
Abstract
Musculoskeletal ultrasound (MSK-US) has been widely incorporated by clinical rheumatologists since its first description in inflammatory arthropathies in the late 1970s. Yet, the percentage of rheumatologists performing MSK-US remains low. Nevertheless, evidence shows it to be superior to clinical examination, comparable to MRI in many conditions, and far less expensive. Its convenience and ability to assess multiple joints make MSK-US particularly valuable in low-resource environments. Point-of-care US also reduces referrals and overall healthcare expenditure. In this narrative review, we aim to delineate current evidence of the role of MSK-US in the diagnosis and management of rheumatic diseases, with particular emphasis on its clinical utility, barriers to implementation, and potential strategies to overcome these challenges in resource-limited settings.
Introduction
Rheumatic and musculoskeletal disease (RMDs) encompass >100 degenerative, inflammatory, and autoimmune conditions. According to the 2010 World Health Organization (WHO) Global Burden of Disease Study, RMDs were reported as the second leading cause of disability worldwide, affecting >2 billion people worldwide, measured by years lived with such disability,1,2 disproportionately in resource-constrained settings.3,4
Early diagnosis and timely treatment are a window of opportunity in treatment and in particular of rheumatological conditions, leading to reduced treatment costs and disability rates. 5
The popularity of musculoskeletal ultrasound (MSK-US) is due to several advantages including its low cost, lack of radiation, bedside use and higher sensitivity than clinical examination. Accuracy in diagnostic and therapeutic procedures and numerous well validated studies have demonstrated its effectiveness in these domains. 6
Despite its advantages, the adoption of MSK-US by rheumatologists remains limited. Barriers such as cost, shortage of machines, insufficient training, time constraints, low revenue generation, lack of general awareness, and the perception of insufficient scientific evidence continue to hinder its widespread utilisation. 6
Our narrative review assesses the need to integrate clinical, practical, and contextual perspectives on MSK-US use in resource-limited settings. Medical databases were searched using keywords such as ‘musculoskeletal ultrasound’, ‘MSK ultrasound’, ‘crystal arthritis’, ‘CPPD’, ‘gout’, ‘chondrocalcinosis’, ‘rheumatic diseases’, and ‘low-resource settings’, alongside manual screening of multiple reference lists, as well as the authors’ own library.
Ultrasonography as an imaging modality was introduced in clinical medicine in the 1950s. However, the first publication detailing the ultrasonographic appearances of inflammatory arthritis emerged in the late 1970s.7,8
In 1990, significant advancement in the technology led to the development of high frequency superficial transducer with its ability to scan superficial structures. Beyond synovitis, it describes tenosynovitis, enthesitis, erosion, tophi, aggregates, double contour, intra-cartilaginous deposition. Numerous studies followed, demonstrating the diagnostic value of MSK-US in assessing spondylo-arthropathies, crystal diseases, osteoarthritis, and other rheumatic diseases.7,9
Since then, the popularity of MSK-US has steadily increased owing to its cost effectiveness, non-invasive nature, ability to provide real time information on inflammation in the synovium, tendon, and bones. At the bedside, therapeutic interventions such as joint injection and aspiration can be done with improved accuracy. Furthermore, MSK-US is more sensitive than clinical examination on detecting joint pathology. Widely validated studies have consistently shown the value of MSK-US an effective imaging modality in evaluating musculoskeletal disorders. 6
For example, the American College of Rheumatology and the European Alliance of Associations for Rheumatology (EULAR) 2023 classification criteria for calcium pyrophosphate crystal deposition (CPPD) disease incorporate MSK-US findings, which have sensitivity of 99.9% and specificity 92.5%. 10
CPPD crystal can be present in joint tissue much before it can be detected in synovial fluid analysis. Therefore, US imaging technique can identify precociously in hyaline cartilage (Fig. 1(a)) and fibrocartilage (Fig. 1(b)). 11 The double-contour sign (Fig. 2(a) and (b)) or tophi is diagnostic, and synovial fluid analysis is not needed to confirm the diagnosis. 12
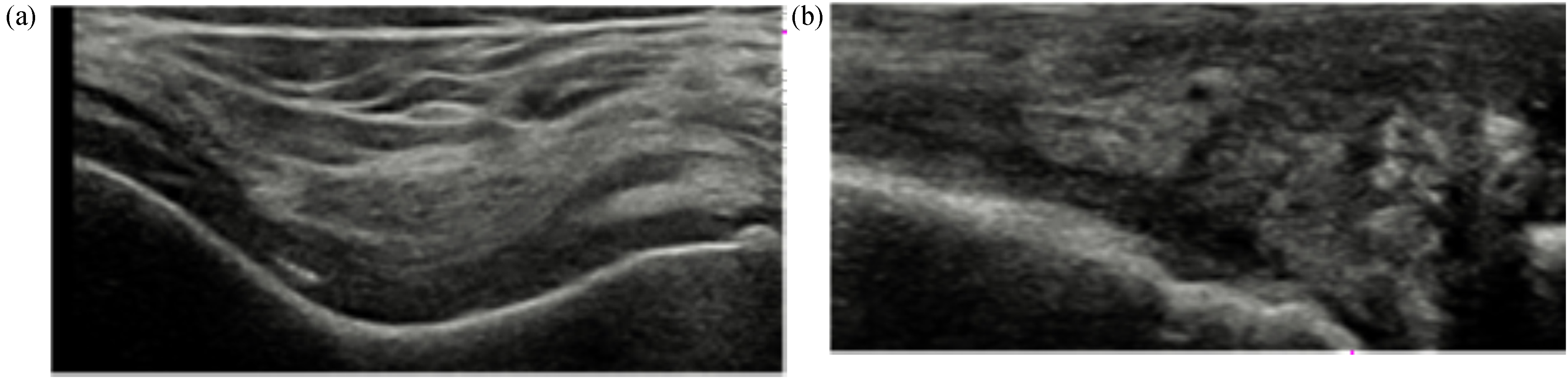
(a) Knee joint transverse scan showing hyperechoic deposits within hyaline cartilage (b) longitudinal scan of medial compartment showing hyperechoic deposits in medial compartment.
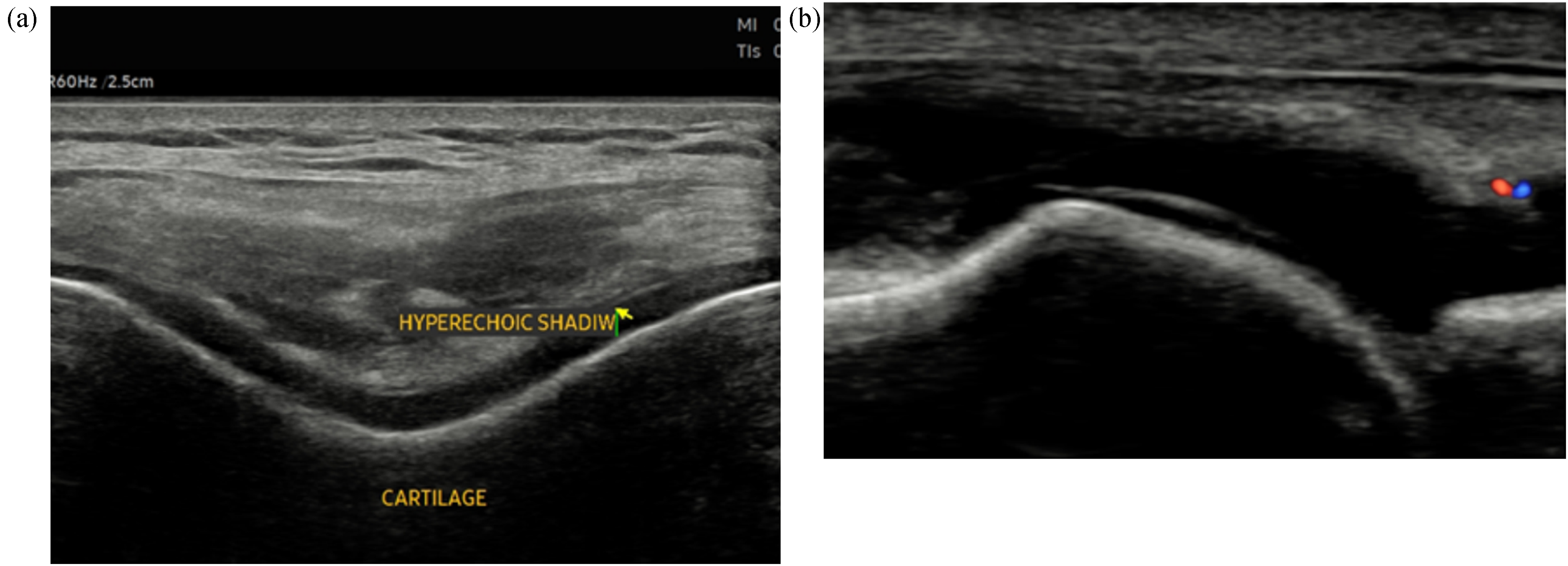
(a) Hyperechoic band over the superficial margin of the femoral hyaline cartilage. (b) Double contour sign in first metatarsophalangeal joint.
In 2012, provisional criteria for polymyalgia rheumatica showed adding MSK-US findings such as US evidence increased the sensitivity of subdeltoid bursitis, bicipital tenosynovitis, glenohumeral synovitis, hip synovitis and trochanteric bursitis classification to 66% and specificity to 81%. 13
Imaging in large vessel vasculitis advocates US of temporal and axillary arteries as the first imaging modality if giant cell arteritis is suspected, with 96% specificity. 14
Discussion
Despite its demonstrated usefulness, MSK-US training varies widely. Only in one country, Germany, had >80% rheumatologists receiving MSK-US training whereas in others it ranged from 10% to 50%.15,16 In Canada, 93% of rheumatologists reported relying on radiologists for US scans.17,18 Significant variation is seen between China where 17% of rheumatologists use MSK-US, Japan 27%, and South Korea 61%.19–21
Challenges are particularly pronounced in low-resource settings, where healthcare systems face additional structural and logistical limitations, viz. (1) financial pressure, (2) suboptimal healthcare service delivery, (3) underdeveloped infrastructure, (4) paucity of knowledge, (5) research challenges and considerations, (6) restricted social resources, (7) geographical and environmental factors, (8) human resource limitations and (9) the influence of beliefs and practices.5,22
Thus, barriers to MSK-US use include:
insufficient supporting evidence for its use, refuted above; lack of available ultrasound equipment but the impact of routine use of MSK-US demonstrated cost-effectiveness, as it facilitated the direct discharge of patients and significantly reduced both the number and cost of radiological referral.23,24 Specifically, the accessibility and portability of US machines allows for assessments to be performed directly in the clinic, thus avoiding delays typically associated with hospital MRI wait times. Furthermore, MSK-US is often preferable to MRI, particularly when cost limitations and in some cases, the former offers diagnostic accuracy superior to the latter; inadequate training opportunities for practitioners.25,26 MSK-US relies on the intrinsic real-time nature of ultrasound image acquisition and is highly operator dependent. Therefore, skilled training is essential. This can be achieved by mentorship, structured theoretical and practical courses, formal or informal training by experienced rheumatologists and radiologists, e-learning platforms, and self-directed learning. National societies, universities, and professional organisations globally provide MSK-US courses and workshops, such as the EULAR Committee on Education and Training facilitates a structured framework with introductory, intermediate, and advanced MSK-US courses.
27
The Bangladesh Rheumatology Society has been organising MSK-US workshops since 2019, contributing significantly to local skill development. Point-of-care ultrasound, developed by EULAR, PANLAR, and APLAR is gaining prominence in clinical practice.
27
To ensure widespread adoption and proficiency in MSK-US, it is essential to integrate continuous training programmes at both national and international levels and anchor imaging modules within rheumatology training curricula.
13
Limited time to conduct ultrasound examinations.12,17,28 This is the most frequently reported constraint, but MSK-US can be performed within 20–30 min, which aligns with the time scheduled for new patient assessments. MSK-US reduces the need for referrals to radiology departments, saving time and resources, enables early and accurate diagnoses, streamlining patient management, and improves overall patient care by integrating imaging into the rheumatology department workflow. MSK-US, when incorporated into clinical practice, complements the clinical history and physical examination, enhancing diagnostic accuracy. Thus, MSK-US serves as an essential tool, particularly in regions with limited access to specialised care. A preference to refer patients to radiologists for ultrasound evaluations. However, the practices of radiologists and rheumatologists differ significantly in the context of MSK-US, as the former focus primarily on the diagnosis of structural pathology. Their role is often limited to diagnosis, without direct involvement in patient management or treatment. MSK-US in rheumatology, however, is not only used for diagnosis but also in therapy, viz. ultrasound-guided injections, where US significantly improves precision and efficacy. Furthermore, by incorporating MSK-US into their practice, rheumatologists reduce the need for radiologist referrals for routine evaluations and procedures. This shift not only optimises resource utilisation but also provides several benefits: (i) On-the-spot imaging accelerates the diagnostic process, (ii) Combining clinical evaluation with imaging ensures a more comprehensive and logical approach to diagnosis and treatment, (iii) A reduced patient burden minimises delays and logistical challenges associated with external referrals to radiologists.
29
A conception that practice without MSK-US is adequate. However, evidence suggests otherwise. US has been proven to be more sensitive than clinical examination, viz. the detection of subclinical synovitis in 26% of clinically non-swollen joints.
30
Additionally, MSK-US contributes significantly to the differential diagnosis of inflammatory arthritis. In psoriatic arthritis, for example, extracapsular inflammation, such as peritendinous oedema, flexor tendonitis, and enthesitis, are more commonly observed. In rheumatoid arthritis (RA), the distribution and size of bone erosions, particularly in specific joints (e.g. second and fifth metacarpo-phalangeal joints, distal ulna, and fifth metatarso-phalangeal joint, are predictive. Synovial and entheseal inflammation patterns also help differentiate between types of arthritis.
31
Further, in patients with early undifferentiated arthritis, the presence of positive US findings increases the probability of developing persistent arthritis from 30% to 94%. This provides a crucial window of opportunity for initiating early treatment. Furthermore, MSK-US detection of synovitis serves as a strong predictor of inflammatory arthritis. An impression of reduced revenue, primarily due to lower reimbursement rates and the increased physician time required to perform and interpret ultrasound images.
24
A suspicion that US is inferior to MRI. Growing evidence, however, suggests that the former offers diagnostic accuracy comparable to the latter, or even superior as in rotator cuff injuries where it offers a dynamic, real-time examination well-tolerated by patients. Furthermore, MSK-US can be easily repeated in follow-up for example of both full- and partial-thickness rotator cuff tears.
32
Additionally, MSK-US is associated with high patient satisfaction, owing to its affordability, convenience, and ease of performance.
Additionally, MSK-US contributes significantly to the differential diagnosis of inflammatory arthritis. For example:
Psoriatic arthritis (PsA): Extracapsular inflammation, such as peritendinous oedema, flexor tendonitis, and enthesitis, are more commonly observed in PsA patients. RA: The distribution and size of bone erosions, particularly in specific joints (e.g. second and fifth MCP joints, distal ulna, and fifth MTP joint), are predictive of RA. Synovial and entheseal inflammation patterns also help differentiate RA from PsA.
31
For patients with early undifferentiated arthritis, the presence of positive US findings significantly increases the probability of developing persistent arthritis, from 30% to 94%. This provides a crucial window of opportunity for initiating early treatment. Furthermore, in patients presenting with symptoms like arthralgia, fatigue, and positive autoantibodies but without clinical synovitis, MSK-US detection of synovitis serves as a strong predictor of inflammatory arthritis.32,33
Incorporating MSK-US into their practice, rheumatologists reduce the need for radiologist referrals for routine evaluations and procedures. This shift not only optimises resource utilisation but also provides several benefits. 34
Conclusion
MSK-US plays a vital role in clinical practice across diverse settings and is increasingly applicable in low-resource environments. While there is a significant lack of training programmes, adequate training can equip clinicians with the knowledge and skills required to perform MSK-US effectively. This, in turn, enhances education, improves diagnostic accuracy, and elevates patient care.
The integration of MSK-US into routine rheumatology clinics has shown considerable value in the diagnosis and management of various rheumatological disorders. Additionally, MSK-US offers several advantages: it is faster, more cost-effective, and particularly suitable for use in low-resource settings, making it an indispensable tool for modern rheumatology practice.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.