnosed causing significant morbidity and high mortality. Hence, in children of all age groups presenting with unexplained shock, dyspnoea, hepatomegaly and ascites, cardiac status should be carefully and critically evaluated so that non-rheumatic AHD may not be missed nor be misdiagnosed as RHD.
Footnotes
Acknowledgements
The authors thank Neeraj Kumar Rao for his help in preparing the tables.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.