
Abstract
Haemophagocytic lymphohistiocytosis occurs due to an uncontrolled inflammatory state and can be life threatening. Common triggers are infections, autoimmune diseases, malignancy or can be familial. Early treatment is life-saving especially in cases due to secondary infections. Here we present a rare case of haemophagocytic lymphohistiocytosis in visceral Leishmaniasis, where complete response resulted following treatment of the primary disease.
Keywords
Case report
A male in his 30s was admitted in our hospital with history of intermittent fever of 38.3οC, loss of appetite and significant loss of weight (10Kg) of six months’ duration. On clinical examination he was pale, had hepatosplenomegaly (liver palpable 4 cm and spleen 9 cm below the costal margin) but no lymphadenopathy. Laboratory investigations revealed an anaemia (Hb 94 g/L), leucopenia (white cell count 1.5 × 109/L), thrombocytopenia (platelet count 105.5 × 109/L, raised erythrocyte sedimentation rate of 42/h, and AST (Aspartate Transaminase) of 5.36 µkat/L and ALT (Alanine Transaminase) of 4.48 µkat/L. Repeated blood cultures were sterile; Brucella serology, HIV, HbsAg and anti-HCV negative. An abdominal CT scan showed hepatosplenomegaly with no lymph node enlargement (Figure 1). Further laboratory tests showed raised serum ferritin of 3695 μg/L (norm: < 500 μg/L), raised triglyceride 3.89 mmol /L (norm: < 3mmol/L) and low fibrinogen of 0.269 g/L (norm: < 1.5 g/L) suggestive of haemophagocytic lymphohistiocytosis according to HLH-2004 criteria. Bone marrow aspiration and biopsy was normal. Splenic aspiration showed extracellular and intracellular Leishmania Donovani bodies within macrophages (Figure 2(a) and (b)). Our patient was thus commenced on intravenous liposomal amphotericin B at 150 mg per day, following which normalization of his laboratory parameters, of fever and splenomegaly, resulted.
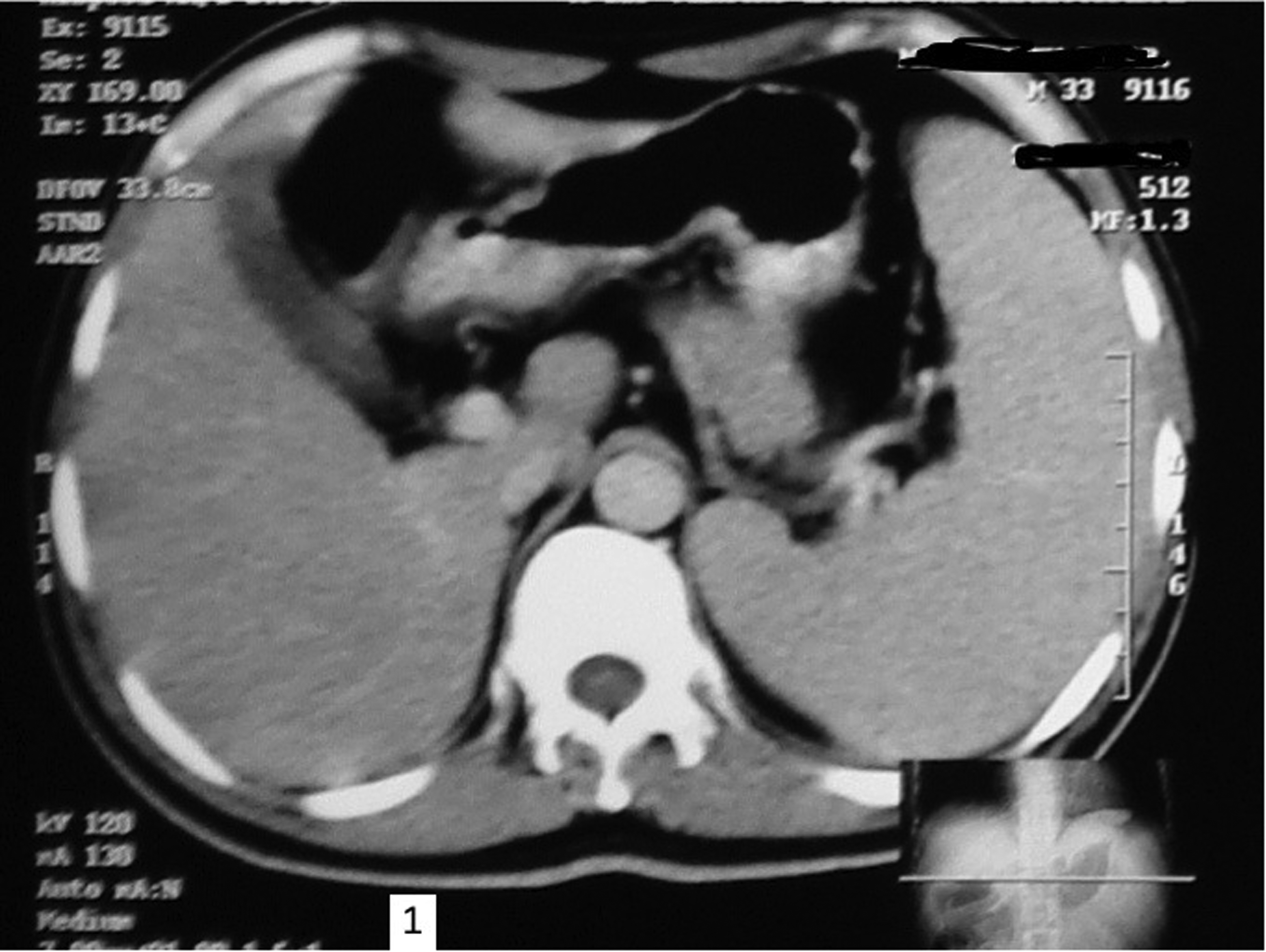
Abdominal CT scan showing hepatosplenomegaly.

Light microphotographs of splenic aspirate showing amastigote forms of Leishmania donovani (LD bodies) within macrophages and few extracellular LD bodies (black arrows) (X400).
Discussion
Leishmaniasis is a major vector-borne illness in tropical regions caused by around 20 species of leishmania parasite transmitted by the female sandfly. Three main forms are visceral, mucocutaneous and cutaneous leishmaniasis. The major burden of disease is in Brazil, China, Ethiopia, India, Kenya, Somalia, Eritrea, Yemen, South Sudan and Sudan which account for 90% of total cases. 1 Visceral leishmaniasis is caused by L donovani in Africa, Asia and infantum type in the Mediterranean, Central Asia, Middle East, South and Central America. 2 Haemophagocytic lymphohistiocytosis is a rare condition with uncontrolled hyperactivation of the immune system leading to a hyper-inflammatory state associated with high morbidity and mortality. It can be primary (familial) or secondary, whose causes include haematological malignancies (56.4%), infections (24.7%), autoimmune conditions and immunodeficiency states. 3 Diagnostic criteria require the presence of one of (1) A molecular diagnosis consistent with HLH for familial type and (2) Five out of the following eight criteria: fever, splenomegaly, cytopenia (affecting two or more lines), raised triglycerides, low fibrinogen, raised ferritin, evidence of haemophagocytosis in bone marrow, spleen, lymph nodes, or low or absent natural killer (NK) cell activity, or elevated soluble CD25 (IL-2 receptor).4,5
It may be difficult to distinguish between HLH and visceral Leishmaniasis associated HLH owing to similar clinical and laboratory findings including fever, cytopenia affecting one or more cell lines, and hepatosplenomegaly. Various diagnostic tests exist including indirect serological tests such as the Rk39 based immune-chromatographic test, PCR assays, enzyme linked immunosorbent assay, Western blot, indirect immune-fluorescent antibody assay and direct visualization of amastigote forms in tissue.6 Rk-39 is a rapid diagnostic test with sensitivity of 97% and specificity of 98.9% with good prognostic value. 6 Definite diagnosis in remains the detection of the parasite. However, its yield differs, the highest being bone marrow, lymph nodes, and blood. 7 Leishmania Donovani bodies are small, oval with diameter of 2–4 μm and indistinct cytoplasm, a nucleus, and a small rod-shaped kinetoplast Extracellular LD bodies can also be visualised if released from damaged cells. 8 Both leishmania or HLH may not be detected on initial bone marrow aspirate. LD bodies were negative in 64.7% of patients and hemophagocytosis was absent in 36.3% on initial bone marrow aspiration in study by Rajagopala S et al. Treatment consists of intravenous amphotericin B; response is good in visceral Leishmaniasis associated HLH, however immunosuppressive therapy may be required in non-responsive patients. 7
Differential diagnosis to be considered includes disseminated tuberculosis, histoplasmosis, scrub typhus and dengue fever. 9 Serological tests for VL may clinch an early diagnosis and enable treatment to be initiated thus avoiding serious complications.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.