
Abstract
In this study, we investigated the barriers to the delivery of internationally accepted breast cancer care in low resource settings (LRS) as compared to well-endowed resource settings (WRS) via an online survey. The survey was completed by 199 surgeons from eleven countries: 51 from WRS and 148 from LRS, based on our definition. The two most common facilities lacking in LRS were sentinel lymph node biopsy and immune-histochemistry (67% and 60% respectively). Only 22% respondents from LRS confirmed that all their eligible patients received hormonal therapy and only 8% radiotherapy as compared to 98% and 75% from WRS. Widespread limitations exist in most LRS, making internationally accepted breast cancer treatment guidelines impossible to follow, and thus resulting in suboptimal cancer care.
Presentation
Oral presentation based on this project under best paper section was done during the 5th Asian Society of Mastology conference, November 2021.
Oral presentation based on this project was awarded Best Faculty Paper Award during the national annual conference of Association of Surgeons of India, December 2021
Introduction
Breast cancer is now the most common malignancy and the most common cause of cancer- related deaths in 110 states globally, all in to low- and middle-income countries (LMICs). 1 Considerable advances in effective treatment have led to decreased mortality rates across Europe and North America,2,3 but the majority of centres in LMICs still struggle against multiple barriers even to provide basic standard care to breast cancer sufferers. Our study surveyed breast surgeons who work in LRS to describe better the impediments they encounter in their practice.
Methods
Our survey in the English language was designed in google forms with 32 discrete items divided in three sections. The first section had basic identification questions and a question concerning the practice set-up of the respondents. They were asked if they had all these six modalities available: X-ray mammography (MMG), Core needle biopsy (CNB), Immunohistochemistry (IHC), Sentinel lymph node biopsy (SLNB) using radiocolloid, Frozen section biopsy (FSB) and Radiotherapy, all necessary according to current guidelines.4–6 Those having all six modalities were considered to be practicing in an WRS environment and were asked to answer section 2 of the questionnaire. Those lacking any of the six modalities were considered to be practicing in a LRS and were asked to answer section 3 of the questionnaire. Surgeons managing breast cancer were targeted for responses. The survey was distributed using personal contacts of the authors, social networking sites and letters to regional surgical societies. The country of practice was self-assigned by the respondent and only LMIC practitioners were invited to complete our survey. Responses were collected over a period of 15 days from September 20th to October 5th, 2021.
All statistical analyses were performed using SPSS (version16.0; SPSS Inc, Chicago, Illinois). Data were expressed as a proportion of respondents agreeing for a variable and were compared using the chi-squared test A value p < 0.05 was considered as significant.
Results
Responses from 199 surgeons from 60 institutes belonging to 11 countries were received [Figures 1,2]. According to our definition, 51 (26%) were practicing in 14 WRS and 148 (74%) in the remaining 46 LRS.

Low- and middle-income countries and respondents.

World map showing countries from South-East Asia and Africa represented in the survey (in blue).
The pattern of care by practitioners from LRS and WRS is depicted in Table 1. LRS practitioners preferred an inferior to the recommended modality if it was available free of cost whereas 39% WRS practitioners would insist patients arrange their finances to provide for a recommended modality. Only 37 (25%) from LRS performed SLNB in eligible patients as compared to 100% from WRS (p = .001), the main reasons being lack of radio-colloid (40%) and lack of a FSB facility (38%), or requisite training (22%). Similarly, only 42% LRS practitioners offered breast conservation surgery (BCS) to eligible patients, as compared to 98% by WRS practitioners, citing reasons as lack of FSB (51%), radiotherapy facility (48%), or requisite training (25%) and concern regarding unreliable follow-up (64%). Thus, over half of all eligible patients did not receive standard targeted therapy in LRS.
Practice characteristics of the respondents.
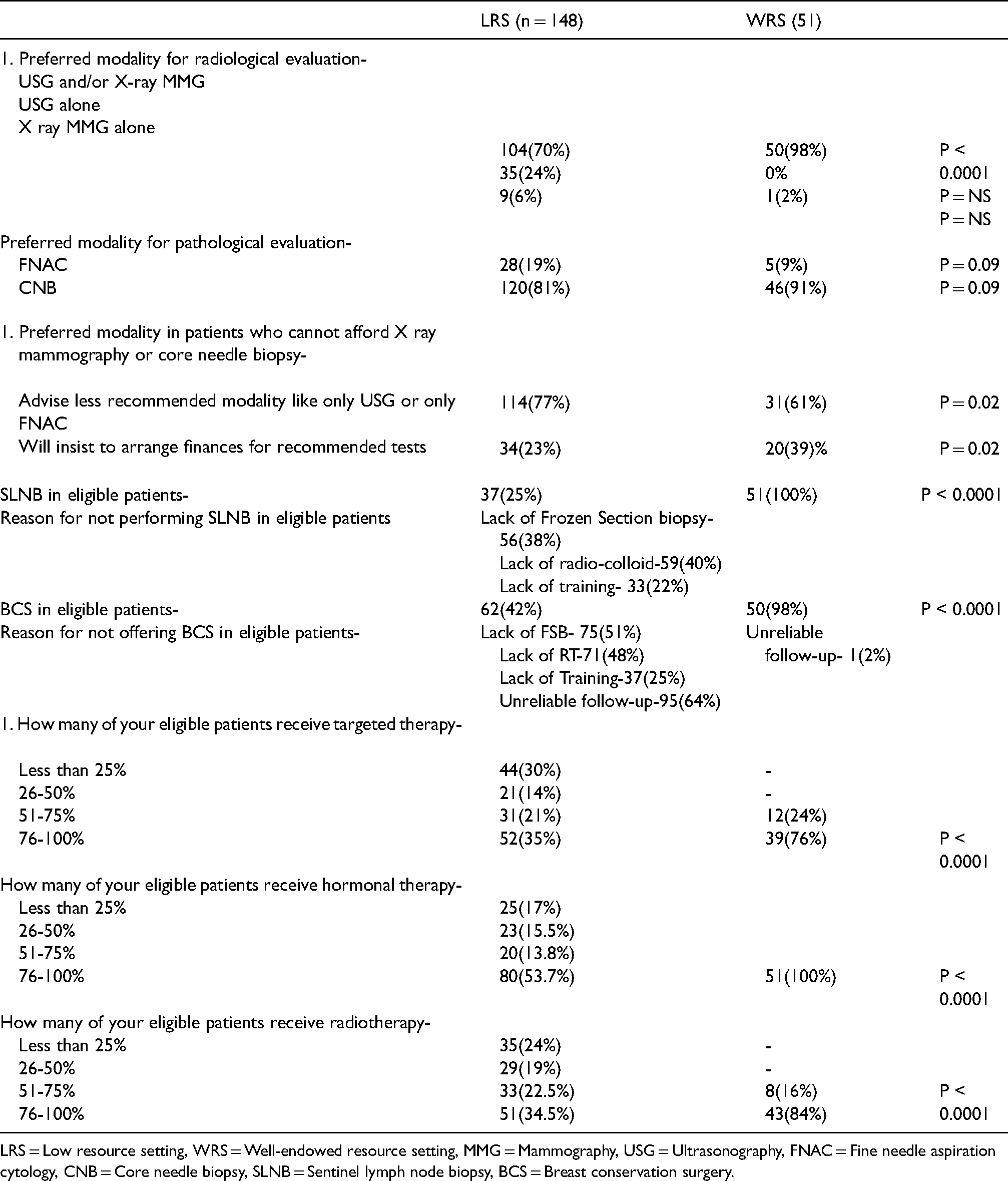
LRS = Low resource setting, WRS = Well-endowed resource setting, MMG = Mammography, USG = Ultrasonography, FNAC = Fine needle aspiration cytology, CNB = Core needle biopsy, SLNB = Sentinel lymph node biopsy, BCS = Breast conservation surgery.
Barriers in delivery of standard breast cancer care as perceived by LRS and WRS practitioners.
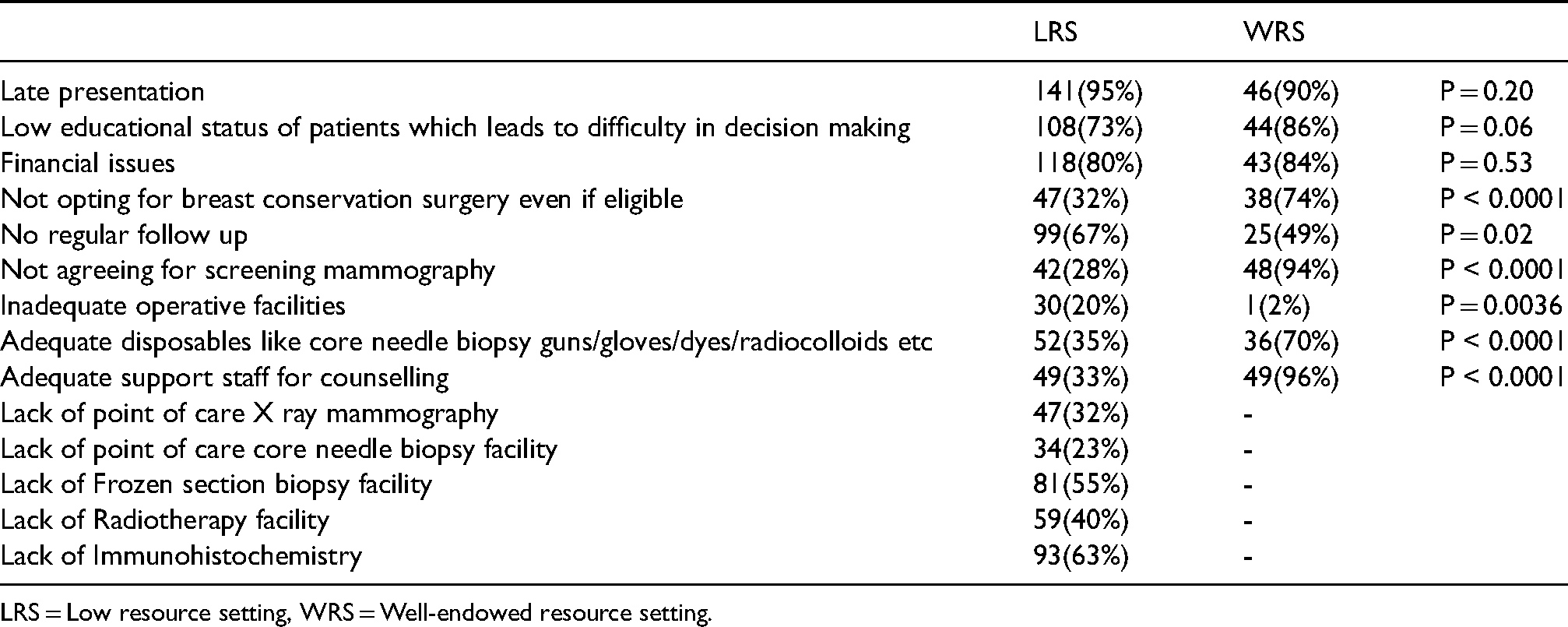
LRS = Low resource setting, WRS = Well-endowed resource setting.
When we compared India-specific data (as Indian surgeons were the most numerous respondents), the pattern remained similar [Table 3]. We also segregated the data based on institutes and unavailable resources are tabulated in Table 4.
Practice characteristics of the respondents from India.
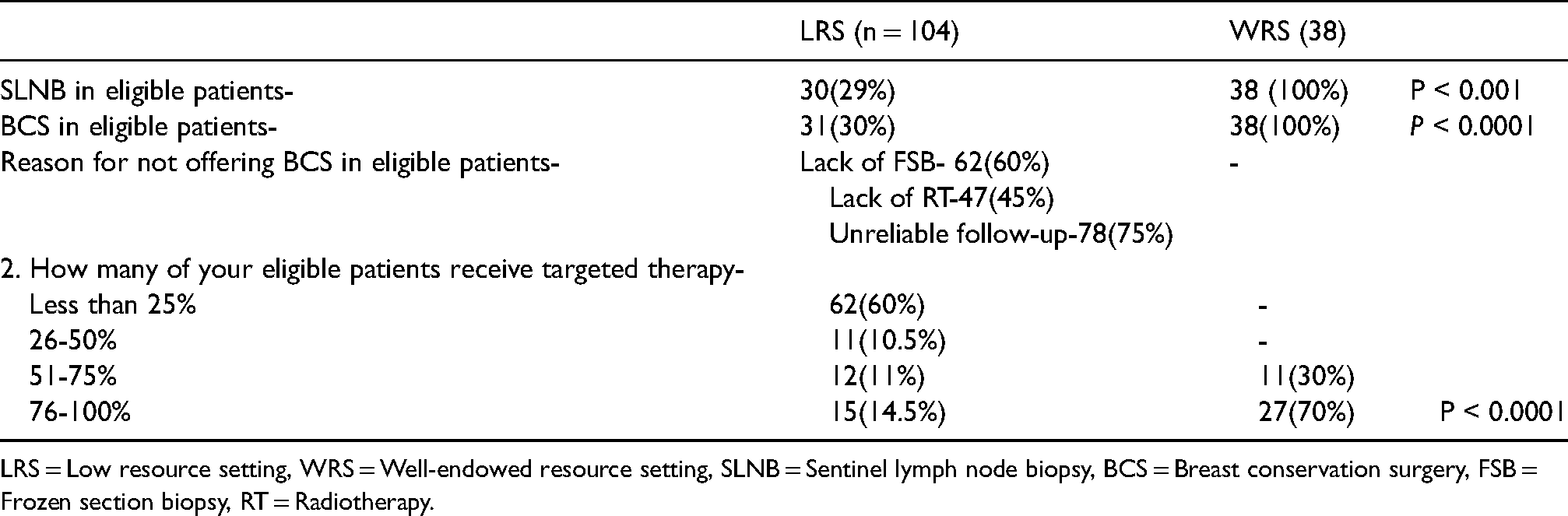
LRS = Low resource setting, WRS = Well-endowed resource setting, SLNB = Sentinel lymph node biopsy, BCS = Breast conservation surgery, FSB = Frozen section biopsy, RT = Radiotherapy.
Unavailable resources at low resource institutes.

Major barriers perceived by LRS (depicted in Table 2) included the lack of IHC (63%), FSB (55%), MMG (32%), CNB (23%) and Radiotherapy (40%). However, all practitioners cited late presentation, lack of formal education leading to difficulties in decision making and financial issues as significant barriers to delivery of established care practice.
Discussion
Many studies have identified the barriers in breast cancer care in LMICs leading to higher mortality.7–9 For example, the cost of a disposable coaxial needle for a core biopsy procedure (minimum US$30) and biomarker studies were frequent barrier in LMICs. 10 Consequently, Breast Health Global Initiative (BHGI) and National Comprehensive Cancer Network (NCCN) have developed guidelines for LRS practice,11,12 recommending the use of IHC to evaluate hormone receptor status in basic resource setting and desirable use of sentinel lymph node biopsy using methylene blue dye alone (instead of combination of radiocolloid and methylene blue dye) at limited resource settings. However, even implementation of these basic guidelines is impossible in the majority of LRS.
In a utopian world ideal breast cancer care would be universally available leading to better overall survival.13–17 However, in the absence of necessary resources, various low-cost innovations can come to LRS’s rescue. These include low-cost core needle biopsy technique, low-cost SLNB technique and clinical breast examination etc.18–20 These validated low-cost alternatives deserve to be included in various guidelines and National Cancer Control Plan (NCCP) of each country.
As with most open online surveys, our survey has notable limitations. Owing to the method of survey distribution, it is likely that those interconnected globally and having academic interests are more likely to have responded, thus skewing the data in favour of desires for utilization of the six modalities. The online format and the sole use of the English language is likewise a serious limitation. Furthermore, practitioners from countries with easy access to the internet and digital literacy are more likely to have responded. Some populous countries for example, China and Brazil, were not represented at all. Other statistical limitations of our study include our inability to calculate actual percentage of responses, the possibility of a non-response, recall bias and brief period of 15 days to collect all the responses.
Earlier studies21–23 which have compared barriers in LMICs do not represent the full spectrum as the classification of countries into LMIC and HIC is inherently broad and limits the comparison of important intra-country- or even inter-city challenges to health care delivery. In spite of inherent limitations of most on-line surveys, our study brings out important information. Sub-optimal access to standard diagnostic and therapeutic modalities24,25 decreases the survival rates, particularly in those patients who might otherwise survive. There is inequity in WRS centres being principally placed in larger cities and such centres are more likely to receive funding than LRS. These WRS, unaware of the resources at LRS, contribute towards best practice guidelines and must be prompted to include what is possible with various low-cost alternatives.
Conclusion
Our survey has brought out various barriers in providing standard breast cancer care in LRSs; not only as compared to WRSs but also among different centers in LRSs. In addition to better resource allocation, there is place for various low-cost alternatives which are deserving of inclusion in guidelines for LRSs.
Footnotes
Author contributions
SKY and DS - Literature search, figures, study design, data analysis, data interpretation, writing.
SS- Data analysis
SKY, DS, DBS, RKL, CKJ- Revision and editing of manuscript
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
This is to declare that all authors have contributed to the study. No part of the manuscript has been sent for consideration elsewhere or published in any International or National journal. The authors clearly certify that there is no aspect of plagiarism. All the conflicts of interest have been clearly defined and the source of grant disclosed. Due ethical permission/consent has been obtained for carrying out the study. In case of any dispute, the authors will be held fully responsible for the statement disclosed in the cover letter. The authors are also aware of the copyright rules and also declare that they will not reproduce any published text without due permission from the journal