
Abstract
Nasal hirudiniasis is uncommon in humans, where a leech invades through the nostrils, adhering to the nasal cavity mucosa. It is rare in urban areas, noted in endemic rural areas, but scarcely documented and, with urbanisation and ecological imbalance has become rarer still. It presents with recurrent epistaxis due to hirudin released by the leech while other symptoms are infinitesimal owing to an analgesic enzyme secreted. A thorough history-taking and examination is of utmost importance as respiratory complications may arise if the leech invades the airways. We present a case series of five patients, within a period of three years.
Keywords
Introduction
Nasal bleeding is a common complaint, most times not life-threatening, and if unilateral, its usually due to digital trauma or impacted foreign bodies in the nasal cavity, either animate or inanimate.
Nasal leech infestation rarely presents as the leech is easily visible and sneezing reflexes expel the organisms. Leeches may pass into the nasopharynx, trachea and bronchi causing signs of airway obstruction with dyspnea, suffocation, and occasionally haemoptysis. 1 Occasionally, persistent nasal bleeding can result, the control of which may be challenging. 2
Leeches dwell in fresh waters, marine, wet lands or terrestrial surroundings. They survive by segmented parasitic feeding. They are more common in agricultural areas, 2 particularly the Himalayan belt of South Asia.3–5
Nasal hirudiniasis is painless and, owing to the leech being often concealed, 6 is frequently overlooked by clinicians; thus a thorough examination is of utmost importance. Nasal leeches can be easily removed by Tilley's forceps; monitoring for bleeding is important as anaemia is a sequela of prolonged nasal leech infestation. 7
Materials and methods
Five patients with recurrent epistaxis of short duration presented to the ENT Department over a three-year period, 2019–2022, in a tertiary care hospital of Sikkim, India. They had infestation by leeches diagnosed by anterior rhinoscopy and nasal endoscopy using a 0-degree 4mm rigid endoscope. Extraction of the leech or leeches was done using blunt forceps by holding the leech mid-body and pulling at it gently, so as not to crush and rupture it (Figure 1). Repeat endoscopy was carried to check for bleeding or further infestation. Local anaesthesia and nasal packing were not used, for fear of pushing a leech into the nasopharynx. All patients were monitored for ten minutes each before being allowed to leave.
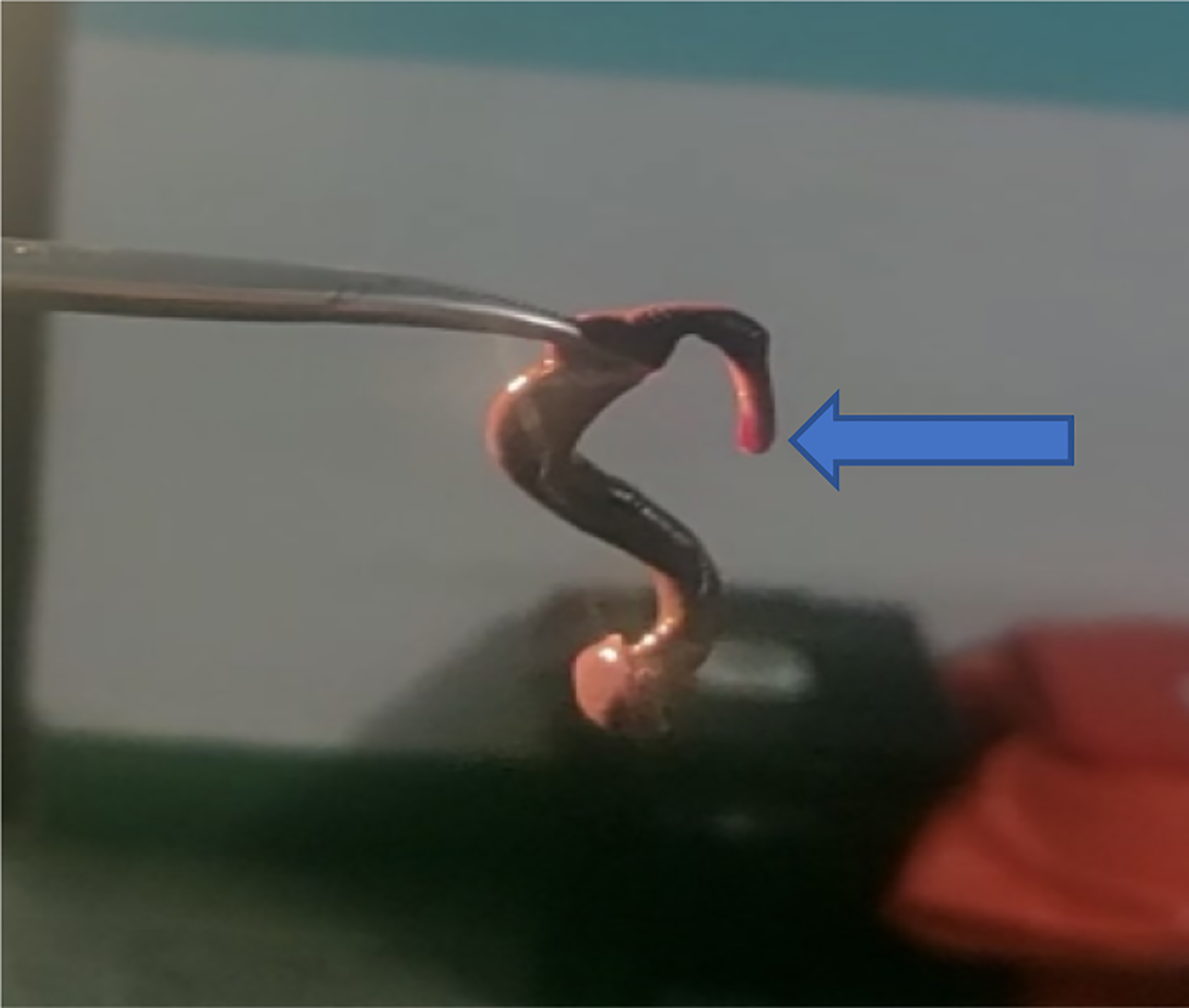
Shows a forceps holding a moving leech, which is dark brown in colour. Anterior sucker is the thinner end (blue arrow) where blood stain is noticeable.
Results
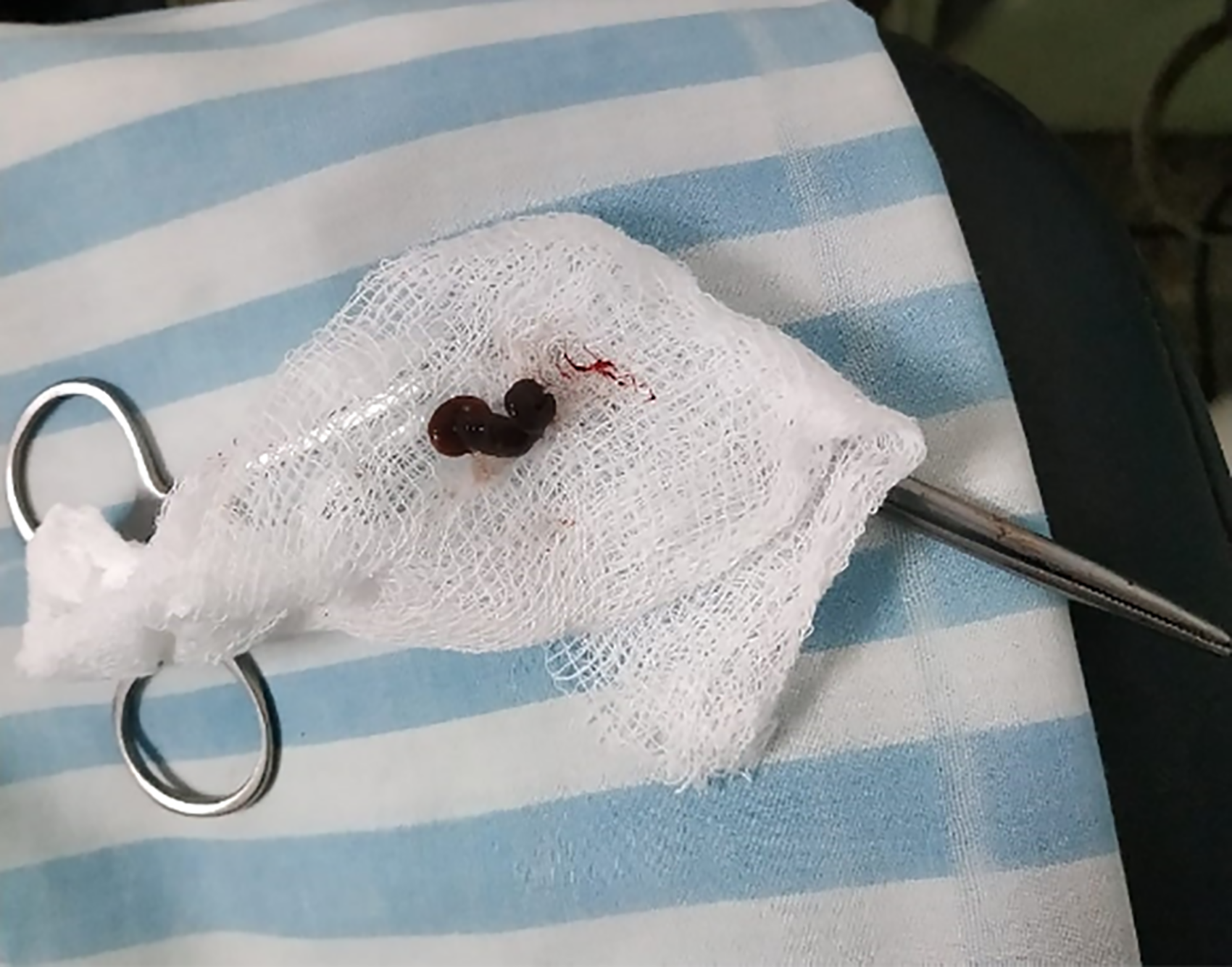
The five had recurrent epistaxis, ranging from one to five days, three with some degree of nasal obstruction. None complained of pain. The leeches were found mostly in the posterior part of the middle meatus (Figure 2), with two only visible by anterior rhinoscopy (Figure 3). One patient was found to have a second leech following removal of the first. Leeches were withdrawn with Tilley's forceps, by grasping the mid-part of the body with a firm but gentle tug. Removal produced minimal bleeding, which stopped spontaneously.

Two dark brown leeches, in various degrees of stretching is seen. The thin ends are the anterior suckers while the thick ends are the posterior suckers.
Shows a dark brown leech in thick shortened state along with Tilley's forceps underneath.
Discussion
Leech infestation, whilst mostly benign, may provoke serious. 8 Leeches are ample in temperate lakes 9 and ponds in the northern hemisphere. 2 Inhabitants and tourists alike, drinking water directly from Himalayan fresh-water falls or springs risk a leech passing into the nostril and lodging there because of its anterior muscular suckers (Figure 4), which latch onto the mucosa siphon off blood. 10 The leech's saliva secretes an anticoagulant, hirudin, which reacts with thrombin and a histamine-like substance that leads to vasodilatation, 2 and an anaesthetic that renders the process painless, probably explaining late presentations of 2–15 days. 10
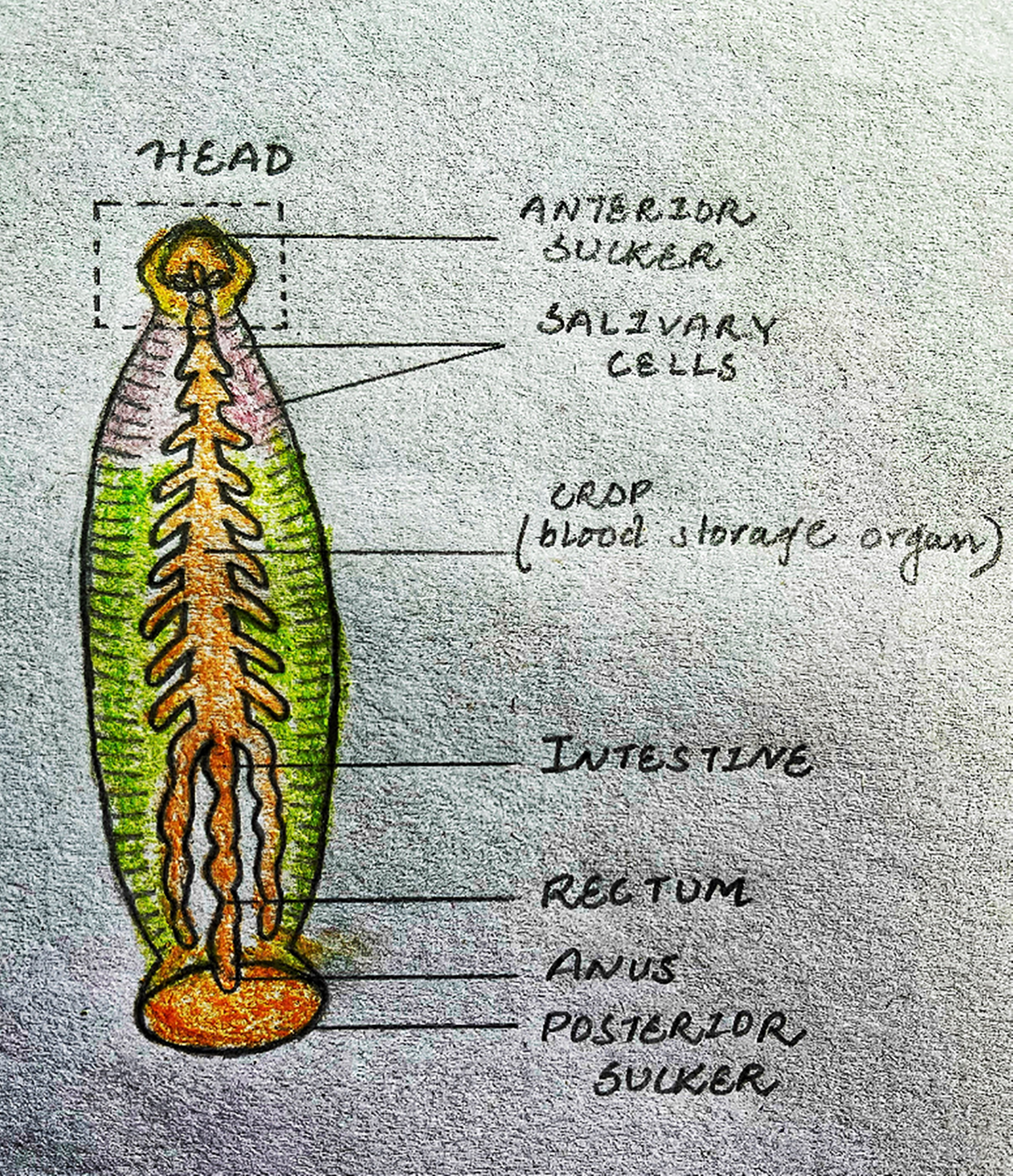
Shows diagram of the anatomy of a leech.
Nasal infestation is much the most common (71%), the nasopharynx (7%), oropharynx (7%) and hypopharynx (14%), being less frequently visited. Commonly leeches are single, but there is documentation of both nasal cavities being infested, and one cavity with multiple leeches.
A leech's stomach can accommodate sucked blood more than eight times its own weight, and thus can cause severe anaemia in patients. 9 They reach a size of 2–12 cm. 10
Examination usually presents with a fleshy dark-brown mobile mass in the infested nostril, best viewed with a nasal endoscope or seen projecting from the naso- or oro-pharynx.2,11,12
Direct extraction of leeches may be onerous, because of their strong sucker affixation to the nasal mucosa and their slithery body 13 and their hiding in the crevices of the meati. A parasitising leech can still evade view, in spite of its enormous blood-engorged state. During extraction, it can rupture easily, thus, care must be taken to detach the leech as a whole. If the head remains, its suckers could still produce bleeding because they contain hirudin. Some have used lidocaine in difficult cases to relax the anterior suckers, or saline to flush out the leech. 1 Alternatively, alcohol, turpentine oil, vinegar, dimethyl phthalate, 1:10,000 adrenaline or 30% cocaine have been tried.14,15
Though suction or using blunt forceps is quicker, manipulation may lead to more bleeding. Extraction may be difficult if a dead leech forms a rhinolith or where the leech is obscured in the middle meati or maxillary antrum.
Footnotes
Acknowledgement
The entire team consisting of the faculty and nursing staff of the Department of ENT, CRH, SMIMS. Special thanks to Ms Chamma Gupta for helping with plagiarism tool and Dr. Amlan Gupta for his guidance. Dr. Gouruv Giri for drawing the diagram, and Dr. Piyush Kumar for helping with converting photo files.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.