
Abstract
Our study aims to ascertain the diagnostic value of the Monocyte-lymphocyte ratio (MLR) and red cell distribution width (RDW)-lymphocyte ratio (RLR) by comparing them with other biomarkers in distinguishing patients with and without acute appendicitis (AA). A total of 223 children were recruited in the study conducted according to the Cross-Sectional Study design. Patients under 18 years were assigned to 3 groups; AA, nonspecific abdominal pain (NAP), and a control group. According to the outcome of our research, while C-reactive protein (CRP), white blood cell (WBC), neutrophil count (NEU), neutrophil to lymphocyte ratio (NLR), and MLR had excellent diagnostic power, RLR had acceptable diagnostic power, and platelet to lymphocyte ratio (PLR) had only fair diagnostic power. MLR and NLR, which are simple, inexpensive, and easily accessible parameters, can be recommended to be used together with other biomarkers in diagnosing AA in children.
Introduction
Acute appendicitis (AA) is an important common cause of acute abdominal pain and accounts for most paediatric abdominal surgery emergencies.1,2 Particularly, limitations in taking a history from young children, non-compliance with the physical examination, inability to speak, and the inability of children to describe pain can make the diagnosis difficult. 3 Delays in diagnosis may result in peritonitis, localised or generalised. 4
We found only one study that studied MLR as a diagnostic tool for AA in children, 5 but none on the RLR. We compared them with other biomarkers in distinguishing patients with and without AA.
Material and methods
A total of 223 patients were enrolled between April 1, 2020, and April 1, 2022 in our cross-sectional study amongst children admitted to the emergency department with a complaint of abdominal pain. The study was approved by our Ethics Board, which waived the obligation to obtain informed consent (ethics committee decision number: 2022/3738 date: April 1, 2022). The research was carried according to the Helsinki Declaration.
Data were scanned retrospectively from our hospital information system. Patients under 18 were assigned to three groups AA, NAP, and a control group. The first included patients who underwent appendicectomy, with confirmed histopathological inflammartion of the appendix. Patients not so confirmed were excluded. The second were patients admitted for clinical observation for suspected appendicitis but recovered completely without the need for surgical intervention. The third group consisted of patients who were seen in the emergency department with non-inflammatory abdominal pain.
Pregnant patients, those with peripheral vascular disease, who suffered heart failure, had haematological or liver disease, who were using anticoagulants or steroids, had other acute or chronic infections, had a pathology result revealing a tumour, or whose records could not be accessed were all excluded.
An automated hematology analyzer (Sysmex Corporation, Kobe, Japan) was used to determine the full blood count (FBC). Haematological parameters total leucocyte count and differential, haemoglobin, haematocrit, platelet levels, RDW, NLR, neutrophil to monocyte ratio (NMR), platelet to monocyte ratio (PMR), platelet to lymphocyte (PLR), MLR, and RLR values were recorded. In addition, C-reactive protein (CRP) values were recorded, using a Mindray Chemistry Analyzer device (BS-2000M, China).
MLR and RLR were tested as predictors of AA and compared to other biomarkers.
Parametric tests were used without the normality test because of central limit theorem compatibility. 6 In the analysis of the data, the mean and standard deviation, minimum and maximum values of the variables were used while performing the statistics of the continuous data. Frequency and percentage values were used to identify the categorical data. One Way ANOVA test statistic compared the AA, NAP, and Control group means. Tukey statistic was used as a post hoc test to detect differences with the ANOVA test A Chi-square test was used to evaluate the relationship between AA, NAP, Control group, and gender. Receiver Operating Characteristic (ROC) analysis was used to determine the cut-off in diagnostic value measurements. Significance was found in the statistics of sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV). The area under the curve (AUC) of 0.5-0.6 was interpreted as poor, 0.6-0.7 as fair, 0.7-0.8 as acceptable, 0.8-0.9 as excellent, and > 0.9 as outstanding. ROC analyses of CRP, WBC, NEU, NLR, and MLR were evaluated with pairwise comparison of ROC curves and 95% confidence interval (CI). The degree of statistical significance of the data was established at p < 0.05. www.e-picos.com New York software and the MedCalc statistical package application were used to interpret the information.
Results
223 patients (AA: 70, NAP: 75, Control: 78) were enrolled. Table 1 shows gender, number and percentage, age, and mean and standard deviations of studied biomarkers. While there was no statistically significant relationship between the presence of AA and gender (p > 0.05), there was a substantial relationship between AA and age (p < 0.05).
Comparison of basic and laboratory characteristics of AA and NAP and control group.
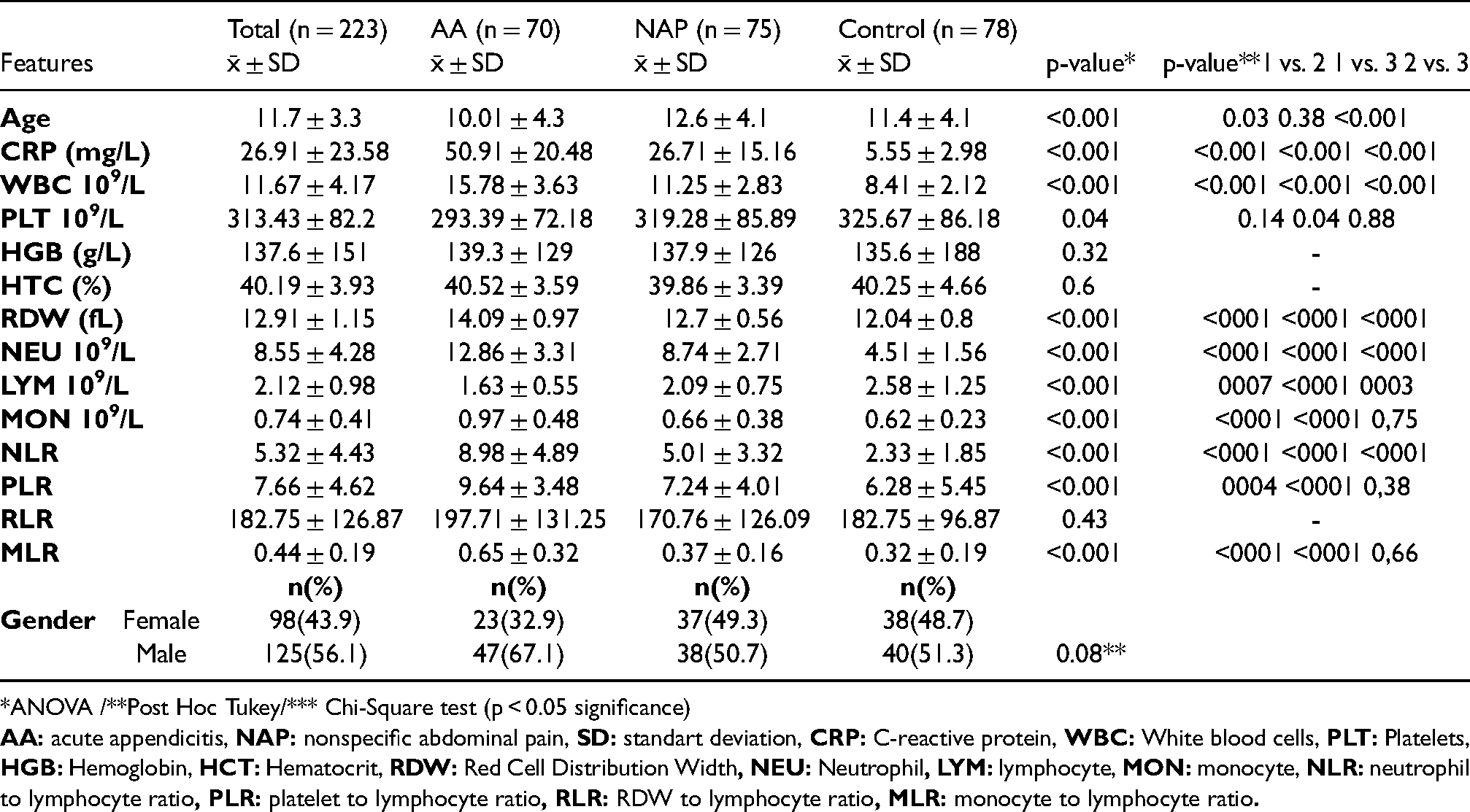
*ANOVA /**Post Hoc Tukey/*** Chi-Square test (p < 0.05 significance)
In
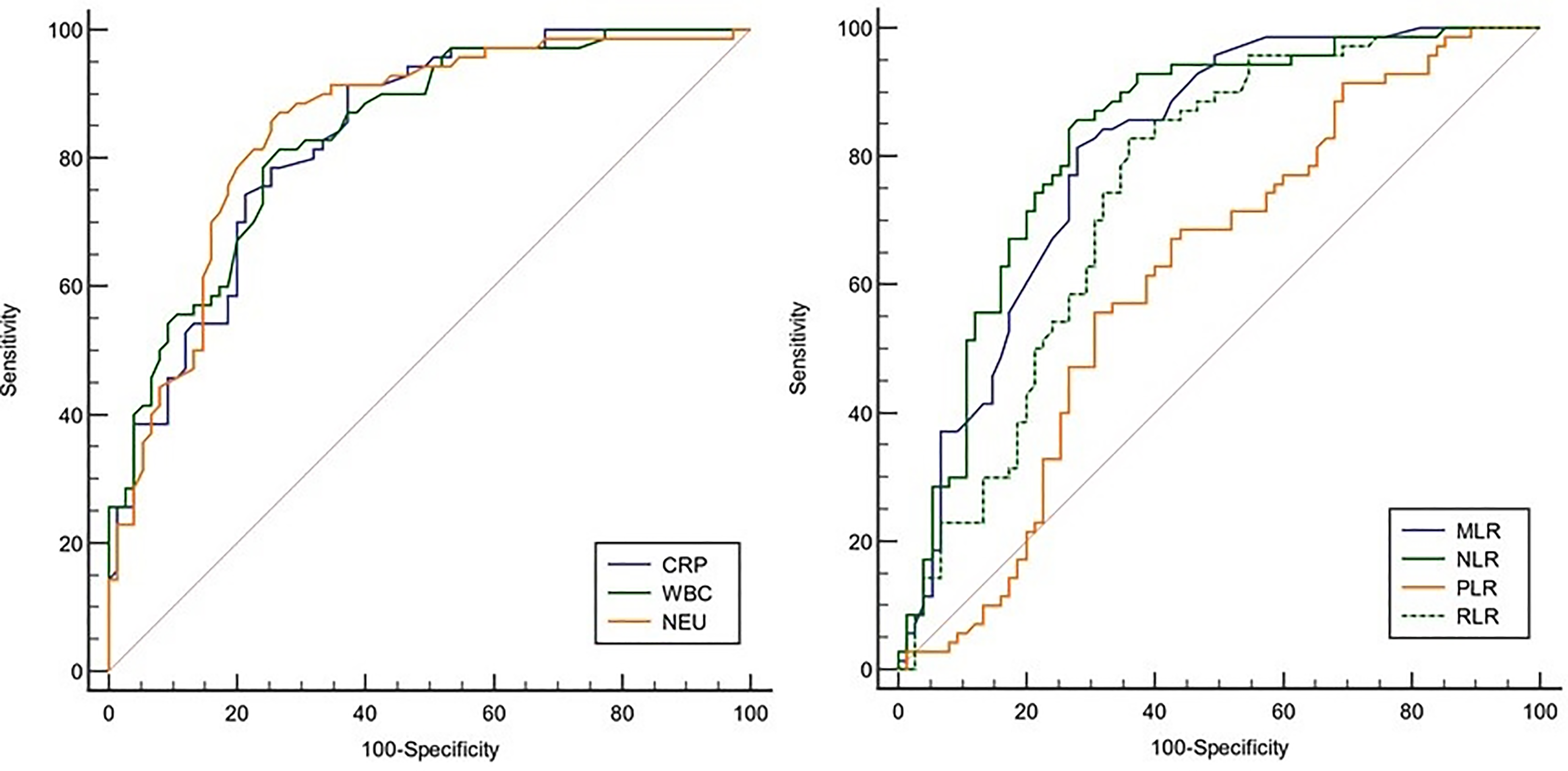
ROC curve of biomarkers for the diagnosis of acute appendicitis.
Diagnostic accuracy of inflammatory parameters for differentiation of AA from NAP.
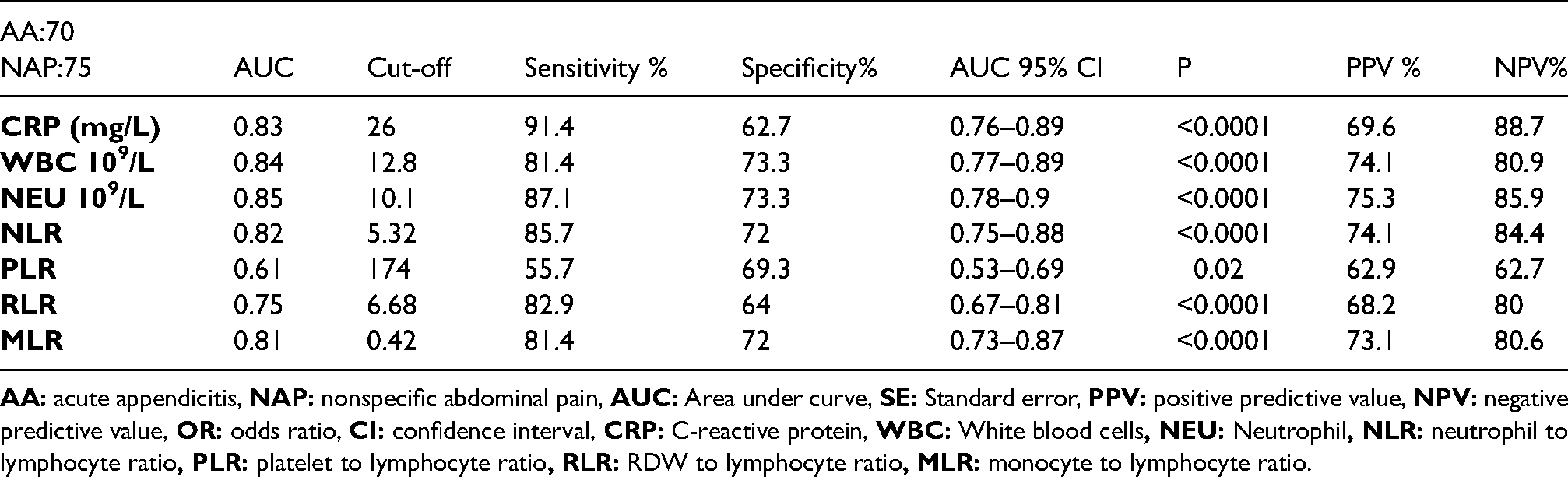
CRP, WBC, NEU, NLR, and MLR were found to have excellent diagnostic power in AA detection (AUC: 0.8-0.9). In detecting AA, RLR was of acceptable diagnostic power, while PLR was only of fair diagnostic power (AUC: 0.075, 0.61, respectively).
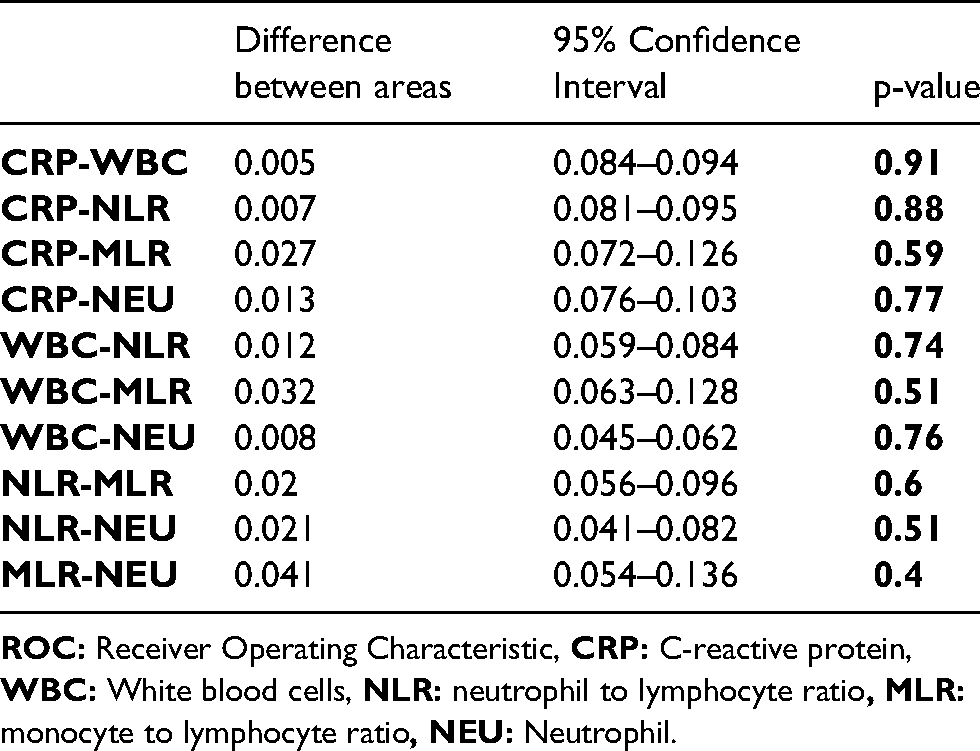
When the similarities of CRP, WBC, NEU, NLR, and MLR in the diagnosis of AA were evaluated by ROC curve comparison, no difference was found between AUC (p > 0.05). Therefore, it was determined that there were no statistical difference in diagnosing AA between these parameters
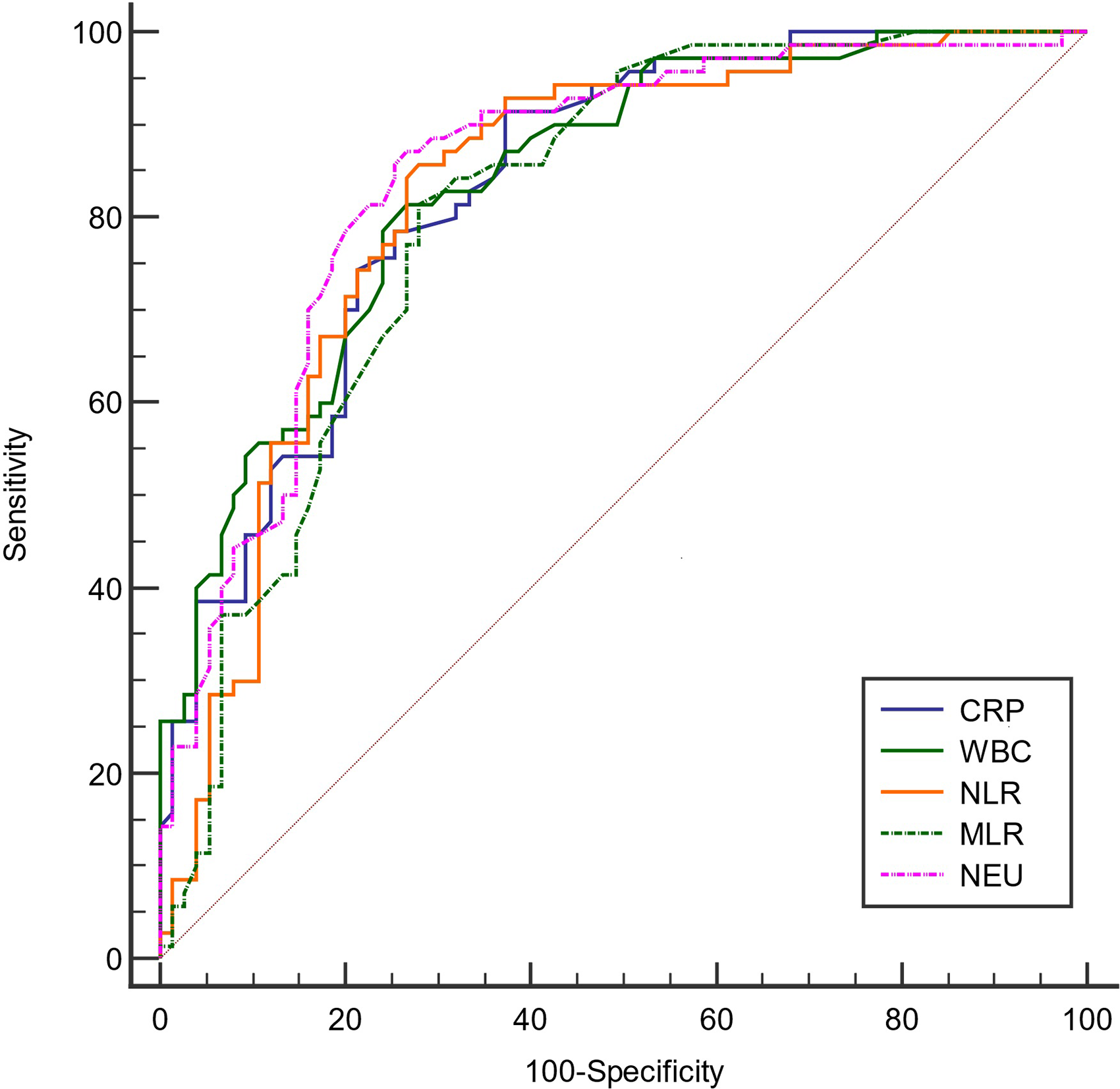
Pairwise comparison of ROC curves for CRP, WBC, NLR, MLR and NEU.
Pairwise comparison of ROC curves, difference between areas and 95% confidence interval.
Discussion
The rate of “negative” laparotomy, i.e., findings of a non-inflamed appendix clinically or histologically in patients with suspected AA is higher in children than in adults. 7
This has sparked a surge of interest in diagnostic tools for assessing AA. Ultrasound and computed tomography (CT) are two radiographic procedures recommended. 8 However, these are costly equipment and require a trained person for interpretation. Further, CT exposes children to undesirable radiation. Therefore, focus has grown on inexpensive, simple, and easy-to-apply inflammatory biomarkers.9,10 The standard tests used are leucocyte, neutrophil count (NEU), and CRP. 11 However, NLR, mean platelet volume (MPV), PLR and pro-adrenomedullin, have been shown to be useful in diagnosis.12–14 However, these biomarkers vary with the severity and duration of the inflammation, 15 and may be raised with non-surgical illnesses which may mimic appendicitis. 16
WBC is reported as having a sensitivity of 19–88% and specificity 53–100% in AA. 17 CRP is a non-specific inflammatory mediator, with a sensitivity of 48% and specificity 57%. 18
Neutrophilia and lymphocytopenia constitute the cell response to systemic inflammation. 19 An increase in the ratio (NLR) thus indicates the magnitude of the inflammatory response, and has excellent diagnostic accuracy in assisting a diagnosis of AA.
Monocytes represent the innate immediate immune system pre-programmed response, migrating into the tissues during infection to differentiate into macrophages and dendritic cells. 20 The primary cells that control the adaptive immune system are the lymphocytes. Thus MLR can differentiate AA and nonspecific abdominal pain (NAP) with a cut-off of 0.47 (sensitivity:75.98%, specificity:72.08%; AUC:0.798) in children, 5 and has excellent diagnostic accuracy. 21
RDW measures circulating erythrocyte size variation that is frequently recorded as part of a routine automated complete blood count. 22 RDW has been linked to rise in inflammatory markers such as CRP, interleukin-6, and erythrocyte sedimentation rate. Circulating inflammatory mediators suppress erythrocyte maturation. Therefore, larger reticulocytes in the circulation cause an increase in RDW. 23
RLR combines RDW and lymphocyte count, thus may improve its diagnostic value. We found it has an acceptable diagnostic power in diagnosing AA, but is not superior to NLR or MLR.
Platelets represent a crucial link between inflammation, thrombosis, and atherogenesis. 24 We found, however, that PLR had a lower diagnostic power.
Our study is a retrospective single-centre study. We used laboratory results from the initial application for analysis. We did not include follow-up values in the study. Since the time between the onset of symptoms and admission to the emergency department is not clear, it is not known at what stage of the inflammatory process laboratory parameters were analysed. However, since delay is likely to worsen symptoms of appendicitis, this is not a radical defect in our analysis. Therefore, although our results cannot be generalised, they can guide future studies for more reliable and precise results.
Conclusion
NLR and MLR, which are simple, inexpensive, and easily accessible parameters, can be recommended to be used together with other clinical signs in diagnosing AA in children. RLR is acceptable but not superior.
Footnotes
Acknowledgments
We thank biostatistics expert Elif Ertaş for her support for the statistical analysis of the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.