
Abstract
The aim of our study was to determine the prevalence of chronic pulmonary aspergillosis in pulmonary tuberculosis patients and the antifungal resistance of Aspergillus spp. isolates in Uzbekistan. Chronic pulmonary aspergillosis was detected in 11.4% and 20.0% of smear-positive and smear-negative pulmonary tuberculosis patients, respectively.
Introduction
Chronic pulmonary aspergillosis (CPA) may present as a chronic and progressive disease occurring mainly in immunocompetent individuals with underlying lung disease, most commonly with pulmonary tuberculosis (PTB). The spectrum of CPA includes simple aspergilloma, chronic cavitary pulmonary aspergillosis, aspergillus nodules, sub-acute invasive aspergillosis, and chronic fibrosing pulmonary aspergillosis.1,2 The distribution of CPA remains wide, with more than 3 million affected, mostly PTB patients.;3–6 a high incidence in Asian countries, followed by Africa and North America, has been described. 5 There is a 5-year prevalence of CPA as a complication of PTB estimated at c. 1.2 million worldwide. 6 Even with antifungal therapy, its mortality rate is 20–33% in the short term and 50% in a 5-year period.7,8 Recent studies have shown differences in the global burden of CPA between populations at risk and countries with different socio-economic and geo-ecological characteristics.
Despite a significant decrease in tuberculosis incidence in Uzbekistan over the past ten years, PTB remains one of the most important challenges in the country. 9 Clinical symptoms such as chronic productive cough, weight loss, fatigue, fever, haemoptysis, and chest pain are clinically indistinguishable between CPA and PTB. Moreover, the progressive cavitation, fibrosis, and pleural thickening seen in CPA are similar features in both.10–12 However, the precise incidence of CPA post-PTB remains unknown, and deciding which groups of PTB patients should be screened for CPA is unclear. 13
In low- and middle-income countries, the lack of the availability of the necessary diagnostic tools leads to late diagnoses or misdiagnoses.14,15 Long-term antifungal therapy, mainly with voriconazole and itraconazole, can significantly improve the survival rate. However, lack of knowledge of the optimal duration of therapy, the high resistance of pathogens to antifungals, and the risk of intolerable side effects can be important limitations of therapy. In addition, relapses occur in c. 33% patients after the cessation of treatment. 16 The prevalence of CPA in smear-positive and smear-negative PTB patients and the antifungal resistance of Aspergillus spp. isolates have not been studied in Central Asian countries, including Uzbekistan.
Materials and methods
Our prospective observational study was conducted by the Republican Specialized Research and Practical Medical Center of Epidemiology, Microbiology, Infectious and Parasitic Diseases and the Republican Specialized Research and Practical Medical Centre of Tuberculosis and Pulmonology, Tashkent, Uzbekistan, during the period from May 2020 until May 2021.
All participants provided written informed consent, and ethical approval was obtained from the Ministry of Health of the Republic of Uzbekistan in accordance with the guidelines of the Declaration of Helsinki. The trial is registered at the US National Institutes of Health (ClinicalTrials.gov #NCT05045391).
A total of 200 patients (aged >18 years) with PTB (140 with smear-positive and 60 smear-negative) were included in the study. Forty-six were excluded, including 12 who refused to participate and 34 who did not meet the inclusion criteria.
The diagnosis of PTB was based on the results of clinical examinations, chest radiographs and laboratory examinations according to the World Health Organization guidelines. 17
The smear-positive PTB group included patients with at least two initial sputum smear examinations positive for Mycobacterium tuberculosis as determined by direct microscopy, or patients with one initial smear examination positive and one positive culture, or patients with one initial smear examination positive and radiographic findings consistent with active PTB.
The smear-negative PTB group included patients with negative sputum smears but positive growth cultures or patients with at least two negative sputum smears and radiological findings consistent with radiologically active PTB.17–19 According to radiological findings, PTB was presented as infiltrative, fibrotic-cavernous, disseminated, tuberculoma, and focal forms.
All PTB patients were treated with standard 5-medicine therapy. Patients with neutropenia or severe immunosuppression owing to chemotherapy, haematopoietic stem cells or solid organ transplantation, prolonged immunosuppressive therapy or HIV, were excluded from the study.
The CPA diagnosis was made according to the guidelines established by the European Society for Clinical Microbiology and Infectious Diseases/European Respiratory Society and Infectious Disease Society of America,20,21 according to the following criteria: (1) chronic pulmonary or systemic symptoms compatible with CPA, for a minimum 3 months, including at least one of the following symptoms: weight loss, productive cough, or haemoptysis; (2) radiological findings showing cavitary pulmonary lesion(s) with evidence of para-cavitary infiltrates and adjacent pleural thickening with or without a fungal ball; (3) positive Aspergillus IgG in blood serum and/or a positive Aspergillus culture or sputum as determined by microscopy; and (4) the exclusion of similar presentations caused by a neoplasm, abscess, Wegener's granulomatosis, etc.
The identification of Aspergillus spp. was performed based on direct examination, colony colour, and mould counts exceeding 105CFU/mL on Sabouraud Agar medium (Geetapharm, India) at 35°C for 24 h.
The E-test was performed according to the instructions of the manufacturer: strips (HiMedia, India) of amphotericin B, voriconazole and itraconazole containing concentration gradients of 32–0.002 µg/ml of the respective drug, were placed on Mueller-Hinton agar, and the plates incubated at 35 °C and read after 24h and 48h. The minimum inhibitory concentration (MIC), determined from the inhibition ellipse that intersected the scale on the strip, was read at the point of significant inhibition of fungal growth. Quality control was ensured by testing the following strains: Aspergillus flavus ATCC 204304 and Aspergillus fumigatus ATCC 204305. The interpretation of MICs for antifungal agents was carried out according the European Committee on Antimicrobial Susceptibility Testing Antifungal Susceptibility Testing Committee (EUCAST-AFST) document. 22
Venous blood was drawn before the administration of any drugs. Serum was separated from 5 mL for immediate testing or was stored at − 80°C for later testing. A commercial ELISA kit (Vector-Best, Russia) was used to detect Aspergillus IgG antibodies, and the experimental procedure followed the manufacturers’ instructions. The optical density (OD), measured at 450 nm, using a Humareader HS (Human Diagnostics Worldwide, Germany), gave an OD index (coefficient of positivity) calculated as the ratio of sample to kit cutoff or the critical OD, (COD) equal to half the sum of OD values of two negative control samples plus a correction factor of 0.3. COD = (OD-1 + OD-2)/2 + 0.3. OD index values of ≥1 were considered positive.
Results are expressed as the mean ± standard deviation (SD) for continuous variables and the percentage for categorical data. Data were analyzed by the odd ratio (OR), 95% confidence interval (CI) of the mean and Pearson Chi-square test for numerical variables. All statistical procedures were performed using Origin 8 software (OriginLab, Northampton, MA), and the level of statistical significance was set at p < 0.05.
Results
The baseline characteristics of study participants (n = 200) are illustrated in Table 1.
Baseline characteristics of PTB patients and the diagnostic criteria for CPA.

Note: ESR – erythrocyte sedimentation rate; total IgE – total immunoglobulin E;.
Data are presented as the number (percentage ± standard deviation) or mean ± standard deviation (minimum-maximum); *Significant difference between smear-positive and smear-negative PTB patients.
Aspergillus IgG-positive results were detected in 13.5% and 21.6% of smear-positive and smear-negative PTB patients, respectively (OR: 0.567; 95% CI: 0.259 to 1.240; P = 0.15). Cultures were positive in 22 PTB patients, and A. fumigatus was the most frequently isolated species (63.6%), followed by Aspergillus niger (22.7%) and A. flavus (13.6%). The prevalence of Aspergillus culture-positive patients was higher in the smear-negative PTB group (15.0%) than in the smear-positive PTB group (9.2%) (OR: 1.724; 95% CI: 0.694 to 4.282; P = 0.23). Although 32 PTB patients had detectable Aspergillus antibody levels, only 28 met the diagnostic criteria for CPA (Figure 1).

According to the criteria used in our study, 13 (6.5%) of 200 patients with PTB met the criteria for chronic cavitary pulmonary aspergillosis, 8 (4.0%) met the criteria for sub-acute invasive aspergillosis, 4 (2.0%) met the criteria for chronic fibrosing pulmonary aspergillosis and 3 (1.5%) met the criteria for single aspergilloma. Chronic cavitary pulmonary aspergillosis was the most frequent type of CPA among PTB patients (Figure 2).

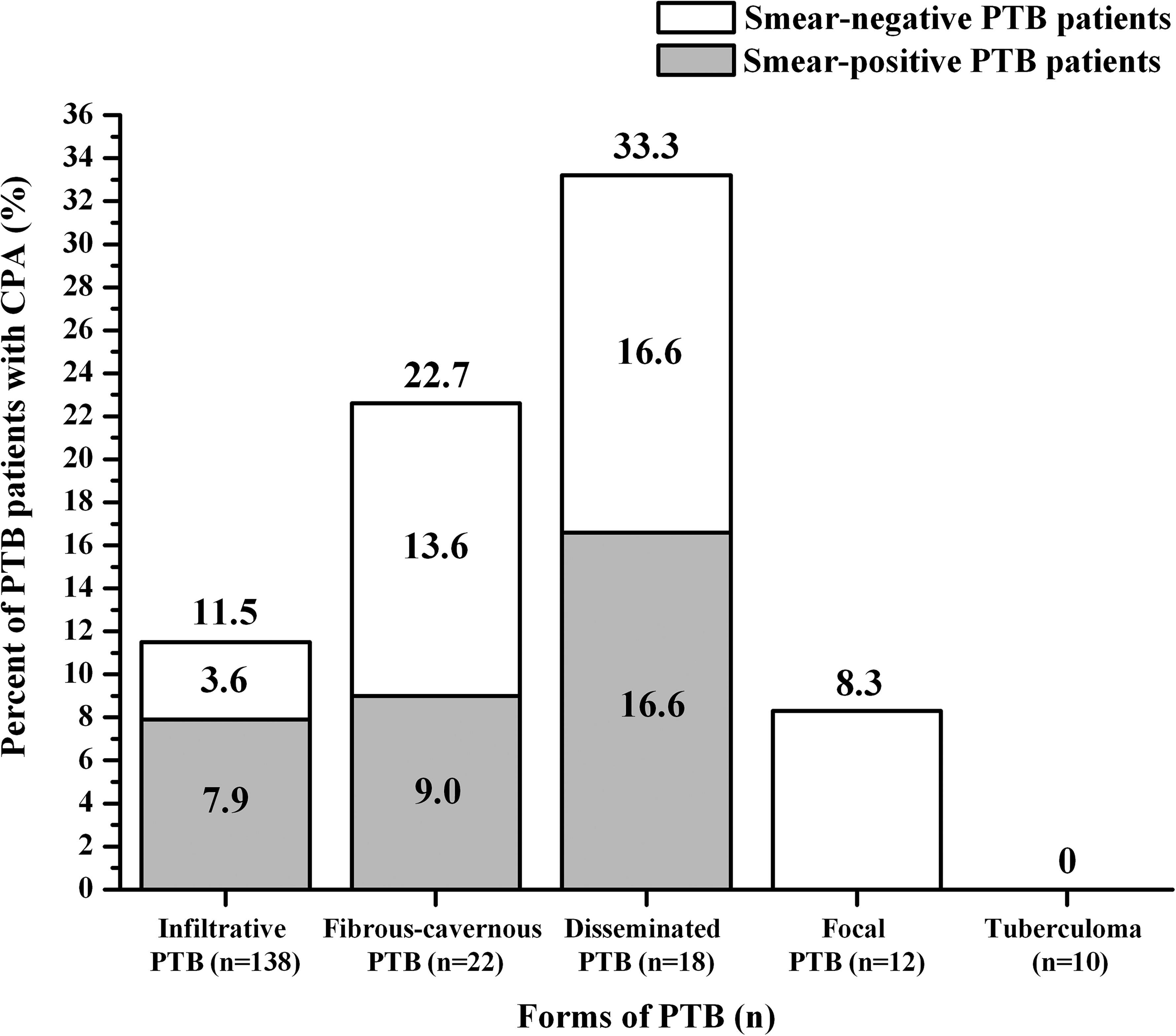
A high prevalence of CPA was detected in patients with the disseminated (33.3 ± 11.1%) and fibrous-cavernous (22.7 ± 8.9%) forms of PTB, whereas in patients with the infiltrative (11.5 ± 2.7%) and focal (8.3 ± 7.9%) forms of PTB, morbidity was low. In PTB patients with tuberculoma, CPA was not detected. Figure 3 demonstrates the CPA prevalence in smear-positive and smear-negative PTB patients.
We analysed the susceptibility of 22 isolates of Aspergillus to three main antifungal drugs. The results showed that the resistance rates of Aspergillus fumigatus to itraconazole and voriconazole were 7.1 and 14.2%, respectively (table 2).
Antifungal susceptibility of Aspergillus spp. isolated from PTB patient sputum.
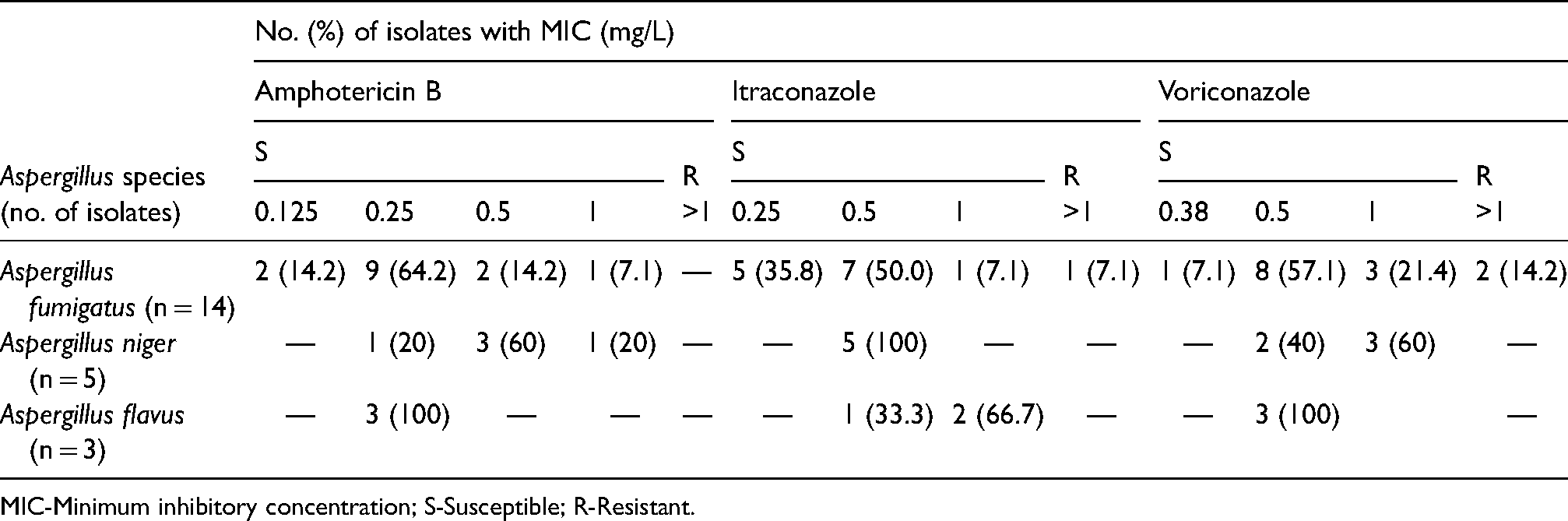
MIC-Minimum inhibitory concentration; S-Susceptible; R-Resistant.
Discussion
The morbidity and mortality of CPA remain high, especially in countries with a high burden of tuberculosis. Uzbekistan has seen a significant decline in the number of reported cases of PTB over the last 16 years (94/100K in 2003 to 49/100K in 2019).23,24 Despite this progress, the country is still amongst the 30 countries in the world with the highest multidrug resistant tuberculosis burden. 25 Furthermore, the situation is complicated by undiagnosed fungal infections among groups at risk as well as limited fungal diagnosis resources in Uzbekistan. 26 The official prevalence of CPA in Uzbekistan (6.3/100K) 26 is considerably less than in Kyrgyzstan (51.6), 27 Kazakhstan (35.5), 28 Tajikistan (46.8) 29 and Pakistan (39.0). 30 Most likely, the low figures in Uzbekistan are associated with underdiagnosis or poor reporting. Furthermore, accurate official data on the prevalence of CPA among PTB patients are not yet available for Uzbekistan. This is the first such study.
The serodiagnosis for Aspergillus IgG is not widely available in Uzbekistan. Epidemiological data on the resistance of Aspergillus spp. to antifungals in Central Asia are limited. Reports of triazole-resistance in Aspergillus spp. are increasing. 31 Itraconazole has a significantly lower cost than other antifungals. Amphotericin B was, however, the drug of choice and is still used against aspergillosis. It has excellent activity in vitro, but in clinical trials the survival rate was <60%.32–35 Underlying disease, immunosuppression, amphotericin B toxicity and antifungal therapy duration significantly affect the mortality in these infections.
Our study has limitations: the number of participants was less than anticipated, and we included only smear-positive and smear-negative PTB patients admitted to the clinic. Additionally, we could not carry out microbiological analysis and detection of antifungal susceptibility in all Aspergillus IgG-positive patients owing to the absence of sputum, as well as bronchoalveolar lavage, samples.
Conclusion
Our study confirmed a high prevalence of CPA in Uzbekistan, mostly in smear-negative PTB patients. Limited availability of Aspergillus IgG testing leads to diagnostic delay. Therefore, it is important to raise awareness not only in Uzbekistan, but wherever tuberculosis is endemic. Antifungal drug resistance also needs further intensive study.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.