
Abstract
Hypoxaemia in COVID-19 does not necessarily imply COVID pneumonia or post-COVID lung fibrosis, and the caveats of finger pulse oximetry should be remembered. Drug-induced methaemoglobinemia should be considered in individuals with unexplained cyanosis, refractory hypoxaemia, or the presence of a saturation gap. Here, we share our recent encounter of ‘spurious hypoxia’ in a patient with COVID-19 and methaemoglobinemia.
Case report
A 21-year old woman presented with fever, sore throat, and dry cough of three months’ duration. There was no breathlessness, chest pain, nor palpitation. A throat swab for a reverse-transcriptase polymerase chain reaction was positive for SARS-CoV-2. She was advised home isolation and self-monitoring of symptoms. During isolation, she noted an oxygen saturation (SpO2) of 84–86% at a fraction of inspired oxygen (FiO2) of 0.21. She was prescribed oral corticosteroids and home oxygen supplementation owing to the possibility of SARS-CoV-2 pneumonia. While she had no respiratory symptoms and continued to have hypoxaemia, she was referred two months later as a case of post-Covid lung disease.
On admission to, she was comfortable, with a respiratory rate of 22/min, and SpO2 of 86% (FiO2 of 0.6). There was no cyanosis, oedema, nor crackles on lung auscultation. Her chest radiograph was unremarkable, and electrocardiogram and echocardiography normal. Compression ultrasonography of both lower limbs and CT pulmonary angiography ruled out a venous thromboembolism. Investigations revealed a haemoglobin level of 126 g/L; arterial blood gas pH of 7.45, partial oxygen pressure 88 mmHg, partial carbon dioxide pressure 41.1 mmHg and bicarbonate level 28.1 mmol/L. The arterial oxygen saturation was 97% when the corresponding SpO2 was 86%. The elevated ‘saturation gap’ (SaO2–SpO2) suggested the presence of abnormal haemoglobin. Co-oximetry showed an elevated methaemoglobin level (12%).
Thus, on further inquiry, she reported a history of leprosy diagnosed six months earlier based on a skin biopsy from hypopigmented anaesthetic macules over her left leg. She had been started on standard multi-drug therapy (MDT) for borderline tuberculoid leprosy with dapsone, clofazimine and rifampicin. Consequently, a diagnosis of acquired methaemoglobinemia due to dapsone and clofazimine, both possible culprit drugs was suggested. Glucose-6-phosphate dehydrogenase (G6PD) deficiency was ruled out. Co-oximetry repeated 48 h later showed a methaemoglobin concentration of 2.8%, and her SpO2 subsequently improved (94% on room air).
Discussion
Methaemoglobin is a form of oxidized haemoglobin where the haeme iron configuration changes from the ferrous to the ferric state. In physiological conditions, the concentration of methamoglobin is <1%. Elevated levels cause a left shift of the oxygen haemoglobin dissociation curve, a reduction in the oxygen-carrying capacity of haemoglobin, and tissue hypoxia. 1 Methaemoglobinemia may be congenitial, due to genetic defects in the enzyme responsible for reducing the ferric iron or acquired, where an inciting agent overwhelms the reducing mechanisms. The latter has frequently been implicated from exposure to dapsone but more rarely with clofazimine. 2 Symptoms and signs depend on the methaemoglobin concentration and may range from mild cyanosis, dyspnea, to shock, severe respiratory depression, or neurologic deterioration (coma, seziures) owning to tissue hypoxia, which can be fatal. The standard pulse oximeter works on the principle of a differential absorption spectrum of oxygenated (660 nm) and deoxygenated (940 nm) haemoglobin in the blood. Methaemoglobin absorbs both 660 nm and 940 nm resulting in a falsely low SpO2 reading. Methaemoglobinemia should be suspected in the presence of cyanosis, refractory hypoxaemia (despite oxygen supplementation), and a ‘saturation gap’. 3
Treatment is primarily guided by the clinical manifestations as well as the methaemoglobin level. The causative agent must be discontinued in all cases. Mildly symptomatic individuals improve with supportive care. Those with higher concentrations of methaemoglobin and severe symptoms should be treated with intravenous methylene blue, ascorbic acid, or red cell exchange transfusion. 4 Methaemoglobinemia in SARS-CoV-2 infection has been described with severe infection, G6PD deficiency or treatment with hydroxychloroquine (Table 1).5–9 In our case, SARS-CoV-2 was probably a ‘red herring’. While erroneous pulse oximetry readings may occur owing to the cutaneous involvement of fingers by leprosy, 10 acquired methaemoglobinemia is an important consideration and has therapeutic implications. Hypoxaemia in COVID-19 does not necessarily imply COVID pneumonia or lung fibrosis, and the caveats of pulse oximetry should be remembered; drug-induced methaemoglobinemia is an important cause of falsely low SpO2.
Cases of SARS-CoV-2 infection-associated methemoglobinemia.
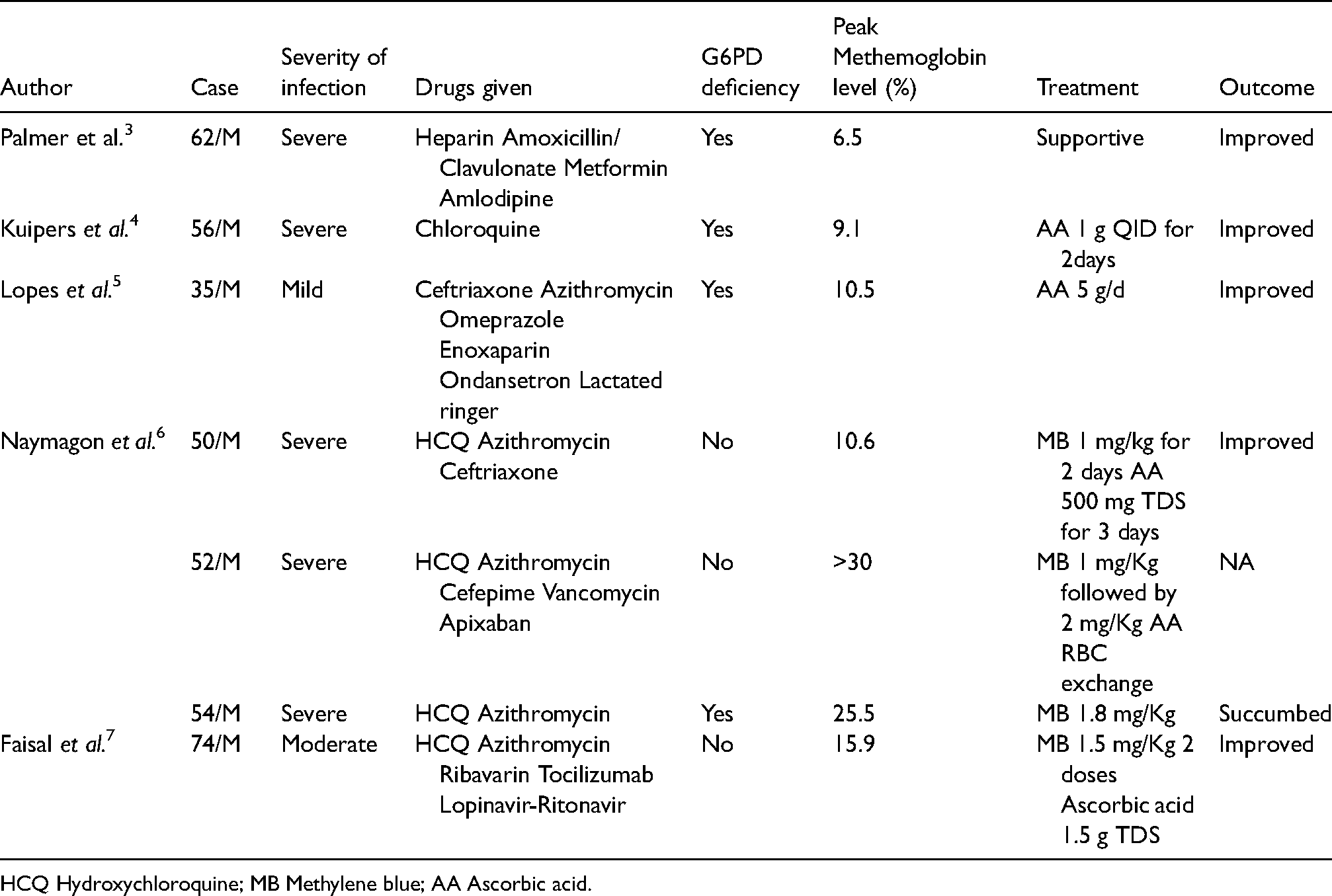
HCQ Hydroxychloroquine; MB Methylene blue; AA Ascorbic acid.
Footnotes
Acknowledgements
None
Author contribution
BC: Patient management drafted and revised the manuscript
NA: Drafted the manuscript
SC: Patient management, gathered the data and revised the manuscript
AKP, VM: Patient management, revised the manuscript
MKH: Patient management, revised the manuscript, conceived the idea, revised the manuscript
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.