
Abstract
Background
Accurate and timely Gram stain interpretation of positively flagged blood culture bottles is crucial for early detection of bloodstream infections and initiation of empirical therapy. However, resin and charcoal particles in culture media may interfere with smear clarity.
Methods
A prospective study was conducted on 100 positive blood culture samples. Four smear preparation techniques – conventional, water wash, blood film, and drop and rest – were applied. These were assessed for diagnostic agreement with final culture results and graded for resin/charcoal interference. Kappa (κ) statistics measured concordance.
Results
The blood film method showed the highest agreement with culture Gram stains (63%, κ = 0.26), followed by conventional (62%, κ = 0.24), drop and rest (61%, κ = 0.22), and water wash (59%, κ = 0.18). It also had the least particle interference and the most deposit-free smears (29/100).
Conclusion
The blood film method offers superior diagnostic clarity and is recommended
Introduction
Bloodstream infections (BSIs), particularly in high-risk individuals, are linked to considerable morbidity and mortality, underlining the critical importance of early pathogen detection and prompt initiation of therapy to improve patient outcomes. Among the initial diagnostic tools available in the microbiology laboratory, Gram staining of positively flagged blood culture bottles plays a pivotal role in the rapid preliminary identification of pathogens. 1
It provides valuable information regarding the morphology and Gram reaction of bacteria, allowing clinicians to initiate or modify empirical antibiotic regimens even before culture results are finalised. 2 Additionally, reliable Gram stain interpretation enables laboratories to perform direct antimicrobial susceptibility testing on blood culture broth, potentially reducing the diagnostic turnaround time by 24 h. 3 Despite its clinical value, direct Gram stain interpretation from blood culture broth is challenging, and errors in interpretation have been linked to inappropriate therapy and poorer patient outcomes. 4
One of the main limitations is the presence of resin and charcoal particles in the blood culture media.5,6 These additives are designed to neutralise residual antibiotics in the patient's blood, thereby enhancing microbial recovery. However, they also retain crystal violet stain, appearing Gram-positive and often obscuring or mimicking bacterial forms. This can lead to misinterpretation, especially in cases with low bacterial load or in laboratories with less experienced personnel. Additionally, technical factors such as smear thickness, uneven distribution of the sample, and improper fixation can further compromise the clarity and accuracy of the results. 6
To address these limitations, several smear preparation techniques have been described, including the conventional method, the water-wash method, the blood film method, and the drop-and-rest method. 7 While the conventional method is widely used owing to its simplicity, it has been associated with high rates of artefact-related interference. In contrast, the blood film and drop-and-rest methods – recommended by automated blood culture system manufacturers – aim to reduce particulate artefacts by facilitating better separation of microbial elements from background debris. 8
Although multiple smear preparation techniques have been proposed to enhance the clarity and accuracy of Gram stain interpretation from blood culture broths, comparative data evaluating their relative diagnostic performance remain limited. Recognising this gap, our study was designed to assess and compare four distinct smear preparation methods – namely, the conventional method, the water-wash method, the blood film method, and the drop-and-rest method – according to standard references described below.9–12 The evaluation focused on two key parameters: the level of agreement between each method's Gram stain findings and the final culture-based Gram stain results, and the extent of interference caused by resin and charcoal particles present in the culture medium.
Material and methods
This prospective cohort study was conducted at the University College of Medical Sciences and Guru Teg Bahadur Hospital, Delhi, India, between January and May 2025. All 100 positively flagged blood culture bottles from the BacT/ALERT automated system were included. The study had been approved by the Institutional Ethical committee No: GTBHEC 2024/P-203.
Upon flagging positive, the bottles were promptly removed from the instrument and transferred to a biological safety cabinet for further processing. A sterile, unused syringe was inserted through the alcohol swab to aspirate 1–2 mL of broth aseptically. Subsequently, four different smear preparation techniques were employed: the conventional method, the blood film method, the drop-and-rest method, and the water-wash method. These were performed according to standard reference protocols, detailed in the subsequent section.
Conventional method
A clean slide is prepared by placing a drop of the sample onto its surface and spreading it evenly to form a smear about 1 cm in diameter. The smear is then left to air dry, followed by heat fixation. 9
Water-wash method
A drop of blood from the culture bottle is placed on a clean, labelled slide and allowed to dry. The slide is then gently washed with water, directing the flow first over the thumb and then allowing it to cascade freely across the smear. After the water wash, the smear is heat-fixed and stained.
Blood film method
This method closely resembles the preparation of a thin peripheral blood smear, following the manufacturer's instructions. 9 A small drop of the sample is placed at one end of a clean, labelled slide. A second clean slide, held at a 25° angle, is used as a spreader to touch the drop. The spreader slide is then pressed firmly against the first slide and quickly pushed forward to distribute the sample evenly. After the smear is prepared, it is air-dried, heat-fixed, and stained. The stained smear is examined in the region where the sample is most thinly and evenly spread.
Drop-and-rest method
A drop of the sample from the blood culture bottle is placed on a clean, labelled slide and left undisturbed for about ten minutes to allow the charcoal particles to settle. 9 After this settling period, the slide is gently tilted so that the clearer portion of the sample could flow away from the settled charcoal. The sample is then spread using an applicator stick, air-dried, and fixed either by heating at 60°C or with 95% methanol for 2 min. After staining, the smear is examined in the area where the sample had been spread, rather than at the site where the original drop is placed.
After preparing the smears using the aforementioned methods, all were subjected to Gram staining following the standard protocol. 11 As part of routine laboratory procedures, broth from blood culture bottles that had flagged positively was streaked onto common bacteriological media such as sheep blood agar and MacConkey agar. Gram staining was subsequently performed on smears prepared from colonies that had grown after overnight incubation at 37°C under aerobic conditions.
To ensure consistency in interpretation, the results of the Gram stain were categorised into five distinct groups: Gram-positive cocci, Gram-positive bacilli, Gram-negative cocci, Gram-negative bacilli, and mixed flora. Additionally, the presence of resin or charcoal particles within the smear was evaluated and classified according to the following scale: ‘Nil’ indicated that no resin or charcoal was observed across 20 fields, ‘Minimal (1+)’ was assigned when resin or charcoal appeared in 1 to 5 of the 20 fields, ‘Moderate (2+)’ was used when they were observed in 6 to 10 fields, and ‘Heavy (3+)’ was given when resin or charcoal was present in more than 10 of the 20 fields. This classification ensured a standardised and systematic approach to the interpretation of the Gram stain results. 13
The smear preparations and Gram staining were meticulously performed by the same skilled laboratory technician throughout the study, ensuring consistency. Three independent observers, each possessing a minimum of three years’ expertise in Gram stain interpretation, meticulously examined the slides. To eliminate bias, the observers remained blinded to the culture smear results until the conclusion of the study. The final interpretation was considered valid only when at least two of the three observers reached a unanimous agreement. Smears where no consensus was reached among all three observers were excluded from the analysis.
To evaluate the level of agreement between the Gram stain results of the blood culture broth and the culture smear, kappa statistics were applied for statistical analysis.
Results
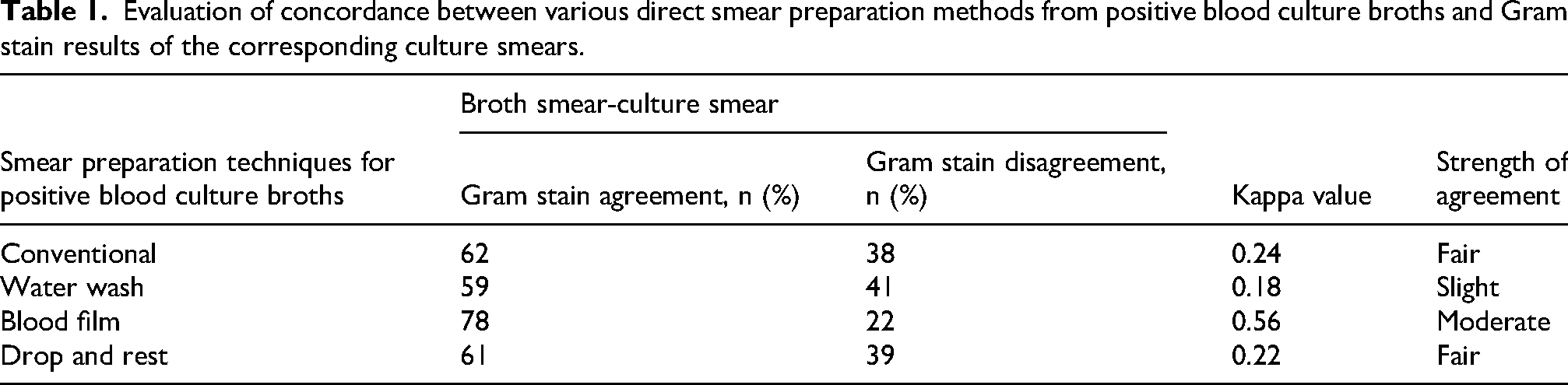
A total of 100 positively flagged automated blood culture bottles were processed. Statistical analysis of concordance was conducted using the kappa (κ) coefficient to evaluate the level of agreement. Among the four methods, the highest agreement was observed with the blood film method (κ = 0.56), followed by the conventional method (κ = 0.24), drop and rest (κ = 0.22), and water wash (κ = 0.18). Based on the interpretive scale for κ, the blood film technique demonstrated moderate agreement with the reference standard, whereas the remaining methods showed only slight to fair agreement ( Table 1; Fig. 1).

The comparison of agreement between different direct smear preparation methods from positive blood culture broth and the corresponding Gram stain results of culture smears (%).
Evaluation of concordance between various direct smear preparation methods from positive blood culture broths and Gram stain results of the corresponding culture smears.
As shown in Table 2 and Fig. 2, Gram-positive cocci in clusters were most frequently identified using the conventional method. Gram-positive cocci in pairs were better detected by the blood film and water wash methods, with lower detection rates observed in the drop-and-rest and conventional methods. Gram-negative bacilli were most accurately identified by the blood film methods. The detection of anaerobic spore bearers and budding yeast cells remained consistent across all smear preparation techniques, each demonstrating uniform identification rates. Sterility was most frequently noted in smears prepared by the water wash method.
The grading of resin/charcoal among various four methods in the study group (n = 100).
Comparative analysis of various methods based on final pathogen identification.

GPC: Gram-positive cocci, GPB: Gram-positive bacilli, GNB: Gram-negative bacilli, BYC: Budding yeast cells; ASB: anaerobic spore bearer.
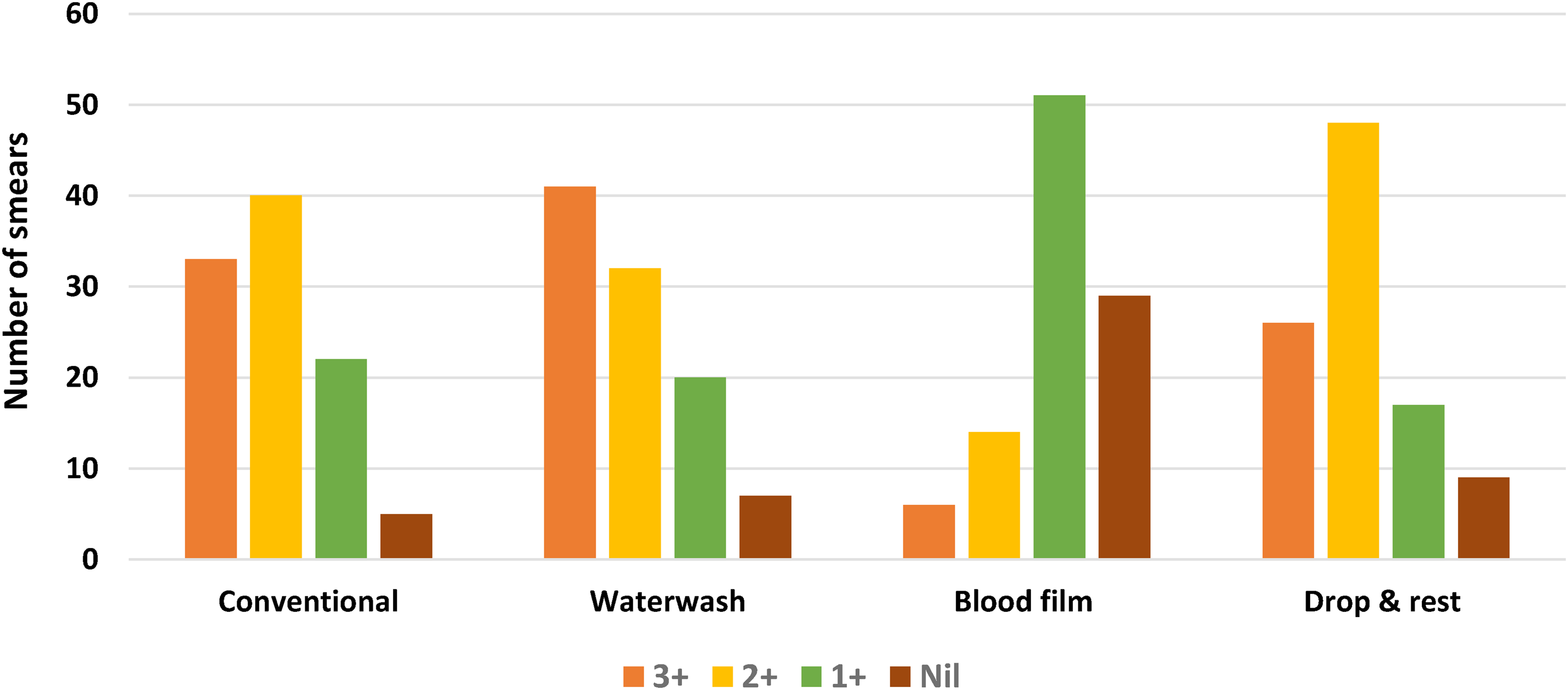
Table 3 presents the distribution of resin/charcoal grading (n = 100) in Gram-stained smears prepared by four different smear preparation techniques obtained from positive blood culture bottles. The presence of heavy resin/charcoal deposits (3+) was most frequently observed in smears prepared by the water wash and conventional methods, followed by the drop-and-rest method. The blood film method demonstrated the lowest frequency of 3 + deposits, with only 6% showing heavy deposits. In contrast, water wash and blood film methods showed a lower proportion of 2 + grading, while the blood film and drop-and-rest techniques offered marginally improved detection of Gram-positive cocci in pairs and Gram-negative bacilli; the water-wash method was associated with the greatest frequency of sterile smear results. These results highlight differences in diagnostic efficacy across smear preparation techniques, emphasising the importance of method selection for optimal outcomes. Additionally, resin/charcoal-free smears were most common with the blood film method, followed by drop and rest, with conventional and water wash methods showing minimal absence of deposits (Fig. 3).

Gram stain morphology demonstrated by four different smear preparation methods (A) drop-and-rest method, (B) conventional method, (C) blood film method, (D) water wash method.
Grading of resin/charcoal among various four methods in the study group (n = 100).

Discussion
BSIs carry a high burden of illness and death, with overall mortality rates surpassing 20%. Timely administration of suitable empirical antimicrobial therapy is essential, but as many as 40% of BSI cases may initially receive inadequate or incorrect treatment prior to the first blood culture result being reported. Delays in final culture and susceptibility results are often the cause. Therefore, the microbiology laboratory must prioritise rapid, stepwise reporting – including direct Gram stain, preliminary identification, and direct susceptibility. Among these, Gram staining serves as a rapid and reliable initial diagnostic tool, facilitating early presumptive identification and optimisation of empirical therapy.14,15
This widely regarded as the first and most critical diagnostic step following a positive blood culture, enabling early presumptive identification of pathogens and guiding timely empirical antimicrobial therapy. However, its clinical significance is largely determined by the quality of smear preparation, which plays a crucial role in ensuring accurate interpretation. The American Society for Microbiology underlines the importance of Gram staining in initial reporting and recommends the use of clear, descriptive terminology. As such, Gram stain findings typically form the basis of the first clinical notification, influencing early treatment decisions and potentially improving patient outcomes. 14
A major challenge, however, in Gram staining from blood culture broths is the interference caused by resin or charcoal particles, which obscure microscopy and hinder interpretation. Suboptimal smear preparation, particularly with the conventional method, further contributes to misidentification or missed detection of organisms. 3
Our results demonstrate that the blood film method had the lowest incidence of heavy background deposits, thereby offering superior visual clarity. On the other hand, the water wash and conventional methods showed a higher percentage of smears with heavy (3+) resin/charcoal deposits, potentially hindering accurate interpretation. The drop-and-rest method showed intermediate results, balancing ease of use and moderate reduction in artefacts. The blood film method had the least interference (29% smears deposit-free), supporting its use as the preferred smear preparation technique for accurate and reliable Gram staining from positive blood cultures as previously shown. 15
Our findings highlight the need for clinical microbiology laboratories to reassess their smear preparation techniques. The blood film method offers superior clarity and minimal background interference, and thus is recommended for optimal diagnostic performance.
Although our study evaluated each smear preparation technique as an independent method, the possibility of using multiple or combined smear preparation approaches to enhance diagnostic reliability warrants consideration. While employing more than one technique may theoretically improve organism detection, such an approach may not be feasible in routine clinical microbiology laboratories owing to increased turnaround time, additional workload, and resource constraints, particularly in high-throughput or resource-limited settings. Future studies may explore sequential or combined smear preparation strategies to determine whether the incremental diagnostic benefit justifies the added complexity in routine laboratory practice.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.