
Abstract
Bipolar disorder is a psychiatric illness that is relatively common among patients presenting for treatment in primary care clinics. Physicians in primary care often face difficult decisions about how and when to intervene when a patient is experiencing depressive, manic, or hypomanic episodes consistent with bipolar disorder. This article reviews the literature on how to assess and diagnose bipolar disorder in primary care, and how to choose from the array of treatment options that exist. The psychotherapy and pharmacotherapy evidence base provides guidance on how to help patients effectively manage this ailment. Collaboration among health and mental health practitioners is key in helping manage the “peaks and valleys” of bipolar disorder. Special considerations need to be made to routinely assess for impulsivity, suicidality, and patient progress throughout the course of treatment.
Introduction
An estimated 2.3 million Americans meet the criteria for Bipolar Disorder. 1 This amounts to roughly 1.5% of the US population. In primary care settings, it is estimated that about 4% of patients currently have bipolar disorders 2 and up to 10% of patients will have been diagnosed with bipolar disorder at some point in their life. 3 These statistics speak to the need for primary care centers to have pathways in place to assist in assessing, diagnosing, and treating bipolar disorder. A collaborative effort among integrated care team members is essential for optimal long term management of bipolar disorder.
Assessment and diagnosis
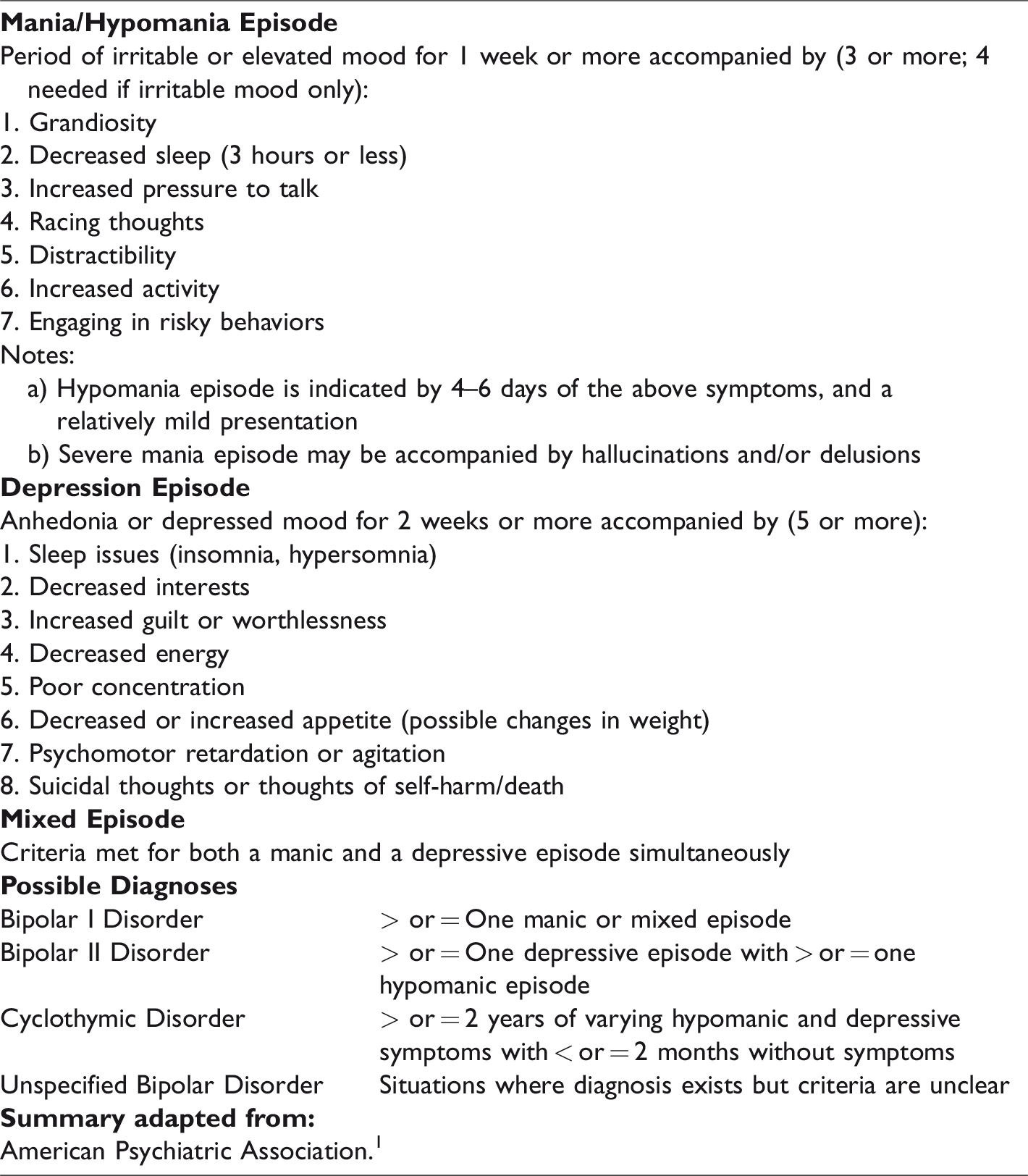
The assessment of bipolar disorder hinges on a sound clinical understanding of mood disorders. Mood disorders can range in severity and cover a spectrum from mild depression to severe bipolar disorder, sometimes with hallucinations and delusions. Bipolar disorder may include periods of mania, hypomania, and/or depressed mood (see Table 1), and the symptoms and criteria vary by diagnosis. A key part of assessment is determining the length of time that patients have had mood symptoms, and the severity of those presentations, so that an accurate diagnosis can be made. The average age of onset for bipolar disorder is generally in late adolescence or young adulthood. 4 People may experience the symptoms earlier or later in life, with early life symptoms generally indicative of poorer outcomes.
Summary of DSM-5 diagnostic features of bipolar disorder.
The proper assessment of bipolar disorder has four key ingredients: It should be thorough, structured, multimodal, and revisited throughout the course of treatment. 5 Information needs to be gathered regarding the patient’s childhood, school performance, and family life. Family physicians, due to their continuity with patients, are in a unique position to see changes over time, and to collect information from family members during appointments. It is helpful to utilize data from a behavioral health provider if one is available in the clinic. When a diagnosis is made, it should be provisional until the patient has been seen on several occasions, unless the patient has a clear cut documented history of bipolar disorder.
The diagnosis of bipolar disorder is fraught with pitfalls. Patients will often have symptoms of bipolar disorder for six to eight years prior to a formal diagnosis being made. 2 Furthermore, symptoms of bipolar disorder often overlap with other DSM-5 diagnoses such as depression, ADHD, schizophrenia, and substance use disorder. One helpful tool to use when diagnosing bipolar disorder is the Mood Disorder Questionnaire (MDQ). 6 The MDQ is a quick 15 item instrument with questions pertaining to bipolar disorder. The measure has good psychometric properties and screens out about 90% of patients who do not have bipolar disorder, while identifying roughly 70% of patients who do meet the criteria.
Clinicians should be cautioned that patients diagnosed with bipolar disorder have a lifetime risk of suicide far higher than the average person. Estimates indicate that up to 15% of patients diagnosed with bipolar disorder die by suicide. 7 Thus, during the assessment phase, patients should be asked openly about suicidal ideation, plans, and intent. Treatment can include inpatient psychiatric hospitalization for those who meet commitment criteria.
Non-pharmacologic treatments
Psychotherapy is an effective adjunctive treatment for bipolar disorder. Empirical support exists for several evidence-based psychotherapies including cognitive-behavioral therapy, interpersonal and social rhythm therapy, family focused therapy, group psychoeducation, and systematic care approach. Despite different theoretical orientations, these psychotherapies share several common treatment components including a) psychoeducation about the nature and course of the disease, b) problem-solving strategies to reduce stress, c) strategies to identify prodromal symptoms, and d) plans for intervention and treatment adherence. 8 Furthermore, psychosocial interventions have been shown to reduce symptoms, improve functioning, and maintain treatment adherence. 9
Psychoeducation is the foundation of psychotherapy for bipolar disorder. Comprehensive psychoeducation should include both the patient and family member(s). Clinicians should provide an overview of common symptoms, the nature and course of the disease, as well as treatment options. Psychoeducation should also include strategies to manage stress, methods for identifying early signs of recurrence, and self-management strategies to maintain a healthy lifestyle (e.g., sleep and exercise). 9
In addition, psychoeducation must emphasize the importance of adhering to pharmacotherapy. Due to high rates of patient non-adherence, maintenance of pharmacotherapy often becomes a primary focus of psychotherapy. 9 Clinicians are encouraged to review medication adherence and the treatment plan on a consistent basis. Often, clinicians are able to identify obstacles to adherence through mood tracking, which is a systematic approach to identifying a patient’s daily fluctuation in mood, sleep patterns, and daily stressors. This strategy allows a clinician to quickly identify a problem area and tailor the session to that specific problem. 8 Common problems in addition to medication non-adherence include impulsive behavior, poor sleep hygiene, and substance misuse. Further, clinicians may improve adherence by asking patients to reflect on life without medication, the consequences of not taking prescribed medications, and identifying social rhythms that may contribute to non-adherence. From there, subsequent sessions may focus on identifying warning signs for manic or depressive episodes and skills acquisition. In the final stages of psychotherapy, treatment should focus on relapse prevention and quality of life. 8
As previously mentioned, participation of family members is essential in the management of bipolar disorder. Clinicians are encouraged to provide family members with comprehensive psychoeducation on the course of the disease, common symptoms, treatment options, and symptom self-management strategies. Caregivers and family members are often crucial in identifying warning signs for recurrence and intervening when necessary. 9 In addition, family members should be included in the development of relapse prevention plans, as well as problem solving and communication enhancement strategies. One effective strategy is “the rule of two” which encourages patients to discuss with two family members or friends prior to engaging in certain decisions and behaviors. Importantly, family members may be asked to develop boundaries or consequences to encourage treatment adherence.
Lastly, in the case of acute bipolar mania, a patient should be assessed for the risk of harm to self or others, the duration of sleep deprivation and the presence of psychotic symptoms. When available, therapists should consult with psychiatry and transfer to a higher level of care when appropriate. In conclusion, psychotherapy should be considered and implemented when both feasible and accessible to the patient.
Pharmacotherapy
Pharmacotherapy combined with psychotherapy has been a mainstay of bipolar disorder disease management. 10 Decisions regarding the initiation of medication therapy hinge on the disease polarity and severity (see Table 2). For patients with acute mania, urgent titration of medications is needed to ensure patient safety, potential resolution of psychosis, and resumption of sleep cycles. Urgency is also needed for patients in acute mixed states or depressive states, due to the high risk for suicide. Acute titrations will typically require inpatient management to monitor treatment adherence and safety. Once the acute episode is resolved, shared decisions between physician, patient, and possibly family members will need to be made concerning maintenance. Bipolar mood disorders are episodic diseases, making evidence based studies difficult to perform, and making it harder to guide therapies for chronic management. Past observations have recommended maintenance medications to reduce social dysfunction, decrease mania episodes, and reduce suicidality. 11
Pharmacotherapy for bipolar disorder by polarity and disease course.
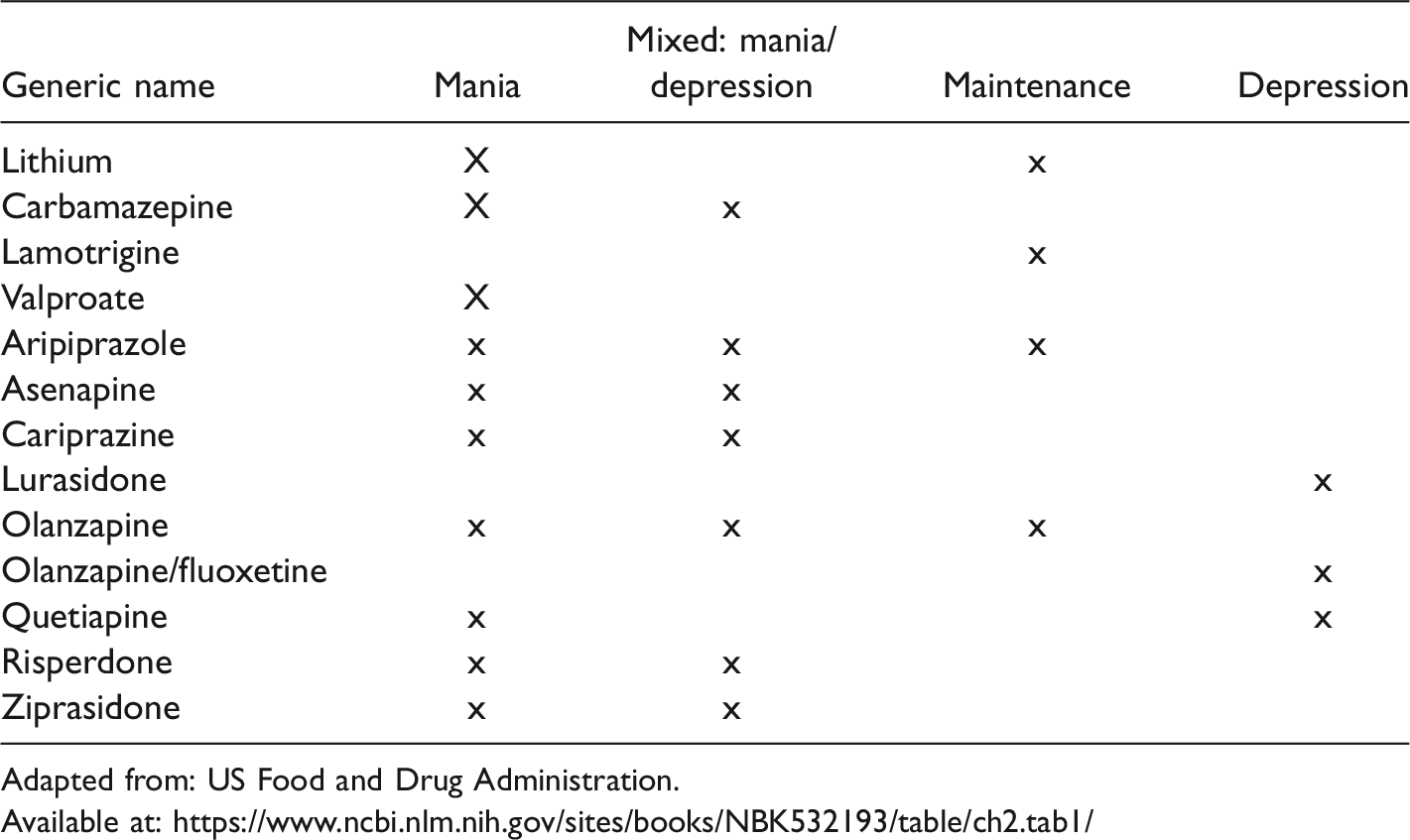
Adapted from: US Food and Drug Administration.
Patients with acute mania may present with severe agitation, violent behaviors, and psychosis. A rapid titration of medications in a secure setting is paramount to decrease potential harm to the patient and others. Intramuscular injections of antipsychotic medications, such as haloperidol, ziprasidone, olanzapine, and aripiprazole are options. Intramuscular lorazepam is an additional option. Oral medications used to treat bipolar disorder include lithium, valproate, aripiprazole, quetiapine, risperidone, ziprasidone, haloperidol, and benzodiazepines. Typical first line therapy includes lithium plus an atypical antipsychotic, or valproate plus an atypical antipsychotic. Lithium should be avoided in patients with bipolar mixed states or rapid cycling. Valproate should be avoided in pregnant patients or those who have liver disease.
The first step in the evaluation of depression in a patient with bipolar mood disorder is to assess for severity and safety. The potential for self-harm can be high. First line medications for acute depression include quetiapine and lurasidone. Second line therapies include valproate alone or in combination with quetiapine or lurisadone. Lithium can be used in combination with quetiapine, lurisadone, or valproate. A newer combination medication of olanzapine and fluoxetine is available. Bupropion in combination with a mood stabilizer is a third line option. Severe or refractory patients and patients with catatonia may require a referral for electro-convulsive therapy. 12
The pharmacotherapy maintenance of bipolar disorder is typically based on the effectiveness and tolerability of the medications used in the acute episode. For patients diagnosed with Bipolar Disorder I, the goal of medical therapy is to delay the recurrence of mania and lessen the severity of depressive episodes. 13 Lithium has been the mainstay of therapy and has the best data in relation to its effectiveness in delaying mania. Valproate and quetiapine are also options for maintenance therapy. The atypical antipsychotics aripiprazole, olanzapine, and risperidone are additional options for mood stabilization. Bipolar Disorder II is a burdensome illness of symptomatic chronic depression with acute flares. Lithium, lamotrigine, quetiapine, and olanzapine have shown efficacy in preventing depressive episodes. It is crucial that no matter the agent chosen, a stable therapeutic response should be in place before any traditional antidepressants be added as adjunct therapy. 13 This is especially true for patients at risk for mania episodes. Regardless of the agent or agents chosen, close follow-up is recommended. Lithium requires close monitoring for renal, thyroid, and parathyroid dysfunction. Valproate has potential to impact liver and hematologic abnormalities. The antipsychotics have known metabolic side effects of weight gain, elevated lipids and abnormal glucose metabolism, and those issues must be monitored. Careful titration of lamotrigine is needed to prevent adverse skin reactions.
Discussion
Patients with bipolar disorder are seen with regularity in primary care settings. It behooves primary care physicians to have pathways in place to assess, diagnose, and treat bipolar disorder. The four essential factors in the assessment and treatment of bipolar disorder include being thorough, structured, and multimodal with assessment; and then being cognitively open to revision of the diagnosis throughout treatment. 5 Clinicians also should routinely monitor patient risk for impulsivity and suicidality.
Pharmacotherapy for bipolar disorders are a necessary, yet difficult process. Medications must be tailored to the polarity and symptom complex, with clear established goals of therapy. Due to the episodic nature of bipolar disorders, a clear evidence-based treatment plan can be a challenge. Co-existing disorders and patient reluctance to adhere with long-term treatments are important factors that should be considered. The medications for bipolar disorders must be understood from the standpoint of effective therapy and potential adverse effects.
Primary care providers are in a unique role to assess, monitor and treat patients with bipolar disorder on an ongoing basis. Furthermore, the treatment of bipolar disorder is a team effort. When available, primary care doctors should encourage patients with bipolar disorder to engage in psychotherapy alongside pharmacotherapy. Evidence supports psychotherapy as an adjunctive therapy demonstrating improved outcomes in treatment adherence, symptom reduction, and improved quality of life. 8 Effective psychosocial interventions include psychoeducation about the disorder, treatment adherence strategies, and methods for identifying and intervening when prodromal symptoms are present. Additionally, psychotherapy should include family members and caregivers when at all possible and work in tandem with the pharmacotherapy goals.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.