
Abstract
Transverse myelitis typically extends two or less spinal segments, whereas longitudinal extensive transverse myelitis (LETM) extends three or more spinal segments in length and may occasionally span all the segments of the spinal cord. We present a case of spinal tuberculosis presenting with LETM with true lower motor neuron-type flaccid paraplegia.
Keywords
Introduction
Central nervous system tuberculosis (TB) accounts for approximately 1% of all cases of TB, with half of these involving the spine. 1 Various presentations of spinal TB have been described in the literature, but intramedullary involvement is very rare. 2 Transverse myelitis extending three or more vertebral segments in length is found mostly in neuromyelitis optica (NMO);3,4 however, we report a case of tubercular longitudinally extensive transverse myelitis (LETM). Lower motor weakness, in transverse myelitis, is usually attributed to spinal shock, but the possibility of damage to the anterior horn cells should be kept in mind, particularly if three or more segment myelitis.
Case report
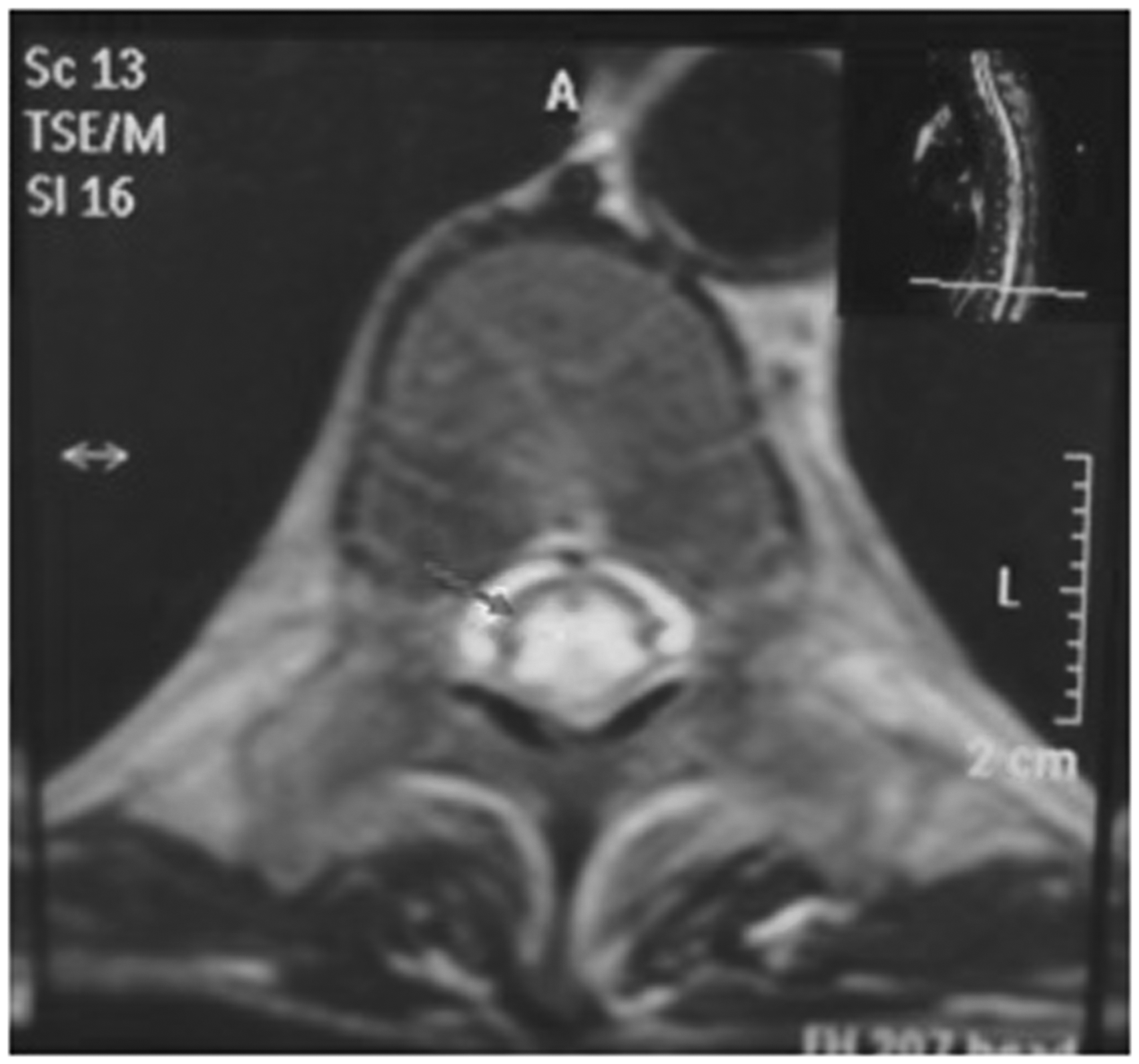
A 35-year-old male patient presented with altered sensorium and tonic-clonic seizures. He had a history of three months of fever and was diagnosed with pulmonary TB but had stopped anti-tubercular treatment (ATT). Routine investigations were normal. A cerebral computed tomography (CT) scan showed dilated third and bilateral lateral ventricles suggestive of communicating hydrocephalus. Cerebrospinal fluid (CSF) revealed the following: protein = 3 g/L; sugar = 5.77 mmol/L; total leucocyte count = 3.17 × 108/L with lymphocytic predominance (90%); and adenosine deaminase level = 93 IU/L (N < 10 IU/L). He was diagnosed as having tubercular meningitis and started on Category II ATT with steroids. After a fortnight, he developed weakness in both lower limbs, which rapidly deteriorated to complete paralysis in only five days. We found decreased tone and loss of all deep tendon reflexes in the lower limbs. Plantar reflexes were indifferent. Spinal shock was assumed to explain this development. The fever subsequently subsided but his lower limb weakness persisted even after seven months. Magnetic resonance scanning of the dorso-lumbar cord revealed a long segment central T2 hyperintensity in the spinal cord extending from T5 to the superior border of L1 with epidural enhancement suggestive of myelitis of infective aetiology likely to be tubercular origin (Figures 1 and 2).
Long segment central T2 hyperintensity in the spinal cord, extending from D5 vertebral level to the superior border of L1 vertebral body. Central T2 hyperintensity in the dorsolumbar spinal cord with post-contrast epidural enhancement suggestive of infective myelitis.
Discussion
The most common central nervous system manifestations of TB are tuberculous meningitis (95%), followed by cerebral tuberculoma and tuberculous abscess. Our patient had evidence of involvement of the lungs, leptomeninges and spinal cord. The latter was in the form of acute myelitis. M. tuberculosis is a very rare cause of this. An abnormal activation of the immune system against the spinal cord is thought to be the main aetiologic mechanism. 5 In a true lower motor neuron disorder due to involvement of anterior horn cells, the flaccidity persists for several weeks. 4 Here there is continuous inflammation of the cord from the conus medullaris to transverse sensory-motor level. 6
Our patient did not have any evidence of autoimmune disease; neither did he satisfy the clinical criteria for NMO. In fact, the term ‘spinal shock’ in this type of myelitis remains a misnomer as there is actually a true extensive involvement of lower motor neurons within the spinal cord. 6 Contrary to common belief, some patients with the para-infectious type of ascending myelitis who develop flaccid paralysis never develop upper motor neurone signs during the course of their illness, which carries a bad prognosis.
Sahu et al. 7 published four cases and Jain et al. 8 published one case in a patient with a cranial tuberculoma, who was already taking ATT therapy. In both papers, steroids ensured good motor recovery.
Our case is unusual on two accounts: first, the aetiology was tubercular; and second, the lung and leptomeningeal lesions showed near-complete recovery whereas the spinal cord lesion was severe and showed no recovery owing to damage to the anterior horn cells.
This case emphasises that TB must be kept in mind in cases of LETM and lower motor neuron paraplegia may not be due to spinal shock but due to damage to the anterior horn cells, especially in long spinal cord lesions. Such cases need to be studied to determine whether administering steroids with ATT improves the prognosis.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.