
Abstract
Although there has been extensive research on attention deficit hyperactivity disorder as a clinical disorder in adulthood, many clinicians remain sceptical about the validity of this disorder. Among the many reasons for this are comorbid conditions which may complicate the disorder. The aim of this study was to determine the prevalence rates of other disorders among a group of adults with attention deficit hyperactivity disorder, based on participants’ scores on the Million Clinical Multiaxial Inventory-III. In order to meet this aim, the Million Clinical Multiaxial Inventory -III results of a group of adults with attention deficit hyperactivity disorder (n = 51) were analysed. In terms of Cluster B personality disorders, the following prevalence rates were found for the attention deficit hyperactivity disorder group: 23% Borderline, 27.4% Antisocial, 19.6% Histrionic, and 19.6% Narcissistic. As far as comparing prevalence rates of possible comorbid conditions, as found in this study, with those of previous studies, the results compare well to those conditions that are reported as the most prevalent in other studies. However, the wide range of clinical and personality disorders that are associated with attention deficit hyperactivity disorder indicate that there are no typical comorbid disorders.
Keywords
Although the diagnosis of attention deficit hyperactivity disorder (ADHD) in adults has been reported in the literature in the past and there has been some room for the diagnosis in the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR) (American Psychiatric Association, 2000), the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) (American Psychiatric Association, 2013) provides clear criteria for this disorder in adulthood. Despite this, especially in the South African context, there are still some areas that require further investigation. One of these is the problem of comorbidity, given the overlap in symptoms between this disorder and many other disorders. This leads to, among others, problems in establishing the prevalence rates of ADHD in an adult population. In this regard, Burke, Austin, and Waldeck (2011) as well as Burke and Austin (2011) reported prevalence rates of between 4% and 16% in a South African student population.
The other problem related to the overlap of symptoms is differentiating ADHD in adulthood from other disorders. The essential criteria for a diagnosis of ADHD are inattention, impulsivity, and hyperactivity (Rösler et al., 2006), although the presence of the hyperactivity symptoms in adulthood is much debated with some authors arguing that it decreases from childhood into adulthood (Bresnahan, Anderson, & Barry, 1999), it manifests differently (Schmidt & Petermann, 2009), or adults find ways of coping with this (Goodman, 2007). Furthermore, hyperactivity and impulsivity in adulthood may often manifest as feelings of agitation and attempts to escape deskbound and inactive tasks (American Psychiatric Association, 2013). The problem arises from the fact that these core symptoms are not unique to ADHD, nor is the way in which they manifest. These core symptoms may also be associated with, result in, or be complicated by other common clinical features. Concomitant emotional difficulties such as low frustration tolerance, unpredictable mood swings, irritability and emotional explosiveness, being emotional labile as well as bossiness, stubbornness, feeling unmotivated, and dysphoria can be frequent (American Psychiatric Association, 2013; Wilens, Biederman, & Spencer, 2002; World Health Organization, 1992). Such difficulties may result in relational problems, rejection by peers, demoralisation, and low self-esteem (American Psychiatric Association, 2013). Again, none of these manifestations are unique to ADHD as they occur in a number of other psychiatric disorders as well. It must be noted, however, that although there may be overlaps in symptoms, there are also differences (see Table 1) which may make it difficult to distinguish between disorders.
Communalities and differences of symptoms shared by ADHD and other disorders.
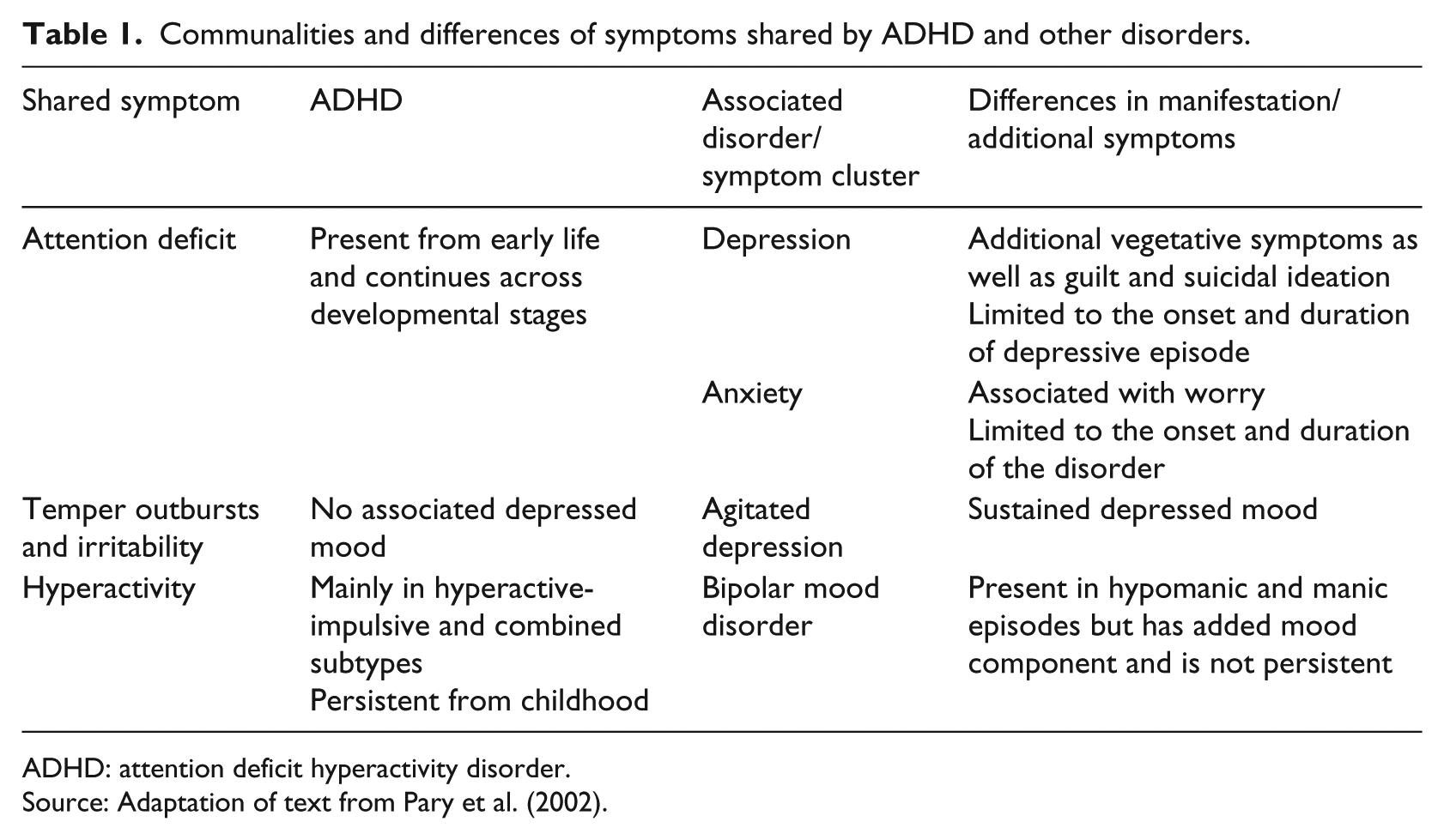
ADHD: attention deficit hyperactivity disorder.
Source: Adaptation of text from Pary et al. (2002).
These overlaps of symptoms between ADHD and other disorders do complicate the diagnostic process not only in terms of deciding on a primary diagnosis but also in terms of the necessity of making a differential or comorbid diagnosis. In 75% of cases where ADHD is the primary diagnosis, additional comorbid disorders are also diagnosed (Pary et al., 2002). Due to the fact that this disorder was previously considered to be an exclusively childhood disorder, and added to the fact that the disorder is characterised by disruptive behaviour, it is not surprising that it has been and is associated with a variety of learning disorders, conduct disorders, and oppositional defiant disorders. As the disorder gains more recognition as a disorder which may continue into adulthood, a number of studies have found comorbidity between this disorder and a number of other psychiatric disorders (Biederman, 2005; Fossati, Novella, Donati, Donini, & Maffei, 2002; Jacob et al., 2007; Kessler et al., 2005; Miller et al., 2008; Sobanski et al., 2007). Examples of these comorbid conditions as well as studies that report these are summarised in Table 2.
Examples of comorbidity studies.
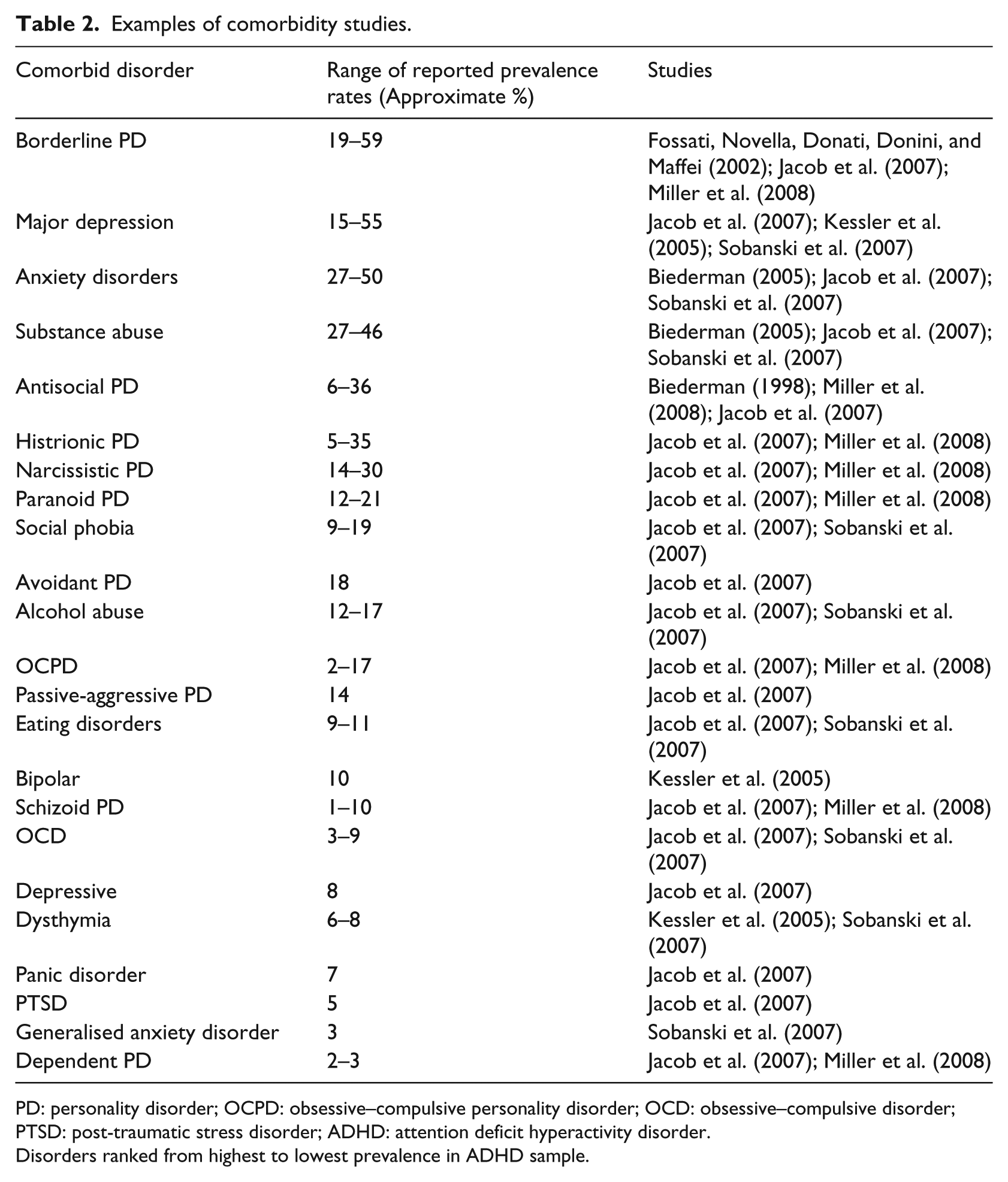
PD: personality disorder; OCPD: obsessive–compulsive personality disorder; OCD: obsessive–compulsive disorder; PTSD: post-traumatic stress disorder; ADHD: attention deficit hyperactivity disorder.
Disorders ranked from highest to lowest prevalence in ADHD sample.
Given the range of disorders stipulated in Table 2, the widely differing ranges of prevalence rates reported thus far, and the lack of research in this regard in South Africa, this study aimed to explore the prevalence rates of comorbid disorders in a group of South African adults diagnosed with ADHD.
Method
Participants
One of the main challenges in this study was to accurately identify adults with a diagnosis of ADHD. Participants who had been part of a larger adult ADHD project were recruited by means of purposive sampling and they had to comply with strict inclusion and exclusion criteria in order to be included in the study. The sample was recruited from various Mental Health Professionals (i.e. Clinical and Educational Psychologists and Psychiatrists in private practice), and all of them had a formal diagnosis of ADHD. All participants had to be older than 18 years of age. Despite the fact that they had a formal diagnosis of ADHD, they were also screened by the research team, which consisted of registered Clinical Psychologists, by means of clinical interviews, as well as the Adult ADHD Self-Report Scale (ASRS). Following the screening, 51 adults, 30 males and 21 females, met the criteria and were included in the study. The ages of the participants ranged from 21 to 45 years, with a mean age of 26 years.
Measurement instruments
Semi-structured clinical interview
The interviews were conducted by any one of the trained Clinical Psychologists who formed part of the research team. The purpose of the interviews was to ensure that participants met the DSM-5 criteria for inclusion in the study, as well as to obtain biographical and clinical information of participants, based on Sadock and Sadock’s (2000) recommendations for clinical interviews.
ASRS
For the purpose of this study, the ASRS was used for screening purposes only. The ASRS is a self-report, 18-item questionnaire which screens adults for ADHD (Kessler et al., 2005). The items are based on the diagnostic criteria for ADHD as listed in the DSM-IV-TR (American Psychiatric Association, 2000). Half of the questions focus on inattention and the other half on hyperactivity. The items are each rated on a 5-point Likert scale, that is, never, rarely, sometimes, often, and very often (Kessler et al., 2005). A number of authors have reported favourable psychometric properties for this instrument (Adler, Ciranni, Shaw, & Paunikar, 2010; Taylor, 2011). The total classification accuracy for the instrument is 96%; however, the ASRS has moderate levels of concurrent validity and sensitivity, but high levels of specificity (Taylor, 2011).
MCMI-III
The Million Clinical Multiaxial Inventory-III (MCMI-III) is primarily a self-report questionnaire that assesses a wide range of information about an adult’s personality and emotional adjustment (Groth-Marnat, 1997). It was designed as a diagnostic tool that yields information about personality disorders as well as clinical syndromes (Craig, 2005). The test consists of 175 questions that are forced-choice, true–false items (Millon, Millon, Davis, & Grossman, 1997). The MCMI-III has 28 subscales, which are categorised into five different categories (Groth-Marnat, 1997), that is, Modifying Indices, Clinical Personality Patterns, Severe Personality Pathology, Clinical Syndromes, and Severe Syndromes. Reliability and validity studies have indicated that the MCMI-III is a well-constructed instrument in the measurement of personality and emotional adjustment (Groth-Marnat, 1997). The results for the internal consistency was .66 for the compulsive scales and .90 for Major Depression, and the Cronbach alpha’s for the remaining 26 scales exceeded .80, showing strong internal consistency (Millon et al., 1997). Test–retest reliability scores indicated the lowest score of .82 for debasement and the highest score of .96 for somatoform, of which the median test–retest coefficient was .91, which shows stability of the instrument over time (Groth-Marnat, 1997). Scores on various subtests of the scale correlate satisfactory with other measures of pathology, for example, the symptom checklist-90, the Beck Depression Inventory, the State–Trait Anxiety Inventory, the General Behaviour Inventory, the Minnesota Multiphasic Personality Inventory (MMPI), the Michigan Alcoholism Screening Test, and the MCMI-II (Groth-Marnat, 1997). Positive predictive power scores range from .30 to .80 (Groth-Marnat, 1997). The MCMI-III has proven construct and diagnostic validity, by comparing test items with other tests and by comparing clinical judgement with the results indicated from the scales on the MCMI-III (Millon et al., 1997).
Procedure
Data were collected over a period of 3 years, with all participants in the bigger ADHD study screened by means of a clinical interview, as well as a number of self-report questionnaires. As a standard practice, participants were required to complete both the ASRS and the MCMI before they participated in any of the sub-projects. The scores on these instruments were stored in a central data bank, along with their results of the other studies. For the purposes of this study, the scores of the ASRS and MCMI were extracted from the database.
Ethical considerations
This study forms part of a larger study on ADHD in adulthood, and ethical clearance was granted for the project as a whole, as well as its subcomponents by the Faculty of Humanities’ Ethical Committee at the University of Johannesburg. Furthermore, participation in the study was voluntary and all participants were of consenting age. Participants were briefed about the study, and once they agreed to participate, written consent was given by the participants. All information was treated with confidentiality, and once the data were captured, identifying information was deleted.
Statistical analysis
In order to understand the rationale for the use of different statistical techniques, the scoring and interpretation of the MCMI-III need to be discussed first. The raw scores on the test are converted to norm scores (base rate scores), for each of the subscales, based on gender. For diagnostic purposes, base rate scores below 75 are considered to be indications of no clinical significance, 75–84 as indicative of pathology, and 85 and higher as persistent pathology (Millon, Millon, Davis, & Grossman, 2009). The base rate scores can be considered to be on an interval level which allows for particular statistical techniques (i.e. mean, median, and standard deviation); however, the base rate scores can also be categorised in one of these three categories, which allows for additional statistical techniques. The frequencies of the number of base rate scores above the two critical cut-off points were also calculated, in order to determine the number of elevated scores participants, per subscale, had. This was done in order to present a clearer picture of the prevalence rates of particular disorders.
Results
In order to determine whether a particular MCMI profile would emerge for the different groups, mean, standard deviation, and median scores were calculated for each of the scales (Table 3).
Mean and standard deviation scores for the clinical and severe personality patterns subscales.
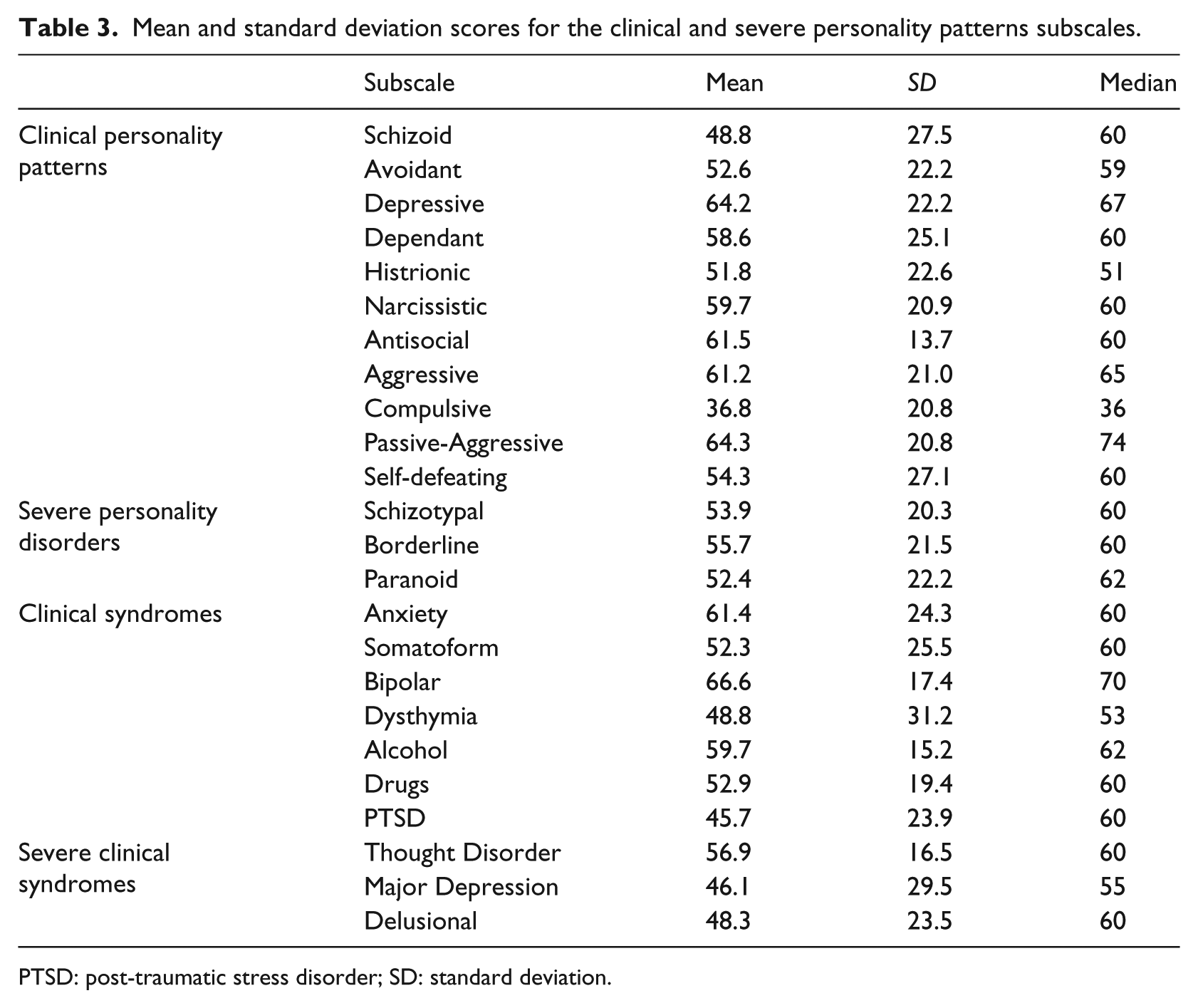
PTSD: post-traumatic stress disorder; SD: standard deviation.
Of importance is that none of the mean scores for the interpersonal styles, severe personality disorders, clinical syndromes, or severe clinical syndromes were elevated above the 75 base rate score (Table 3), which would imply that there is no typical ADHD profile on the MCMI. Of particular interest here is that the two substance scales (alcohol and drugs) were not elevated, which was contrary to expectations as it is often assumed that substance abuse is an expected comorbid condition in this population.
Number of elevated scores
Although mean scores provide some information, it does not provide enough information about the total profile. Using mean scores on the MCMI is misleading as the results on this instrument are typically interpreted by means of categories, as described before. In order to create a clearer picture, the number of participants per category, per subscale is reported in Table 4.
Number of participants per category of scores for the clinical personality patterns.
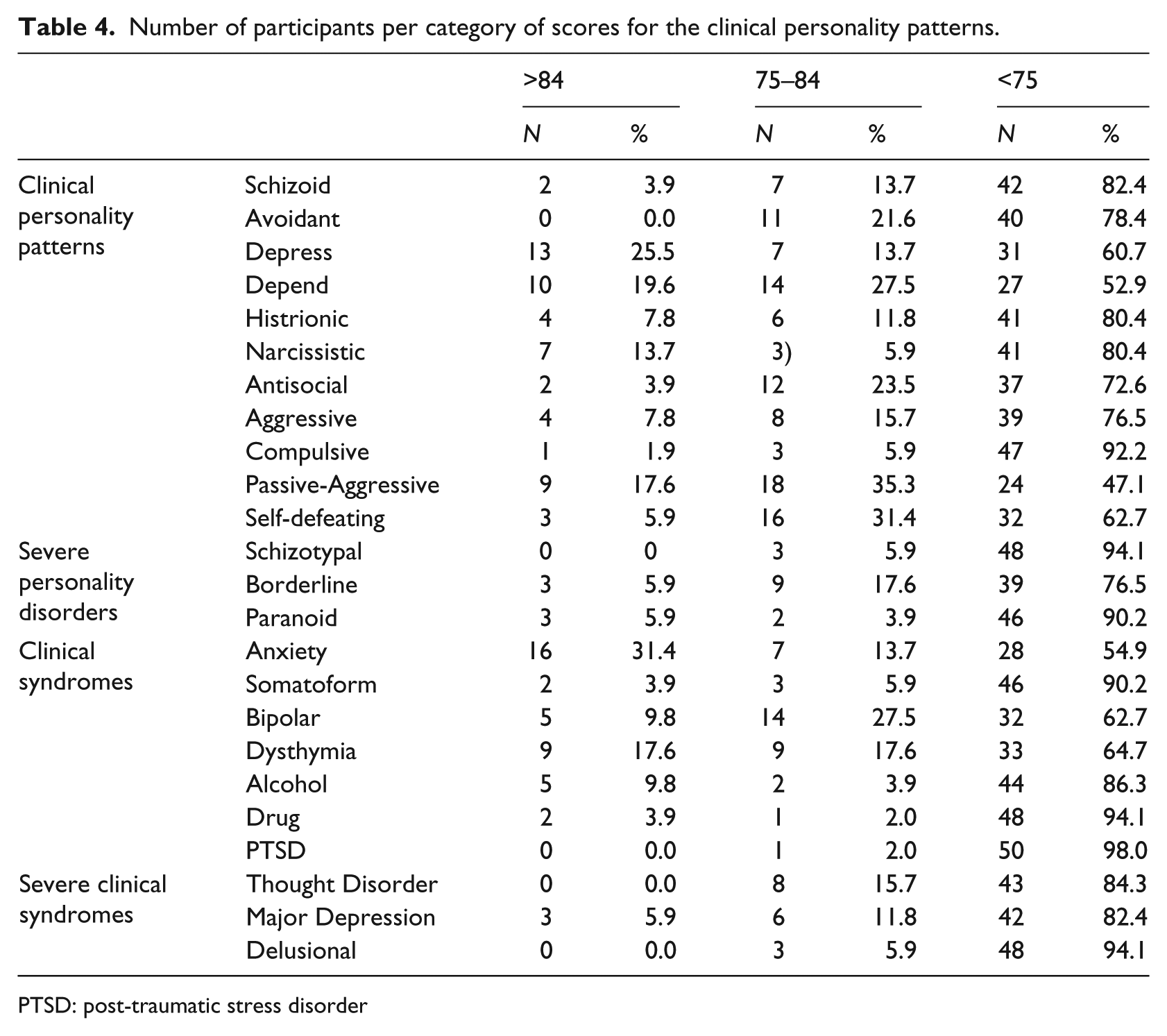
PTSD: post-traumatic stress disorder
A summary of Table 4 shows that the typical significantly elevated scores (i.e. scores >84) for the clinical personality patterns are (in order of highest to lowest prevalence) as follows: Depressive (25.5%), Dependent (19.6%), and Passive-aggressive (17.6%). For the severe personality disorders, it was only the Borderline scale that showed a relatively high prevalence rate, that is, 5.6% of participants in the >84 and 17.6% in the 75–84 base rate score range. As far as the clinical syndromes are concerned, Table 4 indicates that Anxiety (31.4%) and Dysthymia (17.6%) show the highest prevalence rates in the >84 base rate score range. Although Table 4 does not reflect any unexpected results, it is worth noting the relatively high prevalence rate of Major Depression (5.9% in the >84 and 11.8% in the 75–84 range of base rate scores), and Thought Disorder (15.7% in the 74–84 base rate range). The reason for highlighting this is the theme of a mood disorder running through the profile of the sample, that is, elevated Depressive Personality, Dysthymia, and Major Depression, as indicated by relatively elevated scores on these scales.
Discussion
When considering the results of this study, there are a number of factors to take cognisance of. The first is the greater mental health context, where ADHD in adulthood is neither widely recognised nor diagnosed in many quarters. While all of the ADHD participants were formally diagnosed with ADHD, many of them had only been diagnosed later in life, and many of them had consulted a number of practitioners before the ADHD diagnosis had been made. Caution must be exercised when interpreting these results, however, as the prevalence rates reported here are not based on secondary or differential diagnoses that were made, but merely scores on the MCMI-III, which against the backdrop of the context and the nature of the test must be interpreted with caution.
Furthermore, although the labels of clinical personality patterns subscales correspond with the DSM-5 labels of personality disorder, it would be irresponsible to equate a high score on a subscale to a personality disorder. One of the reasons for this would be that there are differing opinions about the diagnostic validity of the MCMI as whole, but more so that different subscales have more or less diagnostic validity (Dyer & McCann, 2000; Hsu, 2002; Retzloff, 1996). Another reason would be that a personality disorder should not be diagnosed on results on one particular test. To err on the side of caution, it is therefore better to interpret high scores as indicative of certain personality traits, rather than disorders. In general, the scores on these scales were higher than the prevalence rates that were reported for corresponding personality disorders in other studies (Jacob et al., 2007; Miller et al., 2008). Of note was the Passive-Aggressive subscale that was elevated in 53% of the participants, dependent in 47%, and depressive in 38%.
As far as comparing prevalence rates of possible comorbid conditions, as found in this study, with that of previous studies, the results compare well with those conditions that are reported as the most prevalent. Although the results fall mostly within the parameters of other studies, there are a number of differences which require some discussion. As far as the Cluster B personality disorders are concerned, Fossati et al. (2002) report a relatively high prevalence rate for Borderline personality disorder (59%), whereas the result of this study found a much lower rate (23%), which is closer to the 27% reported by Jacob et al. (2007), and the 19% reported by Miller et al. (2008). The rates for Antisocial, Histrionic, and Narcissistic all fall approximately midway between the highest and the lowest prevalence rates reported by other studies (Jacob et al., 2007; Miller et al., 2008).
Comparing the clinical syndromes, the prevalence rates found in this study compare favourably with those reported in other studies, although the prevalence rates do lean more in favour of anxiety disorders (45%) than major depression (18%). It must be noted, however, that the MCMI-III does not draw differences between the different types of anxiety disorders, which may have an implication for the relatively high rate reported here. Of concern, however, was the relatively high rate of bipolar (37%) compared to the 10% reported in other studies (Kessler et al., 2005). If one assumes that the MCMI-III is an accurate diagnostic tool, then one would conclude that this high prevalence is indicative of cases of misdiagnosis. Another explanation could be that the items on this subscale may reflect characteristics that are shared with ADHD. A study by Cassidy, Forest, Murry, and Carroll (1998) identified five core factors of mania, three of which could be considered to be indicative of ADHD as well. These three factors are psychomotor acceleration, increased hedonic functioning, and irritable aggression.
Another elevated scale was Dysthymia (35%), which is higher than that reported in other studies that reported prevalence rates between 6% and 9% (Kessler et al., 2005; Sobanski et al., 2007), which seems to indicate a presence of a dysphoric mood. This high prevalence rate, together with the high prevalence of the depressive personality pattern, as well as a relatively high prevalence rate of major depression, indicates the strong presence of an associated mood disorder. The high score on this subscale is indicative of, among others, guilt, pessimism, and decreased overall performance, which may be the result of the challenges faced by adults with ADHD in terms of coping with work and social demands.
The final comment about the prevalence rates relates to substance abuse. Studies by Jacob et al. (2007) and Sobanski et al. (2007) report prevalence rates between 27% and 47% for substance abuse among adults with ADHD. In this study, a prevalence rate of only 6% for drug dependence is reported. There are many possible explanations for this difference, which could be grouped into two main categories, that is, hesitancy among participants to report on this honestly and the items of the MCMI-III. As far as the first explanation is concerned, Craig (2005) fosters the opinion that there is sufficient evidence to suggest that this scale is able to rule out the possibility of drug abuse. If this is true, then the item content and formulation may offer some explanation. Many studies on substance abuse include a wide range of substances, which includes alcohol. The items of the MCMI-III make a distinction between alcohol and drug dependence, which implies that these two scales will have to be grouped together when drawing conclusions on substance abuse. Doing this, however, still yields a lower prevalence rate for substance abuse than reported in other studies.
Sampling adults with this disorder is challenging as potential participants with false-positive diagnoses need to be differentiated from those adults who meet the diagnostic criteria of ADHD. Despite screening the participants in this study, it cannot be guaranteed that no participants in this sample had false-positive diagnoses. In line with this, the relatively small sample cannot be considered to be representative of the population of adults with ADHD. A further limitation in this regard was that the ADHD sample was not compared and contrasted to other groups such as a group that does not have an ADHD diagnosis or groups with other diagnoses. It is recommended that further comparative studies be done.
The reliance on the MCMI-III for diagnosis of comorbid conditions can also be considered to be a limitation of this study as the MCMI-III is a self-report questionnaire which could yield false-positive and/or false-negative results. It is recommended that for future studies more robust diagnostic procedures be followed in order to identify and confirm comorbid conditions.
Given these limitations, these findings should not be generalised to the population of adults with ADHD and should be used mainly as a platform for further research.
Conclusion
The results of this study indicate that ADHD is associated with typical comorbid conditions and that this disorder may be present alongside a number of disorders. This implies that one should not necessarily consider diagnoses that could better account for the symptoms, but that other disorders should be treated in conjunction with the ADHD. Furthermore, in line with this, there do not seem to be typical personality disorders that are associated with ADHD, and therefore, one cannot assume that ADHD in childhood will necessarily lead to a particular personality disorder in adulthood.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.