
Abstract
We present the results of incorporation of low-cost solutions to provide a standard surgical care for early breast cancer (EBC) patients. This surgical pathway consists of a low-cost vacuum-assisted core needle biopsy, sentinel lymph node biopsy (SLNB) using low-cost methylene blue and fluorescin dyes under local anesthesia and oncoplastic breast surgery. Patients assessed as clinically node-negative axilla underwent such treatment. SLNB using low-cost dyes was performed without any complication. Oncoplastic surgical techniques were opted for in 32 patients, and the lumps were all excised with a ∼1-cm all-around margin on the final histopathological examination. Standard breast cancer surgery can be provided in low-resource settings to eligible EBC patients with low-cost solutions.
Introduction
Breast cancer is the most common cancer worldwide and the most common cause of cancer-related deaths in 110 countries globally, all of low- and middle-incomes (LMICs). 1 Several breakthroughs in the management of breast cancer have led to <2–5% disease-specific mortality rates across Europe and North America. 2 Most centres in LMICs struggle to provide basic standard care to breast cancer sufferers, thus leading to sub-optimal cancer care. 3 Hence, effective low-cost alternatives are needed to provide standard breast cancer care in LMICs.
Methods
Our prospective study was conducted between May 2021 and May 2022 at the Department of Surgery, Government NSCB Medical College, Jabalpur, India, with approval from our Institutional Ethics Committee. All early breast cancer (EBC), clinically and ultrasonologically negative axilla (cN0) patients were included. After the assessment, they were treated following our low-cost surgical pathway (Figure 1). All breast lumps underwent triple assessment with clinical, breast and axillary ultrasound, mammography and histopathological examination. A low-cost vacuum-assisted core needle biopsy (VACNB) technique was used to obtain histopathological specimens. 4 All patients were staged as per TNM staging, 8th edition AJCC/TNM manual. 5 All patients were subjected to sentinel lymph node biopsy (SLNB) using a low-cost dual dye technique under local anesthesia at first-stage surgery. 6 After receiving the histopathological report, a second-stage surgery was planned; patients were offered the choice between breast conservation surgery (BCS) and simple mastectomy with or without axillary lymph node dissection (ALND) depending upon the SLNB status. Those opting for BCS underwent oncoplastic breast surgery (OPBS) with a macroscopic margin of at least 1 cm. During this second-stage surgery, ALND was also performed for SLNB-positive patients. Following excision, the breast specimen was orientated with sutures and bisected to identify the tumour and distance to individual radial margins.
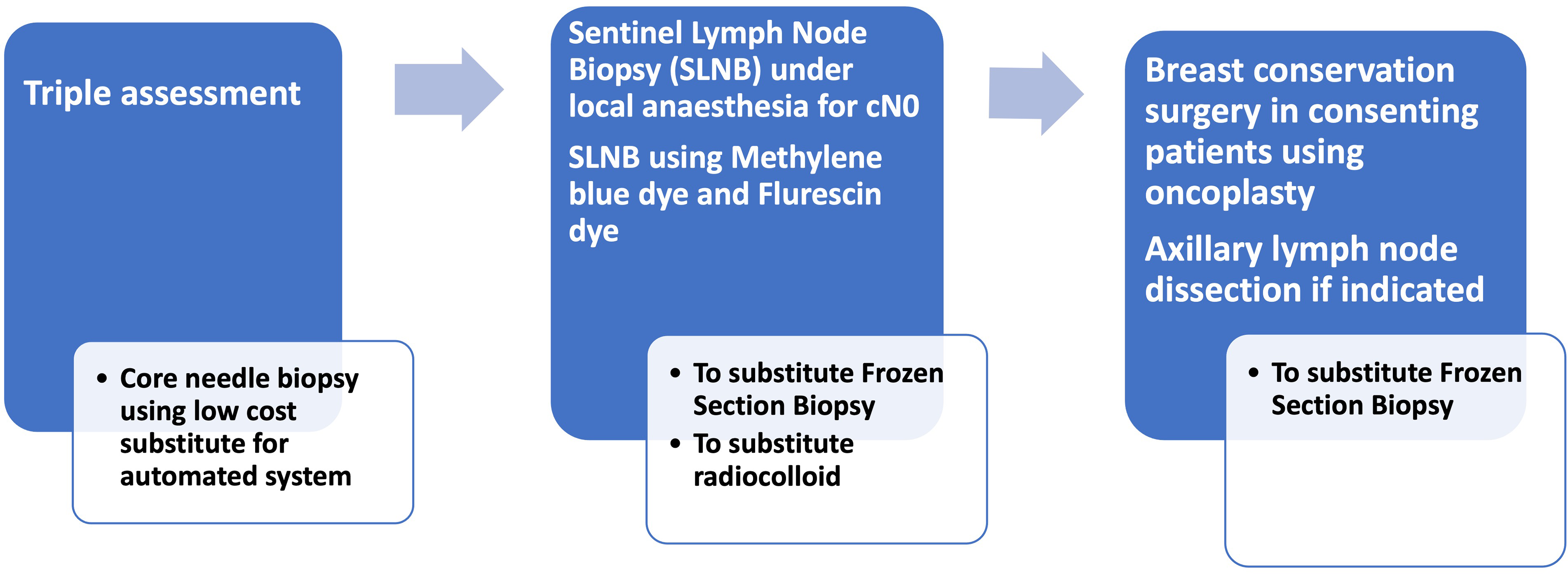
Low-cost surgical pathway.
Results
A total of 45 EBC patients’ basic demographic profile, clinical and molecular details are depicted in Table 1. Our low-cost VACNB technique diagnosed malignancy in 43/45 patients. Two patients required repeat biopsy using an automated core needle biopsy technique. The median number of sentinel lymph nodes identified was 3.5 (range 2–5). BCS was chosen by 32, with the remainder undergoing a simple mastectomy. Oncoplastic surgical techniques were used in BCS patients with the lump being excised with a 1-cm margin all around on gross examination by the operating surgeon. No patient was found to have a positive cancer margin (<1 cm) on gross examination and hence none required re-excision. On final microscopic examination, the mean margin was 14 ± 3 mm (Table 2). Metastatic SLNs were found in 8/45 in patients who underwent ALND during the second-stage definitive surgery. There were no complications related to VACNB nor dual-dye SLNB studies. Two patients had seromas requiring multiple aspirations and one patient had a surgical site infection.
Demographics and clinical profile.

Surgical details and histopathological findings.
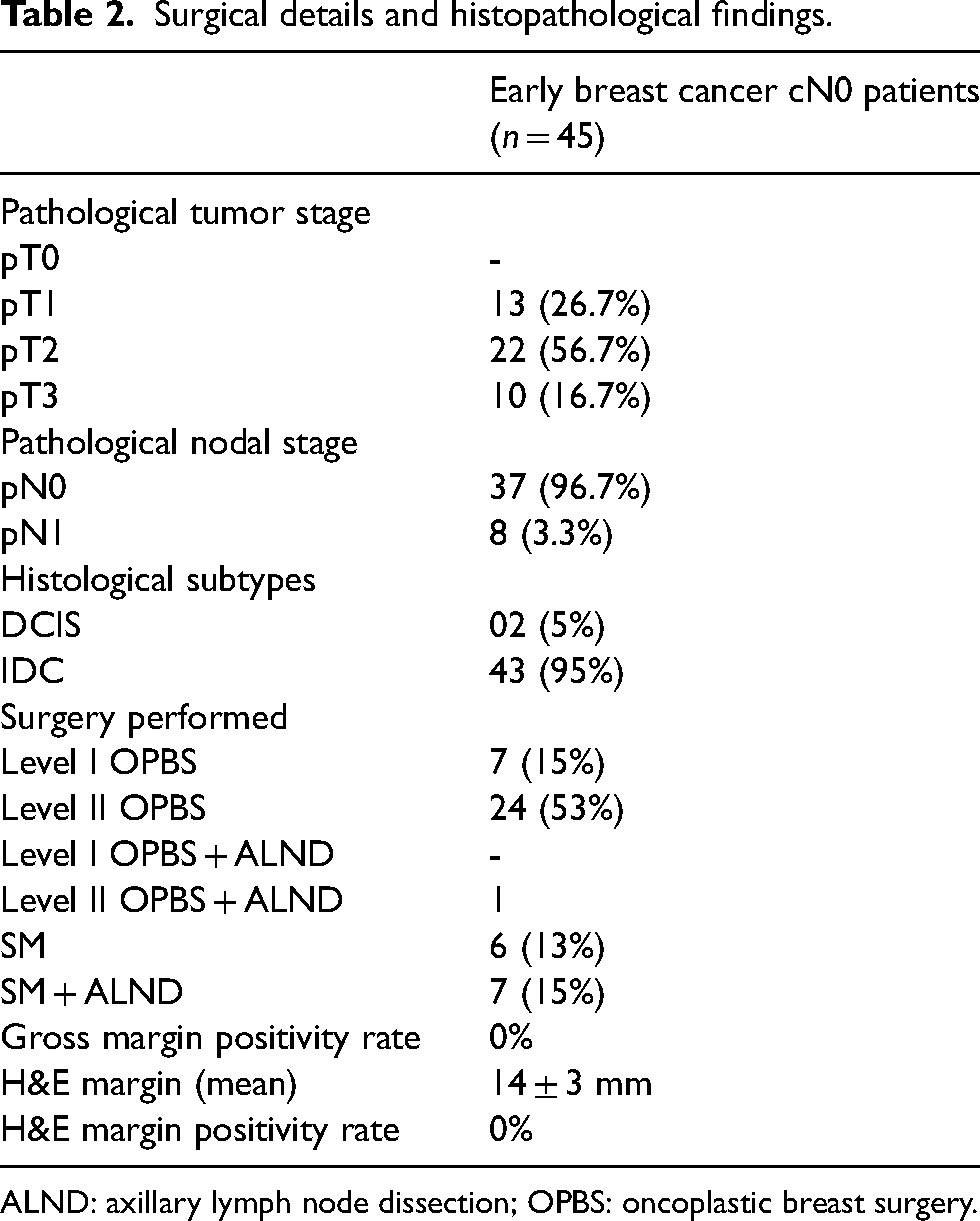
ALND: axillary lymph node dissection; OPBS: oncoplastic breast surgery.
All patients received adjuvant chemotherapy as the average tumour size was higher (>1 cm) in this cohort. Trastuzumab-based targeted therapy (although quite expensive, but fortunately available through a special Government public health insurance fund that provides free treatment for low-income patients) and hormonal therapy were offered to 10 and 21 patients, respectively, based on the immune-histochemistry result. Radiation therapy was administered to 43 patients who include 32 who underwent OPBS and 11 based on positive axillary metastasis or tumour size.
The mean follow-up was 8 ± 5 (range 2–18) months. No patient had clinical features of lymphoedema or restriction of shoulder joint motion post-operatively. There was no local or axillary nodal recurrence in our cohort over this follow-up period.
Discussion
Improved breast cancer survival represents the triumph of scientific advances and the implementation of standard, internationally accepted guidelines. However, widespread limitations exist in most LMICs, making these guidelines impossible to follow, and thus resulting in suboptimal cancer care. 3
Core needle biopsy, SLNB and BCS are the three pillars of standard treatment for EBC. CNB is recommended, by most guidelines, as the technique of choice for obtaining tissue for histopathology. 7 Unfortunately, the cost of commercially available core biopsy systems (needle c. 41 US$; and vacuum-assisted breast biopsy needle c. 341 US$) make this a major limitation in LMICs. We used our frugally innovated and previously validated VACNB system (cost c. 5.50 US$) 4 and were able to confirm malignancy in the vast majority of our ECB patients.
Arm and shoulder morbidity after routine ALND has led to the recommendation of the use of SLNB in cN0 patients.7–9 However, the high cost and lack of availability of radio-colloid dye as well as the absence of frozen section facilities are well-known barriers. Our previously validated technique of low-cost dual dye SLNB under local anaesthesia enabled us to perform SLNB in our EBC patients. 6 These drawbacks were overcome by performing the SLNB under local anaesthesia as the first stage and then performing the definitive BCS ± ALND or SM ± ALND under general anaesthesia in the second stage once the histopathology report became available after a few days. Touch imprint cytology for SLNB specimens may be a substitute and we are currently conducting a prospective study to evaluate its accuracy.
Barriers to offering BCS in LMICs are well known, viz. a lack of trained surgeons, a lack of radiotherapy, a lack of frozen section facilities and low patient acceptance.3,10,11 These are reasons for lower rates of BCS in LMICs (10–50%) as compared to rich countries (>60%).12–14 Likewise, a direct relationship has been observed between the availability of radiotherapy and BCS rates, independent of demographic and tumour variables. 13
We managed intraoperative margin assessment, considered an important standard of care, by having BCS performed by a specialist breast surgeon, followed by radiotherapy. We were emboldened by the fact that OPBS obtains a wider excision margin and the ‘elbow room’ allowed by standard guidelines to individualise treatment according to available resources.15,16
Our approach was validated by our good histopathological margins, with zero gross and histopathological margin positivity rates. This allowed us to increase the rate of BCS to c. 70% of eligible EBC patients.
It is known that relatively fewer EBC cases are seen in LMICs17,18; these patients, therefore, deserve a standard of care to optimise survival rate. Needs-driven low-cost surgical innovations can provide simple, safe, ethical and local evidence-based customised solutions thus to achieve health equity for underserved populations. 19 Another welcome trend in this contemporary medical field, which resonates with our low-cost pathway, is an increased call for ensuring the involvement of all LMIC stakeholders, when framing contextualised guidelines.20,21
The lack of long-term follow-up is a major limitation of our study as we are not able to calculate recurrence rate, overall and disease-specific survival with the short follow-up allowed by our study. Our sample size is also small but since >70% of patients present with locally advanced breast cancer, EBC patients take much longer to recruit. We are continuing to evaluate long-term outcome and validation.
Further, all procedures were performed by a single specially trained breast surgeon, so our results may not extrapolate to a wider group of surgeons. However, the major message is that each low-cost component was validated separately before being incorporated into our standard surgical pathway, and the techniques are readily learnt.
Footnotes
Authors’ contributions
SKY and DS – Conceptualisation, Study design, Implementation, literature search, figures, data collection, data analysis, data interpretation, and writing. DBS, AM, PA – Revision and editing of manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from the participants. This is to declare that all authors have contributed to the study. No part of the manuscript has been sent for consideration elsewhere or published in any International or National journal. The authors clearly certify that there is no aspect of plagiarism. All the conflicts of interest have been clearly defined and the source of grant disclosed. Due ethical permission/consent has been obtained for carrying out the study. In case of any dispute, the authors will be held fully responsible for the statement disclosed in the cover letter. The authors are also aware of the copyright rules and also declare that they will not reproduce any published text without due permission from the journal.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.