
Abstract
Related neurological adverse effects to metronidazole are rarely encountered in clinical practice despite its wide use as an antibacterial or antiparasitic agent. The neurotoxicity is not dose-dependent and is fully reversible with discontinuation of the drug. We describe a young man who was receiving metronidazole for an amoebic liver abscess and developed encephalopathy and seizures. Brain magnetic resonance imaging showed characteristic bilateral symmetrical cerebellar dentate hyperintensities.
Keywords
Case report
A 20-year-old man was admitted as an emergency with a history of altered mental status with seizures over three days. He had been receiving metronidazole treatment for an amoebic liver abscess for 13 days (total cumulative dose 19.5 G). He did not consume alcohol or illicit drugs. On examination, he was drowsy and disoriented, but did not have neck rigidity nor cranial nerve deficits. Laboratory investigations revealed normal serum electrolytes, blood glucose levels, renal functions, liver chemistry, complete blood counts and coagulation profile. The cerebrospinal fluid (CSF) examination was also normal. Cerebral MRI revealed T2-weighted fluid-attenuated inversion recovery (FLAIR) signal hyperintensity in the bilateral cerebellar dentate nuclei, suggestive of drug toxicity (Figure 1). Metronidazole was discontinued and he gradually regained sensorium with conservative treatment.
Axial T2-FLAIR MRI showing symmetric hyperintensities within the dentate nuclei of the cerebellum.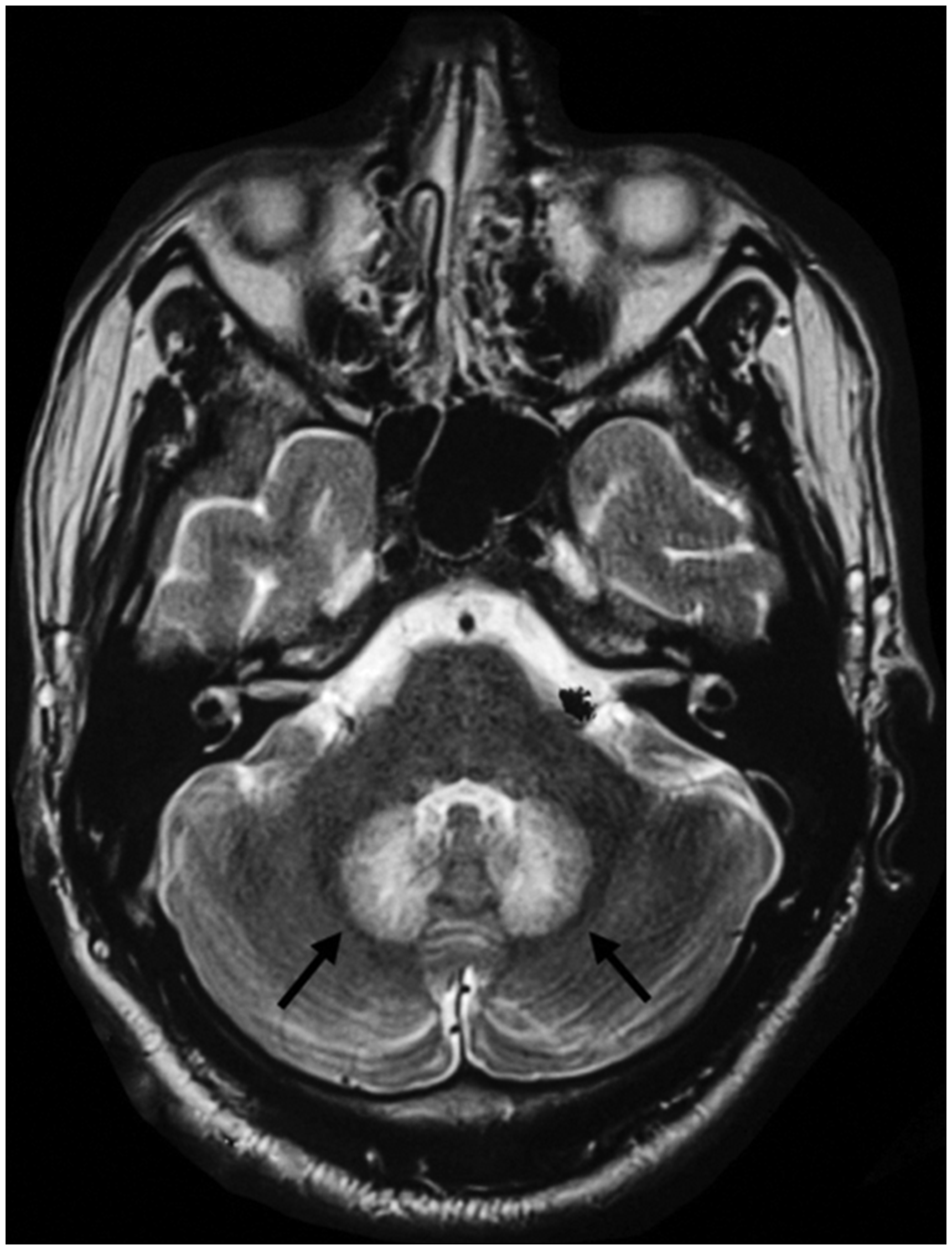
Discussion
Metronidazole is a frequently prescribed antimicrobial agent given its broad-spectrum activity, low cost and low incidence of severe adverse effects. Neurological complications such as cerebellar syndrome, encephalopathy, seizures and neuropathy (peripheral, optic or autonomic) may occur rarely and are not dependent on the dose or duration of treatment. 1 Cerebral MRI of patients with central nervous system toxicity characteristically shows symmetric hyperintensities within the dentate nuclei of the cerebellum on T2-FLAIR without post-contrast enhancement or mass effect. Less commonly, affected areas are the corpus callosum or brain stem.1–3 The proposed mechanism of neurotoxicity is thought to be due to inhibition of neuronal protein synthesis and axonal swelling by metronidazole and its metabolites. The diagnosis is based on history of exposure, clinical features and MRI findings. Serum or CSF concentrations are not routinely available and usually do not aid in diagnosis or management.2,4 CSF analysis is typically normal.3,5 The neurological toxicity is fully reversible after drug discontinuation.1–6 For drug-induced seizures, the first-line therapy is a benzodiazepine and, if required, a barbiturate. 7
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.