
Abstract
Alcohol and other drug testing is used in a range of environments including workplaces, schools, sporting tournaments, substance treatment and criminal justice system settings. It is also the cornerstone of the drug court model. Despite its centrality, it has received little scholarly attention. In this article, we address this gap through a study of how the drug-testing regime unfolds at one Australian drug court. Based on ethnographic observation, qualitative interviews with drug court participants, and analysis of drug court documents, this article examines how participants experience drug testing. Drawing on Carol Bacchi’s poststructuralist policy analysis framework, we examine how the “problem” of substance “dependence” is conceptualized in one drug court’s approach to drug testing, and we consider some of the effects of the policy. We argue that the everyday and seemingly mundane ritual of urination becomes a core technique for the governance of drug court subjects and note that the testing regime is onerous, regimented, and invasive. We also trace some of the effects of this policy and its implementation for participants. We suggest that the urine-testing regimen might operate counterproductively, intensifying participants’ involvement with the criminal justice system. Its reliance on an abstinence model may heighten exposure to substance-related harms and segregate drug court participants from the “rest of society,” inhibiting other aspects of their lives, including their relationships and employment prospects. Overall, we argue that these effects are at odds with the stated purposes of the drug court. We conclude with some reflections on claims about the therapeutic value and potential of drug courts and suggest opportunities for reform.
Originally used in the military with returned Vietnam veterans (Campbell, 2005; Paik, 2006), alcohol and other drug testing has since extended to a variety of environments. It is now used in employment (American Society of Addiction Medicine, 2013), schools (Mosher & Akins, 2014), sports (Wilson & Derse, 2001), social services (Wincup, 2014), child custody (Campbell, 2005), addiction treatment (Rzetelny et al., 2016), and in the criminal justice system (Powell, Bankart, Christie, Bamber, & Arrindell, 2009; Seddon, 2005; Singleton, 2008; Wish & Gropper, 1990). According to Wish and Gropper (1990), this testing achieves four goals in the criminal justice system: detection of recently ingested substances, identification of “chronic” alcohol and other drug users, monitoring and deterrence of consumption among those on parole or community-based justice system populations. Testing is also the cornerstone of many drug court models. Drug court advocates identify several advantages of testing in a drug court environment: deterrence to drug use, identification of individuals who are abstinent for allocation of incentives or rewards, and identification of relapse, allowing for swift intervention and effective use of limited resources by targeting those participants who continue to use substances (Auerbach, 2007; Cary, 2011). Despite the centrality of testing to the drug court model, it has not received much scholarly attention. In this article, we add to the research in this area through a detailed study of testing regimes at one Australian drug court. In what follows, we provide an overview of the Drug Court of Victoria’s testing regime. Next, we discuss the critical literature on drug courts with a special emphasis on studies of drug-testing regimes in drug courts. Third, we provide an overview of the aspects of Bacchi’s (2009) policy analysis framework that we draw on in our analysis. Following this, we analyze drug court participants’ experiences with its drug-testing regime, including experiences of random testing and urine collection, and trace some of its effects. In our analysis, we suggest that the urine-testing regimen can intensify participant involvement with the criminal justice system. Further, we suggest that the court’s use of an abstinence model heightens exposure to alcohol and other drug-related harms and risks and segregates drug court participants from the broader society, increasing their isolation. We also argue that it inhibits other aspects of their lives, including their relationships, social lives, and employment prospects. Overall, we argue that these effects are at odds with the court’s aims. Nevertheless, despite the potential negative effects of the drug-testing regime, some participants find aspects of it beneficial. We conclude with some reflections on claims about the therapeutic value and potential of drug courts. We also suggest opportunities for reform. In this article, we explore in detail a way in which drug court participants are managed once they start their drug treatment order. We begin by providing some background into how the substance testing regime operates in the Drug Court of Victoria.
Background: The Court and Its Testing Regime
The Drug Court of Victoria was established in 2002 and is part of the first generation of Australian drug courts (Indermaur & Roberts, 2005). At the time we conducted our research (July to December 2015), the only existing branch of the Drug Court of Victoria was located in Dandenong. This is the branch we studied. A second branch opened in the Melbourne Magistrates’ Court in March 2017. The Melbourne branch has seen the reorganization of presiding magistrates but is run using the same policies as the Dandenong branch. Given the overlaps in policy and personnel, this article and the possibilities to bring about change it suggests have relevance for both branches and other courts that use similar methods. The stated objectives of the court are to improve the health and well-being of participants through reducing alcohol and other drug use and criminal behavior and improved connection to the community and to reduce the severity and frequency of offending for participants (Klynveld Peat Marwick Goerdeler (KPMG), 2014). Since 2002, two evaluations of the program have been conducted (Alberti, King, Hales, & Swan, 2004; KPMG, 2014). According to an evaluation conducted by KPMG (2014), 90% of Drug Court of Victoria participants are male and 10% are female. Participants currently range in age from 22 to 52. Further, 80% were born in Australia with the remaining 20% born overseas. Three percent identify as Indigenous Australians. Most (78%) have a previous imprisonment history, with the most common offenses committed before entering the program being theft related (47%), driving related (20%), and drug related (15%). The KPMG evaluation found that 61% of individuals accepted into the program did not complete the program but that those who did complete the program experienced improvements in health and well-being and reduced recidivism. 1
The Drug Court of Victoria employs three magistrates who preside over the two branches of the court full time, are responsible for the granting and canceling of drug treatment orders, and are responsible for the judicial supervision of participants. This includes compliance with drug treatment order conditions such as attendance to appointments with various drug court professionals and different substance use treatment modalities (Parsons & Lauritsen, 2013). 2 From time to time, other magistrates sit in, as the presiding Magistrates take leave. The court has strict eligibility criteria. A participant must be “dependent” on alcohol or other drugs, and their “dependency” must have contributed to the commission of the offense (Sentencing (Amendment) Act, 2002, s18Z). Drug court participants are sentenced to a drug treatment order, which lasts from 1 to 2 years. The order consists of two components: alcohol and other drug treatment and supervision and a custodial component that is suspended while the participant undergoes treatment in the community. The treatment component of the order includes specific conditions intended to address the participant’s dependence, such as attendance at appointments with drug court case managers and clinical advisors, alcohol and other drug counseling, regular attendances before the drug court magistrate, and regular substance testing. In addition, the order comprises three different phases. In order to progress from a lower phase to a higher phase, participants must have achieved the specific goals of their current phase. For example, one of the goals of Phase 3 is that the participants become “fiscally responsible” (KPMG, 2014, p. 19).
Because the drug court model first emerged in the U.S., it is important to note that Australian and U.S. drug courts differ in at least three ways. This is reflective of Australia’s approach being more oriented toward harm minimization. First, Australian drug courts were initially set up to target individuals with extensive histories of nonviolent offending, believed to be linked to problematic alcohol and other drug use, and who were likely to be facing imprisonment. In contrast, most U.S. drug courts target first-time offenders (Freiberg, 2002a, 2002b). They also differ at the point in the criminal justice system where participants are first admitted into the program. In Australia, drug courts are generally post-plea, in that defendants enter a “guilty” plea and are then admitted into the program if they meet the eligibility criteria. In the U.S., drug courts admit defendants at different points of the criminal justice system—arrest, bail, sentencing, and post-sentencing. Second, the U.S. practice of targeting individuals at multiple points in the criminal justice system means that U.S. courts bring a larger number of citizens into the system. For this reason, its drug courts have been increasingly criticized for coercing nonviolent, first-time offenders into drug treatment and lengthy court programs (Gowan & Whetstone, 2012; Mosher & Akins, 2014). Finally, Australian drug courts do not require participants to sustain an extended period of abstinence in order to complete the program (KPMG, 2014).
Testing regimes in the criminal justice system typically involve collection of multiple specimens: oral fluids, hair, urine, sweat, blood, and urine (Auerbach, 2007). Urine is generally accepted as the gold standard for drug testing because most of the published scientific literature and legal/court precedents associated with drug testing have been established with urine, but disadvantages to using urine have also been identified (Cary, 2011). First, it requires invasive, witnessed collection procedures (McIntire & Lessenger, 2007). Second, urine drug levels do not provide interpretive data on dose/concentration relationship or level of impairment. Third, the urine collected is susceptible to tampering via dilution or adulteration, and samples can be substituted (Cary, 2011). The last of these disadvantages is based on the assumption that donors will try to conceal their substance use and will engage in illicit strategies (such as drinking copious amounts of fluid to dilute the sample or using devices to substitute their sample with a “clean” one). Because of the perceived potential for collection scams, steps are often taken during sample collection to ensure test integrity, such as direct observation of urination and checking for the use of devices through which samples might be substituted.
According to the Drug Court of Victoria (2012), testing targets the following drug classes: amphetamines, opiates, benzodiazepines, cocaine, cannabinoids, and alcohol. This is based on the premise that they are the most frequently “abused” drugs in the forensic environment. Additionally, at the special request of the court, testing can confirm use of opioid replacement therapy drugs such as methadone, suboxone, naltrexone, and buprenorphine. The court’s urinalysis and breath testing policy (Drug Court of Victoria, 2012, para. 3.1.2) lists four main advantages to having such information. It allows: appropriate decision-making based on accurate information, credibility of the program in determining success and progress of participants, ability to intervene before a lapse or relapse leads to offending, and ability to monitor compliance with pharmaceutical treatments and/or psychiatric medications.
At the time our research was conducted (2015), drug court participants underwent both urinalysis and breath testing. They now undergo urinalysis only, as the court has access to a more sophisticated testing technology. 3 As noted above, participants pass through different phases of the drug court program. Testing frequency depends in part on which phase a participant is in: those in Phase 1 are required to undergo a urine test 3 times a week, while those in Phases 2 and 3 are required to undergo a urine test twice a week (Drug Court of Victoria, 2012; KPMG, 2014). At the time of our research, those on alcohol orders tested more often than others because the body metabolizes alcohol much more rapidly than other substances and the testing technology available to the court was unable to detect it after a few hours. The frequency of urinalysis or breath testing can be increased in any phase by the magistrate as a punishment for lack of compliance with order conditions (KPMG, 2014). Further, case managers can ask participants to undertake random tests at any time.
Literature Review
A growing body of literature critiques the operation, objectives, and effects of drug courts around the world (Boldt, 2010; Bowers, 2008; Burns & Peyrot, 2003; Colyer, 2007; Fischer, 2003; Fitzgerald, 2008; Gowan & Whetstone, 2011, 2012; Hoffman, 2000; Justice Policy Institute, 2011; Kaye, 2013; Lyons, 2013, 2014; Mackenzie, 2008; E. Miller, 2004, 2009; Moore, 2007, 2011; National Association of Criminal Defense Lawyers, 2009; Seddon, 2007; Tiger, 2011; Whiteacre, 2007). Within this literature, there are very few in-depth analyses of the process of urine testing in drug courts. Mackinem and Higgins’ (2007) 4-year participant observation study in three U.S. drug courts found that while urinalysis is considered an “objective” and rigorous method for drug testing, its use is highly subjective in drug court settings. For example, in the testing process known as line identification (which refers mainly to an on-site screening methodology), a chemically embedded paper interacts with drug metabolites in the urine sample. If no illicit drugs are in the urine, a line appears in a field indicator. If a drug is present, no line appears. Because individuals perceive color differently, personnel at times debated whether the line had appeared. Mackinem and Higgins also note that drug court personnel had the discretion to decide whether a participant had intentionally diluted the sample by drinking too much water. In a second study, Paik (2006) analyzed how drug test results were used in court decision-making. She found that depending on the participant, personnel anticipate, recognize, and treat some drug test results (originally reported as either positive or negative) as “false positives,” “false negatives,” or “inconclusive.” They do so by using interpretative tools, including participants’ patterns of behavior, history of substance use, understandings about their client population, and their own assessment of their colleagues’ competence in administering tests and “interpreting” drug concentration levels (see also Cary, 2004, 2011).
In addition to this work, some research on drug courts outside the U.S. has looked tangentially at drug testing. In the UK, Powell, Bankart, Christie, Bamber, and Arrindell (2009) point out that unlike the U.S. drug courts, where the aim is to achieve almost immediate abstinence from drugs, UK staff seemed to operate under a philosophy of harm reduction (Bean, 2014; Powell, Bamber, & Christie, 2007). In the UK, drug testing as part of a treatment order is only used as an indication of compliance, with frequency of testing set by the court at sentencing. The tests are not linked to sanctions because legislation prohibits the administration of such sanctions (McSweeney, Stevens, Hunt, & Turnbull, 2008). In her report on a Canadian drug court, Moore (2011) observes that drug testing was conducted randomly once a week, and although drug use was not punished, not admitting to drug use was. While these studies offer insights into how drug court personnel engage with drug testing technology and illuminate the test results and how they interpret them, drug testing in drug courts remains largely unexplored. This is especially the case in Australia (where alcohol and other drug-testing regimes and technologies might be very different from those reviewed above). This lack of research is important because drug testing is presented as an “objective” way of measuring the extent of alcohol and drug use and as central to the management of dependence. Hence, examining it closely will reveal key representations of dependence and ways in which drug court participants accommodate, resist, or otherwise engage with enactments of dependence in their drug-testing experiences. This is important because drug court participants’ voices remain largely unheard on this issue. In what follows, we aim to address these gaps with a detailed analysis of how urine testing unfolds in one Australian drug court.
Before we begin our analysis, however, it is important to consider research on opioid pharmacotherapy treatment (OPT). Many OPT programs also require urine-testing regimes like those used in drug courts, and some of the research on OPT explores issues that overlap with those of drug-testing regimes in drug courts. For example, Strike and Rufo’s (2010) study of drug testing in OPT found that some patients considered urinalysis procedures (including witnessing) degrading, embarrassing, and invasive and felt it reinforced “lying junkie” identities they were trying to escape. However, other patients came to accept it as part of the treatment. Further, while some clinical staff considered urinalysis beneficial, others believed that it jeopardized the development of the therapeutic alliance between clinicians and clients. Another important similarity between drug-testing regimes in drug courts and OPT is the limited opening hours of drug-testing facilities, dispensing pharmacies, and clinics. Fraser’s (2006) analysis of dosing in methadone clinics and pharmacies in Australia found that the model of waiting and dependence created by dosing processes produced the very kind of methadone subjects (“disorderly, illicit, and unproductive”) that the program assumed existed prior to intervention and that it was intended to reform. While this dynamic was identified specifically in relation to methadone, as will be shown below, her analysis offers a useful starting point for identifying similar counterproductive effects in drug courts.
Approach
The analysis conducted in this article is framed through Bacchi’s (2009) methodological work on analyzing policy. Her “What’s the Problem Represented to be?” (or WPR) approach was designed to facilitate critical interrogation of public policy, and to this end, she argues that policy does not simply “address” social problems, rather policies identify or constitute problems and give them shape (Bacchi, 2009, p. x). In this sense, policy approaches do not simply respond to preexisting, stable “problems,” but actually enact them. According to Bacchi, the way a problem is constituted has important effects for “what can be seen as problematic, for what is silenced, and for how people think about these issues and their place in the world” (Bacchi & Eveline, 2010, p. 112). Here, the term “effects” does not refer to “evaluation” or measurement of “outcomes” (Bacchi, 2009, p.15), but to the repercussions of problem representations and their implications for how we can think about problems. Problem representations also have effects on how participants see and understand themselves as well as material effects on their lives (see Bacchi, 2009, 2012). The WPR approach has been used to examine a range of alcohol and other drug policies and treatment issues (see Fraser & David Moore, 2011a; Lancaster, Duke, & Ritter, 2015; Lancaster, Hughes, Chalmers, & Ritter, 2012; Lancaster & Ritter, 2013). This emerging body of work has identified the multiple ways in which policies do not merely address the “problem” of alcohol and other drug use and “addiction” or “dependence” but discursively constitute it in particular ways. Other research within this “new subfield of drug policy research” (Seear & Fraser, 2014, p. 828) used Bacchi’s approach to critically examine the ways the law produces taken-for-granted assumptions about the “problem” of “drug use” and “addiction,” thus further stigmatizing and marginalizing people who use drugs through the subjectivities enacted (see Lancaster, Seear, & Treloar, 2015; Seear & Fraser, 2014; Spivakovsky & Seear, 2017). In this article, we extend these ideas further through a detailed analysis of the way one drug court conceptualizes the problem of alcohol and other drug “dependence” and seeks to respond to it through the administration of an onerous drug-testing regime. In doing so, we focus on the first, fourth, and fifth questions of Bacchi’s (2009) WPR approach, which consists of the following six questions (p. 2): What is the “problem” represented to be in a specific policy? What presuppositions (background knowledge) or assumptions (about the world) underlie the representation of this “problem”? How has this representation of the “problem” come about? What is left unproblematic in the “problem” representation? Where are the silences? What effects are produced by this representation of the “problem”? How/where has this representation of the “problem” been produced, disseminated, and defended? How could it be questioned, disrupted, and replaced?
Using Bacchi’s approach, we examine the presuppositions and assumptions that underlie the representation of drug problems in the drug court drug-testing policy and consider some of their effects on participants.
Method
The data on which our analysis is based were collected via a combination of methods: court observation, qualitative interviewing, and analysis of the textual materials the Drug Court of Victoria uses to present itself (including policy documents, information given to participants and evaluations). For the observational component of this research, one researcher (E.S.) attended the Drug Court of Victoria weekly across a period of 5 months (August to December 2015), observing public hearings and sitting in on case conferences (meetings involving drug court personnel before review hearings to determine the progress of participants). Extensive field notes were kept. In these field notes, we recorded interactions between drug court staff and participants during court hearings and how members of the drug court team administered sanctions and rewards in the case conferences. These notes constitute the project’s first data set.
The second data set for this project comprises transcripts of semistructured interviews conducted with two main categories of interviewees: court participants and court personnel. Fourteen interviews were conducted with drug court participants recruited through court-related organizations (see demographic details of drug court participants in Appendix A). Recruitment information provided to prospective participants made it clear that participation was entirely voluntary. A snowballing technique was also used to expand access to court participants. The second category of interview participants was drug court personnel. In conducting the observational component of this research, E.S. invited all members of the drug court team to participate via letter. Seven members of the drug court team expressed interest and were interviewed. Because this was the only drug court in the state of Victoria when this research was conducted, staff are readily identifiable, so demographic details about these participants cannot be reported here. Drug court participants were reimbursed for their participation in the research. The interviews explored a wide range of issues including drug court participants’ experiences with the drug court system, processes of entry, diagnosis and treatment, processes of alcohol and other drug testing, and views about alcohol and other drug use. The interviews were confidential, digitally recorded, and transcribed verbatim.
The third data set comprises key drug court policy and procedure documents, information given to participants and evaluations. The researchers identified documents using the report on the most recent evaluation of the drug court (KPMG, 2014). Most of the documents were provided on request by the drug court (see Appendix B). Two of these documents have been used in the Analysis section of this article: the drug court participant manual, given to participants when they start the drug treatment order, and drug court policy No. 8 (urinalysis and breath testing).
All three data sets were analyzed using the Miles, Huberman, and Saldana (2013) approach, which involves thematic analysis and coding in three stages: data reduction, data display, and data analysis. The project has ethics approval from the Curtin University Human Ethics Research Committee (approval number: HR84/2015). We have assigned pseudonyms to drug court participants, and in order to obscure gender and enhance the anonymity of participating staff, we have assigned only initials to drug court professionals.
Problematizing Alcohol and Other Drug Testing in the Drug Court of Victoria
As we noted earlier, the stated objectives of the Drug Court of Victoria are to improve participants’ health and well-being through reducing alcohol and other drug use and criminal behavior and improving their connection to the community and to reduce the severity and frequency of their offending (KPMG, 2014). This focus is instantiated in the legislation establishing both the court’s jurisdiction and the eligibility criteria for participants (the aforementioned Sentencing (Amendment) Act, 2002 , s18Z). Through these criteria, the drug court explicitly problematizes both alcohol and other drug dependence itself and criminal offending thought to be related to (or caused by) such dependence. We argue that these objectives are also underpinned by an implied subject (those who are both “dependent” and “criminal”). From the outset, in other words, the drug court’s objectives and underlying premises produce a set of problematic objects (“dependence” and “dependence-related crime”) and subjects (“dependent criminals”), even though these objects and subjects are assumed to preexist the establishment of the court itself. A key question for consideration then becomes: If the court’s objectives and eligibility criteria enact these as their problems, do the court’s practices and processes—and particularly, for the purposes of this article, the urine screening process—enact or assume the same kinds of problems or different ones? And what is the significance of these alignments or misalignments between the court’s stated objectives/foci and the effects it actually produces? We consider these issues in what follows as we analyze experiences of drug court participants with the court’s drug-testing regime. As we will see, these experiences include random testing. We also trace some of the effects of the alcohol and other drug-testing policy and its implementation for participants. In doing so, we make three key points: the regime is likely to intensify participants’ involvement in the criminal justice system, its emphasis on abstinence may heighten exposure to alcohol and other drug-related harms and risks and isolate participants from broader society, and it inhibits participants’ social relationships and employment prospects. In all these respects, the court can be said to create the very ill effects it is aiming to avoid. Ironically, both problem and solution are underpinned by the same idea: damaged/problematic drug-using subjects. As we will also note, however, despite these negative effects, some participants find aspects of the drug-testing regime beneficial.
Urine collection process
When asked to describe the drug-testing process, court participants responded with varying degrees of detail. Some were reluctant to speak about the process, but others provided very detailed descriptions. Kermit’s was the most complete account. In the excerpt below, he explains the collection process at the court. Additionally, Kermit reports witnessing the initial tests conducted on the specimen to determine that it is valid for subsequent testing,
4
checking color, pH (acidity or alkalinity), temperature,
5
and creatinine
6
levels. Kermit also tells us that before providing a new sample, he must report all drugs taken since his last test; this includes alcohol and drugs taken under prescription (but not caffeine or tobacco). All this information is documented in a form called the “chain of custody”
7
or “admit sheet,” as court staff and participants call them. There is a nurse [sample collector] and they got a little toilet to the side. You go in there, you give her your ID, she asks for your name, date of birth […] She asks who your case worker is, so you tell her that. You wash your hands, put on a pair of gloves. She has got like a sheet she fills out, she has got like to test for pH level, temperature and creatinine levels, I think, so she is getting the sheet ready. When she has got the sheet ready, there is like a little urine cup. She gives the cup, you go to the toilet. She stands behind you, there is a mirror to the left, there is a mirror in front of you, so that she can see from behind, so you pee on the cup, you hand it to her and she goes off and she starts testing for the pH and all that. And, then you are washing your hands, you come back and, um, she signs that sheet because they are getting the sheet ready because they ask you medication or drugs, so you tell them what medication or what drugs you are on. So she is filling that sheet out, she has got some test tubes, sucks the pee up in that, and sticks bar codes on them. You are watching, she does it in front of you […] Out of that sheet there is three copies: one is for you, one goes with the pee because it has got all your details and all that on it, and what drugs you have used, and one must stay there.
Frequency of urinalysis and breath testing
The frequency of urinalysis or breath testing can be increased in any phase by the magistrate as a reward or sanction in response to compliance with drug treatment order conditions. Further, case managers can require participants to undergo testing at short notice (Drug Court of Victoria, n.d., p. 27). The following is an excerpt of case notes written by a corrections case manager, Pablo presented as substance affected during the telephone call. He was queried in relation to this and stated that he is often asked this question when in contact with the drug court team, he denied any substance use today. The writer [case manager] directed Pablo to attend for a random urine screen today before four pm. Pablo argued the point and indicated that he would prefer to attend tomorrow […] The writer stated that he was directed to attend and failure to do so would incur sanctions. He stated that he would “just incur the sanction then.” The writer reminded him that his sanctions are high and this decision could result in a custodial term.
“You are employed by your order”
Collection processing time is lengthy, in part due to the need to carry out specimen validity tests. According to the urinalysis and breath testing policy (Drug Court of Victoria, 2012), collection takes 8–10 minutes per participant. Given that 60 participants are enrolled in the branch of the Drug Court of Victoria located in Dandenong at any one time,
8
and testing windows are short (see Appendix C for testing times), participants often face lengthy waits (and testing windows are adhered to strictly). The drug court participant manual (
Drug Court of Victoria, n.d
.)—given to participants when they begin their orders—lists “tips on how to test quickly” (p. 27): Arrive early to test. Better manage your time. If you drink a good amount of water before you test, you will avoid having to wait around for your bladder to be ready. But make sure you do not drink too much because this may dilute your urine. If your urine sample is negative but dilute, it will be not counted as a clear test.
These tips are important in the way they constitute responsibility for processing times. The first two tips place all the onus of meeting testing requirements on the participant. They imply that if participants do not arrive early, this is because of poor time management skills. Little attention is paid to participants’ need to attend several commitments related to their orders, such as appointments with court professionals and alcohol and other drug service providers, court hearings, community work, and daily collection of medication. Further, this approach neglects at least three important contributing issues: that the testing process (provision of specimen, subsequent validity tests, and documentation) is itself time-consuming, that times for testing are limited, and that many court participants need to be tested.
How does this process and the logic on which it works affect participants? One of the most important effects is that in order to fully comply with the order, some participants feel forced to neglect other areas of their lives such as employment. During the observational component of the study, we noted the magistrate saying to many participants, “you are employed by your order.” Indeed, some of our research participants were forced to turn down employment offers because they conflicted with court commitments. This conflict between adherence to the court order and pursuit and maintenance of paid employment is significant in that it contradicts one of the goals of the court, which is to “improve their connection to the community” (KPMG, 2014, p. 51). As one participant, Cirilo, explained: So [while working, I] missed a few appointments and he [magistrate] goes ‘Your priority’ [is the order]. I said “I know my priorities. You know what? I need to pay rent. If I am not paying rent and I am living on the street, like, this whole thing is pointless.” […] He goes “Yeah, you can only work two days a week at the moment” and he put an order [a further condition on the existing order] only to work two days a week […] and I was trying to tell my case worker, like, “Listen, you know, like the eight hours that I work, I don’t think about drugs, I am not battling in my head all day and then I go home, I am tired, and I just sleep,” you know. I said “If you look at all my clean urines, it would be the days that I worked” you know what I mean? So, and, they go to me “Yeah, but you got to earn, you got to earn [it].”
Like Cirilo, Erik expressed frustration with the commitments associated with testing, including the waiting times he faced: The waiting thing is like it is on purpose. It is like they are trying to get you to wait, and we are always waiting with other people on the order, which isn’t good because then I start hearing things and talking about drug dealers and talking about which one is good, and which isn’t and, you know, things like that. So, I don’t like the waiting at all.
If we return to the “tips to test quickly,” we can see that the third tip is somewhat contradictory and illustrates another challenge drug court participants face. They are advised to drink enough water to have a full bladder by the time they test but not to drink too much because it might cause a diluted sample. Erik illustrates the consequences of living with such conflict: It has happened to me three times this month, where I have missed the train or some stupid thing on the public transport, and I had to go to [void bladder in] train station [midway through home and testing venue], and then I start drinking water again, and then I get done for dilute sample because the water I drink, the 2 liters, comes through quickly sometimes and they say “you are dilute.” It comes out like water, it looks like you can drink it, it is so clear!
Shaping the nature of alcohol and other drug-related harms and risks
According to drug court policy, the drug classes tested are amphetamines, opiates, benzodiazepines, cocaine, cannabinoids, and, as indicated above, alcohol. As noted earlier, this is based on the premise that they are the most frequently “abused” drugs in the forensic environment. At the special request of the court, testing can confirm drugs such as methadone, suboxone, naltrexone, and buprenorphine. Other substances may be tested for whether, during the clinical assessment, the court deems the participant “dependent” on them or suspects they are using them while in the program. For example, by sitting in on the case conferences (held before review hearings), we found that on rare occasions participants were being tested for GHB. 9 The court is unable to test for some drugs because the testing technology available through the contracted pathology service cannot detect them. As Auerbach (2007, p. 220) points out, “as designer drugs evolve, there may be a lag in availability of an appropriate test for the substance.” Court participant Mateo illustrates this point:
I had a conversation with my doctor yesterday about Valium, 10 two by five milligrams every day […] I have found that has helped in the past, so I will use that and a combination with perhaps some synthetic drugs, um, for a couple of weeks so that I pass my urine screens [….] It will just allow me to have, to give those couple of weeks of clean urines whilst still smoking [synthetic] “cannabis” and having the Valium to lean on as well.
So when you say synthetic drugs, they are drugs that aren’t picked up in the tests?
Correct […] this is something that I discuss with you. I have to compartmentalize certain things depending of who I am talking to, so if I am talking to my doctor I am not mentioning the synthetic weed, it is about me relieving the craving for cannabis.
Here, Mateo shows us another way in which the specificities of the testing process (i.e., which substances are tested for) may produce the very kinds of problems that are thought to preexist drug policy and procedures. He tells us that he circumvents penalties associated with drug use by devising his own cannabis “replacement therapy”: a cocktail of “synthetic weed” and (prescribed) Valium. In order to do this, Mateo must draw on several resources and skills. For example, he must investigate which synthetic drugs go undetected by consulting with other more seasoned court participants and “compartmentalize” information in a highly surveilled environment involving a network of professionals who are in constant communication. Here, Mateo resists the power of the court through a form of entrepreneurship that would usually be characterized as duplicity. For the purposes of our analysis, it is important to note that in this outcome, the court may be achieving exactly the opposite of its aims. As Mateo’s case illustrates, some participants use alternative drugs to avoid sanctions, some of which have the potential to be more harmful (Valium and synthetic cannabis) than the substance sanctioned (cannabis). In this way, the drug court appears to be at risk of producing the very kinds of problems it treats as anterior to its own actions, problems it has been established to solve.
Intensifying exposure to the criminal justice system
Drug-testing regimes instantiate the notion that participants are untrustworthy and will try to beat the testing system. At times, this distrust prompts decisions that result in life-changing consequences for participants, including ejection from the program and further enmeshment in the criminal justice system (see Cohen, 1985; Roberts & Indermaur, 2006, for a more detailed discussion of net-widening effects of diversionary programs in the criminal justice system and Fraser, 2006, for related effects in OPT). These effects can be observed in Cirilo’s case, which E.S. encountered in a review hearing. Cirilo was accused of “corrupting” the urine-testing process. He had not attended his regular review hearing earlier that week because he was unwell. Although he had provided a valid medical certificate, the magistrate insisted he attend court. Despite his illness, Cirilo did so. The following excerpt, taken from our field notes, shows the exchange that took place between the magistrate and Cirilo’s lawyer:
I understand that there was some suggestion or thought that perhaps there was a false device being used in relation to Cirilo’s presentation at testing.
I think it was something strongly thought. It was absolutely observed by the collections officer who saw the fake penis, saw him try and manipulate it, challenged him on it, told him to drop his pants, saw the harness arrangement in among his underclothes.
Well, your honor just on that note, I have received the review sheet 11 in terms of the feedback, but an incident report with those sorts of details has not been provided to me. So on the basis of the information that I had received both through the case management team and the review sheet, there was an allegation, but certainly there wasn’t confirmation of that. He denies vehemently that he was using any sort of device.
That was part of the report that I had received: that he denied vehemently, as he did when he tampered with the testing process [a few weeks before] when he delivered a cold urine sample.12
Again, your honor at this stage, my understanding is that no device has been seized—so that there was some sort of evidence that could have been more compelling to consider imposing sanctions in relation to that. What I would be asking the court to consider is—Cirilo has been advised of these concerns this week by his case manager, they have had a discussion in relation to it. I would be asking that the court consider imposing a warning on him, advising him that these concerns have been raised by the tester, and that if there were further concerns raised, that imprisonment sanctions would then be imposed. But certainly I would submit that for him to receive essentially 10 days jail for what is an allegation that there is no proof in relation to…
Well, I am utterly satisfied of the observations of the collections officer, and it is the second time that he has tried to corrupt the testing process in a month. It displays an absolute contempt for this program and for the drug treatment order that he’s on. Lawyer explains that Cirilo’s compliance on the order has greatly improved and that decisions should be made in that light. The magistrate interrupts lawyer’s submission and continues.
Cirilo, this is the second time in a month that you have tried to corrupt the testing program. This matter is extremely serious. It undermines the program for the whole drug court community and it displays the worst attitude that one could expect to see in this program. You are required to serve 10 custody days sanctions
13
today, and an application to cancel your drug treatment order will be listed next Thursday. Thank-you, take a seat please. Cirilo appears dumbfounded, tries to address the magistrate with no success and eventually sits down looking resigned.
In this review hearing, the court imposed 10 custody days, based, as the lawyer indicated, only on the allegation of the collector. In the process, the magistrate shows a fluctuating degree of certainty about the allegation, first saying it was “something strongly thought” (a suspicion), then that “it was absolutely observed” (a fact). It is also of note that the magistrate refers to a separate occasion on which Cirilo allegedly tampered with his urine sample. This acts as an important precedent, so much so that the magistrate does not require evidence to make the decision to sanction Cirilo. Later, we interviewed Cirilo about his drug court experiences. His account of the incident was as follows: I went to do a urine test […] I start urinating, filled up the jar, and she [collector] goes to me, “Oh! That doesn’t look real, that doesn’t look real to me.” I go: “What? What are you talking about?” and I actually showed it [my penis] to her. I go, “What are you talking about?” and then because I had a cup in my hand […] I said “Hold the cup and stay right there!” you know. So I dropped my pants, I dropped my underwear, I lifted up my top; I said “Are you happy with that?” She goes “Yeah, fine,” you know, and that was it. I thought “OK, that is it” [later] my case manager rang and she goes, “What happened today?” I explained it to her, and she goes, “Just be more careful next time.” I said “Listen, I have done everything she [collector] asked, did she say that to you?” She [case manager] goes “Yes, she did say that,” you know. I said “OK, sweet, at least she was honest about that.” Next thing, I go to court [for weekly review] and I am hearing “There was a harness strapped on.” The notes [by the collector] are “I thought there may have been a fake penis, I asked [Cirilo] to pull his pants down, I thought I saw something under his undies, but I didn’t feel comfortable to ask him any further.”
Cirilo was later involved in a serious car accident, and the application to cancel the drug treatment order hearing was adjourned on several occasions. He was not reinstated on the order, and the urine sample subject to all the contention was found to be consistent with “human urine.” The police did not pursue the charge of “perverting the course of justice.” A magistrate from the general court division involved in Cirilo’s subsequent sentencing hearing declared that urine cannot be tested for DNA.
In this example, not unique, we see the program’s ability to intensify participants’ involvement with the criminal justice system. During our research, we observed participants charged with “deception” after being found to be providing fraudulent medical certificates
14
or committing serious crimes while on the order. Many eventually served more time than they perhaps would have served had they gone through a mainstream criminal court. In such cases, the participants were enacted as primarily responsible for their own “failure.” While such experiences are not the case for all the participants, it is clear that, at least for some, the intensity of the drug court program increases the risk of criminalization. Highly regimented and onerous urine testing is the central mechanism by which this effect arises. At least one drug court professional, I find that participants are really over-prosecuted, really, yeah. I would often just think “you are probably better off on a corrections order and doing a bit of time than being put on a [drug treatment order].”
Drug testing: A way to “keep me in check”
Importantly, while these examples raise significant questions about urine testing and its role in producing undesirable drug court effects (and undesirable drug court subjects), not all experiences with the drug-testing regime were negative. Some participants found aspects of it valuable, as was the case with Simon. Having been promoted to Phase 2, the frequency of his testing had decreased from 3 times a week to 2 times a week, but he asked that the earlier testing pattern continue: I am a hundred percent sure [testing] is what keeps my head going in the way of—I know if I do, do dirty [provide positive drug test results], I’ve got to answer to three, four people plus the judge, you know […] then I can be locked up, you know. It is as easy as that […]. When I know that I have to do the three urines, it just keeps me in check more, so that I know what I am looking forward to, you know. I know it is a good feeling walking out, doing three clean urines a week, you know. At the start it was hard to do three. I was only doing one or mainly none [chuckles]. But, to walk out now, and have three [negative drug tests] a week is good.
Conclusion
In this article, we examined the approach to drug testing in one Australian drug court. Drawing on Carol Bacchi’s poststructuralist approach to policy, we explored the problem representations inherent in the drug court’s policy with respect to drug testing and considered some of the underlying presuppositions and assumptions embedded in that policy. We then explored some of the effects of the policy and the process of its implementation, including the effects for drug court participants subjected to the testing regime. We argued that the everyday and seemingly mundane ritual of urination is of central importance to the drug court model, a mechanism by which the drug court seeks to govern participants and solve their problems (particularly their alcohol and other drug “dependence”). As Vrecko (2009) points out, the coercion in drug courts is not carceral; it involves a commitment by the individual “to submit to relatively mundane, but technically precise interventions that target only particular, ‘dividual’ elements of the offending subject” (p. 223). Urinalysis is a clear example of such an intervention because it targets a specific activity of the participants: the several-times-daily, mundane ritual of urination. In our view, for many participants, the governance of urination is one of the most coercive elements of the order and an important way through which particular problems are constituted and particular forms of social control are enacted.
In urine testing, the problems participants face are constituted as anterior to the operations of the drug court. In this sense, urine testing helps constitute the legal and social rationale for the court: It deters substance use, alleviates participants’ dependence, and in so doing, resolves associated problems such as criminality. However, as we have argued, the specific practices of urine testing documented in the drug court may actually allow or even produce the very kinds of problems thought to justify participants’ commitment to the court. Urine-testing regimes are onerous, demanding, intrusive, and time-consuming. Although the drug court purportedly adopts a model of harm reduction, testing regimes are more consistent with abstinence models since substance use is heavily monitored and sometimes formally sanctioned through custodial sentences. This focus on abstaining from alcohol and other drug use can have a range of effects. It can, for example, magnify entrepreneurial efforts on the part of some participants to avoid detection through complex and potentially harmful alternative drug-taking regimes. In this sense, drug courts may allow or encourage the very kind of drug-related harms that are assumed to be resolved by them and which are often claimed to be the effects of “addictive” drugs “themselves” (see Fraser & David Moore, 2011a).
The policy of urine testing has other effects. For instance, frequent attendance and waiting times, added to other drug court commitments, constitute barriers to securing and maintaining employment for some participants (see also Fraser, 2006). Paradoxically, these kinds of broader lifestyle changes (securing stable, ongoing employment) are one of the aims of the drug court model, in that the court problematizes participants as insufficiently gainfully employed and lacking engagement with the broader community (Fraser, 2006). Second, while the treatment and monitoring modalities to which participants submit are community-based, they might further direct participants to the periphery of society and encourage them to form relationships with others who use substances. Again, this is often in conflict with the stated aims of the drug court, which problematizes participants as margin dwellers. These findings are consistent with Fraser’s (2006) findings about OPT, which, in its quasi-coercive forms, bears similarities to drug court approaches. Finally, we have argued that the process of urine testing can intensify rather than reduce participants’ exposure to the criminal justice system and increase criminalization. Again, criminal behavior in drug court participants is often naturalized and positioned as an effect of drug use and/or “dependence,” a problem that preexists enrolment in the drug court and is likely to be alleviated by it. This increased risk of criminalization raises important questions about the efficacy of the drug court model and its putatively more therapeutic approach.
Our analysis suggests that the drug court enacts a wide range of problems and that the effects it produces, in Bacchi’s sense, are sometimes uneven and contradictory. In some respects, the court’s drug-testing processes produce effects that converge with the court’s stated aims. Other effects diverge from them and are more clearly anti-therapeutic, in contrast with the underlying objectives and claims of the drug court as a remedial alternative to traditional criminal justice systems. While similar concerns have been raised before in the context of U.S. drug courts targeting low-risk or low-level offenders (Belenko, Fabrikant, & Wolff, 2011; Justice Policy Institute, 2011; Makkai, 1998, 2002), the analysis that we offer in this article differs from that work in two key ways. First, we have provided examples of how an Australian drug court, which focuses on individuals with a long history of offending, might intensify involvement in the criminal justice system through the mechanism of drug testing. Second, our work demonstrates the simultaneously divergent and convergent effects of these processes and the tensions and overlaps between these and the court’s stated aims. As we know, Carol Bacchi’s framework demands a focus on the ways in which policy processes enact problems. These findings suggest that the “effects” of drug court processes may not always align, at least at first glance, with the formally stated “problems” that lodge within and underpin the rationale of the court. This is most obvious when we consider the extent to which the court’s focus on improving community connections, fiscal responsibility, and reducing criminalization is actually achieved. These divergences (between problem representation and “effects”) expose the difference between the palatable public account and the messy, often negative motivation and logics the court entails. What is more, they pose some challenges for our use of Bacchi’s framework. We argued, however, that the various effects produced by the drug court align with the key presuppositions lodged in the rationale for the court. This involves the presupposition of the abject subject (those who are both “dependent” and “criminal”) in the court’s aims and objectives and the abject subject that drug courts often (although not always) enact.
Research remains to be undertaken in other drug courts to establish whether these issues apply elsewhere and to consider the effects of this seemingly inadvertent drift away from harm reduction. We argue that courts should rethink the very central emphasis they place on alcohol and other drug use per se. It is possible that the drug court’s intense focus on alcohol and other drug consumption forecloses other ways of thinking about participants and their lives, their needs, priorities, and the kinds of supports that might benefit them and improve their well-being. In other words, the focus constitutes the court’s problems in certain ways, and as Bacchi notes, alternative ways of constituting problems can produce significantly different effects. Drug court participants we encountered for this research were socially and economically disadvantaged and struggling with fundamentals such as food and housing. It is important to ask whether the drug court’s particular emphasis on urine tests and urine test results is productive, given the adverse outcomes we have identified. Drug testing could be made available if requested by participants who consider it useful to them. Furthermore, other more respectful forms of accountability can be developed. In this article, we questioned what drug courts prioritize and how these priorities stem from problem representations, presuppositions, and assumptions that lodge in the design of drug courts from the outset. Might things be done otherwise?
Footnotes
Appendix A
Demographic Details of Drug Court of Victoria Participants Involved in Our Research.
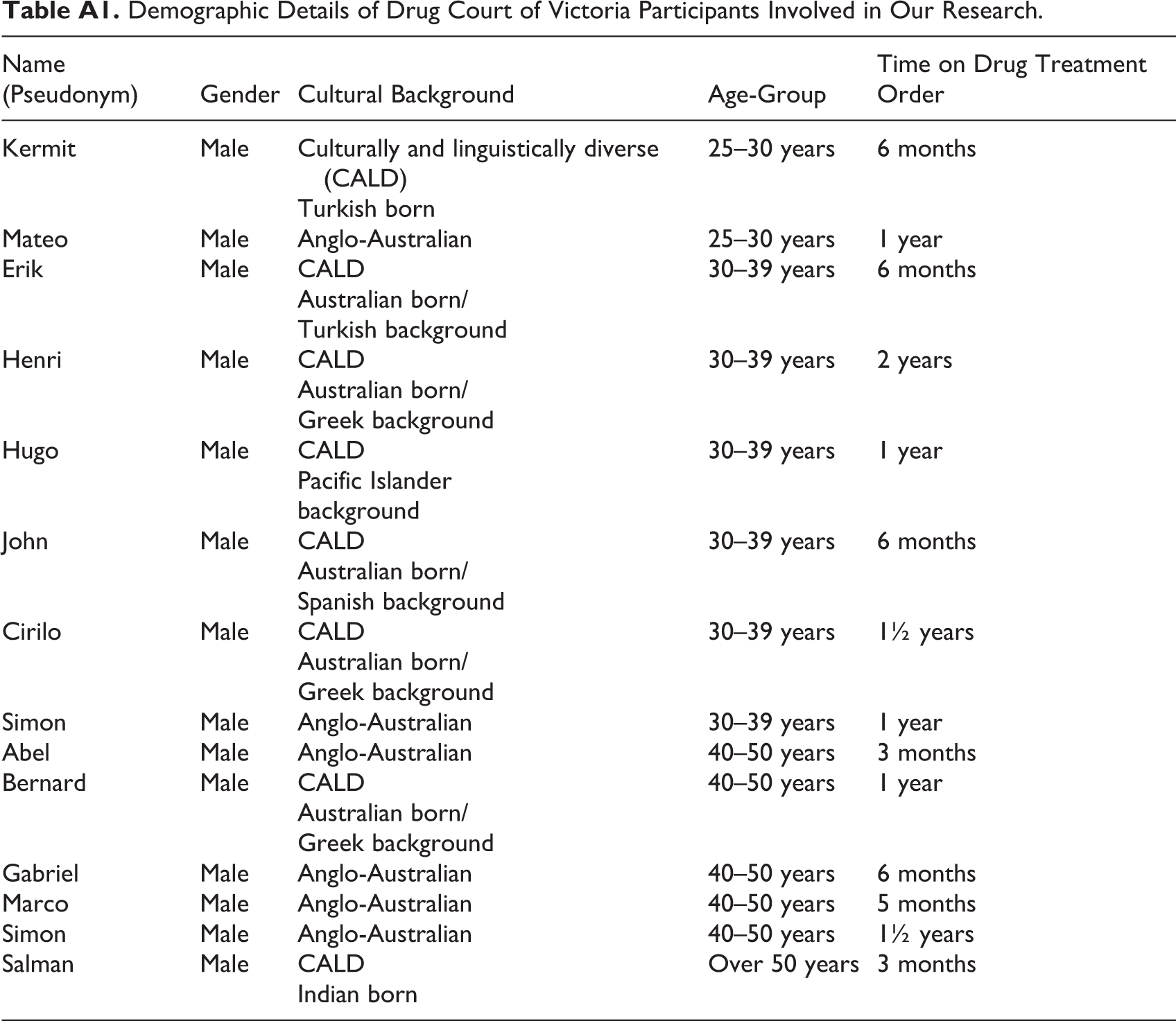
| Name (Pseudonym) | Gender | Cultural Background | Age-Group | Time on Drug Treatment Order |
|---|---|---|---|---|
| Kermit | Male | Culturally and linguistically diverse (CALD) | 25–30 years | 6 months |
| Turkish born | ||||
| Mateo | Male | Anglo-Australian | 25–30 years | 1 year |
| Erik | Male | CALD | 30–39 years | 6 months |
| Australian born/ | ||||
| Turkish background | ||||
| Henri | Male | CALD | 30–39 years | 2 years |
| Australian born/ | ||||
| Greek background | ||||
| Hugo | Male | CALD | 30–39 years | 1 year |
| Pacific Islander | ||||
| background | ||||
| John | Male | CALD | 30–39 years | 6 months |
| Australian born/ | ||||
| Spanish background | ||||
| Cirilo | Male | CALD | 30–39 years | 1½ years |
| Australian born/ | ||||
| Greek background | ||||
| Simon | Male | Anglo-Australian | 30–39 years | 1 year |
| Abel | Male | Anglo-Australian | 40–50 years | 3 months |
| Bernard | Male | CALD | 40–50 years | 1 year |
| Australian born/ | ||||
| Greek background | ||||
| Gabriel | Male | Anglo-Australian | 40–50 years | 6 months |
| Marco | Male | Anglo-Australian | 40–50 years | 5 months |
| Simon | Male | Anglo-Australian | 40–50 years | 1½ years |
| Salman | Male | CALD | Over 50 years | 3 months |
| Indian born |
Appendix B
List of Documents Provided by the Drug Court of Victoria.
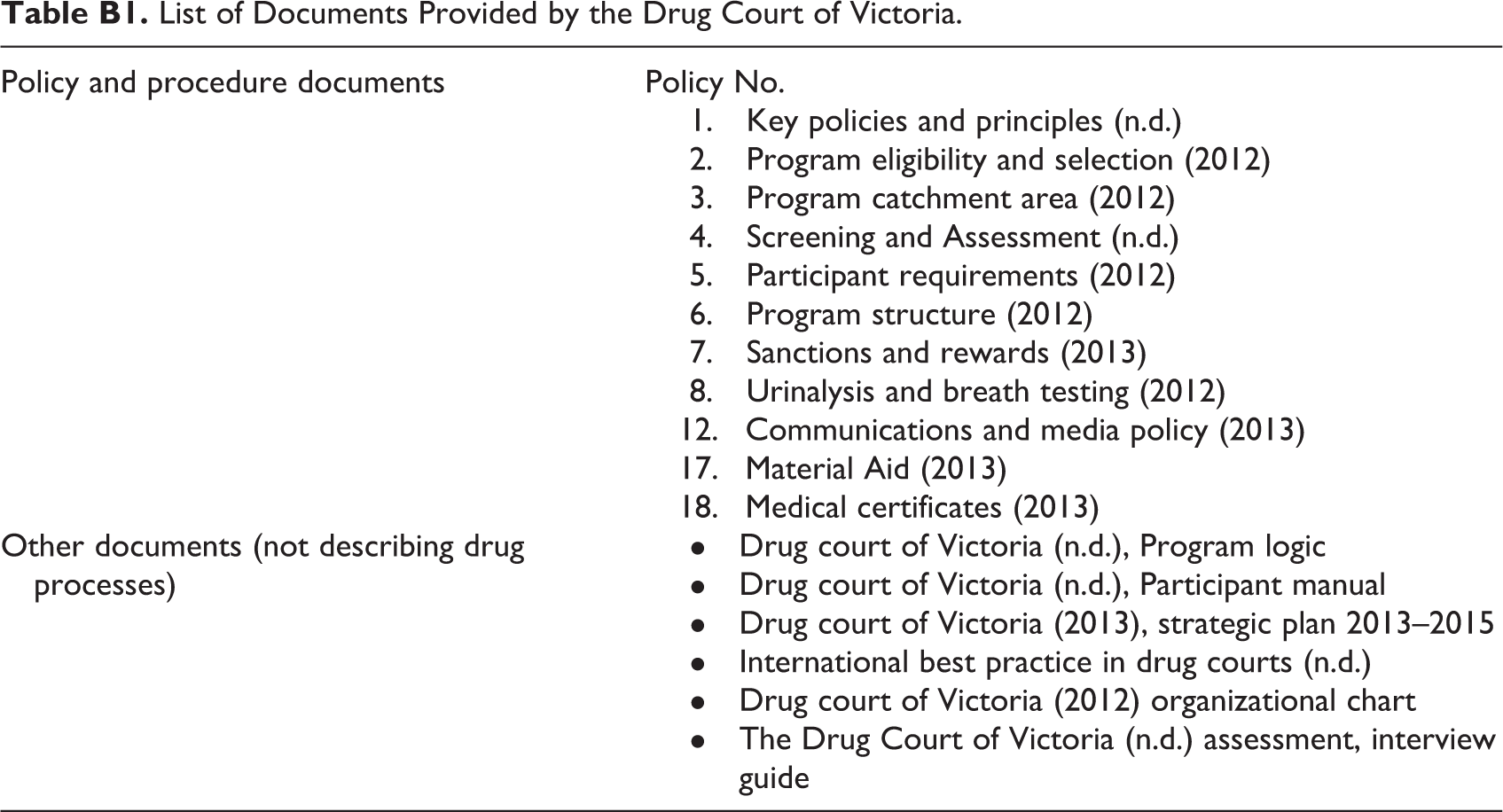
| Policy and procedure documents | Policy No. Key policies and principles (n.d.) Program eligibility and selection (2012) Program catchment area (2012) Screening and Assessment (n.d.) Participant requirements (2012) Program structure (2012) Sanctions and rewards (2013) Urinalysis and breath testing (2012) 12. Communications and media policy (2013) 17. Material Aid (2013) 18. Medical certificates (2013) |
| Other documents (not describing drug processes) |
Drug court of Victoria (n.d.), Program logic Drug court of Victoria (n.d.), Participant manual Drug court of Victoria (2013), strategic plan 2013–2015 International best practice in drug courts (n.d.) Drug court of Victoria (2012) organizational chart The Drug Court of Victoria (n.d.) assessment, interview guide |
Appendix C
And additional rules around testing times: – Participants on Phase 1 must arrive to test before 3 p.m. (unless they have been given permission to test before 5 p.m.). – Testing before lunch. – The drug court closes for lunch between 1.30 p.m. and 2 p.m. The last participant to test before lunch will be accepted not later than 1.20 p.m. Anyone testing after 1 p.m. must accept that they may not get to test before 1.30 p.m. If there are too many people waiting, it is at the discretion of reception whether participants can test before lunch. – Testing before 5 p.m. – The drug court closes at 5 p.m. sharp. This does not mean that if you arrive 1 minute before 5 p.m. that you can still test. It means it closes at 5 p.m. – Participants arriving after 4.30 p.m. risk not being able to test if there are too many people who have arrived at around the same time. This is at the discretion of reception. – Priority will be given to participants who work and have prior permission to test later in the day.
Acknowledgments
The authors are grateful to the Drug Court of Victoria and the Magistrates' Court of Victoria for facilitating access to the field site. Special thanks go to the drug court participants and professionals who took part in the project, and to the individuals from the three welfare organisations who assisted with recruiting drug court participants. Finally, the authors would like to thank the anonymous reviewers for their helpful comments on earlier drafts for this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Eliana Sarmiento’s work was supported by a Curtin University Office of Research and Development PhD scholarship. Kate Seear’s work is supported by an Australian Research Council Discovery Early Career Researcher Award Fellowship (DE160100134). Suzanne Fraser’s work was supported by an Australian Research Council Future Fellowship. The National Drug Research Institute is supported by core funding from the Australian Government under the Drug and Alcohol Program and also receives significant funding from Curtin University.