
Abstract
The wider availability of highly active antiretroviral therapy has resulted in a concomitant increase in adults aging with HIV and the persistence of milder forms of neuropsychological impairment in this cohort. This study investigated the differences in neuropsychological functioning between a group of HIV+ adults and older adults and an HIV− matched control group. Participants from a semi-urban community clinic volunteered to participate in the study. The performance of 50 participants (33 HIV+ and 17 HIV−) who met the inclusion criteria were compared on the following measures: Dementia Rating Scale-2, the Stroop Color and Word Test, the Symbol Digits Modalities Test, and the Delis–Kaplan Executive Function System Trail Making Test. The results indicated that the HIV+ in comparison with the HIV− negative group had poorer performance profiles in global cognitive functioning, memory, executive functioning, visuoconstruction ability, psychomotor functioning, and processing speed. The findings suggest that further research in South Africa will contribute to a better understanding of the neuropsychological profiles of adults aging with HIV and inform intervention strategies specific to addressing the mental healthcare needs of this subgroup.
Due to the resource-challenged context in Africa, particularly in the healthcare sector, few envisaged or planned for a surviving aging African population with HIV (Mills, Rammohan, & Awofeso, 2011). This scenario is commensurate with the limited number of studies in Africa that have focused on aging with HIV and the increasing risk of cognitive impairment in this cohort. Research on the neuropsychological functioning in this group is motivated by the demographic shift from primarily young individuals (91% below 45 years of age in 1996) to approximately one half of the HIV-seropositive adults currently over 45 years of age (Wendelken & Valcour, 2012). The South African scenario parallels those observed internationally with the aging HIV population expected to increase by approximately 50% in the next 15 years (Hontelez et al., 2011).
Notwithstanding the success of highly active antiretroviral therapy (HAART), the long-term use of antiretroviral drugs and their consequent central nervous system neurotoxicity may result in compromised cognitive integrity in an aging brain more susceptible to the neuropathological correlates of HIV infection (Gannon, Khan, & Kolson, 2011; Liner, Ro, & Robertson, 2010). Baseline cerebral blood flow in HIV-positive (HIV+) individuals was found to be equivalent to that of HIV-negative (HIV−) individuals aged 15–20 years (Ances et al., 2010). In an adult and older adult HIV+ cohort, Fazeli et al. (2014) elucidated both the presence of subtle cognitive impairment in 47% of the study sample and the persistence of a mild and diffuse pattern of cognitive impairment in the era of HAART.
Recent cross-sectional and longitudinal studies and reviews have explicated the differences in neuropsychological profiles between HIV+ and HIV− adults and older adults, with lower performance on measures of psychomotor functioning, attention, processing speed, executive functioning, and memory evident in the HIV+ group (Cysique, Maruff, Bain, Wright, & Brew, 2011; Seider et al., 2014; Woods, Moore, Weber, & Grant, 2009). Furthermore, a comparative study revealed that HIV+ older individuals evidenced greater dispersion in neuropsychological performance across cognitive domains than HIV− individuals. The authors concluded that this is likely a function of compromised frontostriatal systems that predispose the older HIV+ cohort to dysregulation of executive control (Morgan et al., 2011). Within the memory domain, for example, deficits observed in older HIV+ individuals may be indicative of compromised executive functioning such as flawed utilization of clustering strategies (Iudicello, Woods, Deutsch, Grant, & The HIV Neurobehavioral Research Program Group, 2012).
Equivocal findings in the literature relating to the influence of age and HIV status on cognitive functioning have been reported. While cross-sectional and longitudinal studies have found independent and synergistic effects of age and serostatus on incident cognitive disorders, a recent study showed no such influences (Scott et al., 2011; Seider et al., 2014; Sheppard et al., 2015). However, cognitive performance profiles consistently show poorer outcomes for the older cohorts with HIV (Vance, Fazeli, & Gakumo, 2013). A review of studies using a screening assessment (International HIV Dementia Scale) and conducted specifically in Sub-Saharan Africa yielded evidence that HIV is a major predisposing factor for cognitive impairment, with a frequency of approximately 40% in HIV+ patients on antiretroviral therapy (Habib et al., 2013). Meta-analyses indicated that no significant association between age and cognitive impairment was evident. Utilizing a comprehensive neuropsychological battery, Lawler et al. (2011) found that 37% of HIV+ patients showed deficits in all cognitive and motor domains (memory, executive functioning, psychomotor speed, language, information processing speed and capacity, as well as fine motor ability) when compared to matched, uninfected control participants. Moreover, among the HIV+ group, those who evidenced cognitive impairment were older and had lower education levels than the cognitively unimpaired participants.
Until recently, cognitive status has been exclusively studied in developed countries on younger cohorts with HIV and in genotypically defined subtypes specific to these regions. In the era of HAART with the commensurate extension of life expectancy, the trajectory of HIV is transforming from an acute to a more chronic inflammatory disease process, and the prevalence and profile of cognitive deficits may reflect this change (Wendelken & Valcour, 2012). There are limited studies on the aging population with HIV in South Africa, and the changing disease parameters indicate that cognitive functioning in this subgroup remains relatively understudied when compared to younger HIV+ cohorts. Based on the above exposition, this study aims to explore the differences in neuropsychological outcomes between a group of HIV+ adults and older adults and an HIV− matched control group.
Method
Participants
A total of 83 participants were recruited for the study over a period of 8 months; however, 33 participants did not meet the minimum requirements as outlined in the exclusion criteria below. The remaining 50 eligible participants consisted of 33 HIV+ participants and 17 HIV− participants. A larger sample size could not be collected due to practical considerations such as time frame, cost, patient accessibility, incomplete medical information, and specificity of the clinical sample. However, the sample size was still relevant to the preliminary and exploratory nature of the research (Hardy & Vance, 2009). All participants included in the study were conversant in English and had English as a second language. Individuals were not eligible for participation if they had an unconfirmed HIV status according to medical records, a diagnosed psychiatric disorder, head injury with a loss of consciousness for more than 30 min, neurologic diseases, opportunistic brain infections, recent (within the last 3 months) history of substance abuse, cytomegalovirus (CMV) retinitis/other overt retinal conditions, or ocular opportunistic infections and dementia.
Instruments
Due to limited context-specific norms in Sub-Saharan Africa (Singh et al., 2010), only the raw scores on the instruments were compared between the HIV+ and HIV− groups. The following instruments were used to assess participants.
The Dementia Rating Scale-2 (DRS-2) (Jurica, Leitten, & Mattis, 2001) consists of 36 tasks which comprise five subscales. These subscales include attention (DRS-2 Attention), initiation/perseveration (DRS-2 Initiation/Perseveration), construction (DRS-2 Construction), conceptualization (DRS-2 Conceptualization), memory (DRS-2 Memory), and a global neuropsychological score (DRS-2 Total). Internal consistency and alpha coefficients of .95 (Attention), .87 (Initiation/Perseveration), .95 (Conceptualization), and .75 (Memory) were reported (Vitaliano et al., 1984). The DRS-2 is reported to be sensitive to cognitive impairment that has a subcortical profile, and this test has been utilized in previous HIV studies (Antinori et al., 2007; Suarez et al., 2000).
The Stroop Color and Word Test (Stroop), the Symbol Digit Modalities Test (SDMT), and the Delis–Kaplan Executive Function System (D-KEFS) Trail Making Test (TMT) were included as additional neuropsychological measures. The D-KEFS TMT comprises five conditions, and for the purposes of this study, the results of the D-KEFS-visual scan (condition 1), the D-KEFS-task switching (condition 4), and the D-KEFS-motor speed (condition 5) were reported. Test descriptions and psychometric properties are reported in Lezak, Howieson, Bigler, and Tranel (2012).
The health-related quality of life questionnaire (EuroQol five dimensions [EQ-5D])—a standardized measure of general health-related quality of life—was used to assess self-reported mood (anxiety/depression) (Robberstad & Olsen, 2010). A sociodemographic questionnaire was used to gather information on age, gender, employment status, and education. Clinical information was obtained from patients’ medical records.
Procedure
Potential participants were recruited from a government-run community clinic with an HIV wellness center. The clinic was located in a semi-urban area of Tshwane. The HIV+ group consisted of individuals who had been consecutively enrolled during routine outpatient visits. The control group consisted of HIV− individuals attending the community clinic in their capacity as caregivers, family members, and other community dwelling volunteers. Individuals identified by the medical staff as meeting the inclusion criteria of the study were given a pamphlet explaining the basic purpose of the research study (in English, Afrikaans, and Tswana). The pamphlets contained a tear-off slip on which interested participants could provide their contact details and place it in a box located in the examination room of the clinic.
Potential participants were contacted telephonically in order to set up an appointment. Participants who met the eligibility criteria and agreed to participate formalized their intention to partake in the study by signing informed consent forms, and this was followed by a more comprehensive explanation of what was required of them. All measures were administered in English by two trained masters psychology students (clinical and research) under the supervision of a qualified psychologist in the neuropsychology field. The assessment session spanned approximately 30 min to 1 hr, depending on the pace of the participant.
Ethical considerations
Ethical approval to conduct the study was granted by the Humanities Postgraduate and Research Ethics Committee of the University of Pretoria and the Department of Health (Tshwane) Research Committee.
Data analysis
Statistical analysis was conducted using the Statistical Analysis Software (SAS) and the Statistical Package for the Social Sciences (SPSS) version 21. Crosstabs and Mann–Whitney U-tests were conducted to summarize the data and to evaluate sociodemographic comparability. The distribution of the neuropsychological performance scores was evaluated by means of the Kolmogorov–Smirnov test, skewness, and kurtosis (Pallant, 2010). Due to the assumption of normality within the distributions not being met (as is common in clinical data), the nonparametric alternative to the t-test (the Mann–Whitney U-test) was used to compare neuropsychological performance between the groups (Field, 2009). Due to the small sample size of the control group (n = 17), an additional nonparametric technique called the bootstrap resampling method was used (Chernick & LaBudde, 2011). Spearman’s rank-order correlation analysis was used to determine associations between clinical variables and neuropsychological performance in the HIV+ group.
Results
Sociodemographic variables
Sociodemographic variables (gender, employment, and ethnicity) are summarized in Table 1. Chi-square tests for contingency indicated a significant association between HIV and gender (χ2(1, n = 50) = 54.56, p < .001, phi = 1.005); however no significant association (χ2(1, n = 50) = .000, p = .995, phi = .044) was observed between HIV status and employment status. Comparisons using Mann–Whitney U-tests (Table 2) indicated no significant differences between the two groups with regard to years of education (p = .076) and age (p = .169). Groups were also comparable with regard to anxiety/depression scores, with no significant differences (p = .767) in self-reported mood states.
Demographic characteristics and chi-square statistics by HIV status.
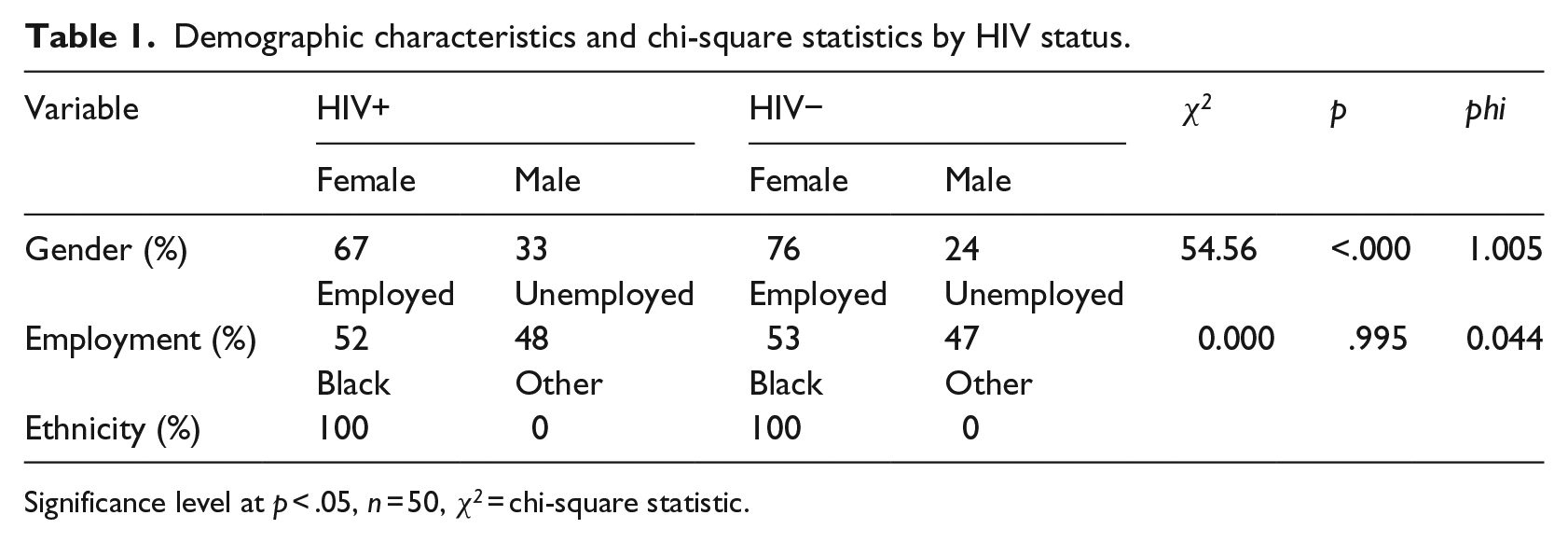
Significance level at p < .05, n = 50, χ 2 = chi-square statistic.
Descriptives and Mann–Whitney statistics for demographic characteristics.
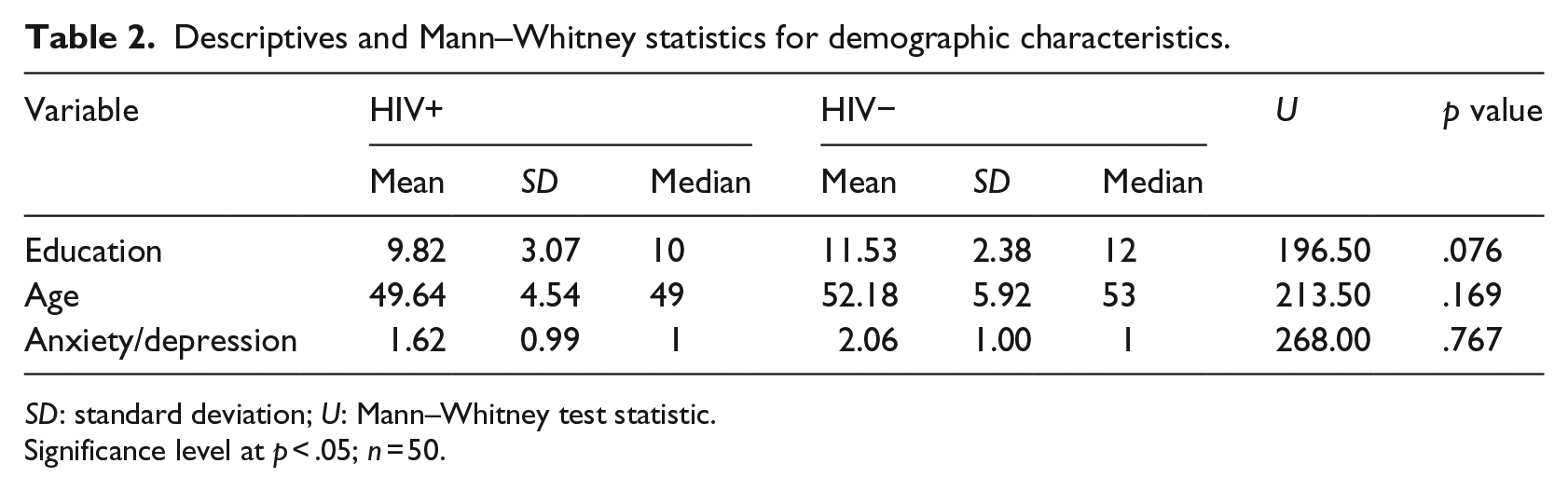
SD: standard deviation; U: Mann–Whitney test statistic.
Significance level at p < .05; n = 50.
Clinical variables
Chronicity (determined by means of the duration between earliest dated HIV+ test result and the date of neuropsychological examination) showed a mean and median of 42.24 months (SD = 37.55) and 31 months, respectively. Duration on antiretroviral medication (determined by means of the date given for antiretroviral therapy initiation and the date of neuropsychological examination) showed a mean and median of 43.18 months (SD = 42.53) and 26 months, respectively. The mean and median CD4 cell count was 415 cell/µL (SD = 231.60) and 403 cell/µL, respectively, with five individuals with a CD4 cell count under 200 cell/µL.
Correlational analyses found a moderate inverse association between duration on antiretroviral therapy and psychomotor processing (rs = −.33, p < .05). The number of months on antiretroviral therapy (duration) also demonstrated a moderate, positive association with the D-KEFS measure of task switching (rs = .40, p < .05). The descriptive neuropsychological performance by HIV status is reported in Table 3.
Descriptive neuropsychological performance scores by HIV status.
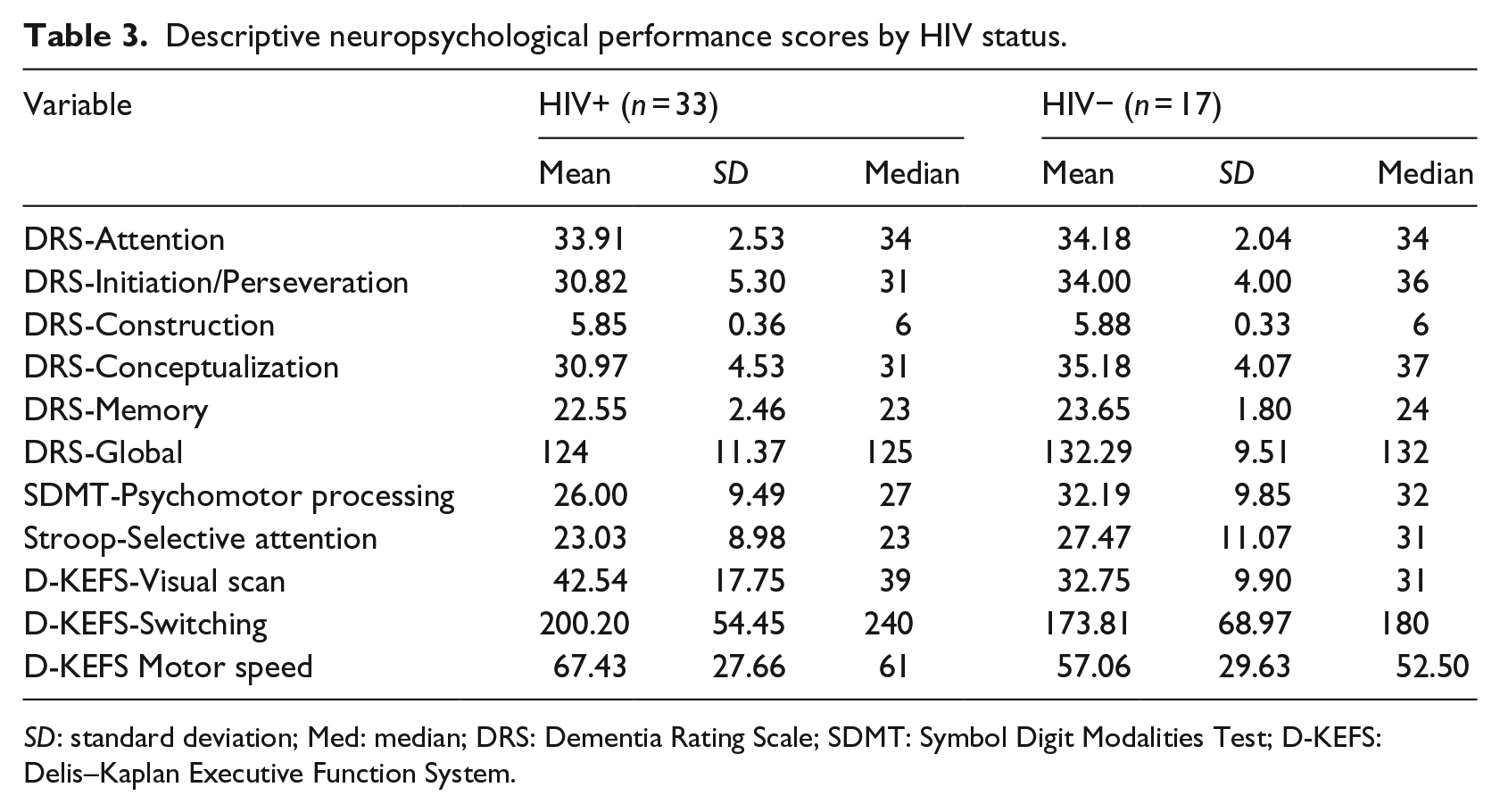
SD: standard deviation; Med: median; DRS: Dementia Rating Scale; SDMT: Symbol Digit Modalities Test; D-KEFS: Delis–Kaplan Executive Function System.
As shown in Table 4, the HIV+ group had poorer global neuropsychological performance in comparison to the HIV− group (p < .001, 95% confidence interval [CI] = [0.006, 0.098]). The executive function domain had the most statistical support for poorer performance by the HIV+ group in comparison with the HIV− group. This was evidenced by the following indicators: switching (p = .027, 95% CI = [0.138, 0.690]), initiation/perseveration (p < .001, 95% CI = [0.004, 0.093]), and conceptualization (p < .001, 95% CI = [0.002, 0.033]).
Comparative neuropsychological performance between the HIV+ and HIV− groups.
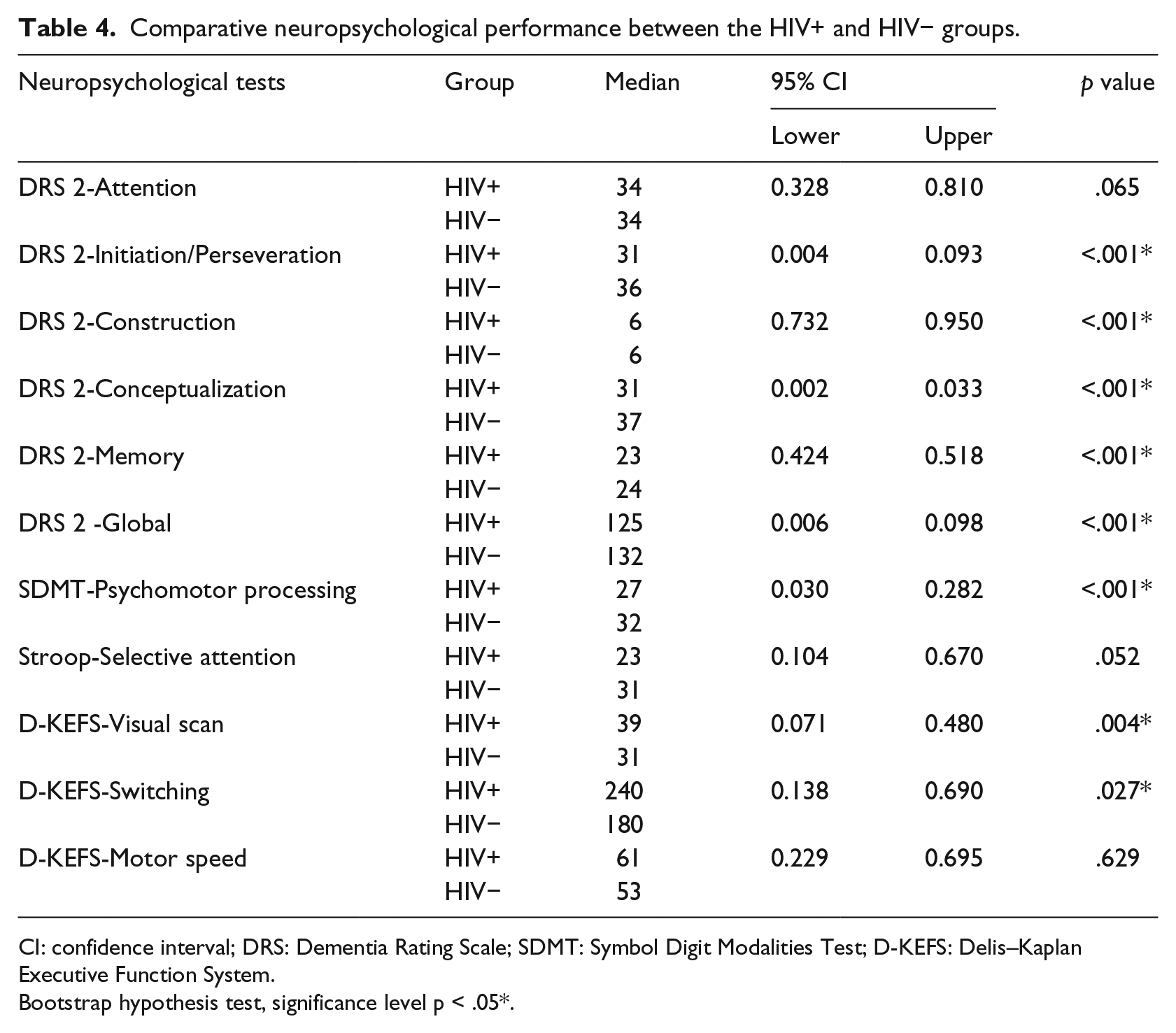
CI: confidence interval; DRS: Dementia Rating Scale; SDMT: Symbol Digit Modalities Test; D-KEFS: Delis–Kaplan Executive Function System.
Bootstrap hypothesis test, significance level p < .05*.
The HIV+ group showed statistically significant poorer performance than the HIV− group in psychomotor processing (p < .001, 95% CI = [0.030, 0.282]). Overall processing speed was significantly poorer for the HIV+ group as evidenced by the following tasks: psychomotor processing, visual scan, and switching. Performance in motor speed did not differ significantly for the two groups (p = .629, 95% CI = [0.229, 0.695]); however, a comparison across serostatus (Table 4) shows that the HIV+ group evidenced slower motor speed relative to the HIV− group.
A pattern of poorer performance was also observed in the memory domain (p < .001, 95% CI = [0.424, 0.518]). Variable results were observed for the attention domain where the HIV+ group performed significantly poorer than the HIV− group in a visual search measure of attention (p = .004, 95% CI = [0.071, 0.480]); however, performance on simple attention and complex attention tasks yielded no significant results.
Furthermore, a significant group difference in performance on the visuoconstructional domain (p < .001, 95% CI = [0.732, 0.950]) was observed.
Table 5 illustrates comparative global performance on the DRS-2 by age and education group for this study and the closest sample equivalent reported in the Schmidt et al. (1994) study. A one-sample t-test was conducted between the HIV− sample and the normative sample reported in Schmidt et al. (1994). Results indicated significantly poorer scores in global cognitive performance (t = 5.43; p < .001) in the HIV− group. Furthermore, the HIV+ group in the current sample also showed significantly poorer performance than the normative group (t = 8.44; p < .001).
Comparison of HIV− participant total DRS scores to age- and education-adjusted scores (Schmidt et al., 1994).
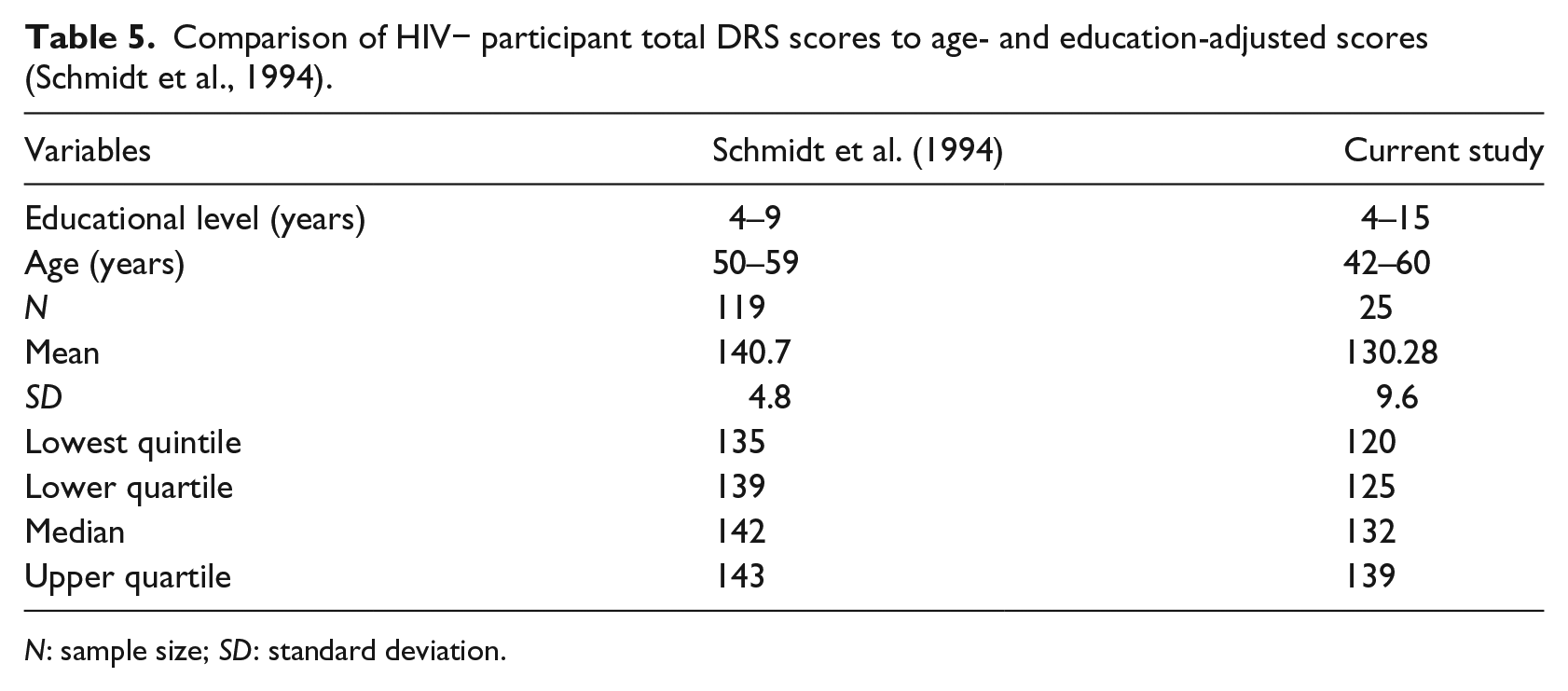
N: sample size; SD: standard deviation.
Discussion
The results presented above advance previous findings that adults and older adults with HIV evidence significantly poorer performance in cognitive domains of psychomotor speed, memory, visuoconstruction, and executive functioning when compared to seronegative adults (Fazeli et al., 2014; Sorlini et al., 2014). Global cognitive functioning in the HIV cohort was also significantly poorer than the age-matched HIV− control group. Although performance profiles were lower and response speed was slower on all attention tasks for the HIV+ group when compared to the HIV− group, simple attention (DRS-2) and selective attention (Stroop test) performance scores indicated no significant differences between the groups. These results are commensurate with findings on the cognitive profile in early stage HIV (Woods et al., 2009). In a study comparing neuropsychological functioning between a seropositive and seronegative group, Reger, Welsh, Razani, Martin, and Boone (2002) observed that effect sizes pertaining to group differences on tasks of attention and concentration increased as a function of disease severity.
Of particular interest is the performance variation in significant score patterns on different attention tasks. Woods et al. (2009) and Levine et al. (2008) espoused the idea that one domain of overlap on tasks measuring attention is psychomotor speed and speed of information processing. Given that impairment in various neuropsychological domains, particularly in speed of mental processing, has been observed in HIV+ adults and older adults, this aspect needs consideration when interpreting performance (Vance et al., 2013). In this study, performance on simple untimed and complex timed attention tasks without psychomotor demands (DRS-2 Attention and Stroop test) indicated no significant differences between the groups. On the tasks of attention requiring a psychomotor interface (D-KEFS-Visual scanning, D-KEFS-Switching, and SDMT), significant group differences were observed. The results may indicate that when processing demands are augmented (divided attention), HIV-associated psychomotor and cognitive functioning is attenuated (Grant, 2008). Multiple factors such as sensory modality through which the tasks are completed (visual/auditory), time pressure, psychomotor component, and complexity of task demands need to be considered when specifying and measuring the attention deficit in adults and older adults aging with HIV in the earlier disease stages.
The current investigation identified significant group differences in multiple cognitive domains. However, no significant difference in underlying component motor skills between the two groups was found. Poorer performance in psychomotor speed/information processing speed may not have emerged as secondary to basic motor slowing, but rather may indicate impairment in higher order cognitive processing capabilities (Woods et al., 2009).
Deficits in executive functioning are one of the foremost features in the neuropsychological profile of HIV (Dawes et al., 2008; Iudicello et al., 2012; Woods et al., 2009). In this study cohort, performance on specific executive functioning tasks (set shifting and graphomotor perseverative tests) that rely on psychomotor speed may be partially modulated by compromised functioning in that domain. Fellows, Byrd, and Morgello (2014) established that processing speed accounted for 77% of variability in executive functioning among HIV+ individuals and appears to notably mediate the influence of age-associated changes.
Results corroborated the association between duration on antiretroviral regimens and neuropsychological functioning that have been reported in several studies (Cross, Combrinck, & Joska, 2013; Kahouadji et al., 2013). Duration of time on antiretroviral therapy in an aging HIV population may potentiate the risk for central nervous system (CNS) neurotoxicity, which can compromise cognitive integrity and result in poorer outcomes on tasks requiring speed of mental processing (timed tasks). The participants’ adherence to medication use was not monitored, and these results on antiretroviral use have to be interpreted with this caveat.
According to Schmidt et al. (1994), the original Mattis Dementia Rating Scale (MDRS) shows a steady decline and a wider range of scores with decreasing educational levels. A significant, positive correlation was found between global DRS-2 scores and years of education, indicating that the DRS-2 scores in this study parallel the same trend in range of scores. However, analyses also indicated a significantly poorer cognitive performance in this study control group compared to the original MDRS sample. These comparisons suggest that although the normative and control group each show a decline in cognitive performance with decreasing educational levels, caution should be applied when using cut-off score determinants to categorize severity of impairment based on norms outside the South African context. Considering the sociodemographic parameters of participants in this study, particularly with regard to the quality and quantity of education status, further research utilizing larger sample sizes is required to determine the clinical utility of the DRS-2 in determining the severity of impairment in adults and older adults with HIV.
There are various limitations to this study. The length of the neuropsychological assessment and the specificity of the cohort being assessed resulted in a small sample size. The HIV+ group comprised individuals not older than 55 years, and future studies should include a wider age range to account for common neurological comorbidities in an older group. Due to incomplete medical records, the provision of a clearer clinical profile of the HIV+ participants was hindered. A more detailed assessment is required of psychiatric status as a potential mediator of neuropsychological outcomes in an older HIV+ cohort.
The recruitment procedure employed may have resulted in a selection bias, as the medical professionals were the first point of contact in approaching participants. However, due to the ethical parameters governing HIV participant recruitment, the main responsibility of the study was to protect the participants’ right to confidentiality, anonymity, and voluntary participation. Several challenges were encountered in ascertaining the HIV status of the participants. This was due to methodological aspects related to ethical issues pertaining to HIV. It is possible that some individuals in the HIV-negative sample may have been HIV positive. However, due to ethical constraints, the participants’ medical records were taken as the final authority in terms of sampling. The performance trend on the DRS-2 global score aligns with the focus of the current debate in the literature (Joska et al., 2011; Robbins et al., 2013) regarding the cultural appropriateness of using established neuropsychological test norms to determine the severity of HIV-associated neuropsychological impairment in the South African context.
Conclusion
In summary, the HIV+ group performed significantly poorer in comparison with the HIV− group on global neuropsychological functioning and specifically in cognitive domains of executive functioning, memory, psychomotor speed, and visuoconstruction. Compromised cognitive status in populations aging with HIV may confer increased risk for declining functional outcomes in activities of daily living, poor medication adherence, maintenance of clinic attendance, and lower overall health-related quality of life (Jacks et al., 2015; Moore et al., 2014; Rodriguez-Penney et al., 2013). Taken together with an aging HIV+ population in South Africa, studies focusing on neuropsychological functioning are essential for delineating the specific mental healthcare needs of this subgroup.
Footnotes
Funding
This work is based on research supported by the South African National Research Foundation (NRF).