
Abstract
Haemolacria is a rare condition that usually occurs secondary to a hidden pathology. On rare occasions when no underlying cause may be found, it is called essential idiopathic haemolacria. Here the authors report a case of a 13-year-old girl presented to the ophthalmology emergency department with spontaneous bloody tears from both eyes for the past six months. There was associated bleeding from the ear. The rest of the systemic and ophthalmology examinations were within normal limits. She was investigated systemically to look for any underlying pathology; however, her blood investigations, radiological imaging and local examinations performed by the Otorhinolaryngology, Ophthalmology, Gynaecology and Internal Medicine departments were all normal. A final diagnosis of bilateral essential haemolacria was made.
Case report
A 13-year-old girl presented to the ophthalmology emergency department with complaints of recurrent episodes of spontaneous bleeding from her eyes and ears (Figures 1 and 2). She stated that these bouts lasted for 4–5 min and had been occurring for the past two years. She had no history of trauma or any other systemic illness. The episodes of bleeding from the eyes were not associated with her menstrual cycles.
Clinical picture of the patient showing bilateral haemolacria at presentation. Clinical picture of the patient showing blood coming from her ears.

On general examination, she was alert with stable vitals. There was no obvious evidence of pallor or icterus. On ophthalmological examination, her best corrected visual acuity was 6/6 in both eyes. Intraocular pressures were within normal limits. A slit lamp examination revealed normal anterior segment with healthy conjunctiva. Her lacrimal drainage system was also evaluated and appeared to be fine. Ocular movements were full and free in both eyes. Indirect ophthalmoscopy revealed normal posterior segment.
In view of blood coming out of her ears, an otorhinolaryngology consultation was carried out where she underwent a thorough rhinoscopy, endoscopic and otoscopic examination. A mild right-sided deviation of the nasal septum was noted. Otoscopy revealed a normal auditory canal, a pinkish gray, translucent, neutrally positioned patent tympanic membrane, which was mobile with an air inflation, consistent with a normal examination of ears. The rest of the findings were unremarkable.
In order to determine the cause, a battery of laboratory investigations were conducted which included a complete haemogram, bleeding time, clotting time, prothrombin time, activated partial thromboplastin time and thyroid function test, the results of which were normal. Smear from the bloody discharge was found to have only red blood cells with no other abnormal cells. A computed tomography scan of the head and orbit also ruled out paranasal sinus-related pathologies. Psychiatric and gynaecological examinations also came back normal.
After eventually ruling out all the possible causes, the patient was diagnosed with a case of essential idiopathic bilateral haemolacria. The patient and her family members were counselled and reassured about the condition and she was advised for a regular follow-up in the ophthalmology and otorhinolaryngology departments.
Discussion
‘Tears of blood’ from the weeping statues of the Virgin Mary has been a topic of interest, debate and multiple discussions in the recent past in Europe and North and South America; however, observing bloody tears, or haemolacria, in the daily practice of a clinician is an exceedingly rare situation. It is an inexplicable and distressing entity to the patient and the patient’s family members. The cause of haemolacria can usually be established by an extensive and thorough history taking combined with a systemic, haematological and radiological evaluation. It is called ‘idiopathic’ when no reason can be found. Evidence suggest that most idiopathic cases are benign and resolve spontaneously without any recurrence.1–5
The first mention of bloody tears dates back to old narrative writings and the first referral to blood from the eyes and ears was given by Brassavola in the 16th century, wherein he described a nun who instead of menstruating, had bloody tears and bloody ears. 1 Weise et al. 6 described a woman who bled from her eyes and ears after trying to stop her epistaxis by pinching her nose. The bloody tears were due to a retrograde flow through the nasolacrimal system and the bloody ears were due to retrograde travel of blood via auditory tube through the longstanding perforated tympanic membranes. In our case, the bleeding was irregular, intermittent and was not related to the patient’s menstrual cycle and her otorhinolaryngological examination was within normal limits.
There are reports of patients with haemolacria caused by hidden subtarsal telangiectasia in a case of hereditary haemorrhagic telangiectasia. 7 Other reported causes include conjunctivitis, capillary haemangioma, nasal and paranasal sinus tumours, lacrimal sac tumours, trauma or its infections, and retrograde epistaxis. 2 Our patient had no vascular pathologies on ophthalmic examination. Her nasolacrimal passage was fine and no pathology was found on radiological imaging.
Haemolacria after a scleral buckle infection and after a Lefort 1 surgery has also been reported.8,9 However, our patient did not have any history of surgery in the past.
Haemolacria is also attributed to conditions such as intensive anti-coagulative therapy, hyperthyroidism, uncontrolled hypertension and vicarious menstruation. 2 It has also been seen as a symptom of hysteria and other psychological illnesses. 2 Pharmacological procedures such as the Mecholyl test and drugs such as acetylcholine and silver nitrate are also known to cause this condition. 10
The cases of bilateral idiopathic haemolacria reported in the past 15 years.
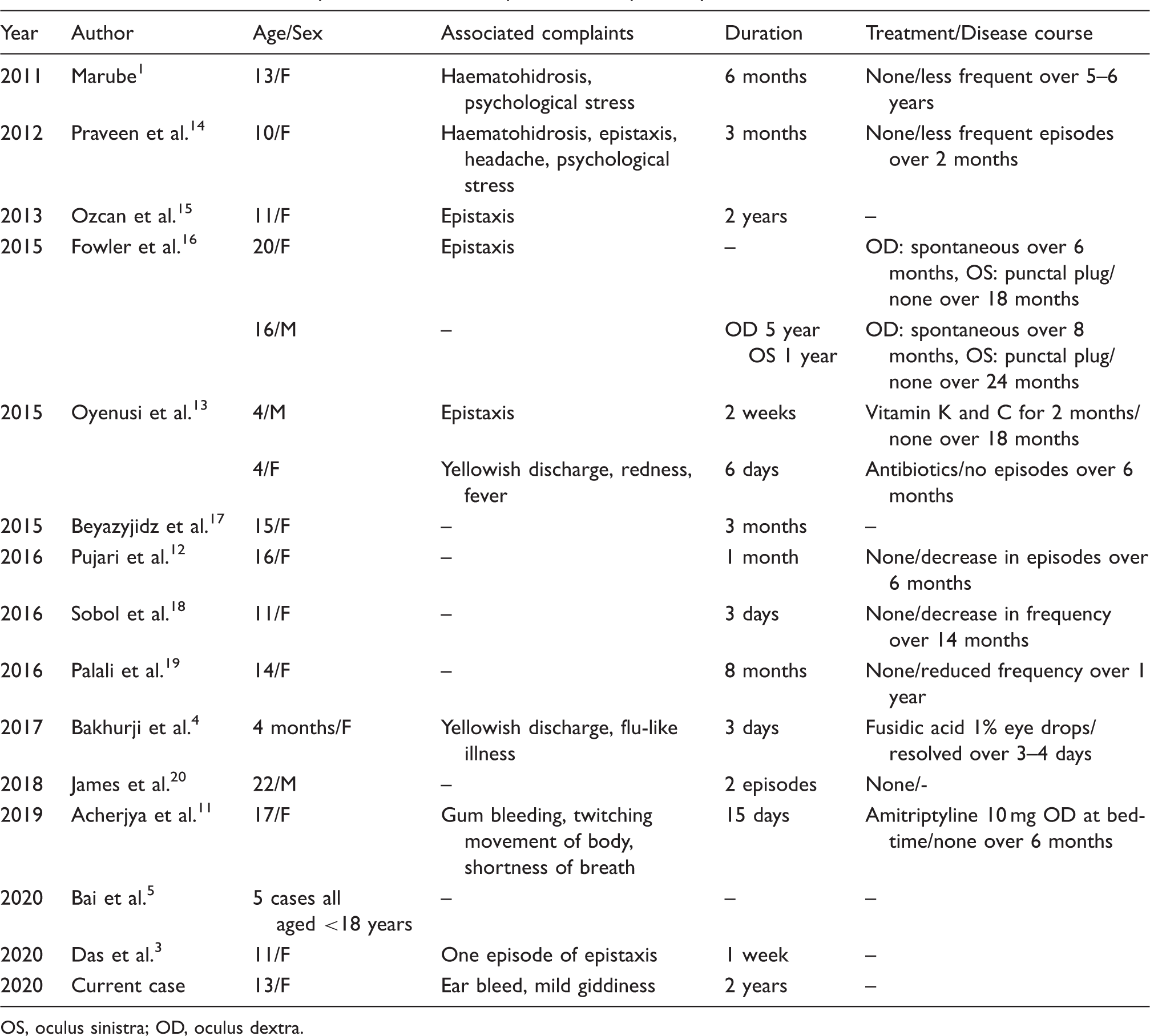
OS, oculus sinistra; OD, oculus dextra.
Although multiple management options in the form of high doses of vitamin C, intramuscular injection of vitamin K, oral amitriptyline and topical antibiotics have been tried in previous years, there is still no definite management protocol for essential idiopathic hemolacria.4,11,13 In most of the cases of idiopathic haemolacria, regular follow-up of the patient and psychological support for the patient and family members are all needed.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Permissions and Consent
A written informed consent has been obtained from the parents of the patient for publication of her photographs in journals for academic purposes. The consent is with the corresponding author and can be produced whenever asked for.