
Abstract
To investigate whether diversion to a pretrial community-based diversion program reduced sexual recidivism in adult intrafamilial child sex offenders, 208 offenders assessed for treatment between 1989 and 2003 were monitored for periods ranging from 2.8 to 18 years. Participants accepted for treatment (n = 88) were compared to those who declined (n = 120). After applying propensity score analysis to control for selection bias, Probit regression analysis and Cox proportional hazards regression were used to estimate rates of desistance between the groups. Although differences were not statistically significant, estimated rates of sexual reoffending were lower and time taken to sexually reoffend was longer in the diverted than the undiverted group. An overall effect size for treatment was large (OR = 0.52, 95% CI = 0.18, 1.5), and examination of the recidivists in the treatment group supported inferences of positive treatment effects. Limitations of this study are examined, and future directions for intrafamilial sex offender treatment are discussed.
Keywords
The most recent data on reported victims of sexual assault in Australia reflected annual estimates of 7,500 child victims younger than 14 years of age (187 per 100,000 children; Australian Institute of Health and Welfare [AIHW], 2009b). Approximately 9% of the estimated 26,200 children who were the subject of a child protection substantiation in 2007–2008 were assigned this status because of sexual abuse (AIHW, 2009a). Difficulties in child and adult sexual assault prosecution proceedings are entrenched (Eastwood, Kift, & Grace, 2006). Among all sexual offenses reported to police in Australia, criminal proceedings are initiated in only 15% of incidents involving child victims (Fitzgerald, 2006). Parallel trends persist in overseas jurisdictions (United States, United Kingdom, Ireland, Canada), where only 17% of reported sexual offenses result in a conviction (Crime and Misconduct Commission, 2003).
Factors contributing to high attrition rates in criminal proceedings involving sexual abuse are well documented (Parkinson, Shrimpton, Swanston, O’Toole, & Oates, 2002; Taylor & Gassner, 2010). Acts of sexual abuse against children are not reported to authorities by parents to protect the child victim from the ordeal of court proceedings, because of a lack confidence or trust in the legal system or the police, from fear of retribution by the offender, because they experience feelings of shame or embarrassment, and, in the case of intrafamilial offenses, because the nonoffending parent may not want to break up the family (Parkinson et al., 2002; Taylor & Gassner, 2010). Once a report is made, charges may not be laid by the police, or the accused committed for trial, because the perpetrator was unidentified, the child victim gave an unclear account of events, there was insufficient evidence, or evidence was contaminated by the police interviewing process (Parkinson et al., 2002; Taylor & Gassner, 2010). A trial may not proceed to determination if the child refuses to testify or becomes too distressed by cross-examination to continue (Parkinson et al., 2002; Taylor & Gassner, 2010).
In light of these difficulties, many communities have explored alternatives to traditional court procedures to better manage child sexual assault cases (Cossins, 2010). To deter repeat sexual offenders, like their North American counterparts, Australian states have increased sentences and supervision, expanded community notification and registration (e.g., Child Protection [Offenders Registration] Act, 2000) and have established rehabilitation programs for convicted offenders (Chung, O’Leary, & Hand, 2006; Lievore, 2004; McSherry, Keyzer, & Freiberg, 2006; Wood, Grossman, & Fichtner, 2000). Rehabilitation programs operate in prison and within the community (Beech, Craig, & Browne, 2009; Chung et al., 2006). This study reports findings from data drawn from Cedar Cottage, a unique community-based pretrial diversion program established in 1989 in Sydney, Australia, that offers treatment to intrafamilial sex offenders, their victims, and other family members. This treatment program was examined because there exists a lack of information on intrafamilial offenders. Previous meta-analyses and single case studies on the effectiveness of community-based treatment programs for sex offenders, and intrafamilial sex offenders in particular, have produced inconsistent and equivocal results (Collins, Peters, & Lennings, 2009; Villettaz, Killias, & Zoder, 2006). The same conclusion was reached more than 20 years ago by Keller, Cicchinelli, and Gardner (1989) following a survey of 553 child sexual abuse treatment programs in prison and community settings in the United States.
The Dearth of Information on Intrafamilial Offenders
Comparatively little is known specifically about intrafamilial sex offenders as many researchers have combined subtypes of sex offenders (e.g., rapists, extrafamilial child sex offenders, voyeurs, and exhibitionists) when measuring recidivism (Finkelhor, 2009; Kingston, Firestone, Wexler, & Bradford, 2008; Stalans, 2004). This practice is problematic as subtypes of sex offenders are known to differ in terms of offense characteristics (Craig, Browne, & Stringer, 2003) and recidivism rates (Harris & Hanson, 2004). For example, extrafamilial child sex offenders tend to have more victims but offend only once or twice against individual victims, whereas intrafamilial child sex offenders tend to have one or two victims but offend against them repeatedly before apprehension (Brown & Brown, 1997; Smallbone, Marshall, & Wortley, 2008). Other features believed to differentiate intrafamilial sex offenders from rapists and extrafamilial sex offenders are less use of violence or force while offending, less likelihood of a criminal record of sexual offending, and cohabitation with a long-term intimate partner (Herman, 2000; Johnson, 2007).
In relation to sexual recidivism rates among subtypes of sex offenders, a meta-analysis of 10 follow-up studies of adult male sexual offenders (combined sample of 4,724) revealed that overall recidivism rates (14% after 5 years, 20% after 10 years, and 24% after 15 years) were similar for rapists (14%, 21%, and 24%) and the combined group of child molesters (13%, 18%, and 23%; Harris & Hanson, 2004). There were, however, significant differences between the subtypes of child molesters, with the highest rates observed among extrafamilial boy-victim child molesters (35% after 15 years) and the lowest rates observed among incest offenders (13% after 15 years; Harris & Hanson, 2004). Accordingly, researchers have recommended that subtypes of sex offenders should be studied in discrete groups to better determine the specific recidivism rates for each subtype of sex offender (Finkelhor, 2009; Stalans, 2004). The current study reports on reoffending in a group entirely composed of intrafamilial child sex offenders.
Inconsistent Findings on Prison and Community-Based Sex Offender Treatment
Evaluations of cognitive behavioral therapy (CBT) treatment programs, the leading treatment intervention for sex offenders (Chung et al., 2006; Lievore, 2004), have demonstrated that these programs reduce sexual recidivism rates. In a meta-analysis of 43 different studies including more than 9,000 offenders in North America, Canada, the United Kingdom, and England, sexual offense recidivism rates were significantly lower overall in offenders who received treatment compared to those who did not (Hanson et al., 2002). In relation to sexual recidivism, 12.3% of treated offenders sexually recidivated compared to 16.8% of untreated offenders (odds ratio = 0.81, 95% CI = 0.70, 0.93; Hanson et al., 2002). Within this meta-analysis, the therapies under review operated from a combination of prison-based and community settings, and recidivism rates were derived from national criminal justice records, state records, child protection records, and self-reports and included a follow-up period with a median of 46 months for both the treatment and comparison groups (Hanson et al., 2002). Substantial variability in sexual recidivism was detected across the studies (Q = 145.02, df = 37, p < .001; Hanson et al., 2002).
Similarly, a larger-scale meta-analysis of 80 independent comparisons of a range of sex offenders (N = 22,181) in institutional settings who were exposed to different types of treatment interventions (CBT, psychosocial and organic treatment modes) yielded results showing an overall positive and significant effect of sex offender treatment: 11.1% of the treated offenders recidivated sexually compared to 17.5% of the offenders in the control groups (mean OR = 1.70 for sexual recidivism; Lösel & Schmucker, 2005). The mean OR of 1.70 for sexual recidivism was highly significant (z = 4.96, p < .001). For the most part, intrafamilial offenders were intermingled in samples containing other diverse types of sex offenders. In the studies in which intrafamilial samples were included, the size of the samples was too small to draw any definitive conclusions, a problem exacerbated by the low base rates typical in sexual reoffending (Craig et al., 2003).
Some more recent single study evaluations of community-based sex offender programs provided positive results. In a study of 175 offenders who were treated at one of the three community-based programs in New Zealand (SAFE Network Inc, STOP Wellington Inc, and STOP Trust Christchurch), the overall sex offense recidivism rate for all clients who completed one of the programs was 8.1%, compared with 16% (odds ratio = 0.51) in the nontreated comparison group and 21% (odds ratio = 0.39) in the assessment-only group (Lambie & Stewart, 2003). However, there was no significant difference in recidivism rates observed between these groups within any one of the programs, presumably because of the diminished statistical power when the data were not aggregated, χ2(df = 2, N = 172) = 0.46 (Lambie & Stewart, 2003).
Conversely, other recent single studies have shown no effect of treatment. For example, adult male sex offenders convicted of a sexual assault offense (ranging from rape to indecent sexual assault of a minor, sodomy, carnal knowledge, and gross indecency), who undertook some or all of the Queensland Sex Offender Treatment Program while in prison and who were released from custody between 1992 and 2001, were monitored for 5 years and 1 month following release into the community (Schweitzer & Dwyer, 2003). The sample consisted of 445 men, 196 completers, 85 noncompleters, and 164 matched controls. No significant reduction in sexual recidivism followed participation in the program: during the evaluation period, 3.1% of completers, 7.1% of noncompleters, and 4.9% of controls were convicted of a sexual offense, χ2(3) = 2.223, p = .317 (Schweitzer & Dwyer, 2003). The results were compromised by extensive missing data and the use of reconvictions, a conservative criterion to apply to measure relapses in sexual offending behavior given the above-mentioned difficulties in securing convictions in cases of child sexual assault.
The foregoing examples illustrated some inconclusive and inconsistent findings from treatment programs in prison and community-based settings in reducing the sexual recidivism rates of adult sex offenders. The review also highlighted methodological shortfalls that pervade treatment program evaluations, including difficulties in evaluating the impact of treatment across different subtypes of sex offenders. The current study reports on sexual reoffending rates of intrafamilial child sex offenders who were diverted from court to attend a single community-based treatment program.
Methodological Deficits in Past Evaluations of Sexual Offender Treatment Programs
Researchers in the criminological field have lamented the lack of scientific rigor and poor methodological quality of many studies evaluating interventions designed to reduce sexual reoffending (Woodrow & Bright, 2010). For example, fewer than 40% of studies included in the previously cited meta-analysis attained scores of three or more out of a possible maximum of five on the Maryland Scale of Scientific Rigor (Lösel & Schmucker, 2005; Sherman et al., 1997). The current study achieved Level 4 on this scale.
A frequent criticism of methods applied to evaluate sex offender treatment programs is the absence of controls for potential selection biases in the assignment of offenders to treatment versus comparison groups (Rice & Harris, 2003). Selection bias is a difficult element to control within studies evaluating sex offender treatment programs as in many instances participation in treatment is mandated by a sentencing order (Chung et al., 2006). To overcome the documented methodological shortcomings, the Campbell Collaborative Outcome Data Committee on Sexual Offender Treatment Outcome Research specified a protocol (the Campbell Protocol) for sex offender treatment program evaluations to increase their robustness (Beech et al., 2007). The Campbell Protocol recommended the random assignment of participants to treatment and comparison conditions to avoid selection bias and, where that is not possible, assessment prior to treatment on risk-relevant variables and matching on risk levels prior to assignment to treatment (Beech et al., 2007). The current study met these constraints by means of propensity matching analysis. The Campbell Protocol also recommended a follow-up period of a minimum of 3 to 5 years to allow sufficient time to detect recidivism at a minimal level (Beech et al., 2007). The current study included an extensive follow-up period.
Purpose of this Study
Few studies on the effectiveness of community-based diversion programs that treat sex offenders have included a scientifically rigorous methodology, and fewer have evaluated samples of intrafamilial sex offenders. The aim of this study was to measure the effectiveness of a community-based, pretrial diversion program that treats adult intrafamilial child sex offenders by comparing rates of sexual recidivism in participants who were accepted for treatment (accepted group) with those of participants who were declined treatment (declined group). To test whether sexual recidivism rates were lower and periods of desistance were longer for participants in the accepted group versus the declined group, a methodology that met the Campbell Protocol when randomization was not possible was applied. The study addressed some of the methodological shortcomings of previous research by use of (a) retrospective propensity analysis to provide a statistical control for selection biases in the accepted and declined groups, (b) a follow-up period ranging from 2.8 to 18 years, and (c) a more inclusive measure of recidivism than conviction rates (Payne, 2007).
Cedar Cottage Pretrial Diversion Program
The community-based treatment program under review is based in Sydney, Australia, and administered by the New South Wales Department of Health. Known locally as Cedar Cottage or the Pretrial Diversion Program for Child Sex Offenders (the Program), it treats offenders who were in a parental role with a victim younger than 18 years of age at the time of the offense(s).
Offenders charged with a sexual offense (indecency, indecent assault, and penetrative sexual assault) are referred to the Program by the NSW Police Force or the Director of Public Prosecutions in accordance with the NSW Pre-Trial Diversion of Offenders Act (1985). To be eligible for the Program, treatment candidates must be older than 18 years of age, have no prior conviction for a sexual offense, and plead guilty to all intrafamilial sex offenses with which they have been charged and the intrafamilial sex charges cannot involve overt use of force or violence or have occurred in the presence of third parties. Offenders accepted into the Program must accept responsibility for their offending and demonstrate some insight into the impact of their behavior on the victim and the family by making statements about the offending behavior that match those provided to the police by the victim (Pratley & Goodman-Delahunty, 2011).
On entry into the Program, a conviction is recorded against the offender’s name and registration of the sex offender proceeds under the Child Protection (Offenders Registration) Act (2000). Treatment lasts for two years, with an optional third year. Offenders who do not qualify, who are not accepted into, or who breach the conditions of the Program return to court for traditional court procedures. The Program has the capacity to treat 25 offenders per year, and an average of six family members per offender receive counseling to strengthen relationships among the victim, the nonoffending parent, and siblings. Treatment offered is based on CBT, narrative therapy, invitational practice, and insight-oriented therapy with a strong emphasis on relapse prevention (Pratley & Goodman-Delahunty, 2011). Further details about the Diversion Program are available from Cedar Cottage at http://www.swahs.nsw.gov.au/services/cedarcottage/.
Method
Research design
A retrospective quasi-experimental research design was applied in this study. The treatment variable in the study had two levels: offenders accepted into the Program (coded as 1) and offenders who were declined entry into the Program and experienced the regular court process (coded as 0). The accepted group (n = 92) was defined on the basis of intention to treat and comprised participants who were offered a place in the Program without distinguishing treatment completers from noncompleters.
Of the 92 participants who composed the accepted group, 58% (n = 53) completed treatment within the Program and 42% (n = 39) did not complete the Program (32 breached the terms of the Program and 7 voluntarily withdrew from the Program before completion). The declined group (n = 120) were intrafamilial sex offenders who were referred to the Program but were declined treatment and attended traditional court and sentencing procedures. Participants were declined entry if they did not meet the statutory criteria specified above or were deemed unsuitable by the Program Director.
Before comparing the two groups on sex offending outcomes, propensity score matching was conducted to control for known differences between the accepted and declined groups. Groups were compared on outcomes related to their absolute risk of sexually reoffending, time to sexually reoffend, and relative risk reduction in sexual offending.
Although a sample of 212 intrafamilial sex offenders is relatively large in comparison to prior studies of this sex offender subgroup, it is small in terms of evaluating the effectiveness of a treatment program using quantitative methods. An analysis of the statistical power of the research design was conducted (Rosner, 2006). Using an effect size consistent with that found for similar treatment programs of a 6% point difference, with an alpha value of .05 and a sample of 212, the power of the design was estimated as .45. This indicated a 45% chance of finding a statistically significant difference when there is an actual difference of 6% between the treatment and control groups and is a low level of statistical power.
Participant Sample
All 214 adult child sex offenders referred by the New South Wales Courts to the Diversion Program between 1989 (the Diversion Program’s inception) and 2003 were eligible participants. A separate study drawing on the same sample compared 96 biological and 118 nonbiological fathers with respect to their demographic features, characteristics of the index victim and index offense, prior offending, and sexual, violent, and nonviolent recidivism (Titcomb, Goodman-Delahunty, & Waubert de Puiseau, 2012).
Two offenders were excluded from further analyses: one participant who died soon after his last contact with the Program and one participant whose file lacked sufficient information about variables relevant to this study. Therefore, analyses were conducted on a participant sample of 212.
Of the participants, a relatively small proportion was Indigenous (6.6%, n = 14). The remaining participants identified as Caucasian. At the time of the index offense, participants ranged in age from 23 to 68 years (M = 39.60, SD = 7.54), with a majority (44.3%, n = 94) between 35 and 43 years of age. As displayed in Table 1, participants in the accepted and declined groups were comparable on most demographic variables. Employment history was the sole variable that differed more widely in the two groups: Accepted participants had a more stable employment history than did declined participants.
Demographic Characteristics of Participants in Accepted and Declined Groups
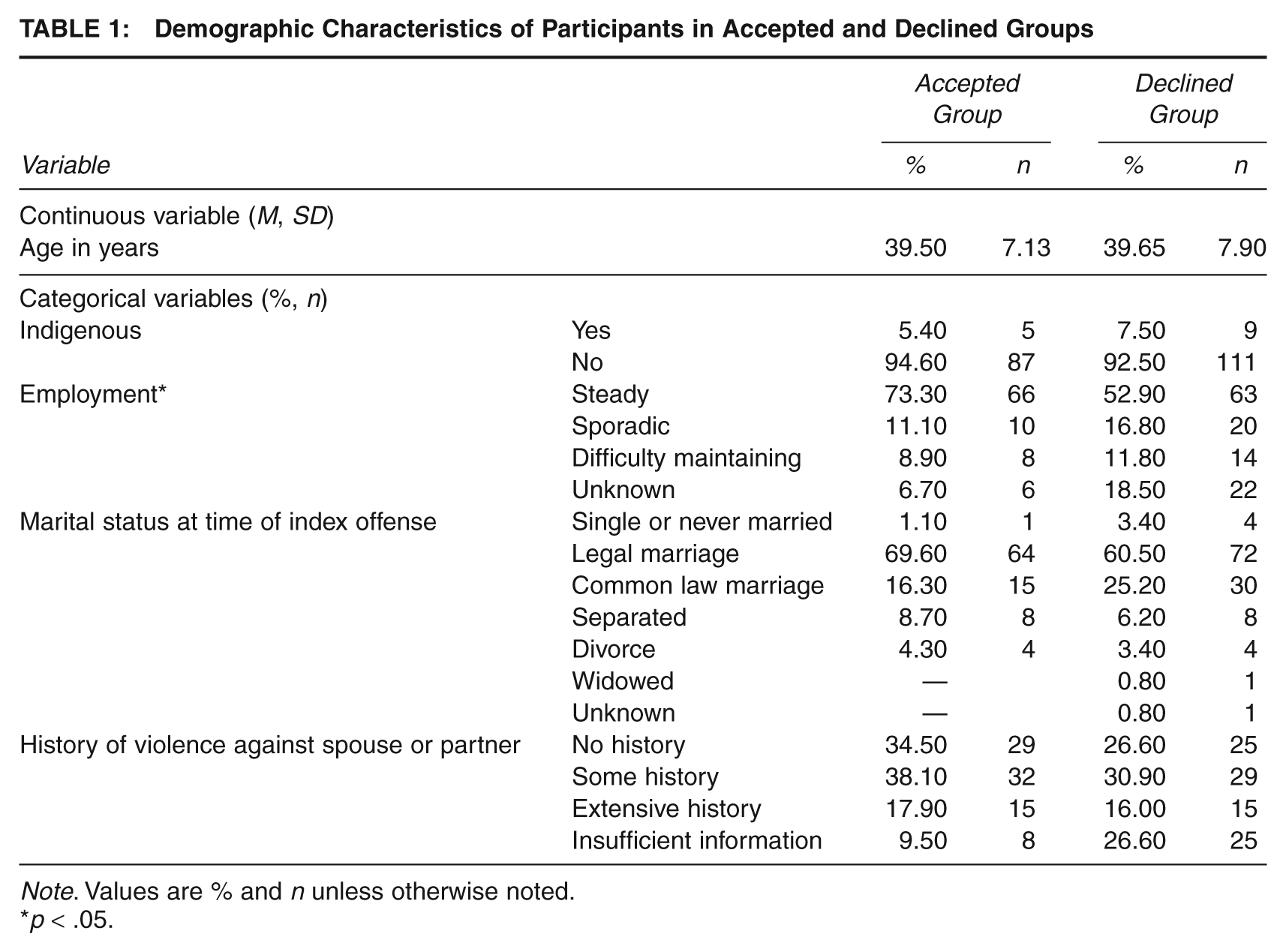
Note. Values are % and n unless otherwise noted.
p < .05.
Table 2 displays the proportion of each index offense-related characteristic in the accepted and declined groups. On most index offense characteristics, the groups of participants were similar; two characteristics revealed larger differences. Participants in the declined group were less varied in their range of sexual offending (committed only one type of sexual behavior; e.g., sexual touching) and were more likely to have abused their victim(s) in an unplanned and impulsive manner compared to participants in the accepted group.
Index Offense Characteristics of Participants in Accepted and Declined Groups
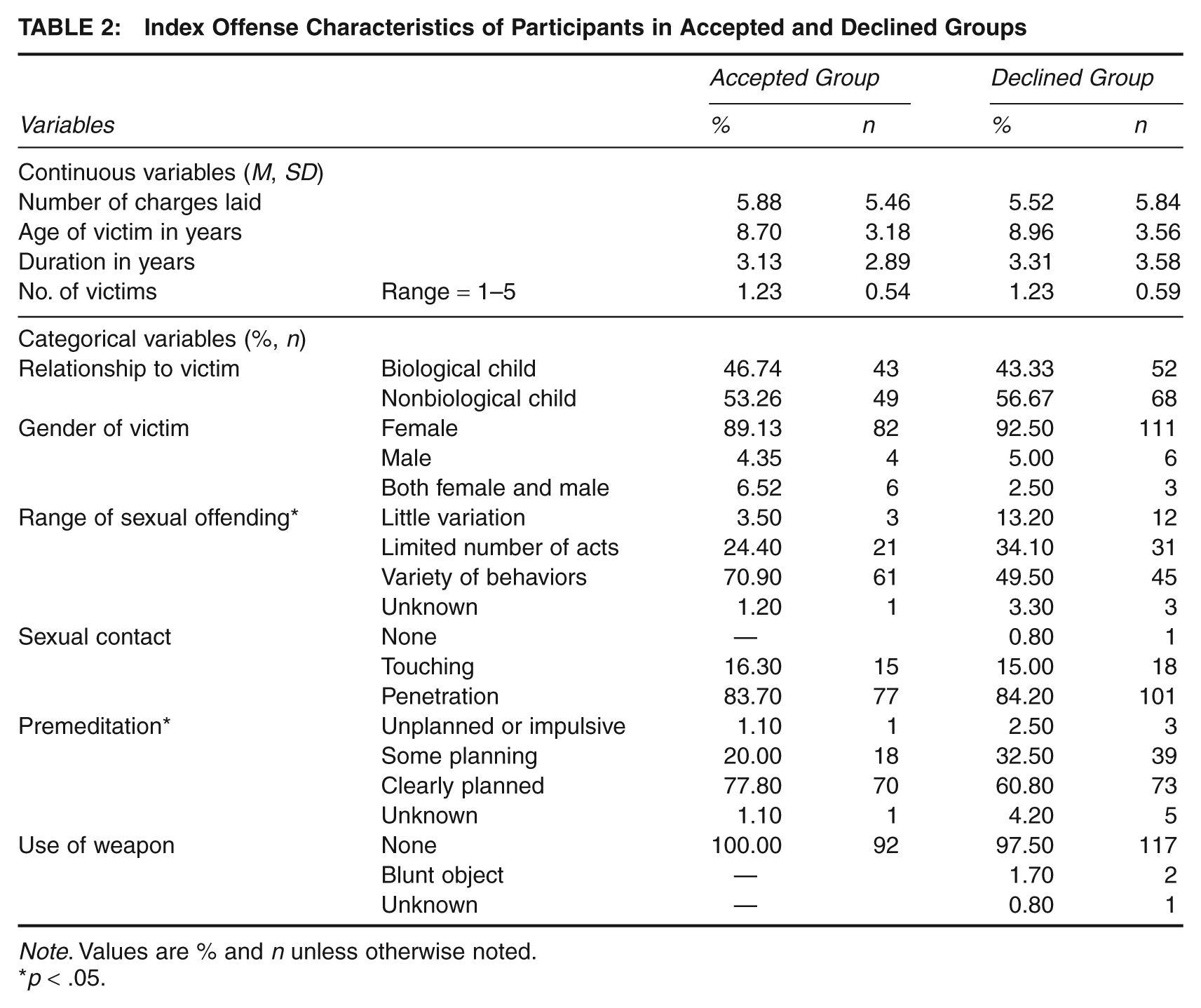
Note. Values are % and n unless otherwise noted.
p < .05.
Table 3 displays the prior offense records of the participant groups. Participants in the declined group had more extensive past offending rates than did accepted participants. Accepted participants were less likely to endorse sexual abuse myths than were their declined counterparts. Otherwise participants in both groups appeared similar in relation to prior offending characteristics.
Prior Offending and Tolerance of Sexual Abuse by Participants in Accepted and Declined Groups
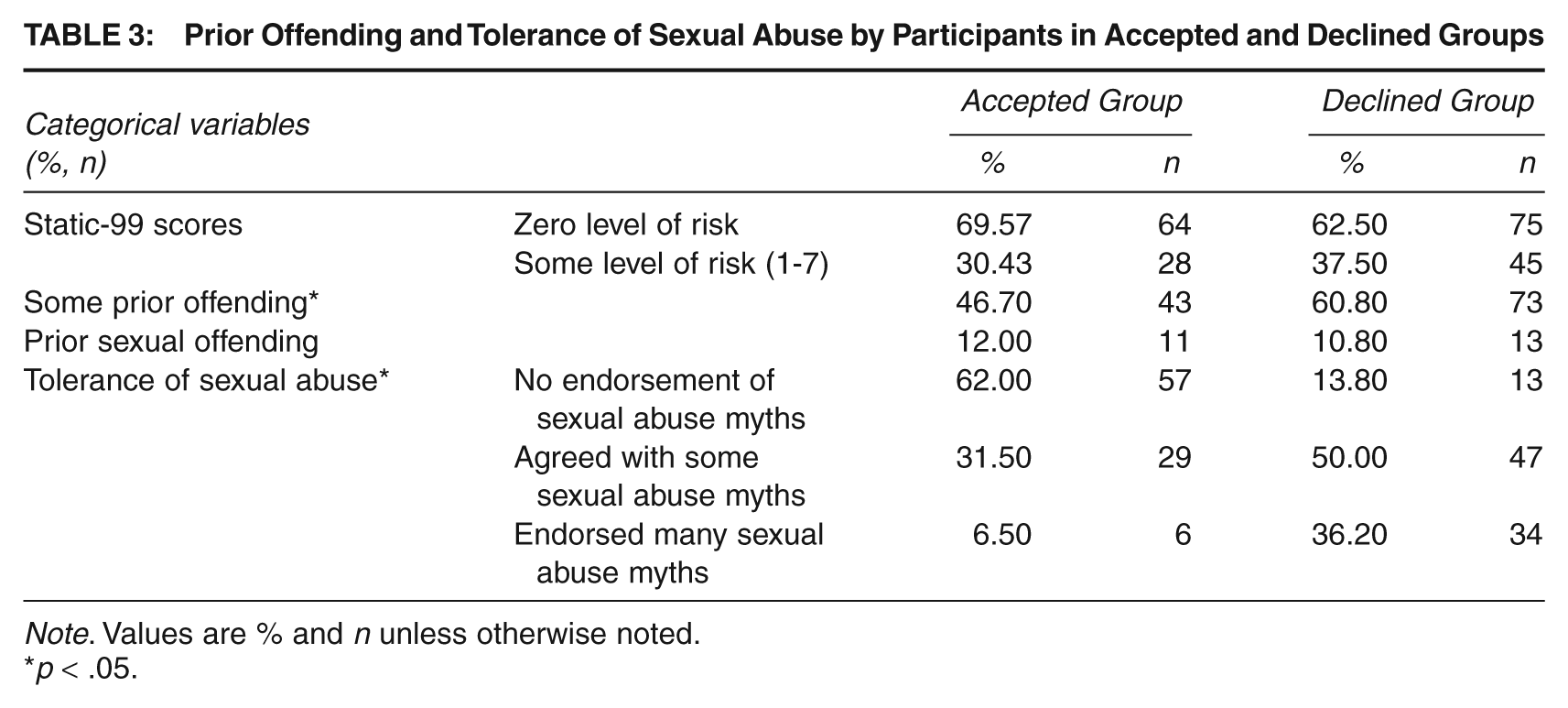
Note. Values are % and n unless otherwise noted.
p < .05.
Data Sources
Diversion program records
A database (the Program Database) containing a total of 116 variables for each participant offender was created by means of a manual audit of each participant’s case file (Goodman-Delahunty, 2009). The coders, 11 graduate-level researchers affiliated with the second author, were double blind to screen them from information regarding participant recidivism. Interrater reliability was assessed by double coding 25 randomly selected cases and computing the kappa statistic for the 60 dichotomous variables (.76), and intraclass correlation coefficients (ICCs) for the 56 continuous variables (.68). All kappa statistics and ICCs were significant (p < .01; one ICC was significant at p < .05).
The extracted data included demographic information, the offenders’ criminal and violent history, and the type of victim of each sexual assault (adults, children, or both). Details of the index offenses (the number of incidents of abuse, the frequency and duration of offending, and the number of charges each participant was facing at the time of referral to the Program) were included along with the degree of sexual contact, the degree of planning or premeditation leading to the offense, and whether threats, physical violence, or weapons were utilized. The offenders’ self-reported reasons for the abuse were noted, as were their employment and marital status at the time of the offense. Victim details (gender, age, relationship to the offender, and the degree of physical and psychological injury sustained) were recorded. Information contained in each offender’s file was used to derive a Static-99 score (Harris, Phenix, Hanson, & Thornton, 2003) for each participant.
Records of offenses
Official records of offending by the participants were obtained from three sources in New South Wales: First, reports made to police, arrests, charges, and convictions were used to code type of offending conduct, specifically sexual offenses (noncontact sexual offenses, indecent assault, and sexual assault), violent offenses, and nonsexual nonviolent offenses before and after the participants contact with the Diversion Program. Second, these data were cross-checked against records of offenses and outcomes maintained by the NSW Bureau of Crime Statistics and Research. Third, data were supplemented by NSW Department of Corrective Services records of periods that any participants were incarcerated (Goodman-Delahunty, 2009).
Dependent Measures of Reoffending
The outcome variable was sexual reoffenses determined by an official report to the NSW Police. Reported sexual reoffenses were defined at the most inclusive level to include sexual reoffenses with adults and extrafamilial and intrafamilial victims including contact and noncontact offenses. Police reports were used in preference to arrest and conviction rates as report rates remain verifiable and were likely to capture with more accuracy the level of sexual reoffending compared to arrest and conviction rates. Although report rates offer a more accurate rate of sexual reoffending compared to arrest or conviction rates, it is acknowledged that report rates may include charges that are subsequently dropped (Gelb, 2007).
The follow-up period was operationalized as the number of days between the date of each participant’s final contact with the Program (on assessment completion, treatment completion, breach or withdrawal) and October 1, 2007. Days when offenders were in custody and unavailable to reoffend were subtracted based on information provided by the Department of Corrective Services to avoid inflating the desistance period. The follow-up period ranged from 2.8 to 18 years for the full participant pool (N = 212), with median follow-up times for the accepted group and declined groups of 4,618 days and 3,451 days, respectively. Cox regression was used to provide a test of treatment effect as it accounts for any impact of differences in follow-up time between the groups (Prentky, Lee, Knight, & Cerce, 1997).
Data Analysis
Statistical procedures to compute the propensity score analysis were performed using STATA IC11 Statistical Software with an add-on procedure called psmatch2 that enables propensity score matching, common support graphing, and covariate balance testing. All statistics were generated using two-tail tests at 95% confidence with alpha set at .05, unless otherwise stated. Pretest differences on categorical characteristics were calculated using Fisher’s exact χ2 test; differences on continuous characteristics were calculated using the Mann–Whitney test.
Procedure: Propensity Score Analysis
Propensity score analysis is a popular technique to estimate causal treatment effects when comparing groups in an observational study while controlling for selection bias (Caliendo & Kopeinig, 2005). Based on each participant’s observed characteristics (e.g., pretreatment demographic and clinical characteristics), statistical analysis is used to calculate the probability of (or propensity for) each participant to receive treatment (Baser, 2006). This procedure combines each participant’s observed differences in characteristics into a single “propensity score.” Next, individual participants in the accepted group are matched to individual participants in the declined group based on nearest matches of propensity scores (Rudner & Peyton, 2006). After accepted and declined participants have been matched and covariate balance established, the outcome variables can be compared—in this case sexual reoffending rates and period of desistance from reoffending (Baser, 2006). Any differences in these outcome measures will be attributable to the Program and not to any known and observed differences that existed between the participant groups before the study began. For a full description of the rationale and methods underlying the use of a propensity score analysis, see Caliendo and Kopeinig (2005), Guo and Fraser (2010), and Joffe and Rosenbaum (1999).
Prior studies were reviewed to determine predictors of acceptance into treatment and factors contributing to sexual recidivism. The selected predictors were cross-checked against the variables available in the Program Database. Sample sizes limit the number of variables that can be included in logistic models (Weitzen, Lapane, Toledano, Hume, & Mor, 2004). Given a sample size of 212 participants, it was not possible to include all potentially relevant variables in the matching procedure. As such, only those variables that were identified as the most important in the literature and that did not suffer from excessive missing data were considered for the logistic regression model used in the propensity score matching analysis.
Using a combination of statistical significance and cross-validation approaches in an iterative process (as specified by Caliendo & Kopeinig, 2005), a logistic regression model was formed to generate a propensity score for each participant for selection into the Program. Unlike a typical regression analysis where the goal is often to build the best predictive model, in propensity score analysis the building of the logistic model is guided primarily by the utility of the model to create samples balanced across all the relevant covariates. As such, the variables ultimately used in the logistic regression model as displayed in Table 4 are those that created the best covariate balance across all available variables between the accepted and declined groups. Several variables were recoded for use in the logistic model (participants’ age at referral to the Program, number of victims, number of index charges, employment history) either because some cell sizes were too small or lacked a distribution approximating normality or because the logistic model performed better. Interactions among variables were not analyzed in this study.
Logistic Regression Model to Estimate Propensity Scores

Kernel matching (with a bandwidth of .06) was used to match participant cases in the accepted group to cases in the declined group. To assess how well the matching procedure balanced the distribution of all known relevant covariates in the accepted and declined groups, the researchers considered descriptive statistics, t test comparisons, and Rosenbaum and Rubin’s (RR) standardized bias estimate (Rosenbaum & Rubin, 1985). There are, however, no clear criteria in the literature to determine when balance is achieved, as common t tests can be misleading because of the impact of sample size and variability on significance. Since standardized bias estimates take into consideration variability as well as difference, a standardized bias estimate less than 5% is regarded as sufficient to assume covariate balance (Caliendo & Kopeinig, 2005).
After matching, sexual recidivism rates in the two groups were compared. The marginal effect was calculated using probit analysis which increased the interpretability of the estimates given the binary outcome measures in this research (Hill, 2008). Cox proportional hazards regression (with failure rate) were performed to evaluate differences between the matched groups in the time it took for participants to reoffend sexually within the follow-up period. Cox regression was used rather than Kaplan–Meier survival analyses because of the need to include analysis weights from the propensity score matching procedure in the model. Consistent with the Campbell Protocol recommendation (Villettaz et al., 2006), we also provided estimates of the relative improvements in recidivism rates of the accepted versus declined groups matched samples (relative risk reduction or RRR). The RRR is the difference in event rates (in this case, sexual recidivism rates) between two groups, expressed as a proportion of the event rate in the untreated (declined) group (Cook & Sackett, 1995).
Results
Propensity score analysis
Overall, the logistic regression model (Table 4) was predictive of treatment, and pseudo-R2 revealed that the equation explained 33.2% of variation in the choice (LRχ2 = 33.20, p < .01). The logistic regression model fitted the data well (Hosmer–Lemeshow test: p = .77), with reasonable discrimination (c statistic = .72). An excellent discrimination of the propensity score model is not ideal as such a result could lead to little or no overlap of the estimated propensity score between the groups, making it impossible to conduct matching (Weitzen et al., 2004). The Kernel matching procedure left four participant cases in the accepted group that could not be matched to another participant in the declined group because of dissimilar propensity scores. These cases were discarded from the analysis, leaving a sample of 208 cases: A total of 88 in the accepted group were matched to 120 in the declined group.
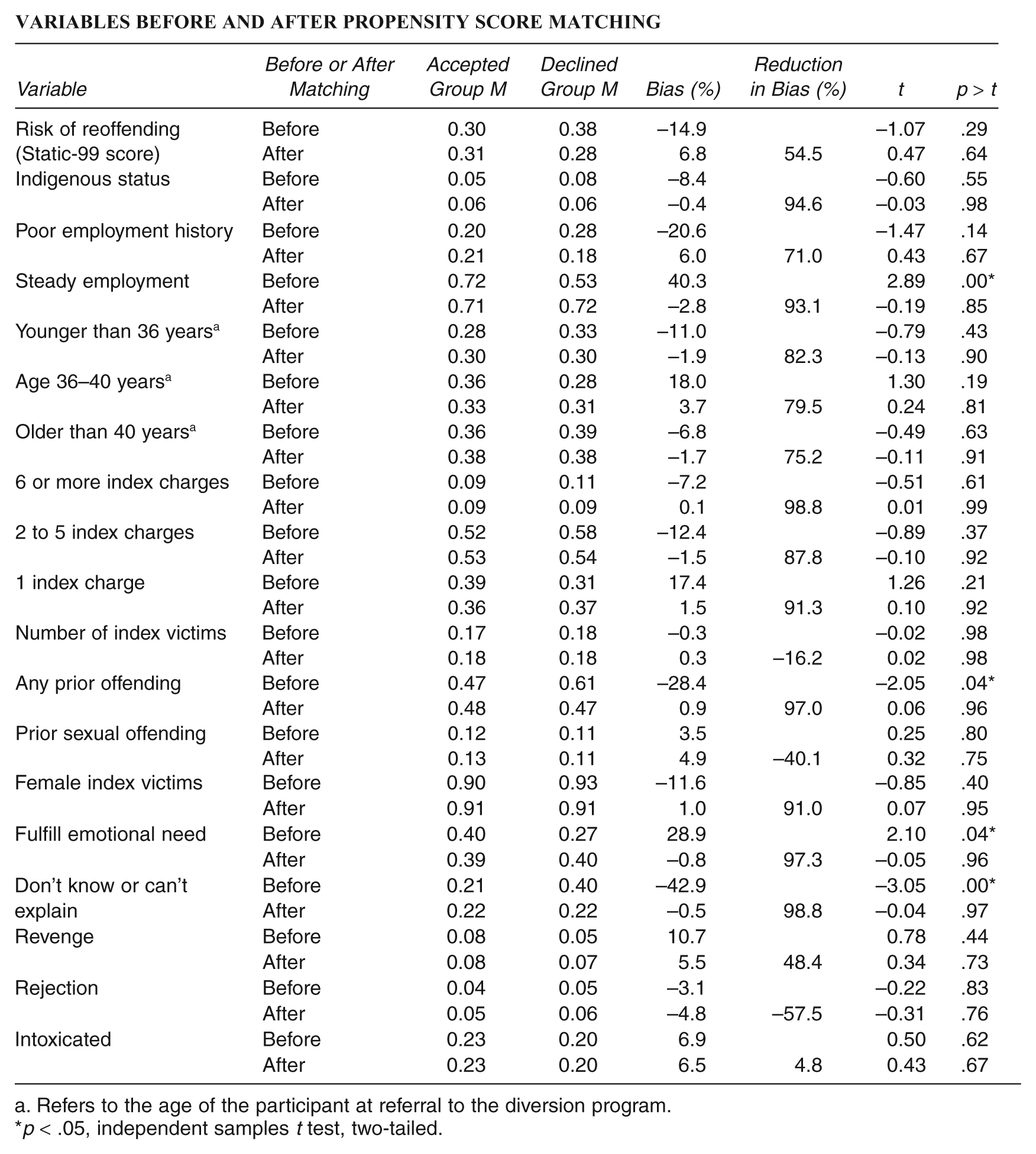
Figure 1 displays the percentage point differences for each variable between the accepted and declined groups before and after matching, illustrating how prematching differences were reduced in absolute terms. Provided in the appendix are RR standardized bias estimates and tests of differences before and after matching for each variable. After matching, no differences between the accepted and declined groups were statistically significant. In terms of RR estimates, all variables except four fell below the 5% threshold suggested as sufficient by Caliendo and Kopeinig (2005). Of the four variables above 5%, all differences were relatively small (Rosenbaum & Rubin, 1985), with none above 6.8%. The RR estimates for these variables were as follows: binary Static-99 = 6.8%, poor employment history = 6.0%, revenge motivated offense = 5.6%, and intoxication at the time of offending = 6.5%. Examination of the direction of these potential biases after matching, for all four variables, revealed higher bias estimates after matching of the presence of these risk factors among more participants in the accepted than the declined group, as shown in Figure 1. Thus, this analysis suggested that in terms of known variables, if there was any remaining selection bias, the likely result of this bias would predict more reoffending in the accepted than the declined group.
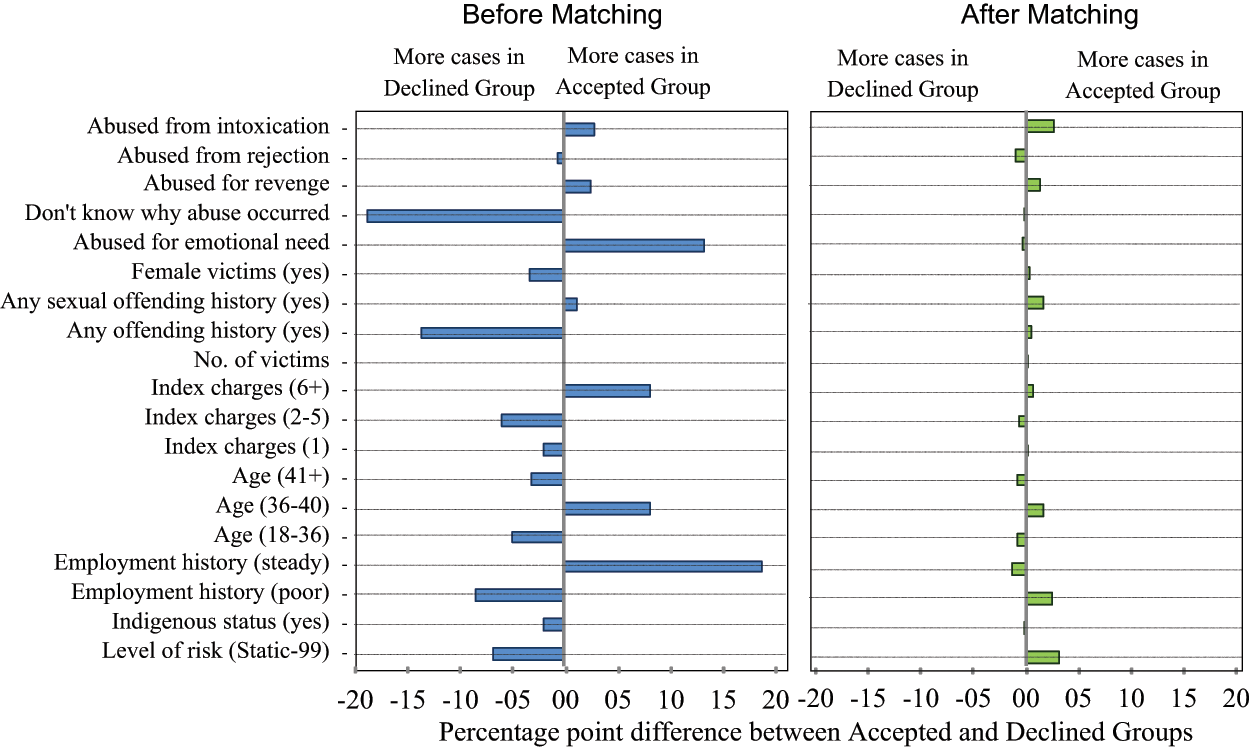
Covariate Balance Achieved Before and After Kernel Matching
Occurrence of Sexual Reoffending
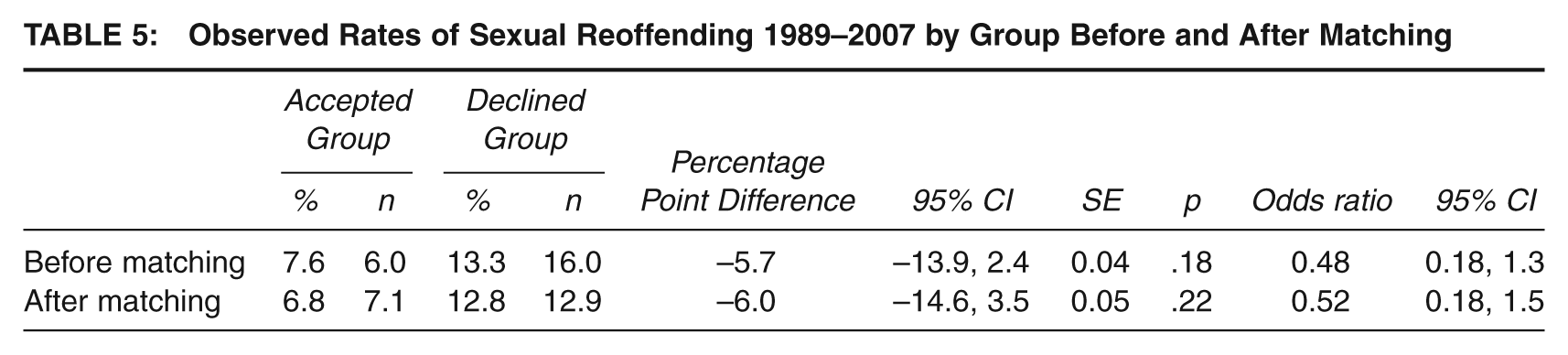
Table 5 displays a comparison of mean and standard deviation scores for sexual reoffending by participants before and after matching. After matching, results yielded a percentage point difference of 6.0 during the follow-up period, as participants who were accepted into the Diversion Program sexually reoffended at a lower rate (6.8%, n = 7.1) than participants who did not receive treatment and who experienced the regular court procedures and sanctions (12.8%, n = 12.9). The estimated effect size of treatment, expressed as an odds ratio, was 0.52 (95% CI = 0.18, 1.5). In other words, treatment reduced the risk of reoffending by 50%. When the incidence of outcomes is rare in the study population, generally interpreted to mean less than 10%, as is the case with sexual reoffending rates, the odds ratio is considered a good estimate of the risk ratio. Probit analysis showed that the magnitude of the reduction in sexual reoffending did not achieve statistical significance (SE = 0.05, p = .22, CI = −0.15, 0.03).
Observed Rates of Sexual Reoffending 1989–2007 by Group Before and After Matching
Period of Desistance from Sexual Reoffending
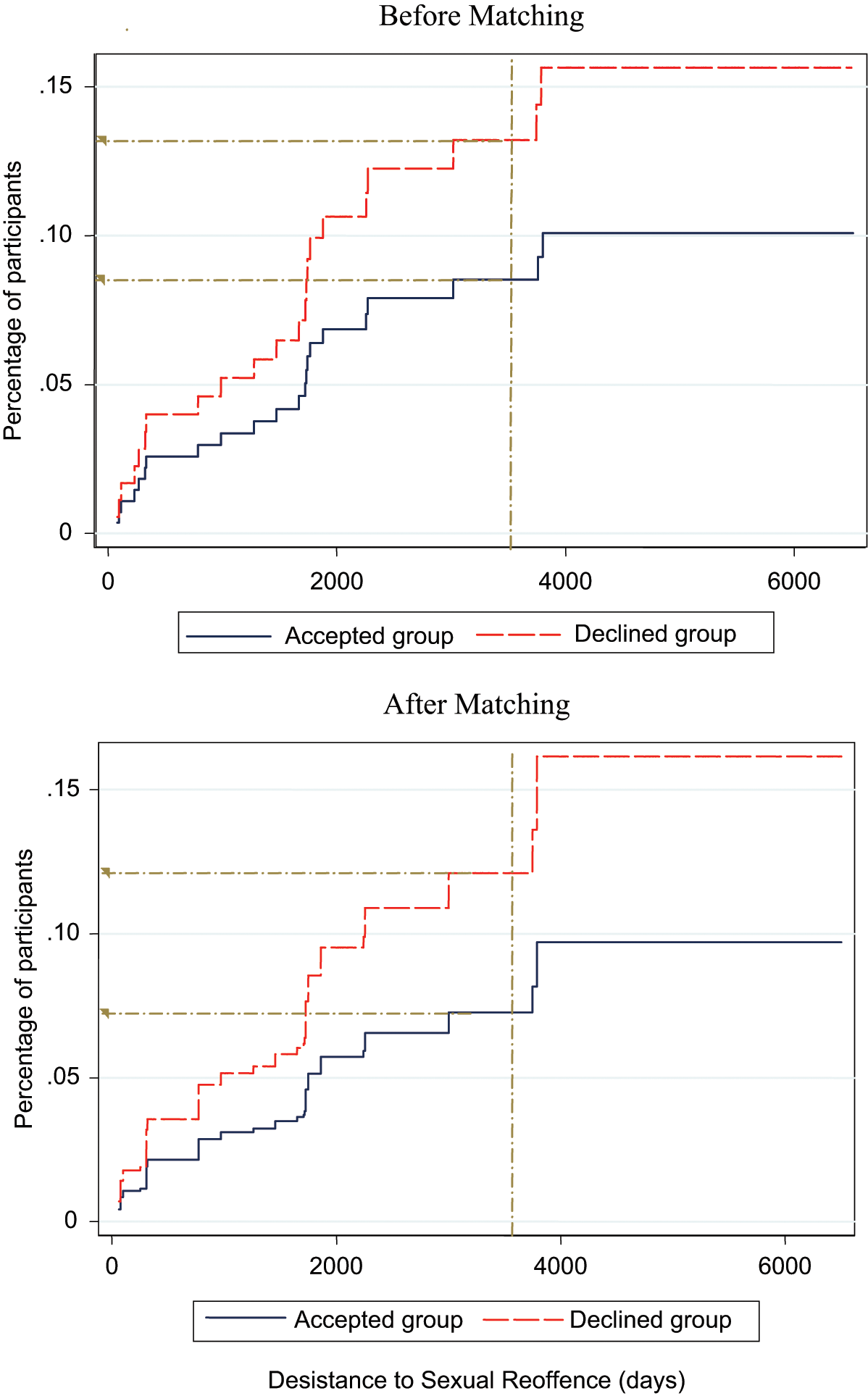
Cox proportional hazards regression analysis with failure rate (see Figure 2) showed that after matching, at a median time of 3,468 days (9.5 years), the failure rate for reported sexual offenses in the accepted group was approximately 7% compared to an approximate failure rate of 12% in the declined group. The difference in failure rates between the two groups was not statistically significant: HR 95% CI = 0.60 (0.21, 1.69), p = .334. There was no evidence that the proportional hazards assumption was violated: χ2(1, N = 208) = 1.58, p = .21.
Cox Proportional Hazards Analysis of Sexual Recidivism in Accepted and Declined Groups Before and After Matching (1989–2007)
Relative Risk Reduction
Computation of the RRR yielded an outcome of 47% (12.8 – 6.8/12.8 × 100) indicating that the Program is estimated to reduce sexual recidivism in adult male intrafamilial child sex offenders by 47%.
Discussion
This study examined whether exposure to a CBT community-based diversion program reduced sexual reoffending rates in adult male intrafamilial child sex offenders by comparing reoffense rates in a group accepted for treatment with those in a group declined treatment. This study also examined whether exposure to the Program extended the period of desistance from sexual reoffending in either participant group. A common concern in evaluations of treatment programs is whether unaccounted-for selection bias is responsible for observed estimates of treatment effects rather than the treatment program itself (Rice & Harris, 2003). Selection bias was explicitly managed in this study by propensity score analysis. The standardized bias estimates and percentage point differences between the participant groups on selected variables before and after matching (see Figure 1) confirmed that propensity score matching successfully created a comparison group similar to the accepted group on the reviewed variables. The Kernel matching procedure provided assurance that the two groups were well matched on factors that commonly influence sexual reoffending. Results of these analyses demonstrated that any selection bias related to any of these variables was controlled. Therefore, observed differences in estimated recidivism rates in the two groups can more confidently be attributed to the effect of the treatment intervention in the Program.
Reduction in Sexual Reoffending
A comparison of the proportion of participants who sexually reoffended before and after matching (a 6% point difference) indicated that participants who were accepted into the Program sexually reoffended less than participants who did not receive treatment and who experienced the regular court procedures during the follow-up period. This result is consistent with previous research outcomes documented in meta-analyses that evaluated treatment effects in more heterogeneous groups of sex offenders (Hanson et al., 2002). Although the Probit analysis showed the magnitude of the reduction in sexual reoffending did not achieve statistical significance, the overall effect size for treatment was large. The lack of statistical significance when evaluating a single sex offender treatment program is unsurprising (Craig et al., 2003; Kingston et al., 2008) given the small number of reoffenders and the low rate of sexual reoffending in this study (7% in the accepted group, 13% in the declined group), producing low statistical power to detect the effects of treatment. The RRR of 47% implied that in a given population, if 100 sex offenders are expected to reoffend, after diversion to Cedar Cottage, the number likely to sexually recidivate will be reduced to 47, or just fewer than one half.
In conformity with the principle of intent to treat (Hollis & Campbell, 1999), participants in the accepted group included offenders who failed to complete treatment at the Program. Of the 92 participants composing the accepted group (before propensity score analysis was applied), approximately three fifths (58%, n = 53) completed treatment and two fifths (42%, n = 39) withdrew or were breached from the Program before completion. Since participants who drop out of treatment programs often recidivate at higher rates than do treatment completers (Hanson et al., 2002), the reduction in sexual recidivism rates observed in the current study is likely to underestimate the effectiveness of the treatment at the Program.
A more fine-grained examination of the seven participants in the accepted group who sexually reoffended within the follow-up period confirmed that the Program produced positive treatment effects. Of the seven recidivists, four had completed treatment, whereas three breached or withdrew before completion. Three of the four completers who sexually recidivated were referred to the Program in the first few years of its operation before legislative and regulatory amendments were implemented in April 1993. One reoffense recorded in that period was a charge of willful and obscene exposure 8 years after treatment completion against an offender with paranoid schizophrenia who was observed walking naked in his yard a few hours after he learned of the death of his victim. No conviction ensued. After 1993, more extensive assessment procedures were adopted by the Program. The report of an offense in the case of the participant who completed treatment after the changes in 1993 was by an adult coworker for peeping and prying when she recognized his face outside her window. This conduct involved no sexual contact and did not involve a minor, and no charge, arrest, or conviction ensued. In all, four of the seven sexual reoffenses committed by offenders referred to the Program were noncontact offenses; three were penetrative sexual reoffenses, two by offenders who completed treatment in the first few years of the Program operation, one by a noncompleter. The overall recidivism data showed that in the 14 years between 1993 and the end of the follow-up period in 2007, no official police reports or convictions of any sexual offense against a minor were made regarding any of the 34 participants who completed treatment in the Program.
As a whole, this study demonstrated the usefulness of propensity score analysis to overcome selection bias and produce empirically sound findings on the effectiveness of sex offender treatment programs where randomized trials are infeasible. These results demonstrated that the Cedar Cottage Diversion Program reduced sexual reoffending in adult male intrafamilial child sex offenders and that community-based programs to rehabilitate low-risk intrafamilial child sex offenders can be effective.
Limitations of the Study
As with all studies, certain limitations in this research must be acknowledged. Foremost among these is a limitation in the available information about offenders because of the retrospective nature of this study. Reoffending rates in this research were derived from records maintained by authorities within the state of New South Wales. Therefore, any reoffending on the part of participants that may have occurred outside of New South Wales was not recorded or included. This omission may have led to an underestimation of recidivism. Propensity score matching cannot control for unobserved selection bias (Guo & Fraser, 2010).
Other caveats include the fact that this research was conducted using a participant group exposed to only one particular diversion program. Although it is a strength of this study that all offenders referred to the Program in the period 1989–2003 were included and monitored for up to 18 years, whether these findings may generalize to other diversionary programs or other treatment program facilities is unknown. The delivery and efficacy of the Program and the precise causes of the reduction in sexual reoffending observed at the Program remain unknown. As time passed, the proportion of offenders referred to the Program who were accepted for treatment increased. For example, in the period 2004–2008, of the 29 referrals, 8 were declined and 20 or 69% were accepted (D. Tolliday, personal communication, July 7, 2008). With the passage of time, the efficacy of the Program appeared to improve. For example, recidivism data for all 138 offenders referred to Cedar Cottage in the period 1993–2004, of whom 64 were accepted for treatment, revealed no official police reports or convictions of any sexual offense against a minor by any of the 34 offenders who completed the Program. The turnover of staff and legislative changes indicated that the quality of the implementation of the Program varied in the years since its inception in 1989. These factors need to be investigated in future research.
Future Research
As discussed, the areas of limitation have given rise to the recommendation of areas of future research. Future research should also be implemented to address factors that fall outside the scope of this study that go toward highlighting the success of the Diversion Program. For example, at the Program, in addition to the rehabilitation of sex offenders, the family members of each offender, including the child victim(s), receive counseling to come to terms with their situation (Goodman-Delahunty, 2009). The design and implementation of the Diversion Program also spares child victims the burden of testifying in legal proceedings and increases the disclosure of further offenses that would otherwise have remained undetected (Pratley & Goodman-Delahunty, 2011). A preliminary estimate of the cost per offender of attending the Program was no different from the cost of traditional incarceration (Goodman-Delahunty, 2009). These potentially positive effects should be analyzed in future research to add to the evaluation of the effectiveness of the Program.
Offender motivation can be an important predictor of both treatment volunteerism and treatment entry among incarcerated adult sex offenders who victimize children (Jones, Pelissier, & Klein-Saffran, 2006). Reductions in sexual recidivism in participants who enter any sex offender treatment program may reflect levels of motivation rather than the effectiveness of the treatment program (Campbell, 2004). Further research is under way to assess the influence of dynamic risk factors in this sample using the Violence Risk Scale-Sexual Offender Version (Wong & Olver, 2010).
Conclusions
This study contributed to the growing body of evidence on practices for the successful management and treatment of intrafamilial child sex offenders in the community, as shown by the lowered sexual recidivism rates and increased desistance to sexual reoffending in the offenders who completed this community-based pretrial diversion program. Given the devastating impact that sexual abuse can have on child victims (AIHW, 2009b) and the dire consequences that victims and their family members can face after disclosures of sexual abuse (Taylor & Gassner, 2010), the reduction in the frequency of sex offending achieved by the Cedar Cottage Diversion Program contributed dramatically to reduce considerable human suffering. There were 3,875 substantiations of notifications of sexual abuse received during 2007–2008 for children aged between 0 and 16 years residing in New South Wales (AIHW, 2009a). If each child was sexually abused by one offender, and those offenders had an expected sexual recidivism rate of 12.8% as was observed in the group declined treatment, 496 additional children would be sexually abused by these offenders. However, if these potential reoffenders attended Cedar Cottage, the estimates produced in this study suggested that some 232 of these 496 children would be spared from sexual abuse.
Strengths of the study include the reduced heterogeneity in sample composition by focusing exclusively on intrafamilial sex offenders, a longer mean follow-up time than many comparable studies, a broad official outcome source to measure recidivism (police reports rather than arrests or convictions), and a statistical control for selection bias between treated and untreated groups. This study followed the Campbell Protocol and achieved Level 4 on the Maryland Scale of Scientific Rigor, securing its place among the small minority of studies (fewer than 10% per Lösel & Schmucker, 2005) that have sufficient methodological controls over treated versus untreated groups to draw meaningful inferences about the impact of the diversion program on sexual reoffending rates. The findings in this study contribute uniquely and substantially to the Australian and international research literature on a subgroup of adult sex offenders about whom relatively little is known. These findings can inform legislators, policy makers, the judiciary, members of the legal profession, and the general public of the potential success of diversionary programs in managing sexual offenders in the community.
Footnotes
Appendix
Variables Before and After Propensity Score Matching
| Variable | Before or After Matching | Accepted Group M | Declined Group M | Bias (%) | Reduction in Bias (%) | t | p > t |
|---|---|---|---|---|---|---|---|
| Risk of reoffending (Static-99 score) | Before | 0.30 | 0.38 | −14.9 | −1.07 | .29 | |
| After | 0.31 | 0.28 | 6.8 | 54.5 | 0.47 | .64 | |
| Indigenous status | Before | 0.05 | 0.08 | −8.4 | −0.60 | .55 | |
| After | 0.06 | 0.06 | −0.4 | 94.6 | −0.03 | .98 | |
| Poor employment history | Before | 0.20 | 0.28 | −20.6 | −1.47 | .14 | |
| After | 0.21 | 0.18 | 6.0 | 71.0 | 0.43 | .67 | |
| Steady employment | Before | 0.72 | 0.53 | 40.3 | 2.89 | .00* | |
| After | 0.71 | 0.72 | −2.8 | 93.1 | −0.19 | .85 | |
| Younger than 36 years a | Before | 0.28 | 0.33 | −11.0 | −0.79 | .43 | |
| After | 0.30 | 0.30 | −1.9 | 82.3 | −0.13 | .90 | |
| Age 36–40 years a | Before | 0.36 | 0.28 | 18.0 | 1.30 | .19 | |
| After | 0.33 | 0.31 | 3.7 | 79.5 | 0.24 | .81 | |
| Older than 40 years a | Before | 0.36 | 0.39 | −6.8 | −0.49 | .63 | |
| After | 0.38 | 0.38 | −1.7 | 75.2 | −0.11 | .91 | |
| 6 or more index charges | Before | 0.09 | 0.11 | −7.2 | −0.51 | .61 | |
| After | 0.09 | 0.09 | 0.1 | 98.8 | 0.01 | .99 | |
| 2 to 5 index charges | Before | 0.52 | 0.58 | −12.4 | −0.89 | .37 | |
| After | 0.53 | 0.54 | −1.5 | 87.8 | −0.10 | .92 | |
| 1 index charge | Before | 0.39 | 0.31 | 17.4 | 1.26 | .21 | |
| After | 0.36 | 0.37 | 1.5 | 91.3 | 0.10 | .92 | |
| Number of index victims | Before | 0.17 | 0.18 | −0.3 | −0.02 | .98 | |
| After | 0.18 | 0.18 | 0.3 | −16.2 | 0.02 | .98 | |
| Any prior offending | Before | 0.47 | 0.61 | −28.4 | −2.05 | .04* | |
| After | 0.48 | 0.47 | 0.9 | 97.0 | 0.06 | .96 | |
| Prior sexual offending | Before | 0.12 | 0.11 | 3.5 | 0.25 | .80 | |
| After | 0.13 | 0.11 | 4.9 | −40.1 | 0.32 | .75 | |
| Female index victims | Before | 0.90 | 0.93 | −11.6 | −0.85 | .40 | |
| After | 0.91 | 0.91 | 1.0 | 91.0 | 0.07 | .95 | |
| Fulfill emotional need | Before | 0.40 | 0.27 | 28.9 | 2.10 | .04* | |
| After | 0.39 | 0.40 | −0.8 | 97.3 | −0.05 | .96 | |
| Don’t know or can’t explain | Before | 0.21 | 0.40 | −42.9 | −3.05 | .00* | |
| After | 0.22 | 0.22 | –0.5 | 98.8 | –0.04 | .97 | |
| Revenge | Before | 0.08 | 0.05 | 10.7 | 0.78 | .44 | |
| After | 0.08 | 0.07 | 5.5 | 48.4 | 0.34 | .73 | |
| Rejection | Before | 0.04 | 0.05 | −3.1 | −0.22 | .83 | |
| After | 0.05 | 0.06 | −4.8 | −57.5 | −0.31 | .76 | |
| Intoxicated | Before | 0.23 | 0.20 | 6.9 | 0.50 | .62 | |
| After | 0.23 | 0.20 | 6.5 | 4.8 | 0.43 | .67 |
Refers to the age of the participant at referral to the diversion program.
p < .05, independent samples t test, two-tailed.
This article is part of a special issue titled “Diversion from Standard Prosecution”, edited by Kirk Heilbrun and David DeMatteo of Drexel University. This research was supported by funding from the School of Psychology, Charles Sturt University and Sydney West Area Health Service. The authors acknowledge the support of the NSW Police and Cedar Cottage staff, in particular A/Clinical Advisor Dale Tolliday, A/Program Director Karen Parsons, and Treatment Coordinator Jessica Pratley.