
Abstract
Little is known about the implications of marital status for the age patterning of depressive symptoms in later life. Drawing on seven waves of data from the Hispanic Established Population for the Epidemiologic Study of the Elderly, this research uses growth curve models to examine age trajectories of depressive symptoms among continuously married and recently and continuously widowed older adults of Mexican descent (aged 65 years and older; N = 1,452). The findings demonstrate that despite having a higher mean level of depressive symptoms, the recently widowed experienced a similar rate of increase in distress with age to that of their married counterparts. Compared with the married, the continuously widowed had a steeper rise in depressive symptoms with age, although they had fewer symptoms at younger ages in later life. Physical health, financial strain, social support, and church attendance might account to a certain extent for marital status differences in depressive symptoms across later life.
Keywords
Introduction
Mental health issues might lead to higher levels of morbidity, disability, and premature mortality in later life (Blazer, 2003). In addition to other factors, marital status has important implications for the prevalence of depressive symptoms among older adults (Djernes, 2006). Specifically, widowhood might be related to elevated depressive symptomatology, relative to being married (Williams, 2004). However, since longitudinal research in this area is scarce, little is known about the implications of marital status for age trajectories of depressive symptoms in later life. Do widowed older adults follow the same general age patterning of mental health as their married counterparts? Does the duration of widowhood make a difference in older adults’ trajectories of depressive symptomatology with increasing age? Does the effect of widowhood become less pronounced at older ages in later life when spousal loss is a more common, predicted, and normative event? Also, prior research has not examined extensively whether such factors known to be associated with depressive symptoms as physical health, financial strain, social support, and church attendance can account for marital status differences in age-related trajectories of depressive symptoms among older adults.
There are several reasons why it is important to examine marital status differences in the age patterning of depressive symptomatology among older adults of Mexican descent in the United States. Hispanics comprise 16% of the U.S. population, with Mexican Americans accounting for two thirds of this largest ethnic minority group (Ennis, Ríos-Vargas, & Albert, 2011). Moreover, the Hispanic elderly population in the United States is expected to grow from its current level of 6% to 17% by 2050 (PEW Hispanic Center, 2008). In addition, older adults of Mexican origin have relatively high rates of depressive symptoms, especially among women (Black, Markides, & Miller, 1998). Moreover, Mexican Americans tend to experience greater levels of interdependency and interconnectedness among family members (Rodriguez, Mira, Paez, & Myers, 2007), and this cultural emphasis on embeddedness in family ties, including spousal relationships, might make a difference in the associations between marital status and depressive symptoms in later life. For instance, long-term widowhood might be more detrimental for mental health among older adults of Mexican descent than in other population groups. At the same time, close-knit extended families and easier access to family support among Mexican Americans might lead to lower increases in depressive symptoms among the recently widowed and to similar patterns of mental health among continuously widowed and continuously married older adults. Also, the implications of physical health, financial strain, social support, and church attendance for the association between marital status and depressive symptomatology may be particularly critical for older adult of Mexican descent, because of their relatively higher rates of chronic conditions and functional limitations, lower socioeconomic status, and greater reliance on social networks for assistance (Chiriboga, Black, Aranda, & Markides, 2002).
Drawing on seven waves of data from the Hispanic Established Population for the Epidemiologic Study of the Elderly (H-EPESE; 1993–2011), this research examines marital status differences in age trajectories of depressive symptoms among continuously married, recently widowed, and continuously widowed older adults of Mexican descent (aged 65 years and older; 5,813 person-periods). In addition, this study investigates whether physical health, financial strain, social support, and church attendance have implications for marital status differences in these age trajectories.
Duration of Widowhood, Gender, and Age
Self-reported depressive symptoms follow a U-shaped pattern over the life course. Namely, depressive symptoms tend to decline from young adulthood to middle age, but they start rising in later life, around age 65 to 70 (Wu, Schimmele, & Chappell, 2012). It should be noted, however, that prior research provides some contradictory findings on age-related changes in mental health in later life. In particular, the association between age and distress might be contingent on how mental health is measured. When a dichotomous indicator of major depression is used, research is more likely to show a lower prevalence of distress after age 65 compared with younger ages. In contrast, when a continuous measure of the number of depressive symptoms is utilized, distress is found to increase after age 65 (Patten et al., 2006). That is, a continuous measure of mental health might be better able to capture psychological distress in later life because although older adults might not reach the cut-off point for the diagnosable major depression, they might still experience elevated depressive symptomatology. At the same time, prior research argues that it is also important to consider age disparities in the diagnosable major depression in later life because even if it decreases after age 65, it might start increasing after age 80 (Wu et al., 2012).
The literature offers several key explanations for the age-related rise in distress among older adults, including health issues, financial problems, diminishing informal support and social activities, and changes in social roles such as widowhood (Yang, 2007). Specifically, compared with continuously married individuals, the widowed are at greater risk for lower psychological well-being (Carr, 2004; Chou & Chi, 2000b; Schaan, 2013). The life course perspective also indicates that it is crucial to take into consideration the impact of age on marital status differences in the mental health of older adults because the effect of any changes, especially stressful life events, on individuals’ psychological well-being can be contingent on age, timing, and a life stage (Elder, 1994). Age-related expectations, beliefs, and norms for social timing of life events can shape individuals’ reactions to these changes and perceptions of their consequences. For example, life events that occur at more predicted times in the life course can be linked to lower levels of depressive symptomatology. Overall, spousal loss might have a less detrimental influence on individuals’ mental health at advanced ages when it becomes a more common, predicted, and normative event which might be particularly true for older women because female life expectancy on average is higher than male’s (Moen, 1996). In contrast, the socioemotional selectivity theory implies that susceptibility to poor mental health among widowed individuals might increase at advanced ages (Carstensen, Isaacowitz, & Charles, 1999). Older adults’ social networks tend to shrink across later life mostly due to the death of relatives and friends and, as a result, spousal relationships may become more influential for individuals’ well-being with increasing age as older adults realize that their time is limited and start focusing on closer and more familiar social ties.
It is also critical to consider gender when examining marital status differences in depressive symptoms among older adults. Regardless of marital status, women, including women of Mexican descent, seem to have poorer mental health in later life than men (Black et al., 1998; Djernes, 2006). Yet, the results of previous studies on gender variations in the implications of widowhood for depressive symptomatology among older adults are mixed. Thus, some prior research demonstrates that the adverse consequences of the death of a spouse might be stronger among men (e.g., Choi & Bohman, 2007; Fry, 2001; Lee, DeMaris, Bavin, & Sullivan, 2001) or among women (e.g., Chou & Chi, 2000b), whereas other studies did not find any gender differences (e.g., Hagedoorn et al., 2006; Sasson & Umberson, 2014; Schaan, 2013).
In addition, theoretical frameworks and prior research demonstrate that it is important to account for the duration of widowhood when examining the role of spousal bereavement in individuals’ mental health. In other words, it is essential to differentiate between recently and continuously widowed persons. For example, according to the crisis perspective, the death of a spouse represents a short-term risk factor for mental health issues and its detrimental effects tend to disappear after 2 to 3 years (Hagedoorn et al., 2006). On the other hand, the chronic strain perspective argues that widowhood might have lasting adverse implications for psychological well-being because disadvantages related to spousal loss may accrue over time (Thoits, 2010). Yet, previous studies in this area are more likely to provide support for the crisis perspective indicating that compared with their continuously married counterparts, the recently widowed have elevated levels of depressive symptomatology, whereas the continuously widowed do not (e.g., Strohschein, McDonough, Monette, & Shao, 2005; Wilcox et al., 2003; Winter, Lawton, Casten, & Sando, 2000). It is unclear, however, whether the short- and long-term effects of widowhood remain equally influential for older adults’ psychological well-being across later life.
The majority of previous studies that have employed longitudinal data to disentangle the effect of the duration of widowhood or gender on individuals’ psychological well-being (e.g., Hewitt, Turrell, & Giskes, 2012; Strohschein et al., 2005) did not specifically examine the age-related dynamics in the interplay among these factors. At the same time, a few longitudinal as well as cross-sectional studies that considered the importance of age seem to suggest that widowhood might be more detrimental for mental health when individuals lose a spouse at younger ages in later life and remain widowed throughout later life. The death of a spouse at younger ages is more likely to be unexpected which might have adverse long-term implications for individuals’ psychological adjustment to this stressful event. For example, using a Swedish sample, Lichtenstein, Gatz, Pedersen, Berg, and McClearn (1996) found that among the recently widowed, the negative effect of spousal bereavement on psychological well-being was less harmful at older ages in later life. These age-graded differences did not exist among continuously widowed older adults, however (Lichtenstein et al., 1996). Similarly, Sasson and Umberson (2014) drew on a nationally representative sample of U.S. older adults from eight waves of the Health and Retirement Study and revealed that individuals who became widowed at younger ages in later life and stayed widowed were the most disadvantaged in terms of depressive symptomatology, compared with those who experienced spousal loss at older ages. Relatedly, utilizing cross-sectional data on older Koreans, Jang et al. (2009) examined age-group differences in the associations between marital status and depressive symptoms, although without controlling for the recency of widowhood. The results of the latter study did not reveal significant differences in psychological well-being between married and widowed women aged 75 to 85 years, although widows had more depressive symptoms at younger ages in later life. Yet, among older Korean men, the widowed reported greater psychological distress than the married across age-groups (Jang et al., 2009). Correspondingly, another cross-sectional research that drew on data from a three-generation study of Mexican Americans in San Antonio demonstrated that the effect of widowhood on depression might become less pronounced with age because the death of a spouse was linked to greater distress in middle age but it was not associated with more depressive symptoms in old age (Markides & Farrell, 1985).
It should be noted that previous longitudinal studies in this area used different numbers of waves with various intervals between data collections ranging from 3 months to 3 years. However, no specific patterns in the implications of the duration of widowhood or gender for depressive symptoms emerged as a result of these differences across previous studies.
Implications of Resources
The marriage protection perspective suggests that when examining the dynamics of depressive symptoms in later life, it is important to disentangle the effect of widowhood from the impact of other factors, including physical health, financial circumstances, social support, and religious involvement, that might vary by marital status (Murray, 2000). Moreover, these resources might shape not only marital status disparities in mental health but also age-related variations in depressive symptomatology. As discussed earlier, age might serve as a proxy for these factors that are considered to be critical predictors of mental health among older adults (Yang, 2007). Therefore, it is essential to examine whether these resources account for marital status differences in the age patterning of depressive symptoms in later life.
Prior research shows, for example, that chronic conditions (Wilcox et al., 2003) and functional limitations (van den Brink et al., 2004) are more prevalent among the widowed than the married. In addition, the literature provides evidence that these aspects of physical health can shape depressive symptomatology among older adults, including individuals of Mexican descent (Black et al., 1998; Chao, 2014; Chiriboga et al., 2002). Yet, prior research did not specifically examine whether higher rates of chronic conditions and functional limitations among the widowed can account for their poorer mental health relative to the married.
The literature also demonstrates that financial difficulties are more common among the widowed than the married (Arber, 2004; Umberson, Wortman, & Kessler, 1992). Moreover, perceived financial strain may have consequences for psychological well-being among older adults, including individuals of Mexican origin (Chiriboga et al., 2002; Chou & Chi, 2000a), and may at least partially account for poorer mental health among the widowed (Bierman, Fazio, & Milkie, 2006; Umberson et al., 1992; van Grootheest, Beekman, Broese van Groenou, & Deeg, 1999).
Furthermore, widowed individuals might experience changes in social support from family and friends which might increase, decrease, or stay the same during the first 3 years of widowhood (Guiaux, van Tilburg, & Broese van Groenou, 2007; Ha, 2010; Powers, Bisconti, & Bergeman, 2014). At the same time, greater levels of social support might be beneficial for older adults’ mental health (Ha, 2010; Han, Kim, Lee, Pistulka, & Kim, 2007). In addition, lower perceived social support can partially explain elevated depressive symptomatology among the widowed, compared with the married (Bierman et al., 2006; Hewitt et al., 2012).
Religions involvement, such as church attendance, might be beneficial for psychological well-being of older adults, including the widowed (Fry, 2001; Lee et al., 2001), because it might be related to stronger social networks and greater access to social support. Some prior research suggests that the widowed might attend church less frequently than the married (Fry, 2001; Lee et al., 2001). However, other studies reveal that religious involvement might also increase during the first 2 years after spousal loss because the widowed might use it as a coping mechanism (Brown, Nesse, House, & Utz, 2004). Although prior research did not extensively investigate the mediating role of religious involvement, one previous study shows that less frequent church attendance can account for higher distress among widowed men (Lee et al., 2001).
Hypotheses
On the basis of theory and prior research, I expect that regardless of marital status, older adults of Mexican descent will experience increases in depressive symptomatology with age (Hypothesis 1). Furthermore, I anticipate that relative to the continuously married, the recently widowed will have elevated depressive symptomatology (Hypothesis 2) and similar or even slower rates of increases in depressive symptoms with age (Hypothesis 3). However, I hypothesize that the continuously widowed will have similar initial levels of depressive symptomatology (Hypothesis 4) but steeper increases in depressive symptoms with age than the continuously married (Hypothesis 5). I also predict that the implications of widowhood for the age patterning of depressive symptoms will vary by older adults’ gender (Hypothesis 6). Following prior research, I expect that adjusting for physical health, financial strain, social support, and church attendance will account, at least partially, for marital status differences in age trajectories of depressive symptoms among older adults of Mexican origin (Hypothesis 7).
Method
Data
The analyses were based on seven waves of data from the H-EPESE. H-EPESE has an area probability, multistage sample of noninstitutionalized Mexican Americans aged 65 years and older, who reside in five southwestern states, including Texas, New Mexico, Colorado, Arizona, and California (Markides et al., 1996). The baseline data were collected in 1993–1994 on 3,050 individuals, with a response rate of 83%. Follow-up waves were collected at approximately two-year intervals: Wave 2 in 1995–1996 (n = 2,438), Wave 3 in 1998–1999 (n = 1,980), Wave 4 in 2000–2001 (n = 1,682), Wave 5 in 2004–2005 (n = 2,069), Wave 6 in 2007 (n = 1,542), and Wave 7 in 2010–2011 (n = 1,078). Wave 5 included interviews with new respondents aged 75 and over (n = 902) who were also reinterviewed during Waves 6 and 7. I excluded data from proxies obtained in H-EPESE when the sampled respondents were not available themselves due to illness, hospitalization, or temporary absence, Wave 1: n = 316 (10.36%); Wave 2: n = 271 (11.12%); Wave 3: n = 267 (13.48%); Wave 4: n = 204 (12.13%); Wave 5: n = 327 or 15.80%; Wave 6: n = 307 (19.91%); and Wave 7: n = 180 (16.70%).
For the purposes of the study, I included only those respondents who were married at Wave 1 for original respondents or at Wave 5 for new respondents and stayed continuously married or became widowed during the course of the survey. However, I excluded those respondents who were married at Wave 1 or Wave 5 but became separated or divorced during the course of the survey (between 0.52% and 1.67% across waves). Respondents also attrited between waves for several reasons, including death, Waves 2 to 3: n = 132 (10.84%); Waves 3 to 4: n = 237 (19.46%); Waves 4 to 5: n = 432 (29.75%); Waves 5 to 6: n = 561 (38.64%); and Waves 6 to 7: n = 740 (50.96%), and refusal to participate, Wave 2: n = 34 (2.79%); Wave 3: n = 46 (3.78%); Wave 4: n = 46 (2.95%); Wave 5: n = 67 (4.61%); Wave 6: n = 55 (3.79%); and Wave 7: n = 157 (10.81%). In addition, I did not include respondents with missing information on depressive symptoms (from 0 to .82% across waves). Thus, in the present analysis, I used the repeated observations from 1,452 respondents to create a data file of 5,813 person-periods. In the final sample, there were some statistically significant differences in the study variables between original and additional respondents. Namely, respondents added at Wave 5 were older, had more chronic conditions and ADL limitations, perceived greater social support, and were less likely to be immigrant and to die during survey (p < .001). Yet, original and additional respondents were not different in terms of depressive symptoms, gender, financial strain, and frequency of church attendance. Respondents who were widowed between waves were defined as recently widowed. If these widowed respondents participated in the next follow-up, they were identified as continuously widowed.
Measures
Immigrant status and gender were treated as time-invariant variables measured at Wave 1 or Wave 5, whereas the rest of the variables were used as time-varying ones measured at each wave. To facilitate the interpretation of results, I centered study variables, so that zero indicated the average value on each measure (Singer & Willett, 2003). Missing values on all independent and control variables were handled using the Stata command mi impute for multiple imputation. Most variables had less than 2% of missing values.
Depressive symptoms were measured at each wave with the Center for Epidemiologic Studies Depression Scale (Radloff, 1977). In H-EPESE, this scale contains 20 items, including 16 negative affects (e.g., I felt depressed) and 4 positive affects (e.g., I felt hopeful about the future). For each item, respondents reported how often they had a particular feeling in the previous week (0 = rarely or none of the time, 3 = most or all of the time). The responses for the positive affect items were reverse coded. The total score of the Center for Epidemiologic Studies Depression Scale was used as a continuous measure (α = .84 to .96, depending on wave).
Age at each wave was measured in years and centered at 65, the lowest observed age. Age was used as a measure of time in growth curve models. Woman was a dichotomous variable (0 = no, 1 = yes).
Marital Status
The continuity and change in marital status between waves was captured with three dummy variables: continuously married (reference category), recently widowed, and continuously widowed (0 = no, 1 = yes). Respondents were labeled as continuously married if they were married at Wave 1 (or at Wave 5 for additional respondents) and stayed married throughout follow-ups. Those respondents who became widowed between waves were defined as recently widowed. Continuously widowed respondents refer to those individuals who were widowed at the next follow-up after becoming widowed at the previous wave. Because information on the duration of marriage and age at widowhood is not available in H-EPESE and because waves of H-EPESE have been conducted at approximately 2-year intervals, I was not able to provide more detailed distinctions between recently and continuously widowed individuals. However, the majority of prior longitudinal studies in this area also had to rely on similar differentiations among the widowed and to analyze stability and change in mental health drawing of data with at least 2-year intervals between waves (e.g., Choi & Bohman, 2007;
Chronic conditions captured how many of the following conditions a respondent had at each wave: heart attack, stroke, hypertension, diabetes, cancer, and arthritis (0 to 6). This measure was based on respondents’ reports on whether they had ever been, or since the last interview, told by a doctor that they had these health issues. ADL limitations, ranging from 0 to 7, reflected the number of the following activities that a respondent could not perform at each wave without any help from a person or special equipment or device: walking across a small room, bathing, personal grooming (i.e., brushing hair, brushing teeth, or washing face), dressing, eating, getting from a bed to a chair, and using the toilet.
Financial strain at each wave captured whether the respondent had problems paying monthly bills (1 = none, 4 = a great deal). Social support at each wave was a mean scale constructed from two questions asking how often the respondent could count on and talk about problems with family and friends in times of need (α = .69 - .86, depending on wave). All responses were recoded so that higher values indicated greater perceived support (1 = hardly ever, 3 = most of the time). Church attendance at each wave measured how often the respondent went to religious services (1 = never or almost never, 5 = more than once a week).
Controls
Prior research indicates that it is important to consider individuals’ immigrant status because it might be a risk factor for elevated depressive symptomatology among older adults. Specifically, being foreign-born might be associated with lower levels of socioeconomic resources, acculturation, and social integration and as a result, it might lead to additional stress and anxiety throughout the life course (Ladin & Reinhold, 2013). Immigrant was a dichotomous variable (0 = no, 1 = yes) created on the basis of respondents’ reports on their place of birth (i.e., whether they were born in the United States). Died during survey (0 = no, 1 = yes) was also included into the analyses to control for the panel attrition due to the death because it was related to more depressive symptoms among respondents. I also created two extra variables to take into consideration the varying length of participation among respondents. Specifically, added at Wave 5 accounted for new respondents at Wave 5. Moreover, I included measurement occasions to control for the number of waves of H-EPESE in which each respondent was interviewed (for a similar approach, see Brown, O’Rand, & Adkins, 2012).
Analytic Strategy
Descriptive statistics by marital status for repeated observations of all study variables are presented in Table 1. Marital status differences in means were examined with t tests. Zero-order correlations (not shown) confirmed that none of the correlations among the independent and control variables exceeded .60.
Means (Standard Deviations) for Study Variables by Marital Status ( N = 5,813 Person-Periods).
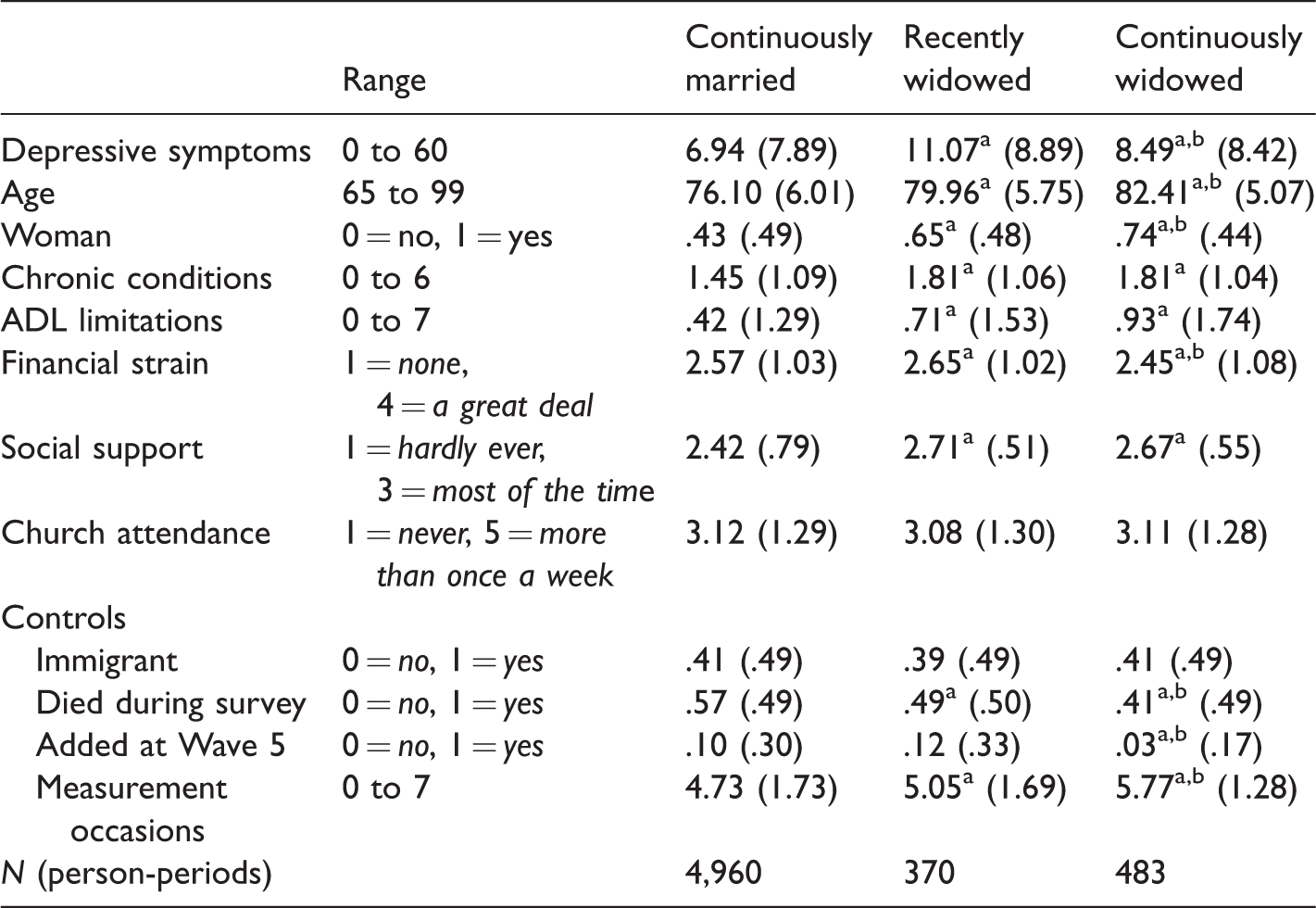
Note. Descriptive statistics are based on noncentered variables. Means for dichotomous variables can be interpreted as the proportion of the observations coded 1 on a specific variable. t-tests were computed for difference in means. Source: 1993–2011 H-EPESE.
aStatistically significant difference between continuously married and recently or continuously widowed at the .05 level.
bStatistically significant difference between recently widowed and continuously widowed at the .05 level.
Because I used panel data, I employed growth curve models to assess marital status differences in age trajectories of depressive symptoms. This analytic method estimates a single model with two levels (Singer & Willett, 2003). Individual trajectories of change are presented at Level 1. This level specifies an intercept, which is, in this analysis, an average level of respondents’ depressive symptoms at age 65 (the youngest age), and a slope, which is an average rate of change in respondents’ depressive symptoms with increasing age. The variance in trajectories of change between individuals is estimated at Level 2. At this level, the random effects for the intercept indicate whether respondents vary in their levels of depressive symptoms at age 65, whereas the random effects for the slope determine whether there are interindividual variations in the rate of change in respondents’ psychological well-being with increasing age.
I applied Stata xtmixed procedure with maximum likelihood estimation which is appropriate for analyzing panel date with attrition. I started with Level 1. First, I modeled a linear change trajectory of depressive symptoms of individual i at time t (DS
ti
), as a function of age (Age
ti
). I did not include a quadratic term for age because likelihood-ratio tests of linear and quadratic models provided a better empirical fit to the data for a linear growth curve. I then included my main independent variables, capturing each marital status group n (MSG
nti
). I specified continuously married individuals as a reference group. To examine whether the marital status effect on the individual’s depressive symptoms can vary by age, I added the interaction terms between age and each marital status group n. The Level 1 equation is presented as follows:

At Level 2, the two submodels of the intercept π0i and the linear rate of change π1i examine the between-individual variations in the age trajectory of depressive symptoms:


In these submodels, β 00 and β 10 are the average level of depressive symptoms and the average linear rate of change in the age trajectory, respectively. Random error terms of the average intercept and the average linear rate of change of the age trajectory are presented with ς 0i and ς 1i , respectively.
The combined model of the Level 1 and Level 2 submodels was written as follows:

This model is included in Model 1 in Table 2. Model 1 estimated the direct effect of recent and continuous widowhood relative to being continuously married.
Marital Status Trajectories of Depressive Symptoms Among Older Mexican Americans: Influence of Health, Financial Strain, Social Support, and Religion (N = 5,813 Person-Periods).

Source: 1993–2011 H-EPESE.
aReference category: continuously married.
*p < .05. **p < .01. ***p < .001 (two-tailed tests).
To consider whether the implications of widowhood for the age patterning of depressive symptoms can depend on older adults’ gender, I included two-way interaction terms between age and gender and between each marital status group and gender and three-way interaction terms between each marital status group, gender, and age in Model 2 in Table 2. The goal of this study was also to examine whether physical health, financial strain, social support, and church attendance account for marital status differences in the level and rate of change in individuals’ depressive symptoms. Models 3 to 6 added health status (including chronic conditions and ADL limitations), financial strain, social support, and church attendance, one by one, to assess whether these factors account for marital status differences in age trajectories of depressive symptoms. Model 7 presents a full model, in which all factors from Models 3 to 6 are introduced simultaneously. All the models control for immigrant status, attrition due to death, added at Wave 5, and measurement occasions. Because H-EPESE contains marital dyads, I also created a flag variable to control for the dyadic nature of the sample. However, supplementary analyses (not shown) indicated that this variable was not a statistically significant predictor of depressive symptoms and the inclusion of this variable did not change the results. Therefore, I did not include this flag variable in the final analyses.
Results
Descriptive Results
As can be seen from Table 1, there were several statistically significant marital status differences among older individuals of Mexican descent. Compared with their continuously married counterparts, recently and continuously widowed individuals reported, on average, more depressive symptoms, with the recently widowed having the highest number of depressive symptoms. The widowed were older than the continuously married. There were more women among the recently and continuously widowed than among the continuously married. Relative to the continuously married, the recently and continuously widowed had more chronic conditions and ADL limitations. The recently widowed had greater financial strain, whereas the continuously widowed reported lower financial strain than the continuously married. Regardless of the recency of spousal death, widowed individuals perceived greater social support than their continuously married counterparts. However, older adults of Mexican descent reported similar frequency of church attendance across marital status groups.
Results From Growth Curve Models
Model 1 in Table 2 examines marital status differences in age trajectories of depressive symptoms among older individuals of Mexican descent. The estimates for the intercept and linear slope for each marital status group should be interpreted together. To facilitate the interpretation of the results, I present the predicted age trajectories for each marital status group in Figure 1. In Model 1, a positive and statistically significant linear slope (.053, p < .05) suggests that the continuously married experience increases in depressive symptoms with age. Also, women on average have more depressive symptoms than men. In addition, compared with the continuously married, the recently widowed have more depressive symptoms on average (positive and statistically significantly intercept) and similar rate of increase in depressive symptomatology with age (not statistically significant linear slope). However, the continuously widowed have a steeper increase in depressive symptoms with age (positive and statistically significant linear slope), in spite of their initial advantage in psychological well-being (negative and statistically significant intercept) related to the continuously married. Model 2 suggests that there are no gender differences in the implications of widowhood for age trajectories of depressive symptoms among older adults of Mexican origin because the two-way interaction terms between marital status groups and gender and three-way interaction terms between marital status groups, gender, and age are not statistically significant.
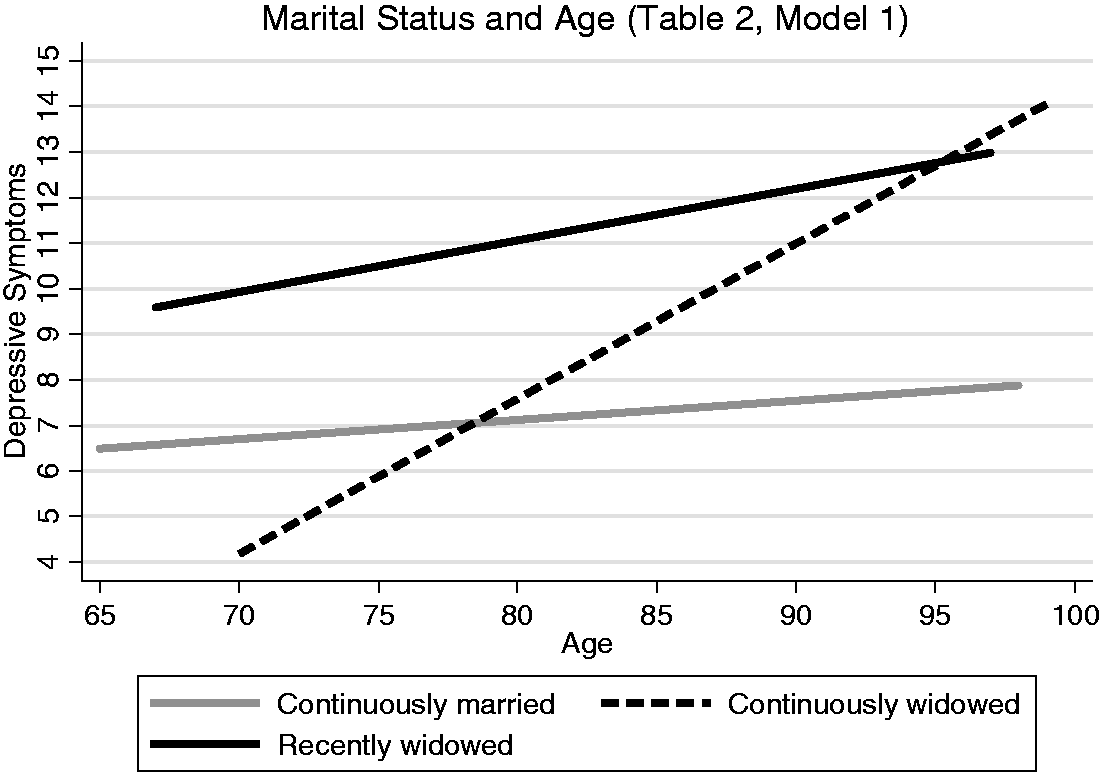
Age trajectories of depressive symptoms by marital status groups.
Models 3 to 6 investigate one by one the role of physical health, financial strain, social support, and church attendance. The models indicate that these factors independently predict psychological well-being among older adults of Mexican descent and might have implications for marital status differences in the age patterning of depressive symptoms. More chronic conditions and ADL limitations (Model 3) and greater financial strain (Model 4) are related to more depressive symptoms, whereas stronger social support (Model 5) and more frequent church attendance (Model 6) are associated with better mental health. Model 3 in Table 2 shows that when physical health is accounted for, the linear slope for the continuously married and the intercept for the recently widowed are decreased to nonsignificance, whereas the continuously widowed become less advantaged in initial levels of mental health but experience a slower increase in depressive symptoms with age. With the inclusion of financial strain, the intercept for the recently widowed is again reduced to nonsignificance, whereas a larger negative estimate for the intercept for the continuously widowed implies even greater initial advantage in mental health compared with the continuously married (Model 4). Models 5 and 6 demonstrate that social support and church attendance, respectively, might have a suppressor effect for the initial levels of depressive symptoms among the widowed. Namely, the recently widowed would have higher initial levels of depressive symptoms, whereas the continuously widowed would be less advantaged in initial levels of mental health, if they did not have greater social support or if they went to church less frequently. In addition, adjusting for church attendance is associated to a nonsignificant linear slope for the continuously married, whereas controlling for social support and church attendance is related to a slower increase in depressive symptoms with age among the continuously widowed.
Model 7 is a full model. When physical health, financial strain, social support, and church attendance are added to the model simultaneously, the linear slope for continuously married becomes nonsignificant, whereas the recently widowed have even higher average levels of depressive symptoms and the continuously widowed are less advantaged in mental health initially but experience a slower increase in depressive symptomatology with age.
Discussion
Widowhood, particularly recent spousal loss, tends to be associated with poorer mental health among older adults. Yet, little is known about the age patterning of marital status differences in depressive symptoms in later life. The present study investigated age trajectories of psychological well-being among continuously married, recently widowed, and continuously widowed older adult of Mexican descent. Moreover, this study considered whether gender can make a difference in the implications of widowhood for the age patterning of depressive symptoms. In addition, this study examined whether physical health, financial strain, social support, and church attendance can account for marital status differences in age trajectories of depressive symptoms in this population group.
Age Trajectories by Marital Status
In line with the literature and Hypothesis 1, the present study indicates that mental distress might increase across later life, regardless of marital status (Wu et al., 2012). The findings of the present study also demonstrate that the duration of widowhood matters for the age patterning of depressive symptoms among older adults of Mexican descent. Compared with their continuously married counterparts, the recently widowed had higher levels of depressive symptoms which is consistent with Hypothesis 2. Also, the recently widowed had a similar rate of increase in depressive symptomatology with age which partially supports Hypothesis 3 and is in accord with the life-course perspective implying that the death of a spouse might not be necessarily related to greater distress when spousal loss occurs at more normative or predicted times for this stressful event (Elder, 1994). In contrast, despite their advantage in psychological well-being at younger ages in later life, the continuously widowed experienced a steeper increase in distress with age than the continuously married. The former finding provides partial support for Hypothesis 4 and the latter one is in accord with Hypothesis 5. That is, the present study suggests that although widowhood is an anticipated event at more advanced ages (Moen, 1996), long-term widowhood might become more detrimental for individuals’ mental health with increasing age. The results on the continuously widowed are congruent with the socioemotional selectivity theory that highlights the growing significance of marital ties for the psychological well-being of older adults across later life (Carstensen et al., 1999). In addition, these findings imply that among the continuously widowed, the crisis perspective appears to be more applicable to younger ages in later life, whereas the chronic strain perspective is more relevant to older ages in later life. The findings of the present study seem to be in line with Sasson and Umberson’s (2014) research suggesting that among U.S. older adults, long-term widowhood after losing a spouse at younger ages in later life might be related to poorer mental health than becoming widowed at older ages. At the same time, the present results are inconsistent with the findings of Lichtenstein et al. (1996) who found that recent widowhood was more distressing for older Swedish adults at younger ages in later life, whereas the effect of continuous widowhood for individuals’ psychological well-being did not vary by age.
Gender
Consistent with prior research across racial and ethnic groups (Black et al., 1998; Djernes, 2006), this study shows that among older Mexican Americans, women on average had more depressive symptoms than men. Gender, however, did not make a difference in the interplay among the duration of widowhood, psychological well-being, and age which contradicts Hypothesis 6. These findings are in accord with some previous studies arguing that the consequences of recent or continuous widowhood on individuals’ distress do not vary by gender in the United States and different European countries (e.g., Hagedoorn et al., 2006; Sasson & Umberson, 2014; Schaan, 2013). Yet, other prior studies suggest that widowhood can have a stronger adverse effect on men’s mental health in the United States and Canada (e.g., Choi & Bohman, 2007; Fry, 2001; Lee et al., 2001). Furthermore, one previous cross-sectional study on older Koreans demonstrated that gender might play a role in the age-group differences in the linkages between marital status and depressive symptoms (Jang et al., 2009). In the latter study, widowed older Korean men reported lower psychological well-being than their married counterparts across age-groups, whereas widowed women reported more depressive symptoms than married women only at younger ages in later life.
The Role of Resources
The present study demonstrates that physical health, financial strain, social support, and church attendance are important for depressive symptomatology among older adults of Mexican descent and, to a certain extent, might have implications for marital status differences in the age trajectory of psychological well-being in this population group which is in accord with Hypothesis 7. In line with prior research across different countries and cultures, the findings of this study show that among Mexican Americans, widowed older adults have more chronic conditions (Wilcox et al., 2003) and functional limitations (van den Brink et al., 2004) and that these aspects of physical health can be related to individuals’ psychological well-being (Black et al., 1998; Chao, 2014; Chiriboga et al., 2002). However, the present study expands upon previous studies in this area by demonstrating that physical health might account for the age-related increase in depressive symptoms among the continuously married as well as higher levels of distress among the recently widowed, although it only partially explains a steeper rise in depressive symptoms with age among the continuously widowed.
Consistent with prior research in various cultures, this study indicates that financial strain can have negative implications for older adults’ psychological well-being (Chiriboga et al., 2002; Chou & Chi, 2000a). Previous studies using data from the United States and Great Britain also suggest that compared with the married, the widowed might have more financial difficulties (Arber, 2004; Umberson et al., 1992). In the present study, compared with the continuously married, only recently widowed individuals reported greater financial strain, whereas the continuously widowed had lower levels of financial hardship. Some prior research also implies that financial problems among widowed Americans might decline over time (Umberson et al., 1992). Additionally, similar to physical health, financial strain in the present study accounted for greater levels of depressive symptoms among the recently widowed. Several previous studies in the United States and the Netherlands also show that the mental health disadvantage among the widowed might be explained by limited financial resources (Bierman et al., 2006; Umberson et al., 1992; van Grootheest et al., 1999). It should be noted that the present study did not consider income because information on household and individual incomes was not available at all waves of H-EPESE. However, according to prior research on various racial or ethnic groups in the United States, not only objective (e.g., income) but also subjective (e.g., financial strain) indicators of economic resources are important predictors of psychological well-being among older adults, including Mexican Americans (e.g., Chiriboga et al., 2002).
In the present study, recently and continuously widowed Mexican Americans perceived greater social support from family and friends than their married counterparts. These findings concur with prior research indicating that informal support might increase following the death of the spouse in the United States and the Netherlands (Guiaux et al., 2007; Ha, 2010). Yet, the findings on the similar levels of social support reported by the recently and continuously widowed contradict previous studies in the United States and the Netherlands that found decreases in social support after about the first 2 years of spousal bereavement (Guiaux et al., 2007; Powers et al., 2014). At the same time, older adults of Mexican descent in the present study also reported the same frequency of church attendance across marital status groups whereas prior research in the United States and Canada shows that following the death of the spouse, church attendance might decrease (Fry, 2001; Lee et al., 2001) and increase (Brown et al., 2004). However, consistent with prior research in the United States, Canada, and Australia, lower levels of depressive symptomatology in the present study were more prevalent among older adults of Mexican descent with greater social support (Ha, 2010; Han et al., 2007) and more frequent church attendance (Fry, 2001; Lee et al., 2001).
In addition, previous studies across different countries, including the United States and Australia, demonstrate that the disadvantages in psychological well-being among the widowed relative to the married can be at least partially accounted for by lower levels of perceived informal support (Bierman et al., 2006; Hewitt et al., 2012) and less frequent church attendance (Lee et al., 2001) after the death of a spouse. The findings of the present study, however, suggest that social support and religious involvement might have a suppressor effect on the age patterning of psychological well-being among the widowed. Specifically, the recently widowed would have reported even greater levels of depressive symptoms and continuously widowed would have been less advantaged in mental health initially if they had not had high levels of social support and if they had not attended religions services as frequently as they did. Greater perceived social support and more frequent church attendance were also predictive of a slower rate of increase in depressive symptoms with age among continuously widowed Mexican Americans.
Overall, it should be noted that previous studies in this area did not specifically examine racial or ethnic differences as well as variations across countries and cultures in the implications of resources for older adults’ mental health, in general, and for the marital status disparities in age trajectories of depressive symptoms in later life, in particular. Therefore, it is not possible to conclude whether the results of the present study on the importance of resources are applicable only to older Mexican Americans or might be relevant to older adults from other racial or ethnic or cultural groups. Future research, however, would benefit from clarifying potential cross-cultural variations in the interplay among marital status, resources, age, and depressive symptoms.
Limitations
There are several factors that I was unable to take into consideration because of data limitations. For example, I did not examine short-term bereavement effects because the duration of marriage and specific date of the death of a spouse are not available in H-EPESE and because there are approximately two-year intervals between waves of data collection in H-EPESE. In addition, I did not account for contact frequency within social networks or the quality of social ties among older adults of Mexican descent. Future research would also benefit by considering whether the linkages between recent widowhood and depressive symptomatology differ by the cause of spousal death, the quality of marital relationship, and caregiving exchanges between older spouses. For instance, prior research suggests that better marital relationships pre-widowhood might lead to poorer mental health post-widowhood (Schaan, 2013). At the same time, spousal caregivers, particularly long-term ones, might experience less considerable increase in distress after the death of a spouse (Carr, 2004). Yet, when a spouse had a painful death, the widowed might report especially low psychological well-being (Carr, 2003). Moreover, prior research points out that additional factors such as personality and coping skills that were not considered in the present research might make a difference in the association between widowhood and depressive symptoms. For example, these factors might include personality traits such as optimism, spirituality, and insecurity (Brown et al., 2004; Montpetit, Bergeman, Bisconti, & Rausch, 2006; Fry, 2001); pre- and post-widowhood health behaviors (e.g., physical exercise and smoking) and social engagement (e.g., volunteering; Choi & Bohman, 2007); and post-widowhood strains related to domestic chores and housekeeping tasks (Lee et al., 2001; Umberson et al., 1992; van Grootheest et al., 1999).
Conclusion
The main contribution of this study is that it examines the implications of marital status for the age patterning of depressive symptomatology among older adults of Mexican descent. The findings indicate that compared with a cross-sectional study, a longitudinal analysis provides a more complex depiction of marital status differences in age trajectories of individuals’ psychological well-being. The present study highlights the importance of being married and the duration of widowhood for mental health in later life. Despite having a higher mean level of depressive symptoms, recently widowed Mexican Americans experienced a similar rate of increase in distress with age to that of their married counterparts. In contrast, relative to the married, continuously widowed Mexican Americans had a steeper rise in depressive symptoms with age although they had fewer depressive symptoms at younger ages in later life. Adjusting for physical health, financial strain, social support, and church attendance accounted to a certain extent for the marital status disparities in depressive symptoms in this population group. Relatedly, the present study suggests that effective interventions after spousal loss should include programs focusing on enhancing physical health, social support, and religious involvement and managing financial hardships among older adults of Mexican descent.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.