
Abstract
This study was designed to assess satisfaction with methadone treatment (MT) in a multidimensional manner among prison inmates and to identify significant independent predictors of inmates’ satisfaction with MT. A total of 158 prison inmates, who were currently on MT for at least the past 3 months, were assessed with the Verona Service Satisfaction Scale for MT. Inmate participants reported slight satisfaction with MT (3.1 on a 1-5 scale), with 51.3% of them feeling dissatisfied. Three factors were found to be independently associated with satisfaction with MT: HIV infection, odds ratio (OR) = 3.72, 95% confidence interval (CI) = [1.79, 7.73]; number of MT episodes, OR = 0.68, 95% CI = [0.53, 0.88]; and perceived influence on methadone dose changes, OR = 1.69, 95% CI = [1.25, 2.28]. Given that perceived involvement in treatment decisions is the only variable independently associated with MT satisfaction that can be modified by changing how MT is implemented, patient participation should be promoted and supported.
Treatment programs for drug-dependent inmates were established in Catalonia, Spain, at the end of the 1980s, when many illegal drug users—40% of whom were intravenous drug users (IDUs)—were incarcerated (Marco, 1997). According to a government survey published in 2007 (survey on health and drug consumption in penitentiary institutions; Delegación del Gobierno para el Plan Nacional sobre Drogas & Secretaría General de Instituciones Penitenciarias, 2007), 41.6% of inmates surveyed had consumed heroin at least one time in their life and 25.9% admitted at least one instance of intravenous drug use; in addition, 11.7% of inmates had injected drugs in the month prior to incarceration and 1.3% had done so in the past 30 days (Delegación del Gobierno para el Plan Nacional sobre Drogas & Secretaría General de Instituciones Penitenciarias, 2007).
Methadone treatment (MT) has been one of the most widely used treatments for heroin addiction in the past two decades. In the year 2009, approximately 700,000 opioid consumers in Europe received substitution treatment, with most (75%) taking methadone as the substitutive drug (European Monitoring Centre for Drugs and Drug Addiction, 2011). MT was not utilized in Spanish prisons until a pilot program was initiated in Barcelona in 1992 (Mallada & Marco, 1993; Marco, Mallada, García, Boguña, & Ballester, 1995). Since then, MT programs have been widely implemented in Catalonia and in the rest of Spain. In 2008, 20,290 inmates (1,749 in Catalonia and 18,541 in other parts of Spain) received MT (Delegación del Gobierno para el Plan Nacional sobre Drogas, 2010).
MT is effective as a drug therapy or risk reduction intervention for heroin dependence in the extra penitentiary setting, as numerous studies have shown (Amato et al., 2005; Gowing, Farrell, Bornemann, Sullivan, & Ali, 2011; Mattick, Breen, Kimber, & Davoli, 2009; Sullivan, Metzger, Fudala, & Fiellin, 2005). MT is also effective among the prison population (Hedrich et al., 2012; Larney, 2010). According to the principle of equivalence of care (United Nations General Assembly, 1990; United Nations Office on Drugs and Crime, World Health Organization, & Joint United Nations Programme on HIV/AIDS, 2006), MT availability, accessibility, coverage, and quality should be equivalent in both of these settings. However, various studies (Larney & Dolan, 2009; Stöver & Michels, 2010) have shown that a high percentage of opioid-dependent inmates still do not have access to MT. Although a few studies have evaluated how inmates perceive MT (Awgu, Magura, & Rosenblum, 2010; Carlin, 2005; Hughes, 2000; Zamani et al., 2010), inmate satisfaction with this treatment modality has never been studied systematically in prisons where inmates have access to MT. This is surprising because satisfaction is an important indicator of treatment quality (Bell, 2000; Trujols & Pérez de los Cobos, 2005) and is also a predictor of treatment retention (Kelly, O’Grady, Mitchell, Brown, & Schwartz, 2011; Villafranca, McKellar, Trafton, & Humphreys, 2006). To partially address this gap, we carried out the present study, which was designed to (a) assess inmate satisfaction with MT in a multidimensional manner and (b) identify significant independent predictors of inmate satisfaction with this treatment modality.
Method
Setting and Participants
This cross-sectional study was conducted in a Spanish prison for men. The Quatre Camins prison, located in the municipality of La Roca del Vallès near the city of Barcelona (northeast Spain), was built with a radial design that includes four modules, with an original capacity of approximately 900 prisoners. The prison opened in 1989, and subsequent expansion (three new modules, a high-security special closed-regime unit, and an open-regime module) increased capacity to 1,800 prisoners. As this is a prison for sentenced prisoners, the internal population is relatively stable. The prison’s Health Service is composed of 11 general practitioners, 10 nurses, and 16 nursing assistants. The health care staff work continuously in morning, afternoon, and night shifts. A psychiatric unit associated with the Hospital de Sant Joan de Déu is also in place and comprises 3 psychiatrists, a psychologist, 2 nurses, a social worker, and 6 nursing assistants.
Participants were methadone-maintained, heroin-dependent men incarcerated at Quatre Camins prison as of May 2010, receiving MT for at least 3 months prior to enrollment in the study, and who voluntarily agreed to participate in the study.
Procedure
All study-eligible inmates were approached by a member of the staff in charge of their MT and asked about their willingness to participate in a treatment satisfaction survey approved by the Department of Justice of the Government of Catalonia. Eligible participants also received an informative fact sheet about the study and those who agreed to participate in the study signed a written informed consent form. Participants received no remuneration or other incentives for taking part in the study. All assessment instruments were administered individually. A member of the health care team was present to provide help or answer questions while participants answered the survey instruments. This staff member assisted low-literacy participants by reading the items with them. To assure anonymity, inmates were asked not to write their name on the questionnaires. Sociodemographic information and clinical and MT data for each patient were obtained from the medical registry at the institution after the participant completed the survey.
Assessments
Satisfaction With MT
The Verona Service Satisfaction Scale for MT (VSSS-MT; Pérez de los Cobos et al., 2002) was used to measure MT satisfaction. This scale is an adapted version of an instrument originally designed to evaluate the satisfaction of patients who use community mental health services (i.e., the VSSS; Ruggeri et al., 2000). The VSSS-MT (Pérez de los Cobos et al., 2002) is a self-reported, 27-item scale comprising four factors or subscales: Basic Interventions, Specific Interventions, Social Worker Skills, and Psychologist Skills. The Basic Interventions subscale evaluates the patients’ appraisal of the activities and manners of those professionals (i.e., doctors and nurses) who are essential to carrying out MT, as well as perceptions of the help received in interpersonal relationships and self-care (two areas that are specially deteriorated in heroin-dependent patients). The Specific Interventions subscale contains those interventions (mainly psychosocial) that are not considered essential to MT (e.g., individual psychotherapy, group psychotherapy, family therapy). The remaining two subscales (Social Worker Skills and Psychologist Skills) include two items about these professionals’ manner and ability to listen.
All items on the VSSS-MT use a 5-point Likert-type scale response option (1 = terrible, 2 = mostly dissatisfied, 3 = neither dissatisfied nor satisfied, 4 = mostly satisfied, and 5 = excellent), presented with alternate directionality to prevent similar responses. Items that refer to professional manner or activities also had a “not applicable” response option (score = 8), which makes it possible to assess the perceived availability of professional services. In the Specific Interventions subscale, the first question asked if a specific service had been received. If the response was “yes,” satisfaction was described using the above 5-point scale; if the response was “no,” the next question asked the patient to indicate if he or she would have liked to have been offered that particular service (6 = no, 7 = yes, 8 = not applicable, and 9 = I don’t know). In this way, it is possible to assess satisfaction with the nonprovision of services in the Specific Interventions factor. VSSS-MT scores are the average of applicable items. To obtain VSSS-MT means, Specific Intervention responses of 6 (no) and 7 (yes) are scored as 4 (mostly satisfied) and 2 (mostly dissatisfied), respectively, whereas 9 (do not know) is not counted. The VSSS-MT overall and subscale scores should be interpreted according to the following ranges of significance (Pérez de los Cobos et al., 2004): 1-2 (very dissatisfied), >2-3 (slightly dissatisfied), >3-4 (slightly satisfied), and >4-5 (very satisfied). The four VSSS-MT factors showed moderate to excellent internal consistency (Cronbach’s α coefficients of .87, .79, .94, and .94, respectively).
Satisfaction With Methadone As a Medication
Satisfaction with methadone as a medication can be defined as the patient’s evaluation of the process and outcomes of taking methadone (Trujols, Iraurgi, et al., 2012; Trujols, Siñol, & Pérez de los Cobos, 2010). This definition excludes areas such as nonpharmacological interventions, accessibility, or other aspects of biopsychosocial care. Satisfaction with methadone as a medication is thus a much narrower construct than satisfaction with MT (Trujols et al., 2010; Trujols, Iraurgi, et al., 2012). The following question was used to evaluate patients’ opinions about methadone as a medication for treating heroin dependence (Pérez de los Cobos, Trujols, Valderrama, Valero, & Puig, 2005): “Taking into account your overall experience, what is your impression of methadone as a medication for carrying out maintenance treatment for heroin dependence?” The 5-point Likert-type scale (1 = terrible to 5 = excellent) response option used in the VSSS-MT was also used for this question.
Desired Adjustment of Methadone Dose
Patients’ desire to adjust the methadone dose was assessed by a vertical visual analogue scale of methadone dose (VAS-MD; Pérez de los Cobos et al., 2005). The following instructions were given to participants to complete the VAS-MD: “Please indicate with a horizontal mark on the continuous line to what extent you would like to increase (+) or to reduce (−) your current daily methadone dose. If you prefer not to modify your dose, please place a mark at the level of ‘same dose’ (=).” Based on these results, patients were divided into three distinct groups: patients who indicated a desire to raise, lower, or leave unchanged their methadone dose.
Perceived Participation in MT Decisions
Patients’ perception about involvement in their own treatment was assessed through the following two questions (Pérez de los Cobos et al., 2005): “Does the center’s staff keep you informed about changes in your methadone dose?” (1 = never, 2 = very rarely, 3 = sometimes, 4 = almost always, and 5 = always) and “Do you think that your opinion has an influence on staff decisions to modify the methadone dose you take?” (1 = not at all, 2 = a little, 3 = somewhat, 4 = quite a lot, and 5 = a lot).
Data Analysis
Univariate analyses of sociodemographic characteristics, clinical data, and MT-related information included central tendency (mean) and dispersion (standard deviation) measures for continuous variables, and percentages and their corresponding 95% confidence intervals (CIs) for categorical variables. A set of t tests for continuous variables or χ2 tests for categorical variables was conducted to test differences among inmate groups. A multivariate analysis was then performed using a logistic regression to identify those variables that were independently associated with MT satisfaction. This last analysis incorporated only those variables found to be significant at an alpha level of .20 in the bivariate analyses of differences between satisfied and unsatisfied inmates (VSSS-MT total score >3 vs. ≤ 3; Pérez de los Cobos et al., 2004). A p value less than .05 was considered statistically significant for all analyses. Analyses were performed using the SPSS 15.0 statistical package.
Results
Acceptance and Completion of the Survey
Of the 182 potential candidates for inclusion in the study, 12 were excluded because they failed to meet the inclusion criteria: 7 potential participants had been receiving MT for less than 3 months, and 5 were no longer in prison when the survey was conducted. Of the 170 inmates invited to participate, 158 (92.9%) agreed to take part.
Participant Characteristics
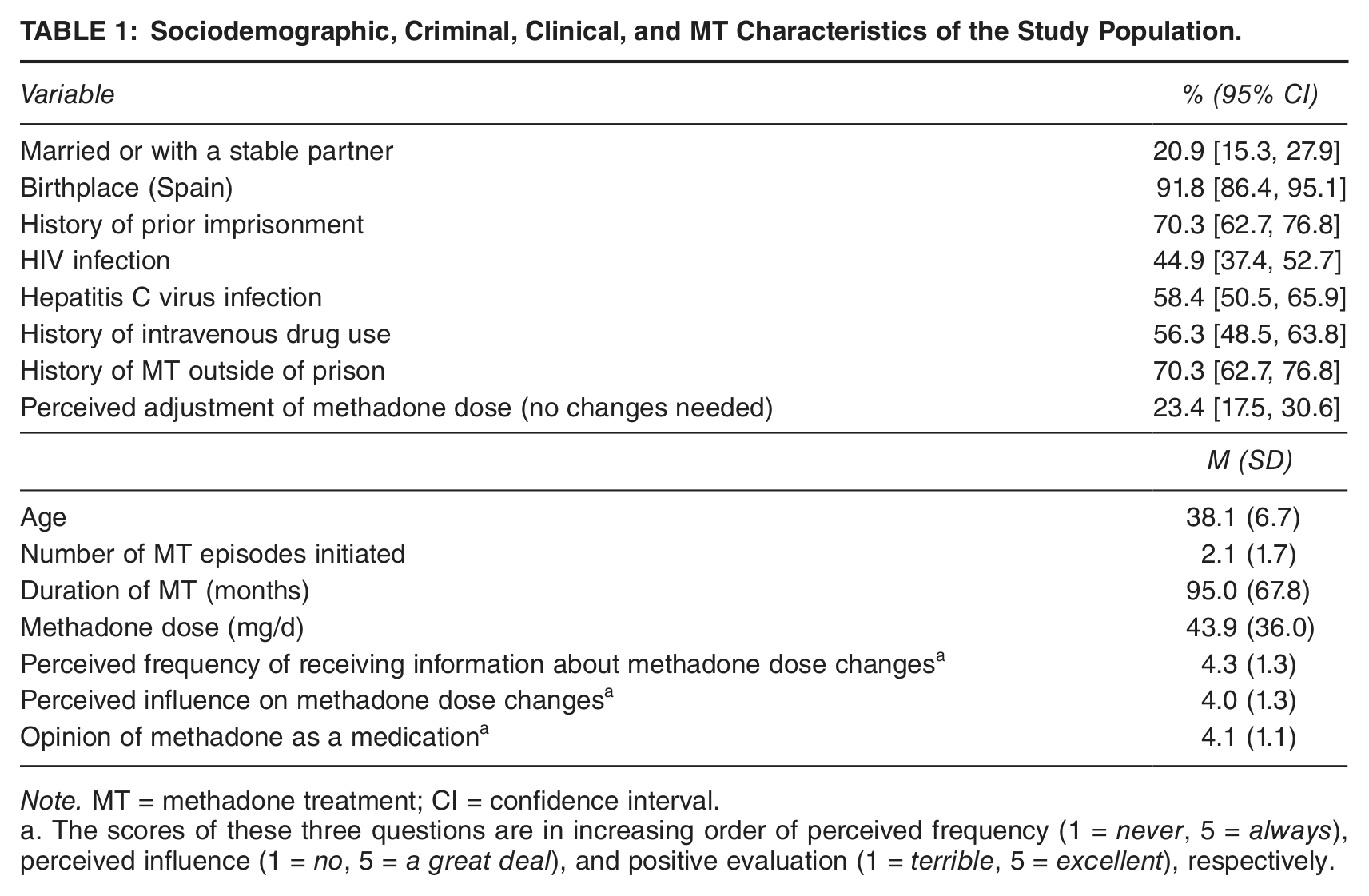
All 158 study participants were male ranging in age from 22 to 56 years (M = 38.1 years, SD = 6.7 years). Most participants (91.8%) were born in Spain, 70.3% had previously been incarcerated, 56.3% had a history of IDU, 44.9% were infected with HIV, and 58.4% were infected with Hepatitis C Virus. Data on other sociodemographic, criminal, clinical characteristics, and MT history are shown in Table 1.
Sociodemographic, Criminal, Clinical, and MT Characteristics of the Study Population.
Note. MT = methadone treatment; CI = confidence interval.
The scores of these three questions are in increasing order of perceived frequency (1 = never, 5 = always), perceived influence (1 = no, 5 = a great deal), and positive evaluation (1 = terrible, 5 = excellent), respectively.
MT: Dose, Dose Adjustment, and Opinion of Methadone as a Medication
The average duration of MT was 95.0 months (SD = 67.8 months). The mean methadone dose was 43.9 mg/d (SD = 36 mg/d). Nearly a quarter of the inmates (23.4%) thought their dose was adequate and preferred not to modify it, whereas 68.4% and 8.2%, respectively, either wanted to reduce or raise the dose.
Slightly more than two thirds (67.7%) of inmates stated that they were well informed about changes in methadone dose by physicians, while 10.1% reported that they were never informed of changes. Most inmates believed that their opinions influenced these changes “a great deal” (44.3%) or “quite a lot” (35.4%), while only 10.1% felt that their opinion had no influence on dose changes.
Most inmates had an excellent (46.2%) or mostly satisfied (36.7%) opinion of methadone as a medication for maintenance treatment. The other patients gave the following opinion of methadone as a medication: “neither dissatisfied nor satisfied” (4.4%), “mostly dissatisfied” (7.6%), or “terrible” (5.1%). Methadone dose was not significantly associated with satisfaction with methadone as a medication (r = −.10, p = .898).
Satisfaction with MT
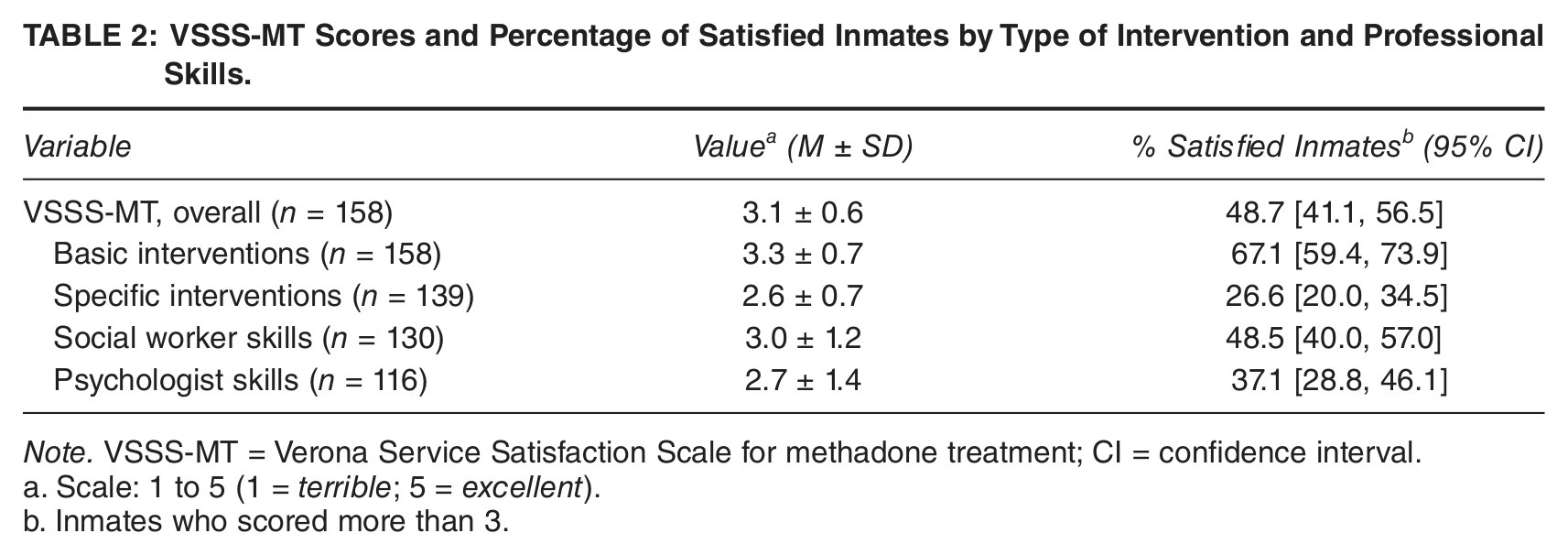
Table 2 shows the dimensional and categorical analyses of VSSS-MT scores. Overall satisfaction was 3.1, a score that is between “neither dissatisfied nor satisfied” and “mostly satisfied.” Only those inmates who scored more than 3 (“neither dissatisfied nor satisfied”) were considered satisfied according to the ranges of clinical significance for the VSSS-MT. Thus, 48.7% of the inmates surveyed were satisfied overall with the services received (see Table 2). The highest percentage of satisfied inmates was found in the Basic Interventions subscale (67.1%), in contrast to the Specific Interventions subscale, in which only 26.6% of inmates were satisfied.
VSSS-MT Scores and Percentage of Satisfied Inmates by Type of Intervention and Professional Skills.
Note. VSSS-MT = Verona Service Satisfaction Scale for methadone treatment; CI = confidence interval.
Scale: 1 to 5 (1 = terrible; 5 = excellent).
Inmates who scored more than 3.
Differences in Satisfaction with MT Between Inmates with or Without History of MT Outside of Prison
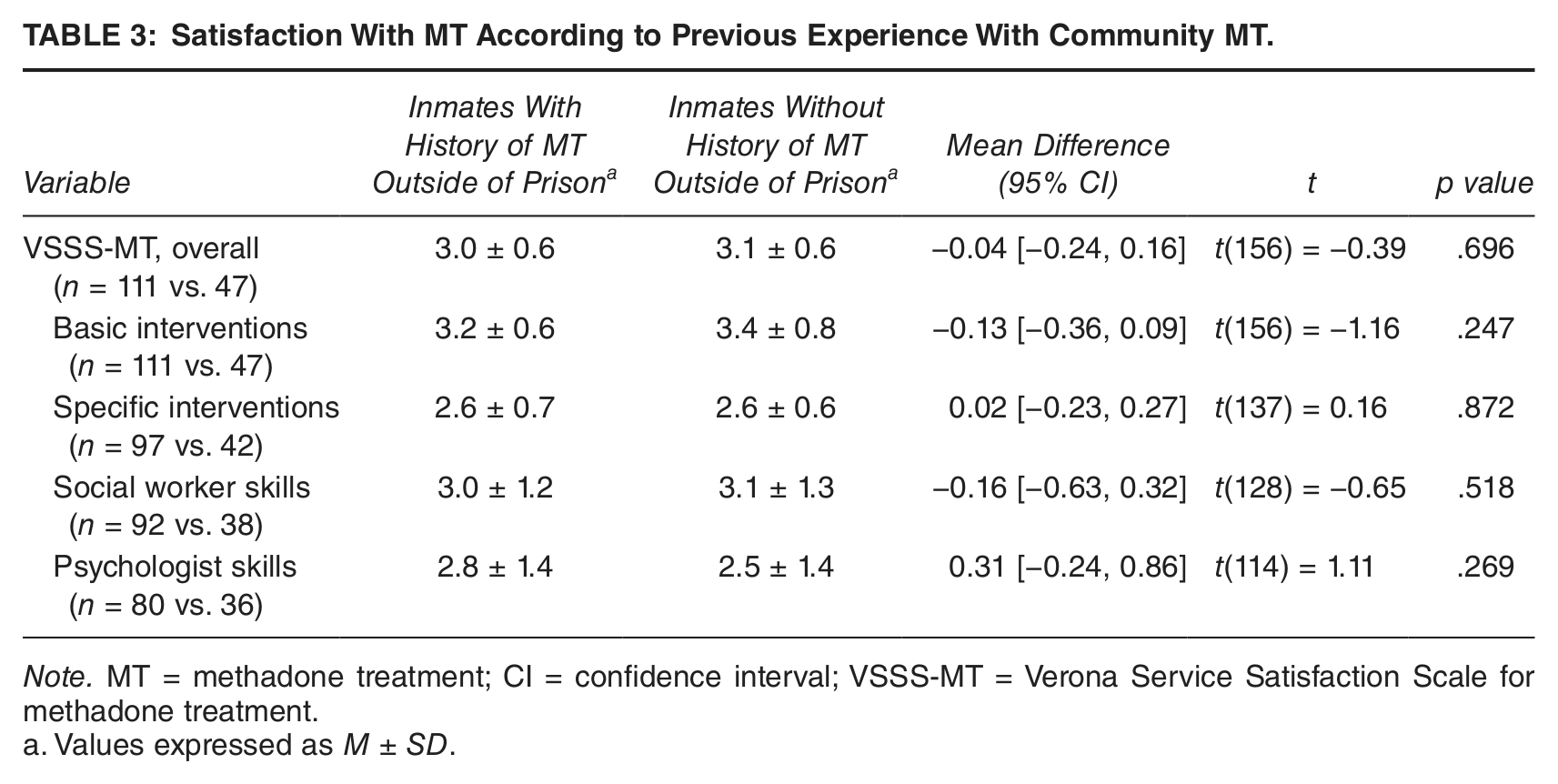
Table 3 shows the VSSS-MT mean scores by factor. Scores are shown by group (participants with a previous history of MT outside of prison vs. those with no prior history). No statistically significant between-group differences were found in overall satisfaction or in the VSSS-MT subscales.
Satisfaction With MT According to Previous Experience With Community MT.
Note. MT = methadone treatment; CI = confidence interval; VSSS-MT = Verona Service Satisfaction Scale for methadone treatment.
Values expressed as M ± SD.
Differences Between Satisfied and Dissatisfied Methadone-Treated Inmates
Table 4 shows the main sociodemographic, criminal, clinical, and MT characteristics according to the level of satisfaction with MT. Compared with inmates dissatisfied with MT, satisfied inmates (a) had a higher prevalence of HIV infection (57.1% vs. 33.3%,p = .003), (b) reported fewer episodes of MT (1.8 vs. 2.4, p = .023), (c) had been on MT for longer (105.9 vs. 84.7 months, p = .049), (d) were more likely to report being informed about changes in methadone dose (4.5 vs. 4.0, p = .008), (e) reported having significantly more influence on dose changes (4.3 vs. 3.7, p = .001), and (f) tended to have a more positive opinion of methadone as a medication (4.3 vs. 4.0, p = .061). Table 4 also shows the results of a multivariate binary logistic regression analysis (Hosmer–Lemeshow test: χ2(7) = 3.062, p = .879, Nagelkerke R2 = .240), which identified the following variables as having a significant association with MT satisfaction: HIV infection, odds ratio (OR) = 3.720, 95% CI = [1.790, 7.730]; number of MT episodes, OR = 0.681, 95% CI = [0.525, 0.882]; and perceived influence on methadone dose changes, OR = 1.691,95% CI = [1.254, 2.280].
Sociodemographic, Criminal, Clinical, and MT Characteristics Associated With Satisfaction With MT.

Note. MT = methadone treatment; CI = confidence interval; VSSS-MT = Verona Service Satisfaction Scale for methadone treatment.
Inmates who scored more than 3 on the VSSS-MT.
Inmates who scored 3 or less on the VSSS-MT.
The scores of these three questions are in increasing order on perceived frequency (1 = never, 5 = always), perceived influence (1 = no, 5 = a great deal), and positive evaluation (1 = terrible, 5 = excellent), respectively.
Discussion
To our knowledge, the present study is the first to perform a multidimensional assessment of satisfaction with MT among methadone-treated penitentiary inmates. The mean overall satisfaction with MT was 3.1, indicating that participants were only slightly satisfied with MT according to the VSSS-MT ranges of clinical significance (Pérez de los Cobos et al., 2004). While it might at first appear surprising that patients would continue with a treatment with which they were only slightly satisfied, this apparent contradiction can be explained by the fact that it is possible for patients to be critical of certain components of care even as they still feel strongly that, overall, the treatment is relatively effective and, more importantly, indispensable to well-being. In this regard, a recent study (Rademakers, Delnoij, & de Boer, 2011) evaluated the extent to which certain aspects of satisfaction determine patients’ overall satisfaction rating. Interestingly, the authors found that the most important predictors of overall satisfaction were aspects related to process, whereas aspects of structure and outcome were less important to patients.
This result, although in the same range, is somewhat lower (3.1 vs. 3.4 and 3.5) than those reported previously in studies that used the same instrument to evaluate MT satisfaction nationally (Pérez de los Cobos et al., 2004) and in specific regions of Spain (Pérez de los Cobos et al., 2005; Trujols, Garijo, et al., 2012). However, we cannot compare the present study with the other studies due to differences in the study population. Only the study by Pérez de los Cobos et al. (2004) included methadone-maintained inmates, with a reported satisfaction level of only 2.9 in this subgroup. However, inmates comprised only 11% of the sample in that study and more than half (50.5%) of inmates refused to participate (i.e., more than twice that of the nonincarcerated sample, and 7 times higher than the rate obtained in the present study). Such a high rate of refusal makes comparison between that study and the present one very difficult.
Although the level of satisfaction with MT found in the present study may seem acceptable, it is important to note that just more than half (51.3%) of the study participants were not satisfied with MT overall. This is because many more inmates were dissatisfied than satisfied with certain aspects of the treatment, thus lowering the score on some of the VSSS-MT subscales. Basic interventions, such as information, help, and methadone information, as well as doctors’ and nurses’ skills, were considered satisfactory by most study participants. In contrast, certain specific interventions, such as individual and group psychotherapy and family therapy, as well as psychologists’ skills, were considered unsatisfactory by two thirds of the participants. Interestingly, we would not have been able to identify these differential findings without the use of a multidimensional instrument such as VSSS-MT, and we believe that such findings are important to consider for future improvement of MT in penitentiaries.
In discussing these results, it should be noted that the low levels of satisfaction with specific interventions and psychologists’ skills are not unique to this prison population. Similar results have been found in previous studies among community samples (Pérez de los Cobos et al., 2004, 2005; Trujols, Garijo, et al., 2012). This could be explained in part by the usual mode of MT implementation—pharmacotherapy alone, with minimal or no counseling or other psychosocial interventions—in our country. In the nonpenitentiary field in Spain (March, Martín-Ruíz, Oviedo-Joekes, Rivadeneira, & Rodríguez-Reinado, 2006), MT is commonly administered with little to no adjuvant interventions, and this approach is even more common among penitentiary centers (Mallada & Marco, 1993; Marco, 1997). This limited implementation of psychosocial interventions in MT seems to underlie our findings of dissatisfaction with specific interventions and psychologists’ skills, especially if we take into account an important feature of VSSS-MT: the ability to assess satisfaction with the nonprovision of the main psychosocial interventions.
An interesting result that at first sight might seem counterintuitive is the finding that despite the low mean methadone dose (44 mg/d), more than two thirds (68%) of participants wanted to reduce their dose. This figure is comparable, though higher than the 36% to 54% found in previous studies (Pérez de los Cobos et al., 2005; Trujols, Garijo, et al., 2012). The desire to reduce the dose may be related to the possibility that patients may see higher methadone doses as an obstacle to discontinuing maintenance treatment, and discontinuation is an important goal for a large percentage of methadone-maintained patients (Lenné et al., 2001; Stancliff, Myers, Steiner, & Drucker, 2002; Winstock, Lintzeris, & Lea, 2011). The desire to come off of MT might be especially strong in a prison setting due to the increased social stigma associated with methadone in this setting.
This commonly observed desire of patients to reduce the methadone dose could lead one to conclude that giving patients some degree of control over treatment decisions could produce results that are counter to clinical practice guidelines. However, this statement is erroneous for several reasons. First, we only assessed a change that patients would have liked to make, not changes that were actually made. Moreover, it is very likely that most patients who expressed a desire to reduce their dose also had concerns about this desire (e.g., withdrawal discomfort). Second, clinical guidelines emphasize and support the notion that clinicians take patient perspectives into account when making clinical decisions (Chong, Chen, Naglie, & Krahn, 2009; Krahn, 2010). In fact, some of the most recent systems for establishing the strength of the recommendations of such guidelines (e.g., the GRADE approach; Guyatt et al., 2008) include patient’s preferences as one of the determinant factors. Third, integration of the patient perspective does not imply that clinicians will automatically fulfill the patient’s wishes. Thus, to give one example, in patients who are active heroin users, the clinician can decide not to reduce the methadone dose, and explain to the patient his or her reasons for not lowering it and the criteria commonly used to regulate the dose.
A noteworthy finding was the absence of a significant difference between satisfied and dissatisfied inmates in terms of mean methadone dose. This result was not entirely unexpected given that two previous studies found no linear relationship between methadone dose and satisfaction with MT (Pérez de los Cobos et al., 2004, 2005). However, it should be noted that the Pérez de los Cobos and colleagues’ (2005) study showed that patients who received daily methadone doses of <60 mg/d felt, overall, more satisfied with MT than patients treated with higher doses (60-100 mg). In any case, when attempting to interpret these results, it is important to consider the differences between satisfaction with MT and satisfaction with methadone as a medication: Satisfaction with MT is a broader construct involving evaluation of more than just satisfaction with methadone as a medication (Trujols et al., 2010; Trujols, Iraurgi, et al., 2012).
Of the many sociodemographic, criminal, clinical, and MT-related variables assessed in the present study, we found three factors that were independently associated with MT satisfaction, as follows: HIV infection, number of MT episodes initiated, and perceived influence on methadone dose changes. The association between satisfaction with MT and HIV infection may at first seem counterintuitive. However, in the case of HIV-infected opioid-dependent persons, MT is associated with (a) acceptance or initiation of antiretroviral treatment (ART; Lum & Tulsky, 2006; Uhlmann et al., 2010), (b) better treatment adherence (Lum & Tulsky, 2006; Malta, Magnanini, Strathdee, & Bastos, 2010; Palepu et al., 2006; Palepu, Milloy, Kerr, Zhang, & Wood, 2011; Uhlmann et al., 2010), (c) better ART outcomes (Malta et al., 2010; Palepu et al., 2006; Roux et al., 2009), and (d) more commitment to health care (Lum & Tulsky, 2006). Presumably, this positive association between MT and ART may lead to a greater level of satisfaction with MT due to the improved health status achieved through both treatments.
The inverse relationship between satisfaction with MT and number of MT episodes initiated (satisfaction with MT is associated with a lower number of episodes) is consistent with an acute care perspective—an analytical framework still shared by many patients and some treatment providers. If patients do not view the recovery process as a progressive and cumulative process requiring multiple treatment episodes over time (Hser & Anglin, 2011; Trujols et al., 2007), then those patients who have undergone multiple treatment episodes over several years may come to believe that recovery is not possible regardless of the particular treatment (Trujols, Tejero, & Casas, 1996). This belief in turn may generate further negativity and passiveness toward future treatment episodes (Trujols et al., 1996) and, very likely, dissatisfaction with new treatment episodes.
The association between satisfaction with MT and inmates’ perceived influence on methadone dose changes (one of the two variables that operationalize patient involvement in treatment decisions) may reflect the desire among opioid-dependent inmates to be considered competent patients and for shared decision making regarding their health care. The association found in our study is consistent with previous findings of a positive relationship between patients’ participation in and satisfaction with treatment (Brener, Resnick, Ellard, Treloar, & Bryant, 2009; Trujols, Garijo, et al., 2012).
The present study has several limitations that merit discussion. First, the instrument used to assess satisfaction with MT was not originally designed for incarcerated patients and thus contains some items that are of little relevance in a prison setting (particularly those items related to work, help at home, and family relations). The VSSS-MT is, however, the only psychometrically sound instrument designed for specific and multidimensional assessment of satisfaction with MT. A second limitation is that the survey was completed by inmates in the presence of a health care professional and we do not know if this affected the results (either positively or negatively), nor the extent of the impact (if any). However, the contrast between a high rate of participation (93%) and only a slight level of satisfaction with MT (3.1 on a 1-5 scale with 51.3% of inmates dissatisfied with MT) suggests that this potential bias is improbable. Third, it should be noted that the results are probably not generalizable to all opioid-dependent patients enrolled in a prison-based MT in Spain because the present study was conducted in only one prison and did not include any patients who had discontinued MT or had been treated for less than 3 months. Fourth, we performed numerous bivariate analyses, thus increasing the probability of a Type I error, although we attempted to minimize this problem by focusing our discussion on the results of the multivariate analysis. Finally, the cross-sectional design used precludes a causal interpretation of the associations found. However, this last limitation is common to most patient satisfaction studies.
Based on the results obtained, two recommendations can be made to improve the quality of prison-based MT at the local level (i.e., in the prison studied) and in other geographical areas sharing a similar model of prison-based MT. First, psychosocial interventions, which are encouraged but not mandatory, should be improved. Their availability, coverage, and quality should be assured to enable a true psychosocially assisted pharmacological treatment of opioid dependence (WHO Department of Mental Health and Substance Abuse, 2009). Second, patient participation in treatment decisions should be maintained, or strengthened in cases in which patients perceive participation to be insufficient, to assure a shared decision-making process. It is important to promote and support patient input into treatment because perceived involvement is one of only three factors identified as having an independent association with MT satisfaction, and, more importantly, it is the only factor that can be modified by changing how we implement MT.
Footnotes
Authors’ note:
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. Points of view are those of the authors and do not necessarily represent the official position or policies of the Catalan Department of Justice.