
Abstract
Our study aims to assess the prevalence of coeliac disease (CD) among patients with irritable bowel syndrome (IBS), a recognised high-risk group for CD, in Rajasthan. We found 9/287 consecutive adult IBS patients seropositive or with biopsy-confirmed CD. Lower haemoglobin levels were independently associated with CD.
Introduction
Coeliac disease (CD) is a chronic, systemic immune-mediated enteropathy triggered by gluten ingestion in genetically predisposed individuals. With the advent of better diagnostic modalities and increasing awareness about the disease, CD is now recognised as a global health concern, with a rising prevalence worldwide. 1 Its estimated prevalence in India is 1.04%, which is significant considering its large population. 2 While classical CD presents with gastro-intestinal symptoms such as chronic diarrhoea and malabsorption, extraintestinal manifestations are well documented. Moreover, many patients exhibit non-classical symptoms such as dyspepsia, constipation, and symptoms overlapping with IBS. 3 IBS is classified as a disorder of gut–brain interaction and is characterised by recurrent abdominal pain associated with altered bowel habits. 4 Multiple studies show that IBS is common in the Indian population and its prevalence varies from 0.4 to 4.2%.5–7 Notably, there is considerable symptom overlap between CD and IBS. Studies suggest that up to 4% patients with IBS may have underlying CD, and up to 35% patients with CD have IBS-like symptoms. 8 This overlap poses a diagnostic challenge, as IBS is typically diagnosed clinically, and organic conditions such as CD may remain undetected without targeted evaluation. Furthermore, some patients with CD may continue to experience IBS-like symptoms despite adherence to a gluten-free diet, further complicating clinical differentiation. Regional differences in the prevalence of CD have also been well described, largely due to variations in dietary habits and staple foods, with a prevalence higher in wheat-consuming populations, 9 such as Rajasthan. However, there is a lack of systematic data on the prevalence of CD in this region. While population-based studies are ideal for determining the true disease prevalence and provide the most accurate estimates of disease burden, they are resource-intensive and often not feasible in low- and middle-income settings. Alternatively, studying high-risk groups, such as individuals with chronic diarrhoea, type 1 diabetes, anaemia, short stature, or IBS, can provide valuable insights, as the prevalence of CD in these groups is expected to be significantly higher than in the general population. 10 Establishing a high prevalence in such groups may pave the way for future population-based studies.
Materials and methods
Our prospective observational study was conducted at a tertiary care centre in Rajasthan between November 2021 and December 2022. Consecutive adult patients diagnosed with IBS attending as out-patients were screened for inclusion. The primary objective was to determine the prevalence of CD among patients with IBS, while the secondary objective was to identify potential clinical and biochemical predictors of CD in this population.
Our study was designed, data collected and analysed, and the manuscript written independently by the study authors without involvement from any funding agency or external sponsor. All authors vouch for the accuracy and completeness of the data. The study adhered to good clinical practice standards, and written informed consent was obtained from all participants. The study protocol conformed to the ethical guidelines of the 1975 Declaration of Helsinki and was approved by the Institutional Ethics Committee (Approval No. AIIMS/IEC/2021/3609).
Patients aged ≥18 years who fulfilled the Rome IV diagnostic criteria for IBS and provided informed consent were included. We excluded pregnant women, patients with type 1 diabetes mellitus, inflammatory bowel disease, Down's syndrome, dermatitis herpetiformis, co-existing malignancy, co-existing severe organ dysfunction (viz. decompensated heart failure, chronic kidney disease on haemodialysis, respiratory failure requiring oxygen therapy etc.), and those with previously diagnosed CD or taking a gluten-free diet.
Baseline data including demographic details and laboratory investigations (e.g. liver function tests, alkaline phosphatase, complete blood count, and coeliac serology) were recorded.
All enrolled patients were screened for CD using IgA anti-tissue transglutaminase (anti-tTG) antibody levels measured via ELISA (Quanta Lite® R h-tTG IgA ELISA, Innova Diagnostics, USA). Test results were interpreted as negative (<4 U/ml), equivocal (4–8 U/ml), and positive (>8 U/ml). All those with positive results underwent upper gastro-intestinal endoscopy and at least four biopsies were obtained from the second part of the duodenum. These were evaluated for mucosal changes by an expert histopathologist with a particular interest in gastro-intestinal pathology, who was blinded to patients’ clinical or serological results. Histological changes were graded according to the modified Marsh classification system. 11
IBS was diagnosed based on Rome IV criteria, as recurrent abdominal pain for at least 3 months (with symptom onset at least 6 months prior), associated with two or more of the following: defecation, change in stool frequency, and/or change in stool form. Subtypes were classified using the Bristol Stool Form Scale into IBS-with predominant diarrhoea (IBS-D), IBS-with predominant constipation (IBS-C), IBS-Mixed (IBS-M), and IBS-Unspecified (IBS-U). 12
CD seropositivity was defined as a positive IgA anti-tTG antibody result. Definite CD biopsy-positivity was made on positive serology and the presence of villous abnormalities of modified Marsh grade ≥2, consistent with Indian Council of Medical Research (2016) and ESPGHAN guidelines. 13
Continuous variables were summarised as mean ± standard deviation or median with interquartile range, depending on data distribution. Categorical variables were expressed as frequencies and percentages. Comparisons between groups were performed using Student's t-test for normally distributed continuous variables and the Mann–Whitney U test or Kruskal–Wallis test for non-normally distributed variables. Categorical variables were compared using the chi-square test or Fisher's exact test, as appropriate. Sample size was calculated assuming a prevalence of 4% for CD in IBS, 14 with a precision of ±2% at a 95% confidence level, yielding a required sample size of 275. To account for potential exclusions, 300 patients were enrolled. A p-value <0.05 was considered statistically significant. Data were entered using Microsoft Excel (version 16.62) and analysed with RStudio (version 2024.09.1 + 394) with base R and additional packages including tidyverse, readxl, and tableone.
Results
Baseline characteristics of IBS patients screened for coeliac disease.
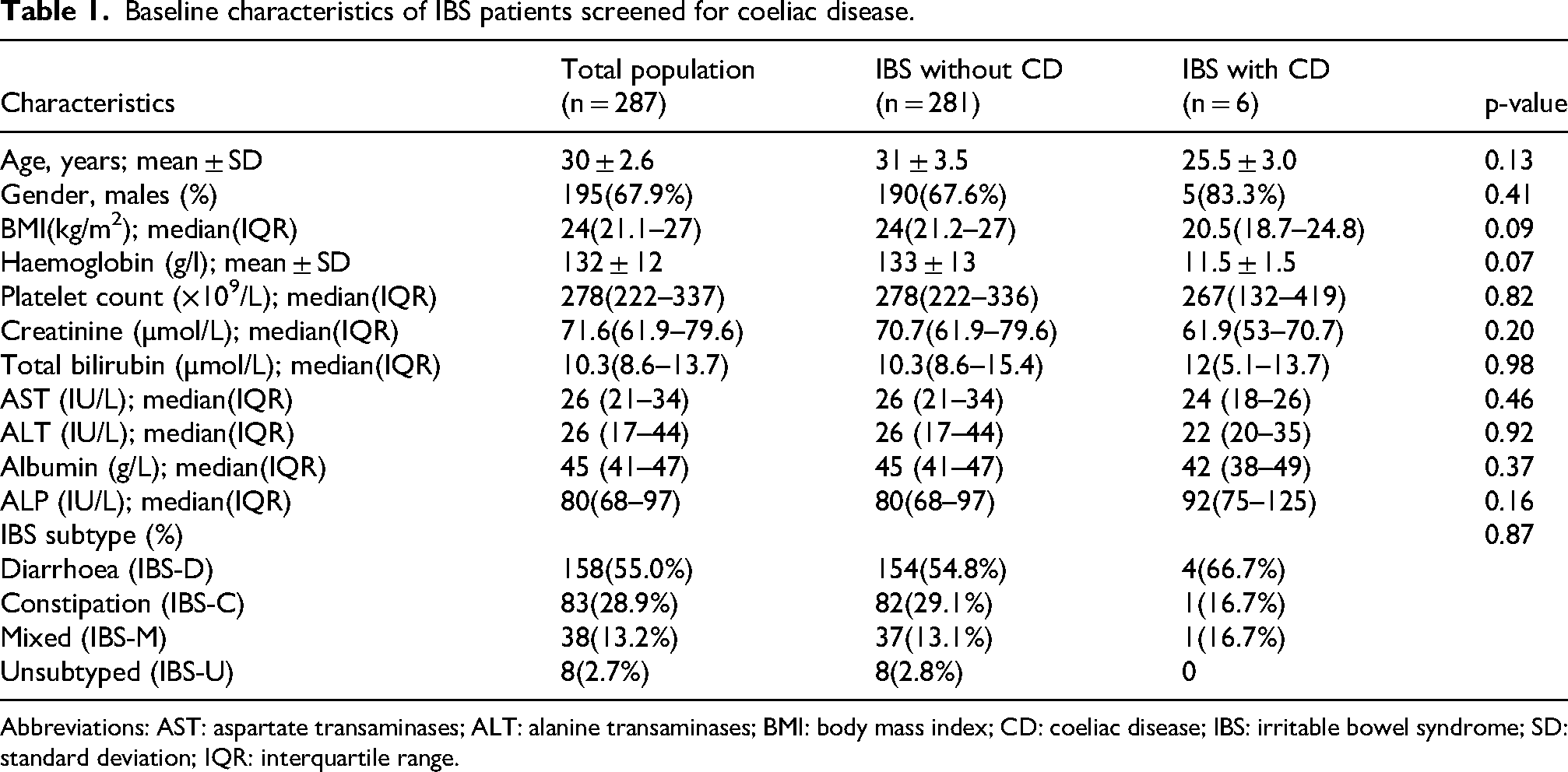
Abbreviations: AST: aspartate transaminases; ALT: alanine transaminases; BMI: body mass index; CD: coeliac disease; IBS: irritable bowel syndrome; SD: standard deviation; IQR: interquartile range.
A total of 9/287 with IBS were seropositive for IgA anti-tTG antibodies, corresponding to a seroprevalence of 3.1% (95% CI: 2.7–4.3%). The distribution of anti-tTG Ab titres (expressed as fold elevation above the upper limit of normal) was: >10-fold elevation in five (1.7%), five- to10 folds elevation in two (0.7%), and two- to fivefold elevation in one (0.3%), respectively (Table 2).
Prevalence of coeliac disease in patients with irritable bowel syndrome.
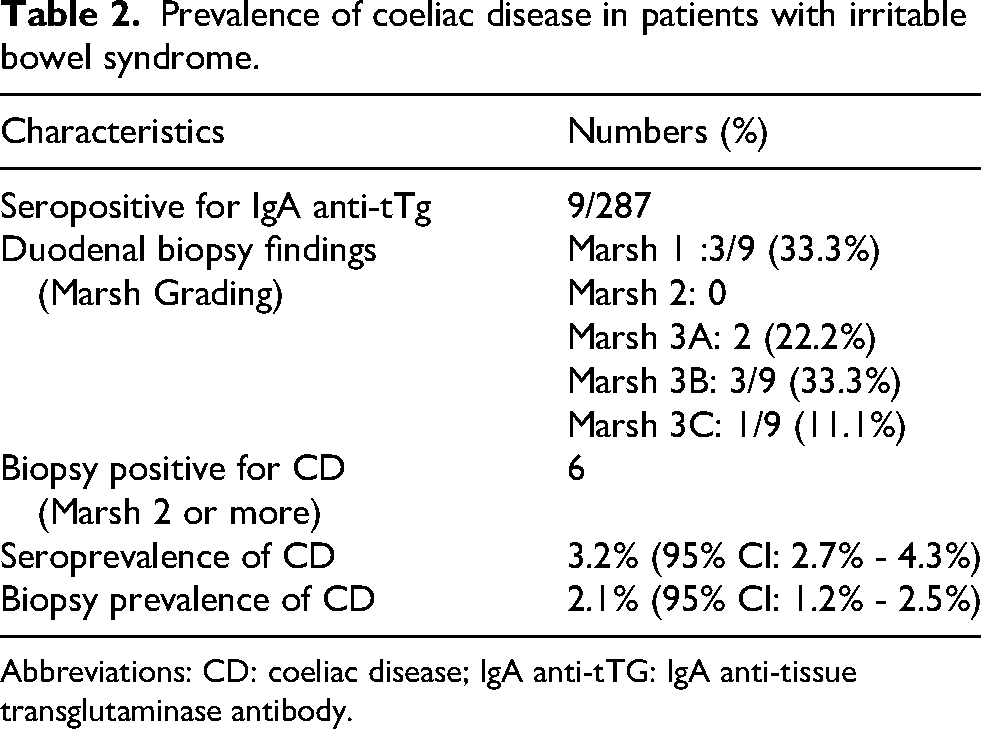
Abbreviations: CD: coeliac disease; IgA anti-tTG: IgA anti-tissue transglutaminase antibody.
Of nine seropositive patients villous abnormalities consistent with modified Marsh grade ≥2 were identified in six, giving a prevalence of biopsy-confirmed CD of 2.1%, (95% CI: 1.8–2.5%) (Table 2).
Among patients with IBS, univariate analysis identified low haemoglobin, low total protein, and elevated alkaline phosphatase levels as significant predictors of CD. However, on multivariate logistic regression, only anaemia remained independently associated (adjusted OR 0.89, 95% CI: 0.56–0.95, p = 0.03). This suggests an important and clinically relevant indicator to prompt evaluation for CD (Table 3).
Odds ratio for variables as investigated by univariable and multivariable analyses as possible predictors for coeliac disease in irritable bowel syndrome.
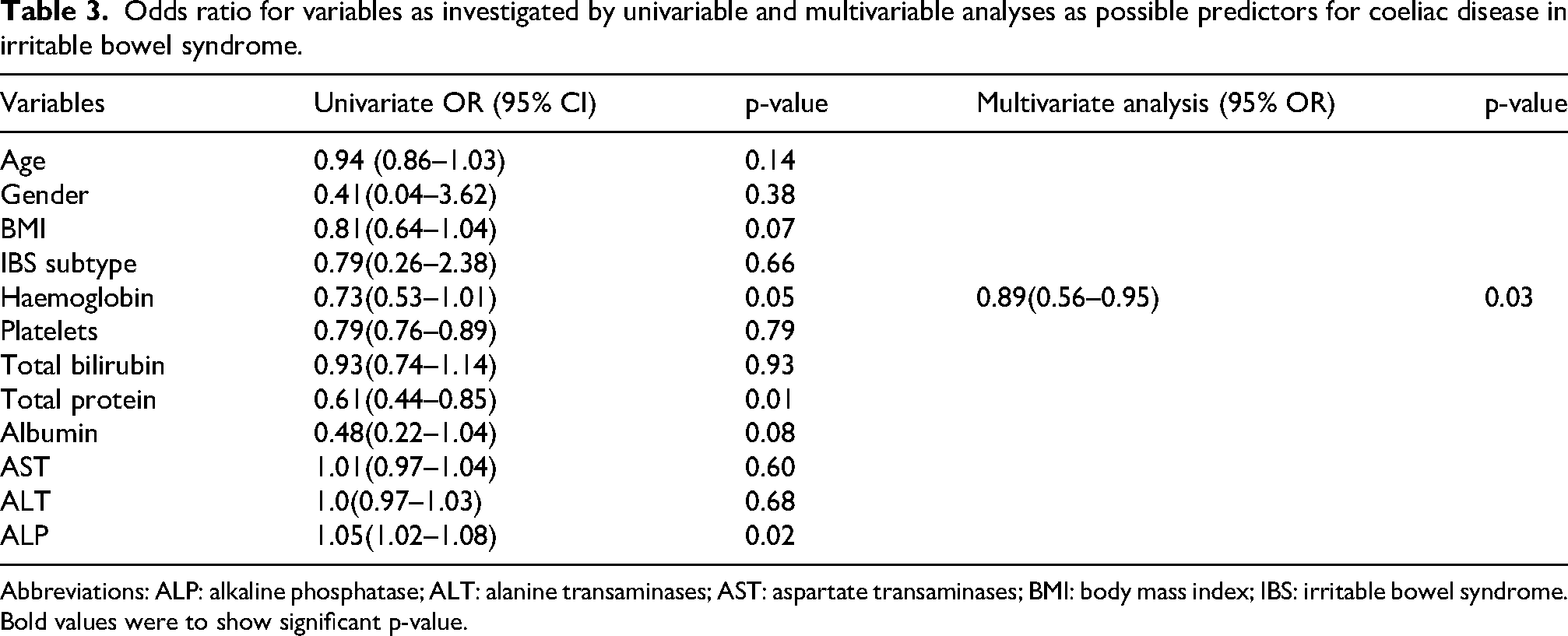
Abbreviations: ALP: alkaline phosphatase; ALT: alanine transaminases; AST: aspartate transaminases; BMI: body mass index; IBS: irritable bowel syndrome.
Bold values were to show significant p-value.
Discussion
We found a relatively high prevalence of CD in patients with IBS in Rajasthan, consistent with reports from other regions of India.9,15–17 Globally, CD is increasingly recognised in this group. 14 Indian studies suggest variable prevalence, with seropositivity up to 6.1% and biopsy-confirmed disease in 0.8%. 8 High wheat consumption probably contributes to a CD prevalence similar to or higher than that seen in other northern states. Gluten exposure therefore remains high in these populations, and in the absence of systematic screening strategies, a substantial number with underlying CD may remain undiagnosed.
Although CD is classically associated with diarrhoea-predominant symptoms, non-classical presentations (including constipation or extraintestinal manifestations) are increasingly recognised. Therefore, reliance solely on symptom subtype to suspect CD may lead to underdiagnosis, and screening strategies should not be restricted to diarrhoea-predominant IBS alone. Larger studies are warranted to confirm the association between IBS subtypes and CD.
Anaemia may be a useful clinical clue to prompt CD screening in IBS patients. This finding is clinically relevant and biologically plausible, as iron deficiency anaemia is a well-established extra-intestinal manifestation of CD and may precede gastro-intestinal symptoms. Given that IBS is a functional disorder characterised by subjective symptoms, its diagnosis is typically clinical, with investigations typically reserved for patients with alarm features. 18 Incorporating haemoglobin as a trigger for screening may offer a pragmatic approach in resource-limited settings. Importantly, several organic conditions, including CD, small intestinal bacterial overgrowth, lactose intolerance, and parasitic infections, may mimic or co-exist with IBS.19,20 Failure to identify these conditions can delay appropriate management. Our findings reinforce the need for a more nuanced approach to IBS evaluation, particularly in high-risk populations.
However, our study has a few limitations; the relatively small number of biopsy-confirmed cases limits the power to detect associations with other predictors. Additionally, serological testing was limited to IgA anti-tTG without confirmatory anti-endomysial antibody testing, which may have influenced diagnostic accuracy. The absence of a non-IBS control group precludes direct comparison with the general population. Finally, the observational design limits causal inference. Nonetheless, our prospective design, systematic screening approach, and use of histological confirmation strengthen the validity of our findings.
In conclusion, our study suggests that CD is not uncommon among patients presenting with IBS-like symptoms, and clinical differentiation based on symptoms alone is unreliable. Targeted screening, particularly in patients with anaemia, may facilitate earlier diagnosis and improve clinical outcomes.
Footnotes
ORCID iDs
Ethics approval
The study protocol was approved by the Institute Ethics committee (Approval No. AIIMS/IEC/2021/3609).
Patient consent
Written and informed consent were taken from all patients before enrolment in the study.
Permission to reproduce material from other sources
Not required.
Author contributions
Conception and design of study was done by AA and BK. Generation, collection, assembly, analysis, and/or interpretation of data were done by DM, AA, VCG, and TS. Drafting or revision of the manuscript was done by DM, AA, VCG, TS, BKG, and AA. Critical revision of the article for important intellectual content was done by AA, CLB, MKG, BK, and AA. Approval of the final version of the manuscript was obtained by all authors.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Writing assistance
None.
Guarantor of article
Ashish Agarwal.