
Abstract
Barbados is a Caribbean island with a high incidence of colorectal cancer. This study collected epidemiologic data from Barbadian patients with colorectal cancer. There was an opportunity for targeted screening in patients actively enrolled in clinics for management of chronic diseases, accounting for 72% of cases. We also identified areas of high incidence where resources should be directed in a screening programme.
Introduction
Barbados is an Eastern Caribbean island with a population of 277,821 persons. With an age-standardised colorectal cancer (CRC) rate of 14.8 per 100,000 population, it has the highest incidence of CRC in the Caribbean and second highest in Latin America after Uruguay. 1
Despite this high disease burden, up to the year 2021, Barbados did not have a national CRC screening programme. Consequently, many patients already have locally advanced or metastatic disease at diagnosis when there is less opportunity for cure. It is clear that there is an urgent need for national screening. This study sought to collect epidemiologic data from patients with CRC in Barbados in order to direct national programmes.
Methods
In Barbados, all legal residents are offered free health care funded by a Government administered taxation scheme. Primary care is delivered through a widely distributed network of public clinics. Patients with CRC are referred the Queen Elizabeth Hospital (QEH), the island’s sole government-subsidised tertiary referral centre, for definitive oncologic care. We secured permission from the institutional review board to audit hospital records retrospectively for patients with CRC treated by a surgical team at the QEH between 1 January 2015 and 1 January 2019. Patients’ records were retrieved, and the following data were extracted: age, gender, ethnicity, comorbidities and parish of residence. Descriptive statistical analyses were generated with SPSS version 21.0 using the χ 2 test of independence to investigate correlations.
Results
There were 97 patients with a mean age of 64.9 ± 12.2 years (mean ± SD) treated for CRC over the study period. There was a male preponderance, with 54 males at 64.5 ± 11.3 (mean ± SD) and 43 females at 65.4 ± 13.5 years (mean ± SD). Overall, 93.8% of persons treated for CRC were of Afro-Caribbean ethnicity.
There were 27 otherwise healthy patients at a mean age of 58.4 years (SD ± 12.7). Seventy patients regularly visited clinics to control chronic diseases, including hypertension (52), diabetes (32), cardiac disease (11), restrictive lung disease (7), chronic neurologic disorders (6) and other chronic disorders (7). This group was older, at a mean age of 67.4 years (SD ± 11.2).
We examined the distribution of disease across the island and noticed that the cases were clustered in the southwestern part of the island (58.8%). There were 72 new cases over the four-year study period, within a 10 km radius of the QEH, where an estimated 176,881 persons resided (estimated annual incidence 10.18/100,000 population). Outside the 10 km radius, there were 25 new cases where an estimated 100,940 persons resided (annual estimated incidence 6.19/100,000). The estimated annual incidence was significantly greater within the 10 km radius (P = 0.0396).
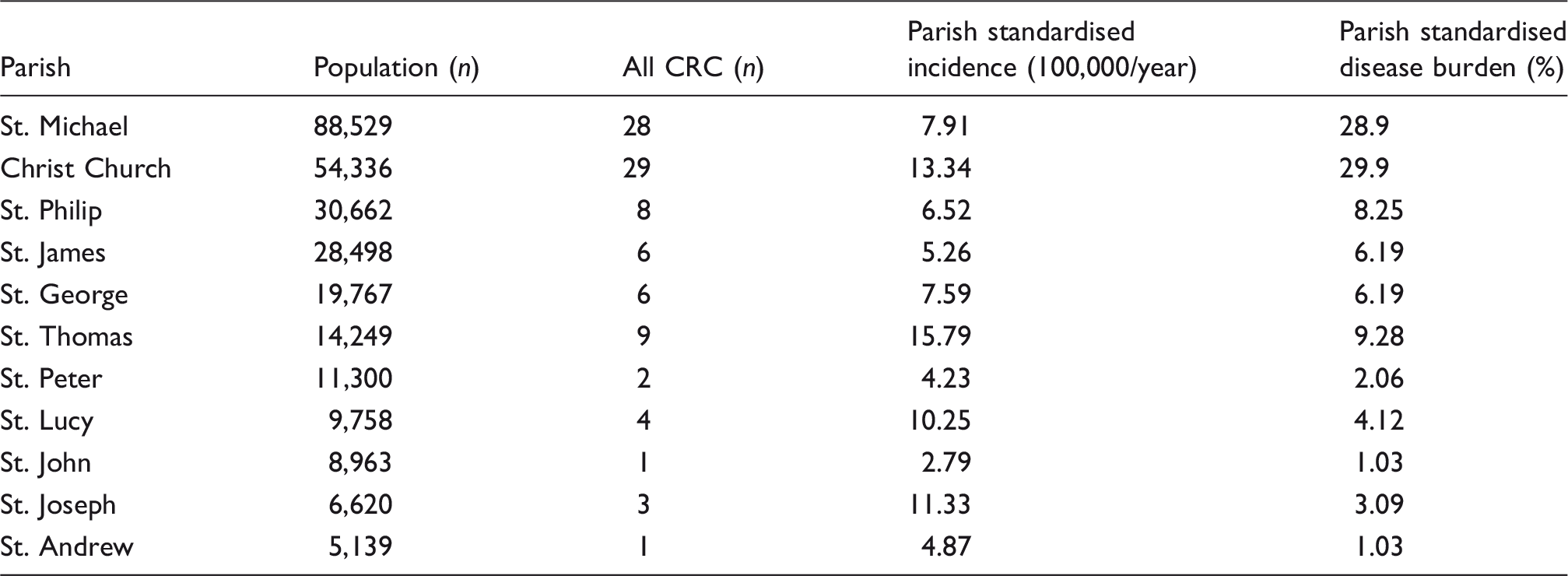
In an attempt to evaluate the disease distribution, we calculated the parish-standardised annual incidence of CRC using the following equation: [100,000 × number of cases in a parish during the study period/parish population]/4 years (Table 1). We also calculated the parish-standardised disease burden using the following equation: (cases in a parish/total number of national cases × 100%) (Table 1). We compared the parish-standardised incidence and disease burden across the island (Figure 1).
A comparison of CRC distribution in parishes across Barbados by case load (a) and parish-standardised annual incidence (b). Distribution of CRC diagnoses according to parishes in Barbados.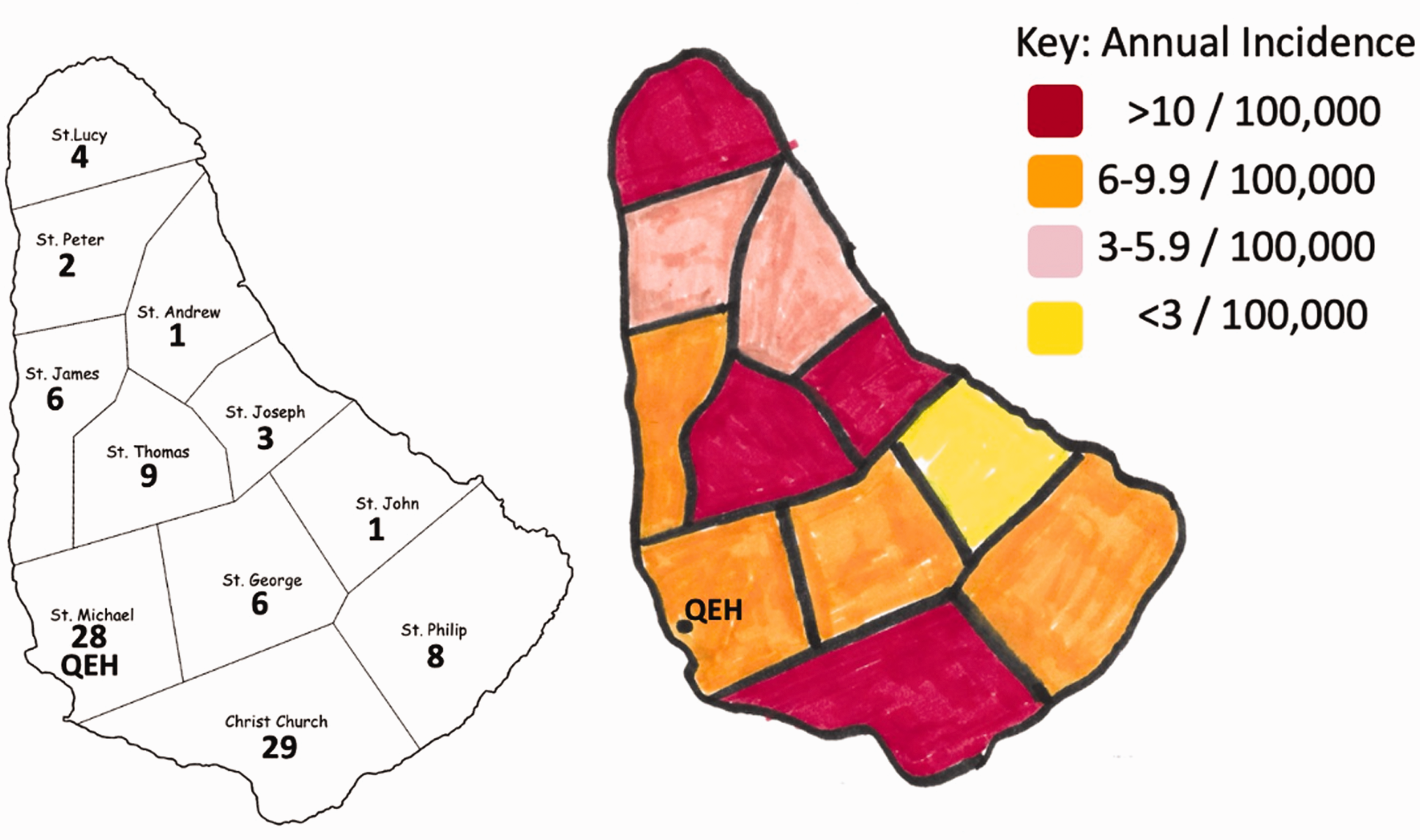
Discussion
With such a high incidence of CRC, most authorities agree that a national screening programme is warranted.2–5 This study provides epidemiologic data from patients with CRC in Barbados that will be useful to guide such programmes.
Although the incidence in Barbados is known to be higher than other Caribbean nations, the demographics were similar to CRC in other Caribbean territories,4–6 with a peak incidence in the seventh decade of life. The high proportion of Afro-Caribbean patients was expected since > 90% of the Barbadian population was black. Although it was an expected finding, one must acknowledge the international data suggesting that blacks tend to have a more aggressive disease course than other ethnicities.7–9 This fact further drives home the need for a national screening programme.
It was noteworthy that 72% of persons diagnosed with CRC were already enrolled in outpatient clinics with regular appointments to control chronic non-communicable lifestyle diseases. It presents a unique opportunity to target them for opportunistic screening as an interim measure while national screening programmes are organised. We do not wish to suggest this as a long-term policy because 28% of persons with CRC were healthy persons in the general community who would be missed.
The distribution of disease was interesting. There was a higher incidence of cases clustered within a 10 km radius of the QEH. We contemplated whether this reflected reduced access to care or lack of transportation for patients outside the 10 km radius, but we did not have sufficient data to make this association. It deserves further investigation because if this is the case, special arrangements would have to be put in place to target persons in the peripheral neighbourhoods.
The parish-standardised annual incidence demonstrated locations across the island where CRC incidence was high. This information can be used to direct distribution of resources when the national screening programme is designed and also for focussed educational drives. The information may also be useful if a further study were able to correlate environmental and/or population-specific risk factors in high-incidence areas.
Supplemental Material
sj-pdf-1-tdo-10.1177_00494755211020573 - Supplemental material for Epidemiology of colorectal cancer in Barbados: A short report
Supplemental material, sj-pdf-1-tdo-10.1177_00494755211020573 for Epidemiology of colorectal cancer in Barbados: A short report by Sahle Griffith, Greg Padmore, Sierra Moore, Keisha Walkes, Abdelaziz A Gohar and Shamir O Cawich in Tropical Doctor
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.