
Abstract
Multidrug-resistant (MDR) Acinetobacter baumannii has become a major concern of hospital care. The objective of the study was to evaluate the evolution of antimicrobial resistance of A. baumannii in a Peruvian hospital from 2013 to 2019. A total of 993 A. baumannii clinical isolates were recovered. Antimicrobial resistance levels were extremely high, except for colistin. Among the remaining antibacterial agents, ampicillin plus sulbactam (AMS) was the most active (71.4% of resistance), with resistance levels to the remaining agents ranging from 75.9% to amikacin to 99.2% to ertapenem. The presence of significant differences was observed in extensively drug-resistant (XDR) A. baumannii according to samples origin. No association was observed between MDR or XDR isolates and seasonality. An impressive rate of XDR A. baumannii isolates was found, including a growing number of only-colistin-susceptible isolates highlighting the urgent need for new therapeutic alternatives.
Introduction
The genus Acinetobacter accounts for 65 species with standard nomenclature and an undetermined number of non-validated or Candidatus species. Acinetobacter is a ubiquitous genus, which inhabits soils and aquatic environments and may also be found as a member of the human or animal microbiome. It is also frequently recovered from food samples of either animal or vegetal origin.1,2
Several Acinetobacter species are able to produce infections in both humans and animals.1,3 Among these, except for Acinetobacter calcoaceticus, which is a less common cause of human infection, the species grouped in the so-called A. calcoaceticus–-Acinetobacter baumannii complex, including A. baummanni and A. lactucae (also known as dijkshoorniae), A. nosocomialis (formerly genospecies 13), A.pittii (former genospecies 3) and A.seifertii (also known as RUH 1139), rank among the most common species reported at the clinical level.1,4–9
Undoubtably, A. baumannii is the most relevant clinical species. It is one of the most common microorganisms causing nosocomial infections,1,5,6 and usually presents high levels of resistance to antimicrobial agents, which strongly hinder efficient and timely treatment.6,10 In fact, the presence of pan-resistant A. baumannii clinical isolates is now being described worldwide.11,12 Thus, this microbe makes a severe impact especially in sensitive hospital zones, such as intensive care units (ICUs). Here, fragile patient status, the presence of comorbidity and the frequency of invasive procedures make its invasion particularly hazardous; in turn, these infections result in longer hospitalisation, higher economic costs and, more importantly, increasing patient mortality, rising to 70% for A. baumannii-induced ventilator-associated pneumonia. 10 This organism is now considered a major threat and has been classified, together with Enterococcus faecium, Staphylococcus aureus, Klebsiella pneumoniae, Pseudomonas aeruginosa and Enterobacter spp., as a member of the so-called ESKAPE group. 13
Reports in Peru are scarce, but multidrug-resistant (MDR) and extensively drug-resistant (XDR) A. baumannii isolates are frequently isolated, and antibiotic resistance reaches 97.5% to carbapenems, >90% to third and fourth-generation cephalosporins, piperacillin–tazobactam (PTZ) or fluoroquinolones and >60% to ampicillin–sulbactam (AMS), aminoglycosides, cotrimoxazole and tetracyclines, among others.5,6,14 Recently, reports of 100% resistance to several antibacterial agents has been published. 15 Furthermore, colistin-resistant A. baumannii isolates has been observed.5,6
We aimed retrospectively to evaluate the levels, evolution and seasonality of antimicrobial resistance in A. baumannii clinical isolates recovered during the period from 2013 to 2019 in a level III Peruvian hospital.
Materials and methods
The Hospital Nacional Arzobispo Loayza (HNAL) is a tertiary level hospital in Lima, with 806 beds (in 2014), 26 of which are ICU beds.
All A. baumannii isolates recovered between January 2013 and December 2019 were included in the study. Samples were cultured in selective media, with the exception of blood and cerebrospinal fluid (CSF), which were processed using BACTEC 9240 (Becton-Dickinson, Franklin Lanes, NJ, USA). Identification was done by an automated system (Vitek, Biomerieux, Marcy l’Etoile, France). When more than one isolate was recovered from a patient, only the first recovered was considered.
The following data were extracted from internal databases: sample type, including abdominal, blood, CSF, respiratory, urine, wounds and others; wards categorised as outpatient (ambulatory and emergency), inpatient (critical, including ICUs and special care units, hospitalisation, including internal medicine wards, and surgery), and other wards (including paediatrics and neonatology).
Antimicrobial susceptibility to ceftazidime, ceftriaxone, cefepime, AMS, PTZ, aztreonam, ciprofloxacin, levofloxacin, norfloxacin, amikacin, gentamicin, imipenem, meropenem, ertapenem, cotrimoxazole and colistin was established using the Vitek system. Standard classification and definitions were followed to classify antibiotic families and to define MDR and XDR 16 Aztreonam, norfloxacin and ertapenem were not considered for MDR or XDR determination. Moderately resistant (MR) isolates were defined as non-susceptibility to at least one antibacterial agent of one or two antimicrobial categories. 17
Categorical variables were presented as absolute numbers and their relative frequencies. The presence of statistically significant differences was established using the Fisher’s exact test. Bivariate analysis was performed between the outcome variable and the covariates of interest using the chi-square test. STATA 16.2 was used for the analysis. The results are reported according to their 95% confidence intervals
Results
A total of 993 non-duplicated A. baumannii clinical isolates were recovered, with the highest number (204) from 2016. Of the total, 506 (51.0%) were recovered from respiratory samples, 198 (19.9%) and 168 (16.9%) from urine and blood, respectively, 64 (6.4%) from wounds, 14 from CSF and 17 from abdominal secretions.
Sites of collection are shown in Table 1.
Characteristics of the isolates studied.
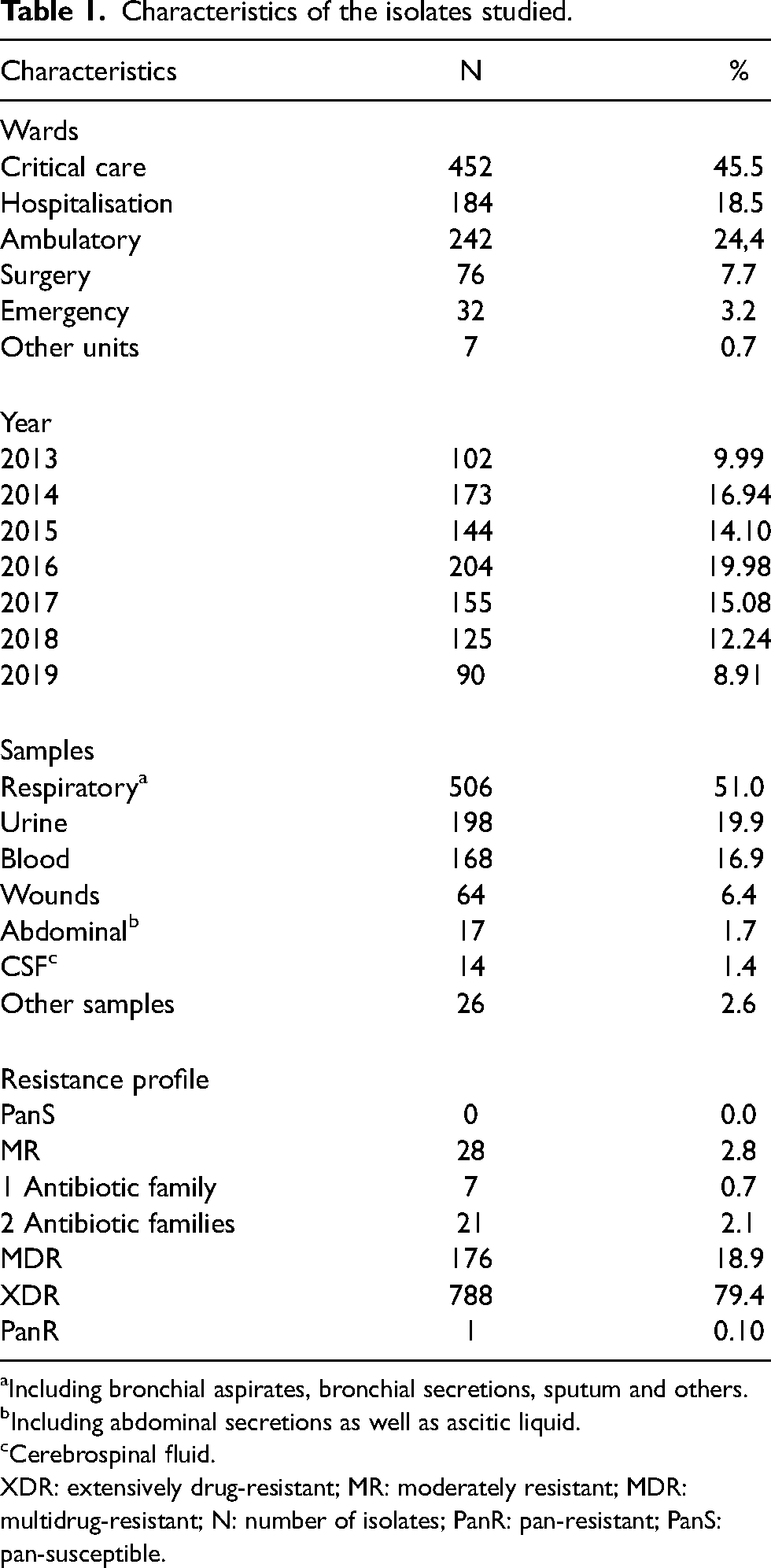
Including bronchial aspirates, bronchial secretions, sputum and others.
Including abdominal secretions as well as ascitic liquid.
Cerebrospinal fluid.
XDR: extensively drug-resistant; MR: moderately resistant; MDR: multidrug-resistant; N: number of isolates; PanR: pan-resistant; PanS: pan-susceptible.
The source differed among wards. In the outpatient setting, urine infections were more frequent among ambulatory patients (p = 0.012), while among inpatients, respiratory (p < 0.001) and blood (p = 0.030) infections were more frequent in critical patients, and urine (p < 0.001), wounds (p < 0.001), abdominal (p = 0.036) and other infections (p = 0.002) were more frequent among hospitalised and surgical patients.
When inpatients and outpatients were analysed as a whole, A. baumannii urine infections were significantly (p < 0.001) more frequent among outpatients (41.8%), and A. baumannii respiratory and blood infections were most frequent among inpatients (p = 0.010 and p < 0.001, respectively) (Table 2). Of note, despite the above-mentioned significant differences, respiratory infections were the most common source of A. baumannii infection among outpatients (44.5%).
Types of infections by Acinetobacter baumannii in outpatients and inpatients.
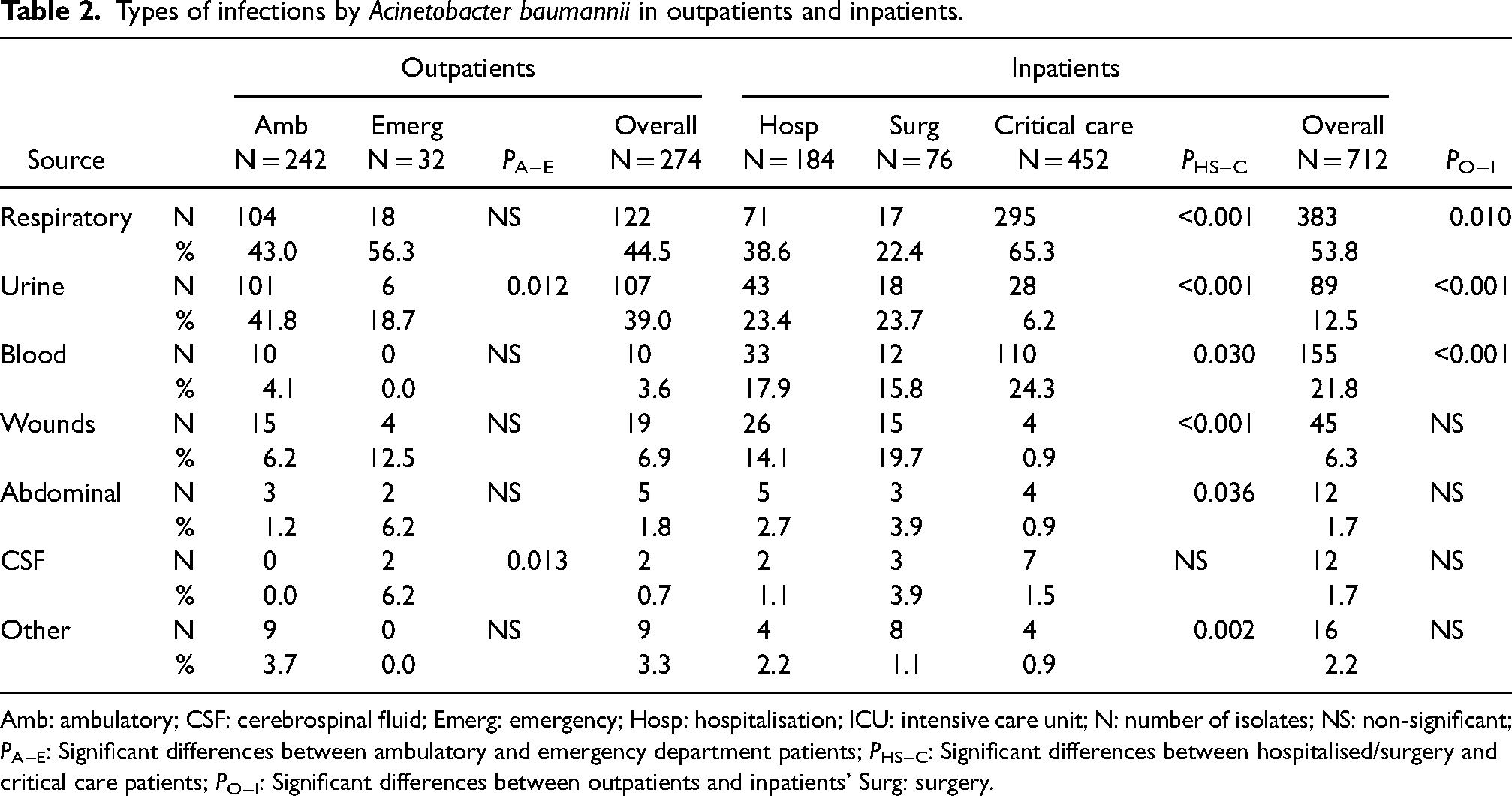
Amb: ambulatory; CSF: cerebrospinal fluid; Emerg: emergency; Hosp: hospitalisation; ICU: intensive care unit; N: number of isolates; NS: non-significant; PA−E: Significant differences between ambulatory and emergency department patients; PHS−C: Significant differences between hospitalised/surgery and critical care patients; PO−I: Significant differences between outpatients and inpatients’ Surg: surgery.
The antimicrobial resistance levels were extremely high, though colistin resistance was found only in two, both being recovered from respiratory samples in critical patients in 2013, with one being susceptible to aminoglycosides as well as ciprofloxacin (but not to levofloxacin). AMS showed greatest activity at 71.4% of resistance. Resistance to the remaining agents ranged between 75.9% to amikacin to 99.2% to ertapenem (Table 3).
Antimicrobial resistance levels in the period from 2013 to 2019.
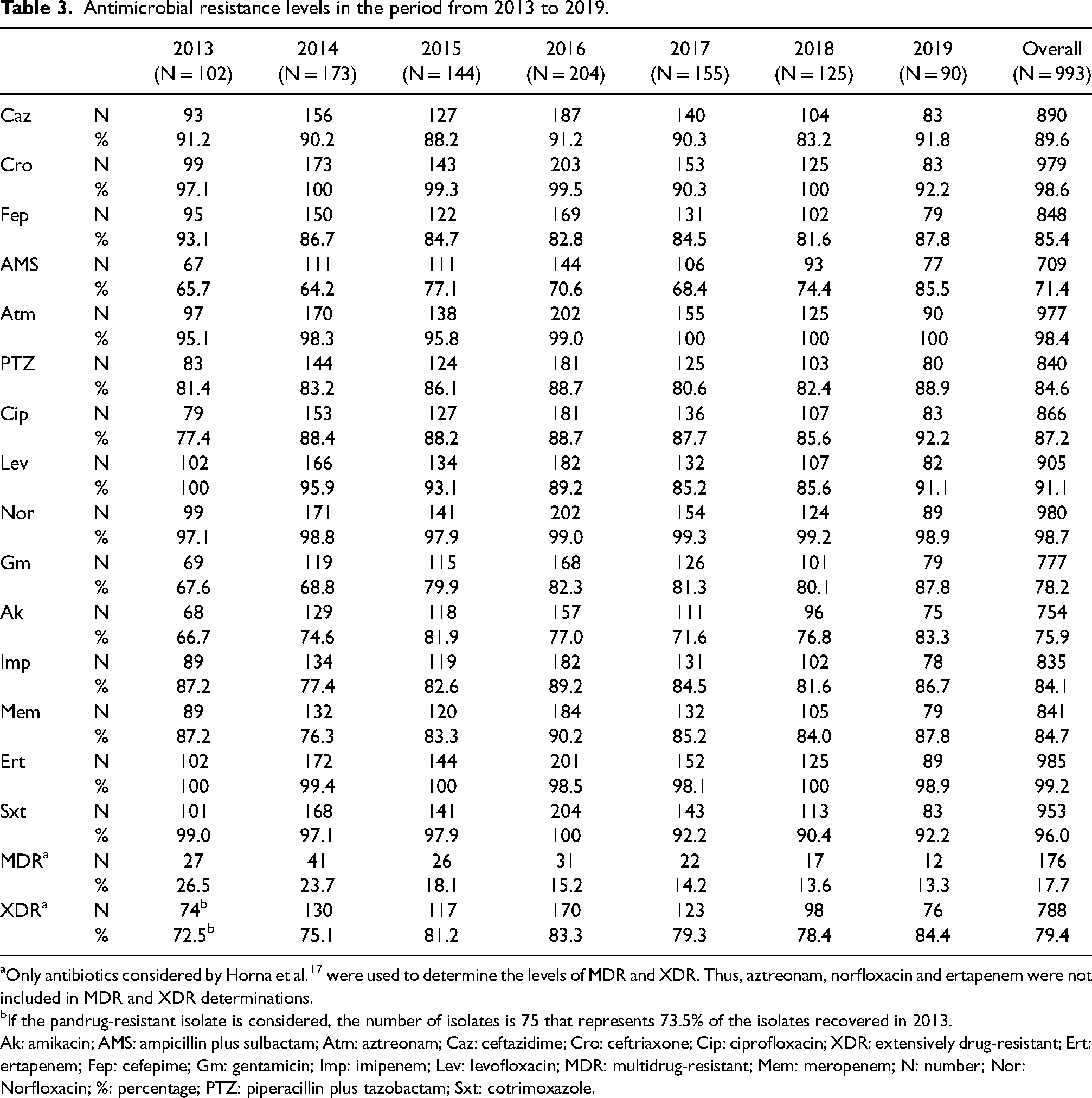
Only antibiotics considered by Horna et al. 17 were used to determine the levels of MDR and XDR. Thus, aztreonam, norfloxacin and ertapenem were not included in MDR and XDR determinations.
If the pandrug-resistant isolate is considered, the number of isolates is 75 that represents 73.5% of the isolates recovered in 2013.
Ak: amikacin; AMS: ampicillin plus sulbactam; Atm: aztreonam; Caz: ceftazidime; Cro: ceftriaxone; Cip: ciprofloxacin; XDR: extensively drug-resistant; Ert: ertapenem; Fep: cefepime; Gm: gentamicin; Imp: imipenem; Lev: levofloxacin; MDR: multidrug-resistant; Mem: meropenem; N: number; Nor: Norfloxacin; %: percentage; PTZ: piperacillin plus tazobactam; Sxt: cotrimoxazole.
Specific antibacterial agent family resistance showed highest levels in extended spectrum cephalosporins (100%), mostly related to high levels of resistance to ceftriaxone (98.6%). Similarly, extremely high levels of resistance to other agents, such as 99.6% to fluoroquinolones (excluding norfloxacin) and 99.6% carbapenems (excluding ertapenem), were observed (Table 3).
A total of 788 (79.4%) isolates were classified as XDR, with 498 (63.2% of XDR isolates; 53.4% of total isolates) only showing susceptibility to colistin (Table 3). In addition, 176 (17.7%) isolates were MDR, and 1 isolate was potentially pan-resistant. The number of isolates presenting resistance to one or two families of antibacterial agents was 7 and 21, respectively. No isolate was pan-susceptible.
High levels of antibiotic resistance were present in A. baumannii from both in- and outpatients. Resistance to AMS and ceftriaxone was always significantly higher among in- than outpatients, ranging from 64.6% and 74.0% to 98.9% and 99.4% in outpatients and inpatients, respectively (Table 4).
Evolution of antibiotic resistance in Acinetobacter baumannii causing infections in outpatients and inpatients.
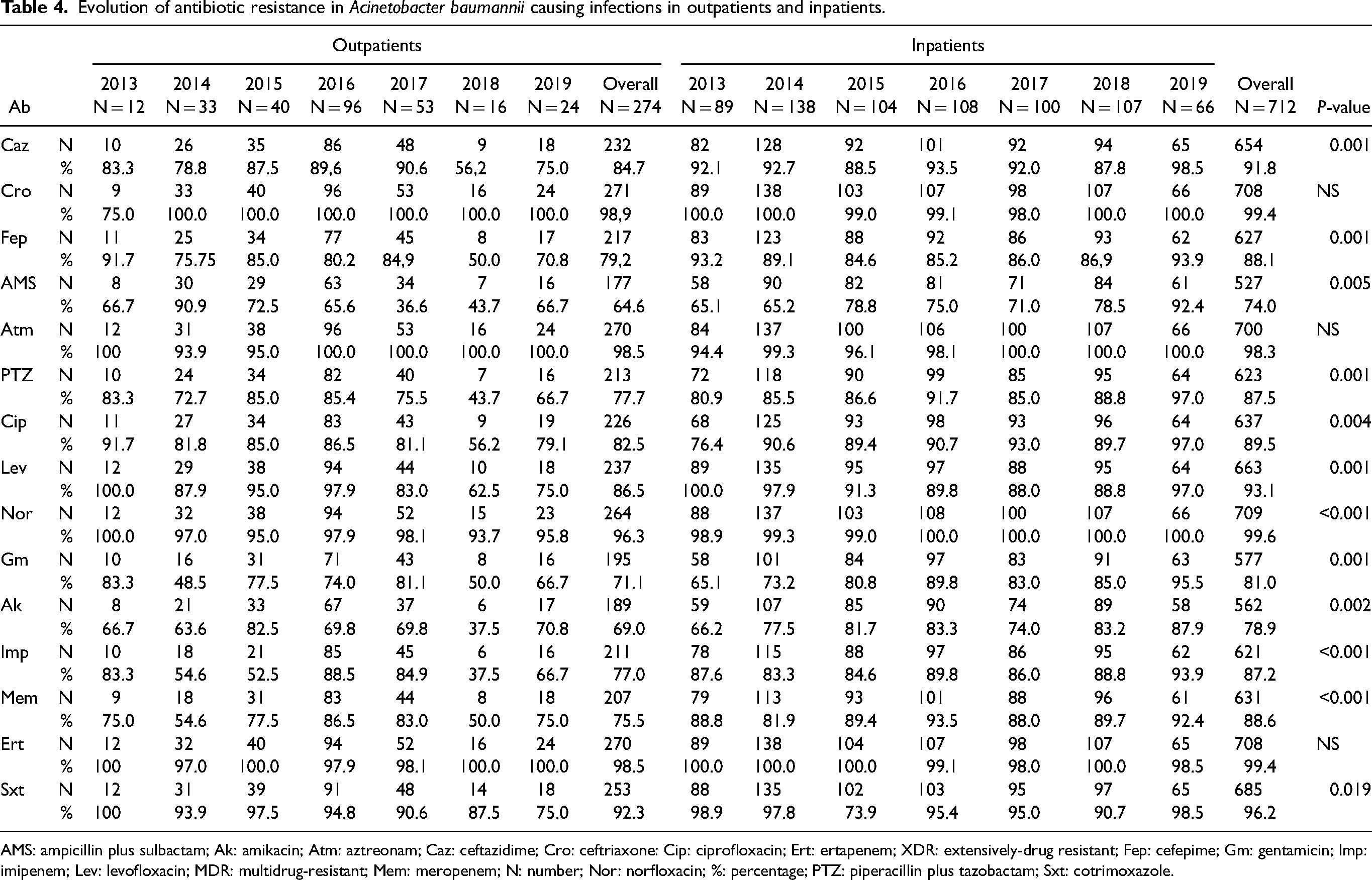
AMS: ampicillin plus sulbactam; Ak: amikacin; Atm: aztreonam; Caz: ceftazidime; Cro: ceftriaxone: Cip: ciprofloxacin; Ert: ertapenem; XDR: extensively-drug resistant; Fep: cefepime; Gm: gentamicin; Imp: imipenem; Lev: levofloxacin; MDR: multidrug-resistant; Mem: meropenem; N: number; Nor: norfloxacin; %: percentage; PTZ: piperacillin plus tazobactam; Sxt: cotrimoxazole.
XDR was more frequent from respiratory (83.7%) and wound (82.7%) samples. Similarly, isolates from hospital and critical care wards presented significantly high levels, with the only pan-resistant isolate being recovered from a critical respiratory patient. No association was observed between MDR/XDR isolates and seasons, with spring and summer having the highest number of isolates and autumn the highest proportion of XDR isolates (82.5%) (Table 5).
Antimicrobial resistance and origin of the samples.
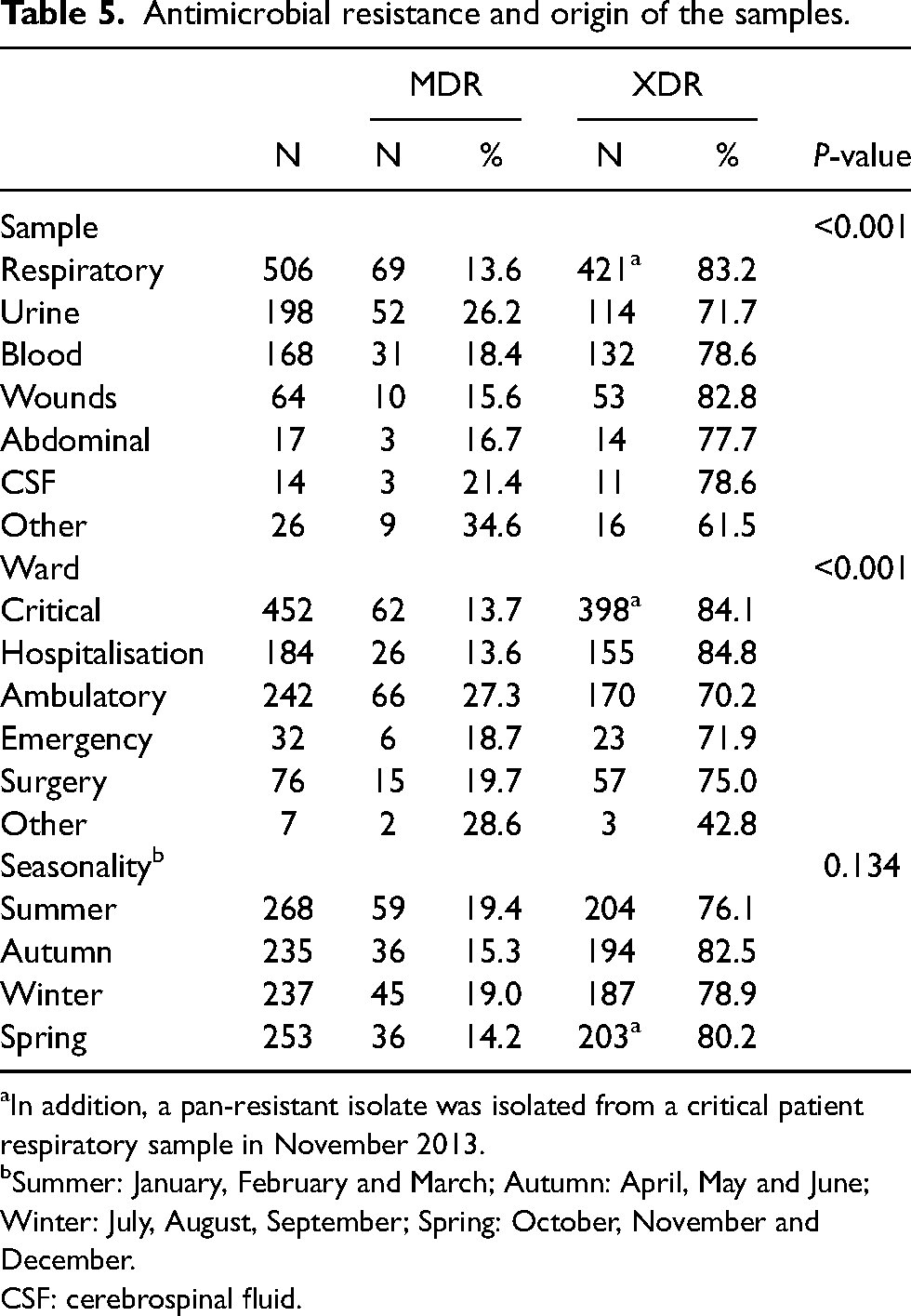
In addition, a pan-resistant isolate was isolated from a critical patient respiratory sample in November 2013.
Summer: January, February and March; Autumn: April, May and June; Winter: July, August, September; Spring: October, November and December.
CSF: cerebrospinal fluid.
Overall, the levels of antimicrobial resistance did not show relevant variations, with only slight yearly fluctuations and a trend to slowly increasing over time, except for AMS and amikacin, which showed a clear trend to increasing over time (Figure. 1a).

Evolution of MDR and XDR isolates in the period from 2013 to 2019. (a) Overall data. (b) XDR isolates in inpatients in the period from 2013 to 2019. (c) XDR isolates in outpatients in the period from 2013 to 2019.
While microorganisms recovered from samples from inpatients (critical care, hospital and surgical wards) showed increasing XDR levels, those from outpatients (ambulatory and emergency department) showed a high fluctuation in the levels of resistance (Table 4; Figure 1b and C).
Susceptibility to colistin showed a clear trend to increasing over time, from 41.2% in 2013 to 66.7% in 2019. When the analysis was limited to inpatients, XDR isolates only susceptible to colistin increased to 81.8% in 2019 (Figure 2).

Increasing isolation of Acinetobacter baumannii only susceptible to colistin.
Discussion
The phenomenon of antibiotic resistance is challenging current medical approaches to the treatment of infectious diseases, and organ transplantation, 18 for example, resulting in higher costs, requiring the frequent use of expensive antibiotics and longer admission, and morbidity, with increasing fatality.10,19
Most data about current point-of-care of antibiotic resistance are generated in high-income countries, with a relevant gap of knowledge of the current situation in a numerous low- and middle-income countries.
The initial increase in A. baumannii positivity probably reflects the improvement in the diagnostic processes, rather than a lower number of A. baumannii infections. On the other hand, the decrease in the number of isolates in 2019 was not related to the establishment of our Optimization Program for the use of antimicrobials (PROA), as this became active from 2010 and affected both in- and outpatients. This decrease therefore remains unexplained.
Differences in sample sources between in- and outpatients reflect the opportunistic nature of A. baumannii infections, which can lead to the most severe pathologies, such as respiratory and blood infections, especially in more delicate patients, such as those in ICUs. 20
Of note was the high number of respiratory infections among outpatients which agrees with other studies in which this kind of A. baumannii infections are the most common on community patients. 20 Although community-acquired infections are less common than those acquired in a hospital, they have been described in different geographical areas20–23 and are considered of special concern owing to related poor outcomes, especially with risk factors such as alcoholism or chronic obstructive pulmonary disease.20,22 The lack of data concerning previous admissions might explain several outpatient infections as actually being hospital acquired; however, the differences in antibiotic resistance from in- and outpatients, as well as the differences in the evolution of MDR/XDR isolates in both populations, suggest a different origin and support the presumption of a truly community-acquired A. baumannii.
Our data show worrisome levels of resistance to almost all antibacterial agents tested. Indeed, all the antibacterial agents tested, with the exception of aminoglycosides and colistin, presented levels of resistance higher than 80%, with these rates increasing when limited to inpatients. These findings highlight that this is not related to hospital specificity, but rather to the expansion of highly resistant A. baumanni clones in the area. This worrisome scenario is fuelled by the lack of control of antibacterial agents, which may be easily acquired over-the-counter, 24 as well as their incorrect or unnecessary prescription. 25
Our finding of >70% A. baumannii isolates from ambulatory and emergency departments as XDR is of special concern, as it strongly suggests the continuous arrival of asymptomatic carriers of highly resistant A. baumannii (or other microorganisms) to sensitive hospital areas, which may become new nosocomial residents and infect admitted patients.
Our data demonstrate an insidious, albeit clear, trend of an increase in the number of XDR isolates and a parallel decrease of MDR isolates, clearly related to the evolution of XDR levels. While it is comforting to observe that colistin remains highly active, the extreme risk of the introduction of colistin resistance, likely pan-resistant, A. baumannii, is worrying, highlighting the need for new treatment alternatives, such as cefiderocol and tigecycline,12,26 whose testing is urgently needed to establish their usefulness.
The lack of data on previous admissions of outpatients precludes a more accurate analysis and is one of the limitations of our study. Also, the lack of molecular analysis to determine the presence of clonal relationships among isolates or to establish horizontal dissemination of specific mechanisms of antimicrobial resistance may be considered as the more relevant limitation of our analysis since it precludes more in-depth knowledge of the dynamics of XDR A. baumannii populations.
At the clinical level, it is very difficult to recognise signs and symptoms that differentiate an A. baumannii infection. Comparing two Acinetobacter species (A. baumannii and A. nosocomialis), is also very difficult. 27 It is thus essential to have a quality microbiology service for a correct diagnosis and follow-up.
Footnotes
Acknowledgement
The authors would like to thank Donna Pringle for English editing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This work was supported by internal funds of Universidad Científica del Sur. JR was supported by Fondo Nacional de Desarrollo Científico, Tecnológico y de Innovación Tecnológica (FONDECYT – Perú) within the “Proyecto de Mejoramiento y Ampliación de los Servicios del Sistema Nacional de Ciencia, Tecnología e Innovación Tecnológica” [contract: 08-2019-FONDECYT-BM-INC-INV”]. This study has been performed within the frame of the net P220RT0168 from Programa Iberoamericano de Ciencia y Tecnología para el Desarrollo (CYTED).