
Abstract
Our study was done to identify patient or health system related delay in diagnosis of treatment naïve sputum positive PTB patients and its impact on sputum conversion at 2 months. A total of 280 patients were enrolled and followed up for 2 months following which repeat sputum examination was done. Detailed clinical history was taken with emphasis on duration of symptoms, day of presentation, diagnosis and starting of therapy. The median(range) of delay in treatment initiation was 15 (0–82) days, most commonly because of delay due to the health system. Patients with positive sputum at the end of two months had significantly higher delay in treatment initiation (p < 0.05). Being remote (>5 km) from a health provider, being an unskilled labourer, and visiting a private practitioner were associated with delay in diagnosis. Eradication of tuberculosis in India requires training of health professionals, intersectoral cooperation and better public outreach.
Introduction
Globally, an estimated 10 million people developed active TB disease in 2019, with 1.4 million succumbing. More than a quarter (26%) of these patients are in India. 1 Out of these estimated 10 million, only 7.1 million were identified and reported to national TB programs around the world. 1 The 2.9 million missing people include those who were diagnosed with TB, but were not reported to public health authorities, (including those not reported from the private sector) and those who were not diagnosed and therefore not treated. 1
Coupled with this under-reporting of active cases is another malady that plagues the TB programme in India; this is the delay in presentation, diagnosis and initation of antitubercular treatment (ATT). A single person with infectious TB may infect 10–15 others in a year; therefore, early detection of infectious cases, followed by effective treatment, is imperative for a successful control of tuberculosis. 2 Delay in diagnosis not only causes spread of infection in the community, but increases patient expenditure, and is associated with a higher risk of mortality. 2 Several studies have looked at delays,3–6 but most of these are retrospective and do not examine the associated risk factors, nor subsequent detrimental treatment outcome.
Sputum conversion rates at the end of intensive phase of ATT is an important marker of success, and reduces the risk of Multi drug resistant (MDR) tuberculosis. Early sputum conversion also leads to decreased community transmission and brings down disease burden.
Materials
Our prospective observational study was carried out over a period of one year from 1st July 2016 to 30th June 2017. All treatment-naïve patients of PTB who attended our institute and were found to be smear positive were included in the study. Retreatment cases, patients with extrapulmonary tuberculosis, and suspected or diagnosed cases of MDR tuberculosis were excluded. We obtained approval from our Institutional Human Ethics Committee. An informed, written consent was obtained from all the patients.
Methods
Considering a possible delay in treatment delay of 35%, 4 95% confidence interval and 10% absolute precision, the minimum sample size calculated was 89.
Study subjects were enrolled and proforma were filled by personal interview. After a detailed history and physical examination, reports of sputum microscopy and chest radiography were recorded. Socio-economic status was assessed with the help of modified Kuppuswamy scale. 7 After 2 month follow up, reports were recorded. (Figure 1)
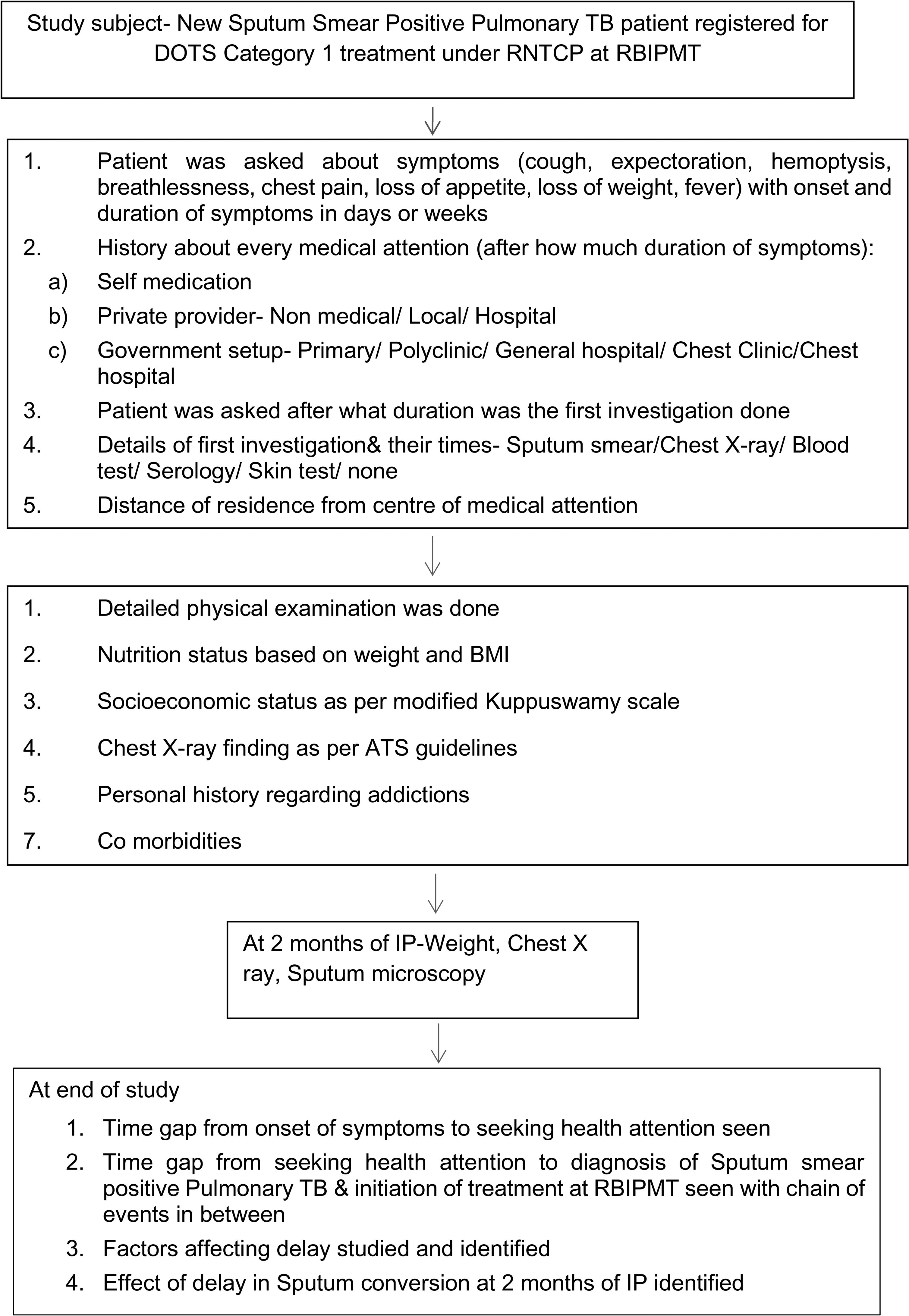
Flow chart and methodology of study.
We used the following definitions: ‘patient delay’ as reaching any health care provider after 15 days or more of symptoms; ‘delay in diagnosis’ as being diagnosed by sputum smear for AFB after 7 days of reaching the health system; ‘Delay in initiation of treatment’ as being started on ATT after 7 days of being diagnosed by sputum for AFB; ‘Delay due to health system’ as the sum of the latter three.
Statistical testing was conducted with SPSS 17.0 and MS excel 2007. Descriptive statistics were analysed with SPSS version 17.0 software. As appropriate, Chi square and Student t-test were used to fulfil the objective of study. For all statistical tests, a p value < 0.05 was taken to indicate a significant difference.
Results
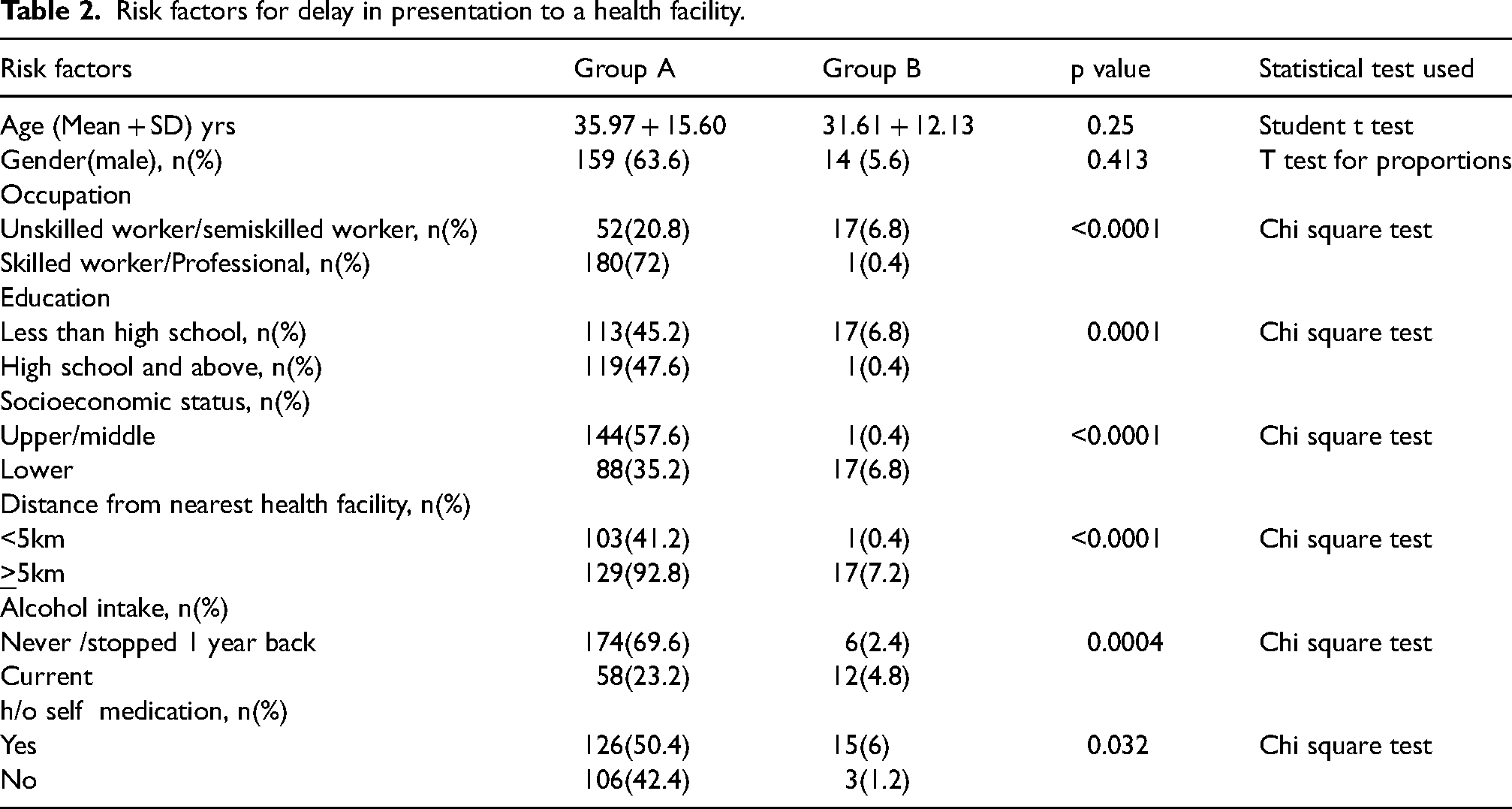
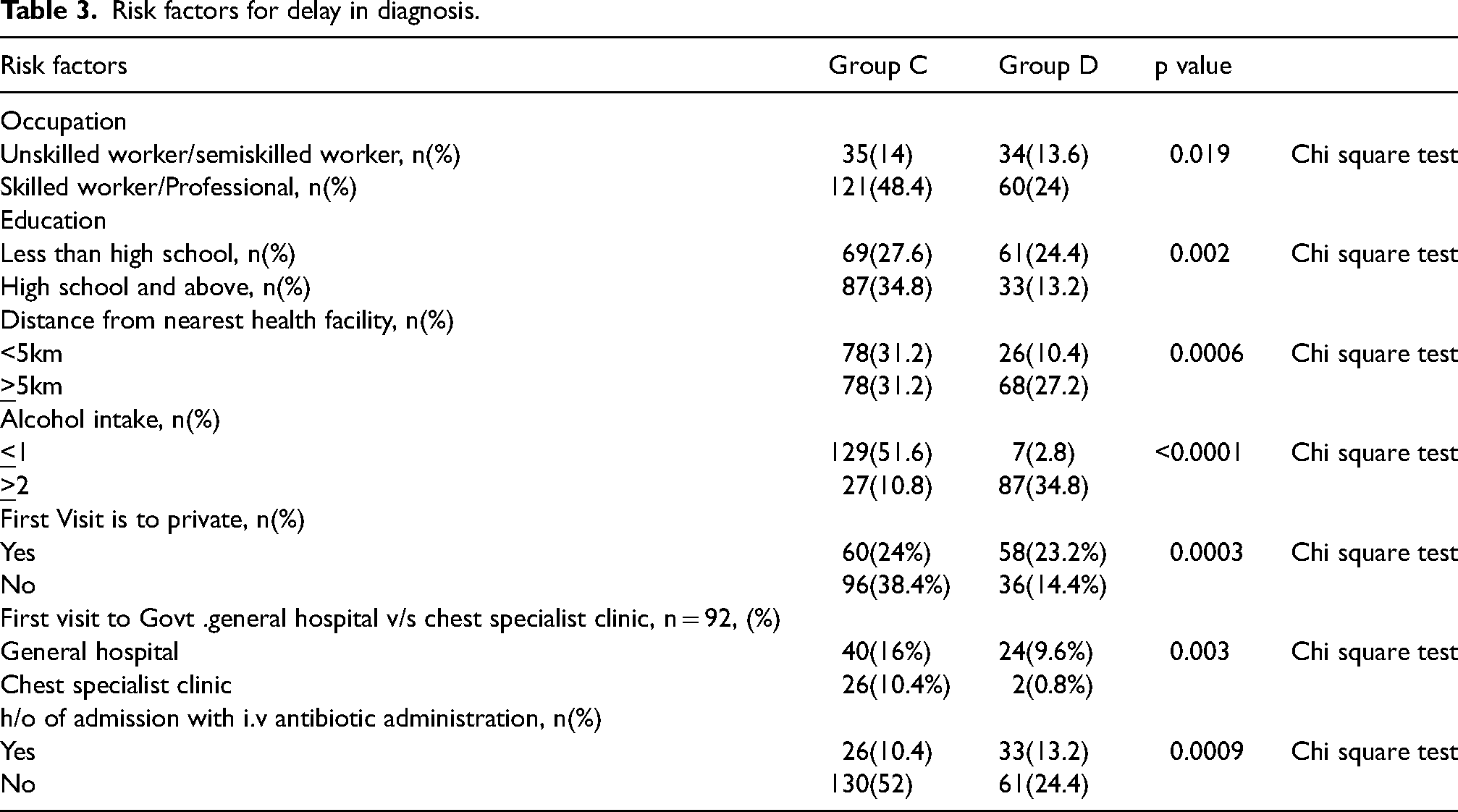
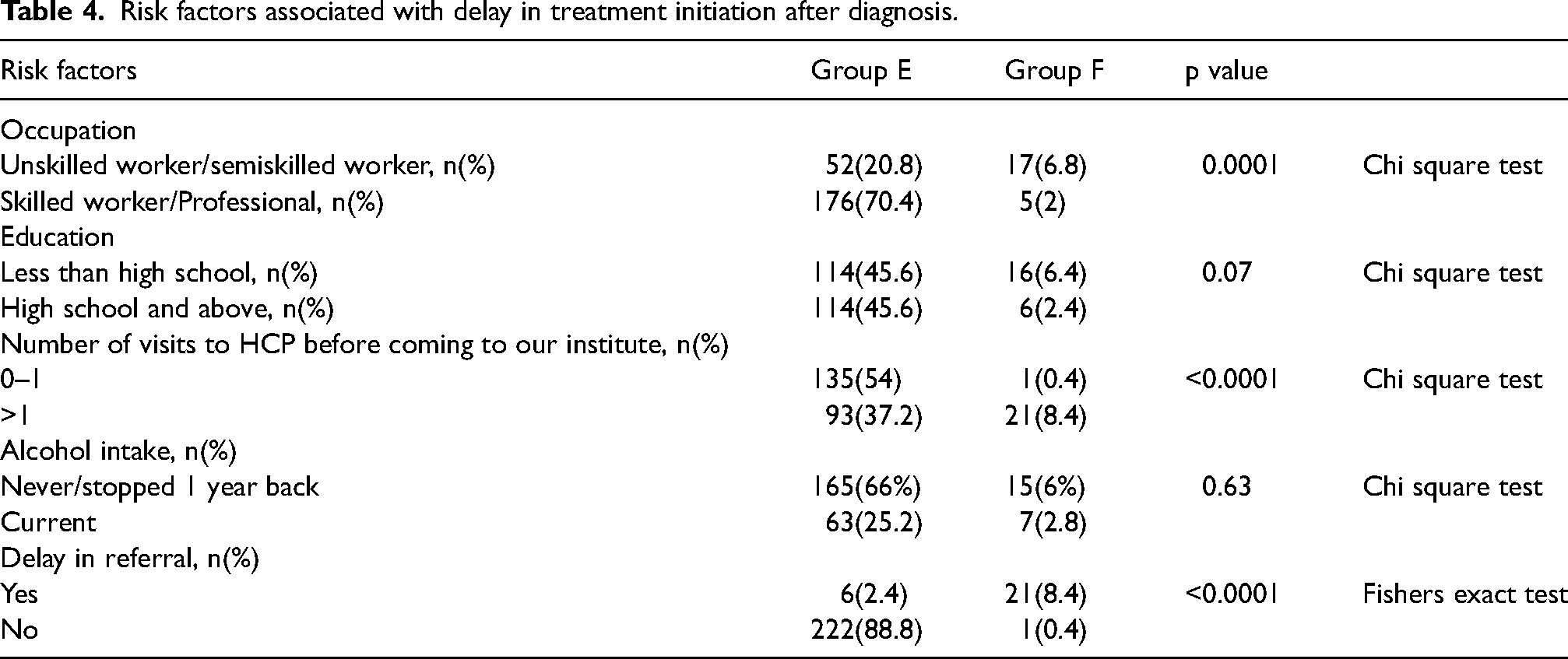
Some 280 new sputum smear positive PTB patients were enrolled, of whom 250 completed the study and were included. The following groups were identified based upon the definitions of delay:First health care seeking delay (patient delay):Group A- Presenting to any health care provider (HCP) by 15 days of symptoms, seen in 232(92.8%) subjects .Group B (first health care-seeking delay/ patient delay)- Presenting to any health care provider(HCP) after more than 15 days of symptoms ,seen un 18(7.2%) subjects. Diagnostic delay-Group C- Patient diagnosed as PTB by sputum smear for AFB within 7 days of presenting to a health care provider = 156 (62.4%) subjects, Group D (patients with diagnostic delay) - Patient diagnosed as PTB by sputum smear for AFB after greater than 7 days of presenting to a health care provider = 94(37.6%) subjects.Treatment initiation delay-Group E- Patient being initiated on ATT within 7 days of diagnosis by sputum smear for AFB = 228(91.2%) subjects, Group F (patients with delay in treatment initiation) - Patient being initiated on ATT after greater than 7 days of diagnosis by sputum smear for AFB = 22 (8.8%) subjects.
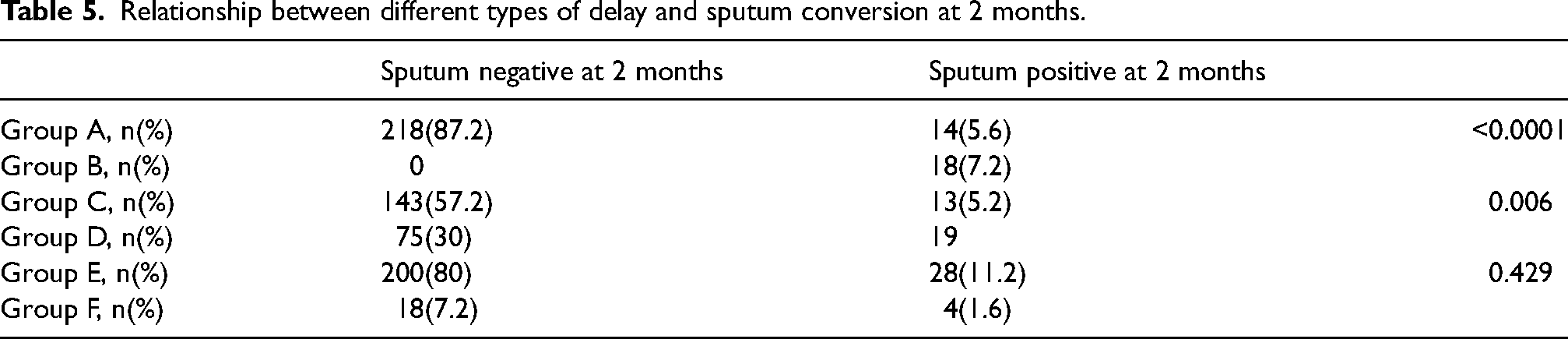
Various delays, as defined, are detailed in Tables 1–4, with significant associations. Out of our 250 patients, 236 (94.4%) had visited at least one other HCP before coming to our institute, having investigations such as chest radiographs (220, 93.2%), Mantoux test (35,1%) and serological tests such as TB-GOLD and Quantiferon GOLD (30,1%). Sputum for AFB ZN stain were done in only 43 (17.2%). We found that 27 (10.8%) had suffered delay in referral to their home area. Patients who were smear positive at 2months had significant delay(p < 0.0001) in mean duration of initiation of anti-tubercular treatment from onset of symptoms (43.59 + 29.94 days) compared to patients who were smear negative at 2 months (11.72 + 4.76 days). Table 5 shows association of the various forms of delay and sputum conversion rates at end of two months of Intensive phase of antitubercular treatment. Out of the 43 patients who underwent sputum for AFB ZN stain before coming to our institute, we found that all of them underwent sputum testing only once, instead of twice as recommended. Some 25 (58.1%) had positive sputum samples.
Type of delays and their duration.

Risk factors for delay in presentation to a health facility.
Risk factors for delay in diagnosis.
Risk factors associated with delay in treatment initiation after diagnosis.
Relationship between different types of delay and sputum conversion at 2 months.
Discussion
As long as a patient has not completed 2–3 weeks of ATT, the bacillary load will not reach a level deemed non-infectious.8,9 Low socio-economic class, 10 long hours of work 11 and rural residence 12 have been associated with treatment delays, but we ascertained that a first visit to a private practitioner or a heath facility was associated with prolonging the diagnostic delay. The use especially of quinolones, simply prolonged patient delay exposing patients to develop drug resistant 13 Avoiding prescription of expensive tests, uncertainty about the presentation of TB, 14 and lack of awareness or uncertainty about the accuracy of available TB tests may be responsible. 1 5
Table 5 showed that delay in presentation and diagnosis were significantly associated with sputum non conversion at the end of Intensive phase of 2 months. We believe that this is due to the higher bacillary load and greater morbidity of the patients associated with these delays.
The fact that 25 patients had positive sputum samples and still attended another health facility, namely ours, suggests a social stigma associated with being diagnosed with TB and a non-acceptance linked with it. These 25 patients also had late initiation of ATT, showing that even after diagnosis by two separate health facilitiesre remained resistance in attending a TB health centre to start ATT. At its root is a systemic failure to properly educate and motivate patients. Onward referral in our national programme evidently, from our data, needs streamlining.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.