
Abstract
Research suggests it is important to consider criminogenic needs among individuals with severe mental illness. This study aimed to determine the severity of criminal thinking in community-based clinical samples, understand the association between criminal thinking and psychiatric and criminal justice outcomes, and compare these associations between consumers enrolled in Assertive Community Treatment (ACT) and Forensic Assertive Community Treatment (FACT) programs. Participants (N = 234) were male and female consumers enrolled in ACT and FACT programs in five states. Results revealed no significant differences in criminal thinking when comparing participants by program type or history of criminal justice involvement. There were significant positive relations between general criminal thinking and psychiatric symptomatology and the number of lifetime arrests, a negative association between recovery attitudes and general criminal thinking, and ACT participants reported a greater number of lifetime psychiatric hospitalizations than FACT participants. Result implications are discussed with specific reference to treatment programming.
People who engage in crime evidence thinking styles that support and reinforce antisocial behaviors such as manipulation, impulsivity, and irresponsibility (Walters, 1990; Yochelson & Samenow, 1976). Andrews and Bonta (2010) identified criminal thinking as one of the “Big Four” risk factors that increase one’s likelihood of engaging in criminal behavior. Criminal thinking not only contributes to engagement in criminal behavior, but also influences prolonged and persistent involvement in criminal activity. Specifically, “a criminal belief system supports the evolving criminal lifestyle by shielding it from the light of corrective environmental experience” (Walters, 2006, p. 5). Research has begun to examine the role of criminal thinking in the disproportionate involvement of persons with mental illness (PMI) in the criminal justice (CJ) system; however, the severity of criminal thinking and its association with psychiatric and criminal justice outcomes remains unclear.
Research with CJ populations has found that PMI who are incarcerated evidenced criminal thinking styles that were consistent with nonmentally ill offenders (Morgan, Fisher, Duan, Mandracchia, & Murray, 2010; Wilson et al., 2014; Wolff, Morgan, & Shi, 2013; Wolff, Morgan, Shi, Huening, & Fisher, 2011). In addition, the psychiatric symptomatology of the incarcerated PMI was similar to that of inpatient psychiatric samples (Morgan et al., 2010; Wolff et al., 2011). Furthermore, PMI admitted to a short-term psychiatric facility with a history of, but no current, CJ involvement reported criminal thinking similar to incarcerated PMI (Gross & Morgan, 2013). Finally, Girard and Wormith (2004) found that CJ involved PMI evidenced higher total scores on the General Risk/Need scale of the Level of Service Inventory/Case Management Inventory (LS/CMI; a commonly used measure of criminal risk assessment; Andrews, Bonta, & Wormith, 2004) than CJ involved individuals without mental illness. Taken together, it appears that PMI who are CJ involved “are both mentally ill psychiatric patients and criminals” (Morgan et al., 2010, p. 333) with complex criminogenic and mental health treatment needs.
Interestingly, criminal thinking may be a psychiatric risk factor for PMI who are not CJ involved. For example, civil psychiatric patients scored significantly higher on five out of eight criminal thinking style scales than an incarcerated sample without mental illness (Carr, Rosenfeld, Magyar, & Rotter, 2009). This increased severity of criminal thinking among PMI appears to affect both CJ and psychiatric outcomes (e.g., reincarceration or psychiatric rehospitalization). When compared with offenders without mental illness, PMI who are placed on community supervision (i.e., parole) after being released from a correctional facility are significantly more likely to recidivate (i.e., continue criminal behavior resulting in an arrest and/or reincarceration; Messina, Burdon, Hagopian, & Prendergast, 2004). Similarly, it is estimated that approximately 53% of PMI released from mental health facilities psychiatrically recidivate (i.e., decompensate and are consequently readmitted to a mental health facility) within 12 months of being discharged (Millman, 1993; Segal & Burgess, 2006). The increased risk for criminal recidivism and the high rate of psychiatric recidivism may be attributable to shared risk factors that affect both criminal and psychiatric recovery. For example, PMI receiving community mental health services attributed factors such as unemployment, lack of education, lack of housing, and economic difficulties as contributing to their likelihood of psychiatric recidivism (Mgustshini, 2010), and these factors also correspond to risk factors used to predict criminal behavior (Andrews & Bonta, 2010; Draine, Salzer, Culhane, & Hadley, 2002). In addition, incarcerated PMI were found to have psychiatric hospitalization rates that were three times higher than PMI who were not CJ involved (Fisher et al., 2002), suggesting a unique feature that may increase the potential for psychiatric hospitalization.
Given the poor CJ and psychiatric outcomes related to traditional mental health treatment, treatment programs that address both criminogenic (e.g., substance abuse, emotion management, criminal attitudes, criminal associates) and psychiatric (e.g., mental illness awareness, medication compliance, social skills, problem-solving) needs of offenders may be most efficacious in terms of reducing criminal behavior and improving mental health recovery (Moran & Hodgins, 2004; Morgan et al., 2010). The need for integrated treatment is further highlighted by findings that PMI have higher indicators of criminal risk factors compared with individuals without mental illness (Girard & Wormith, 2004). However, treatment programs available to offenders in corrections appear to focus primarily on mental health treatment and minimally incorporate, if at all, approaches for treating criminal behavior (Bewley & Morgan, 2011; Diamond, Wang, Holzer, Thomas, & Cruser, 2001). It is unclear what percentage of community mental health programs integrates criminogenic needs into their treatment programs. For example, Assertive Community Treatment (ACT) programs emphasize a community-based multidisciplinary team approach and have been found to improve mental health outcomes (Bond, Drake, Mueser, & Latimer, 2001); however, there is no indication that they address criminogenic risk factors commonly found in this population. Forensic Assertive Community Treatment (FACT) programs concurrently address mental health and criminogenic needs with the goal of improving both mental health functioning and CJ outcomes (Cuddeback, Morrissey, & Cusack, 2008; Skeem, Manchak, & Peterson, 2011), but FACT programs are not as widely available. Compared with ACT programs, FACT programs address both psychiatric and criminogenic needs, which are consistent with the current best practices in the literature (e.g., Moran & Hodgins, 2004; Morgan et al., 2010) for PMI with CJ involvement and should be associated with better outcomes for these individuals. Furthermore, individuals in FACT programs likely evidence greater criminal thinking because this program is designed for individuals with CJ involvement and criminogenic needs, whereas ACT programs do not address these same issues.
In sum, the literature suggests identifying factors that are related to criminal risk and psychiatric hospitalization rates could be influential in the development and implementation of specified and targeted interventions appropriate to the unique needs of PMI who are and are not CJ involved. PMI who are CJ involved may have unique psychological needs and risk factors regarding offending behavior. In addition, similarities in criminal thinking may be associated with decreased psychological functioning of PMI who are not CJ involved. The current study examined criminal thinking, CJ involvement, and mental health recovery attitudes among individuals in ACT and FACT programs affiliated with community-based mental health centers located across the United States. We hypothesized the following:
The participants enrolled in FACT programs, and participants with a history of CJ involvement would report greater criminal thinking than those enrolled in ACT programs.
Psychiatric symptoms would be positively associated with criminal thinking, and program type would moderate this association (individuals in FACT programs would evidence a stronger association than those in the ACT programs).
Positive attitudes toward psychiatric recovery would be negatively associated with criminal thinking, and program type would moderate this association (individuals in FACT programs would evidence a stronger association than those in the ACT programs).
Criminal thinking would be positively associated with self-reported number of lifetime arrests, and program type would moderate this association (individuals in FACT programs would evidence a stronger association than those in the ACT programs).
Criminal thinking would be positively associated with self-reported number of lifetime psychiatric hospitalizations, and program type would moderate this association (individuals in FACT programs would evidence a stronger association than those in the ACT programs).
Method
Participants
Sites
ACT and FACT programs were identified using a database of community-based mental health treatment programs that participated in a web-based survey of mental health programs conducted by the Center for Behavioral Health Services & Criminal Justice Research (CBHSCJR) at Rutgers University (n = 59) and via referral from contacted treatment programs (n = 5). Researchers were unable to initiate contact with 22 programs (34.4%). Of the programs that were contacted, but did not participate, 12 (28.6%) refused to participate, 10 (23.8%) did not have an ACT, ACT-like, FACT, or FACT-like program, and 15 (35.7%) initially expressed interest, but were nonresponsive to follow-up contact attempts made by researchers. A total of five sites (11.9%) located in five different states (Colorado, Florida, Idaho, Texas, and Washington) agreed to participate, which included three FACT and three ACT programs (two sites had both ACT and FACT programs). Researchers attempted to gather programmatic data (e.g., number of consumers enrolled, funding source) to allow for differences between programs to be assessed and controlled for as needed; however, due to low response rates to surveys sent to program coordinators, such analyses could not be conducted.
Consumers
Data were collected from 234 PMI receiving community mental health services from an ACT (n = 159, 67.9%) or FACT (n = 75, 32.1%) program. Ten (4.3%) consumers recruited to participate refused participation, elected not to provide demographic information to compare differences between consumers who did, and did not agree to participate in the survey. Notably, this refusal rate likely underrepresents the actual refusal rate as consumers may have elected not to present to the agency after being informed of the study (see Procedure). Of the 234 consumers who participated in the study, data were lost for four of the participants due to computer error during data collection. All descriptive data and analyses are based on the remaining 230 participants. See Table 1 for participants’ demographic data.
Descriptive Statistics and Frequencies for Demographics Data
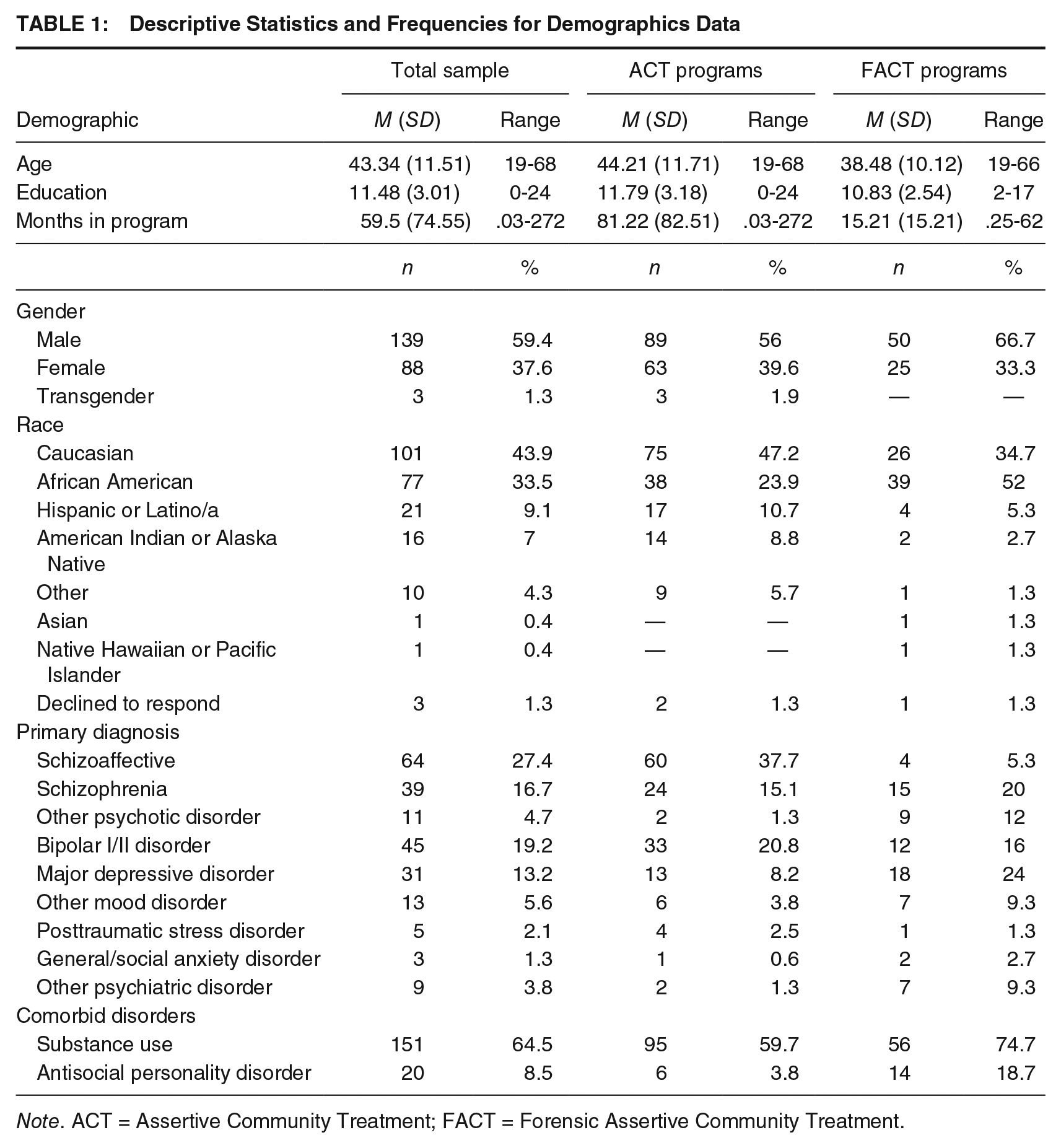
Note. ACT = Assertive Community Treatment; FACT = Forensic Assertive Community Treatment.
Most participants had a history of CJ involvement as 88.9% (n = 208) had been arrested at least once in their lifetime, 76.5% (n = 179) had been incarcerated at a jail, and 29.5% (n = 69) had served a prison sentence. Many participants (n = 86, 37.4%) were under community supervision (i.e., probation or parole) at the time of participation. In addition, in the past year 34.6% (n = 81) of participants indicated they had spent time with criminal associates, 39.7% (n = 93) used illegal drugs, 72.2% (n = 169) experienced financial difficulty, 32.1% (n = 75) experienced homelessness, and 50.9% (n = 119) had difficulty getting along with family members. Histories significant for inpatient psychiatric hospitalization were also common as 80% (n = 184) had been hospitalized at least once in their lifetime.
Measures
Demographic Form
A self-report demographic form was used to gather a broad array of information including, but not limited to, age, ethnicity, relationship status, education, number of hospitalizations, and psychiatric history (e.g., treatment, psychiatric diagnoses).
Behavioral and Criminal History Form
The researchers developed a behavioral and criminal history form composed of 23 items regarding CJ involvement (e.g., arrests, legal charges, incarcerations), behaviors that have been shown to increase the risk for CJ involvement (e.g., criminal associates, drug use, family problems), and other problematic behaviors or experiences (e.g., fighting, feelings of rage, gambling).
The Brief Symptom Inventory (BSI)
The BSI (Derogatis & Melisaratos, 1983) is a 53-item, self-report assessment of distress due to current (the previous 7 days including the assessment day) psychiatric symptoms. Response options to items on the BSI are provided using a 5-point Likert-type scale (0 = not at all, 1 = a little bit, 2 = moderately, 3 = quite a bit, 4 = extremely; Derogatis, 1993). The BSI yields nine primary symptom scales, and three global indices of distress (i.e., Global Severity Index, Positive Symptom Distress Index, Positive Symptom Total). Given the mixed evidence for the nine symptom scales (Hayes, 1997), only the Global Severity Index and Positive Symptom Total were utilized (separately) in the analyses. Literature has indicated that the BSI has internal consistency reliability greater than .70 for the subscales (Derogatis, 1993), and good convergent validity for the BSI scale scores with the Symptom Checklist-90-Revise (SCL-90-R) and Minnesota Multiphasic Personality Inventory (MMPI; Derogatis, 1993). The BSI has been normed utilizing several different samples including adult psychiatric outpatients and is written at a sixth-grade reading level (Derogatis, 1993). The internal consistency of the items on the BSI in this study was high (α = .98).
The Psychological Inventory of Criminal Thinking Styles–Layperson Edition–Short Form (PICTS-L-SF)
The PICTS-L-SF is a 35-item, self-report measure. Like all versions of the PICTS (Walters, 1995), the PICTS-L-SF is designed to assess thought patterns that are associated with criminal behavior (Walters, 2006). A layperson version of the PICTS, the PICTS-L, was developed by James Kaufman to measure criminal thinking in nonoffender populations (G. D. Walters, personal communication, March 2011) by altering the wording of the questions so that a history of criminal behavior was not assumed. For example, the question on the PICTS reading, “I have used alcohol or drugs to eliminate fear or apprehension before committing a crime” was changed on the PICTS-L to read, “I have used alcohol or drugs to eliminate fear or apprehension before doing something risky.” In addition, a Short Form version of the PICTS (Walters, 2006), the PICTS-SF, was developed to reduce the number of items from 80 to 35. The PICTS-L-SF was developed by the researchers for this study. This was done by selecting the test items on the 80-item PICTS-L that corresponded to the 35 items on the PICTS-SF (PICTS-SF; G. D. Walters, personal communication, February 2012). Response options to items on the PICTS-L-SF are provided using a 4-point Likert-type scale (1 = disagree, 2 = uncertain, 3 = agree, 4 = strongly agree; Walters, 2006).
The PICTS-L-SF produces multiple scales; however, Walters identifies General Criminal Thinking and the composite scales (i.e., Proactive Criminal Thinking and Reactive Criminal Thinking) as the “most important scores on the inventory” (G. D. Walters, Personal Communication, March 2013). There are no cutoff scores distinguishing the presence or absence of each of the criminal thinking scales, but guidelines are provided for interpreting the criminal thinking styles T-scores as Low (<40), Average (≥40, <60), High/Clinically Significant (≥60, <70), and Very High (≥70; Walters, 2006). Therefore, T-scores were utilized (as opposed to raw scores) in the analyses to enhance the clinical interpretability of the results. Three validity scales (i.e., the number of omitted items, Confusion–revised [Cf-r], Defensiveness–revised [Df-r]) are also produced that assist in the determination of the validity of the profile. Profiles were determined to be invalid if the profile yielded T-scores greater than 80 on either of the validity scales or if a response was not provided for two or more items. A recent study (Mitchell, Bartholomew, Morgan, & Cukrowicz, 2017) evaluated the psychometric properties of the PICTS-L-SF among college students without a history of CJ involvement. Results of bi-factor categorical confirmatory factor analyses supported the structure of the PICTS with a General Criminal Thinking and two domain-specific factors (i.e., Proactive Criminal Thinking and Reactive Criminal Thinking). In addition, the items evidenced strong internal consistency in this study for the Proactive Criminal Thinking (α = .87), Reactive Criminal Thinking (α = .91), and General Criminal Thinking (α = .93) scales.
The Recovery Assessment Scale (RAS)
The RAS (Giffort, Schmook, Woody, Vollendorf, & Gervain, 1995) is a self-report, 41-item assessment of self-perceived psychiatric recovery. Respondents are asked to indicate the degree to which the items (e.g., “I have a desire to succeed,” “If I keep trying I will continue to get better,” “My symptoms interfere less and less with my life”) describe how they feel. Response options to items are provided using a 5-point Likert-type scale (ranging from 1 = strongly disagree to 5 = strongly agree). The RAS yields five domain scores: personal confidence and hope, willingness to ask for help, goal and success orientation, reliance on others, and no domination by symptoms. The RAS has previously demonstrated good internal consistency (α = 0.93; Corrigan, Giffort, Rashid, Leary, & Okeke, 1999). Although the RAS scale scores have also been shown to have good concurrent validity with a number of measures including the Mental Health Recovery Measure (MHRM), and the Self-Identified Stages of Recovery (SISR; Burgess, Pirkis, Coombs, & Rosen, 2010), research indicates mixed findings regarding the association between RAS scores and objective assessments of recovery (e.g., Andresen, Caputi, & Oades, 2010; Salzer & Brusilovskiy, 2014). That being said, the RAS appears to perform similarly to other self-report assessments of recovery (Andresen et al., 2010). The internal consistency of the items on the RAS in this study was high (α = .95).
Procedure
Participant Recruitment
All procedures were approved by the individual sites’ and the researchers’ university Institutional Review Boards. For all ACT and FACT programs (N = 59) identified in the CBHSCJR database and the five referrals received from the contacted programs, contact was attempted via electronic mail and telephone. A program was determined to be “unreachable” after two emails were sent with no response and four phone calls (a message was left on the first and fourth phone call). Contacted sites were provided with information regarding participation and were informed that appropriate approval from the researchers’ university Institutional Review Board was obtained.
Data Collection
Participating sites were visited for either 2, 3, or 5 days depending on the number of consumers served and treatment program schedules. Researchers provided the program site with a recruitment letter that was printed on the site’s letter head and provided to ACT and FACT consumers who were potential participants.
Upon arrival at the site, potential participants individually met with the researchers and were verbally informed about the nature (e.g., the survey would take approximately 60 min, they would receive US$10) and purpose of the study. Individuals willing to participate were provided a written informed consent form. For those consumers who were unable to read (n = 8) an oral summary of the consent was provided, and the survey was administered orally by a researcher. Participants who could complete the measures independently were presented the measures as a computer-based survey in a room where other consumers could also be completing the measures via individual computers. The Demographic Form was presented first, followed by the Behavioral and Criminal History Form, BSI, PICTS-L-SF, and RAS that were alternately presented across the five computers to limit sequencing effects.
Data Preparation
Prior to completing the analyses, data were screened for incomplete/missing data, the validity indices of the PICTS-L-SF were reviewed, and assumptions of multivariate, univariate, and regression analyses were assessed. The PICTS-L-SF was the only instrument utilized that provided response pattern scales that assess for validity. As indicated in the “Measures” section above, all PICTS-L-SF clinical profiles that yielded a T-score of greater than 80 on either the Confusion or Defensiveness (n = 63) scale, PICTS-L-SF profiles with greater than two missing items (n = 6), and BSI profiles with greater than 13 missing items (n = 1) were removed from further analyses involving these measures (i.e., pairwise deletion) because these profiles are considered invalid.
Data were reviewed for outliers, and those identified were changed to one unit greater or smaller than the most extreme score on the variable that fell within a z score of ± 3.29 (Tabachnick & Fidell, 2007). Normality was assessed by dividing the skewness statistic by the skewness standard error for each variable. If this value was greater than ± 3.29, that variable was considered significantly skewed (Tabachnick & Fidell, 2007). The same procedure was used to determine significant kurtosis using the kurtosis statistic and standard error (Tabachnick & Fidell, 2007). The following variables were significantly skewed: one PICTS-L-SF subscale (Proactive Criminal Thinking), three RAS subscales (Goal and Success Orientation, Reliance on Others, Willingness to Ask for Help), and the RAS Total score. The logarithm transformation yielded the best improvement in the normality of Proactive Criminal Thinking; however, the pattern of results and significance did not differ when using the transformed variable compared with the nontransformed variable. Hence, for ease of interpretation, the nontransformed Proactive Criminal Thinking variable was used in analyses. Transforming the RAS scales did not improve normality; therefore, the nontransformed RAS scales were included in analyses despite their deviations from normality. Results were conservatively interpreted for the RAS considering this violation. There were no violations of linearity and colinearity assumptions.
Results
Statistical Analyses
Data Cleaning and Preparation
Descriptive data were calculated for the overall sample, for those participants in ACT or FACT programs, and for those with and without a history of arrests. Average scores for the PICTS-L-SF Proactive Criminal Thinking, Reactive Criminal Thinking, and General Criminal Thinking scales were below 60 (i.e., threshold to be considered high) for all groups. The descriptive data for the overall, ACT and FACT, and CJ and non-CJ (arrest history) samples are presented in Table 2.
Descriptive Statistics
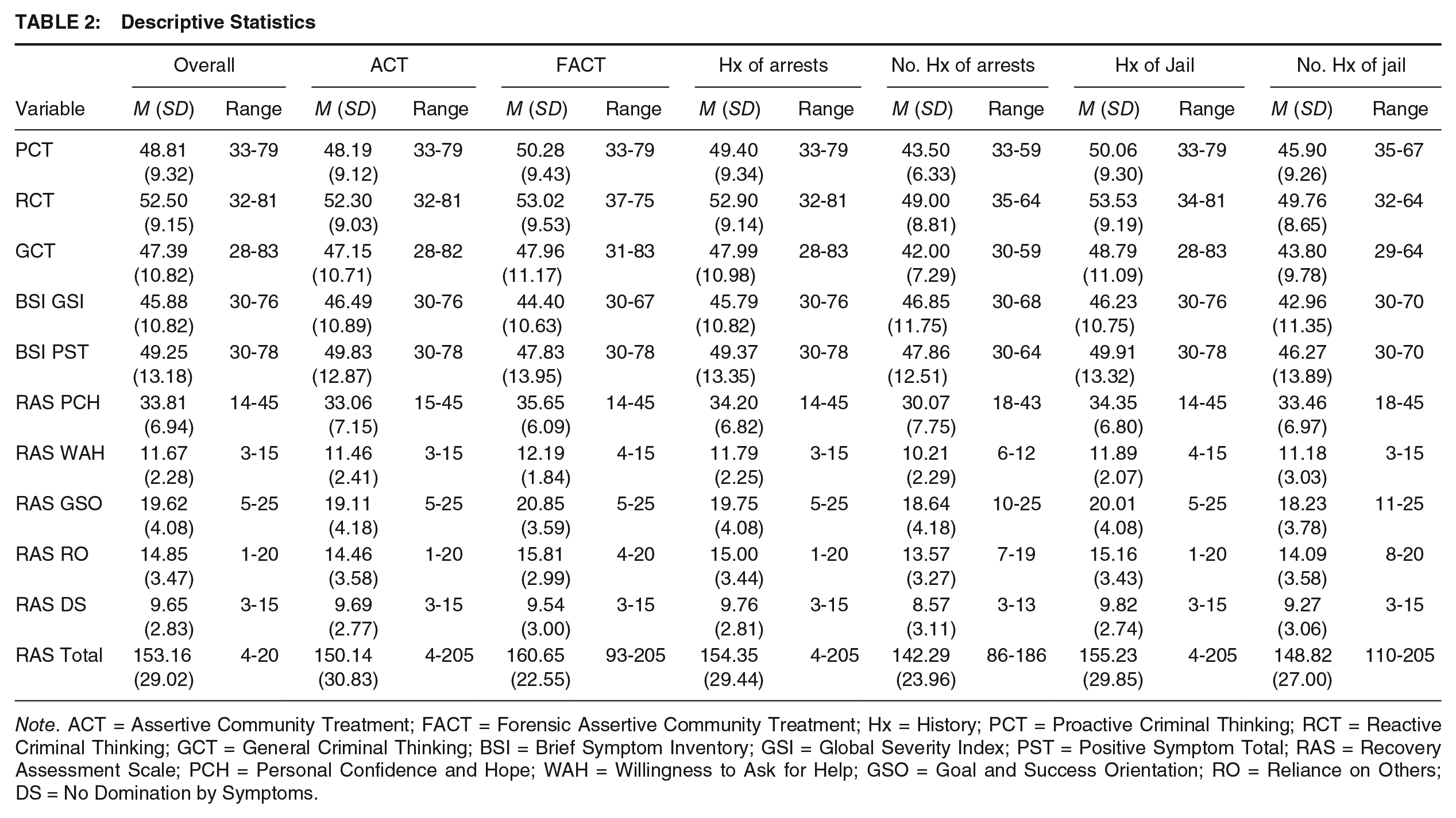
Note. ACT = Assertive Community Treatment; FACT = Forensic Assertive Community Treatment; Hx = History; PCT = Proactive Criminal Thinking; RCT = Reactive Criminal Thinking; GCT = General Criminal Thinking; BSI = Brief Symptom Inventory; GSI = Global Severity Index; PST = Positive Symptom Total; RAS = Recovery Assessment Scale; PCH = Personal Confidence and Hope; WAH = Willingness to Ask for Help; GSO = Goal and Success Orientation; RO = Reliance on Others; DS = No Domination by Symptoms.
Examining Demographic Differences Between Groups
Prior to conducting the between group analyses for criminal thinking, Analysis of Variance (ANOVA) and Chi-square procedures were conducted to determine if there were demographic differences between the ACT and FACT samples, and the CJ versus non-CJ involved participants (i.e., arrests vs. no arrests, and jail incarcerations vs. no jail incarcerations) that would need to be included as covariates in the between group analyses. Age, substance abuse comorbidity, gender, race, years of formal education, symptom severity (i.e., BSI Global Severity Index score), and the length of time they had been enrolled in their current community mental health treatment program were all assessed. Between ACT and FACT participants, there were significant between-group differences found for age, F(1, 166) = 8.03, p = .005; time in treatment, F(1, 152) = 31.85, p < .001; and race, χ2(7, N = 167) = 21.11, p = .004. For those with and without a history of arrests, there were significant between-group differences found for time in treatment, F(1, 151) = 4.50, p = .013, and substance abuse comorbidity, χ2(1, N = 155) = 6.58, p = .037. For those with and without a history of jail incarcerations, there were significant between-group differences found for time in treatment, F(1, 151) = 4.72, p = .004. Thus, these variables were entered as covariates in the appropriate analyses below.
Hypotheses 1 and 2
Although the average scores across the criminal thinking scales on the PICTS-L-SF did not exceed the threshold to be determined as “high,” a majority of the participants who produced a valid PICTS-L-SF profile elevated at least one criminal thinking scale (n = 116, 69.5%). A one-way MANCOVA was conducted for the PICTS-L-SF scales (i.e., Proactive Criminal Thinking and Reactive Criminal Thinking), with the necessary covariates (based on the independent variable used in each analysis) to examine group differences in criminal thinking between the participants enrolled in ACT and FACT programs, those with and without a history of arrests, and those with and without a history of jail incarcerations. In addition, an ANCOVA was conducted to examine between-group differences for participants enrolled in ACT and FACT programs, those with and without a history of arrests, and those with and without a history of jail incarcerations on the PICTS-L-SF General Criminal Thinking scale with the appropriate covariates (based on the independent variable used in each analysis).
The MANCOVA analyses indicated no significant multivariate between-group differences on the PICTS-L-SF Proactive Criminal Thinking and Reactive Criminal Thinking scales for those in ACT (n = 99) and FACT (n = 46) programs, Wilk’s Λ = 0.99, F(2, 136) = 0.48, p = .621, ηp2 = .01; those with (n = 127) and without (n = 13) a history of arrests, Wilk’s Λ = 0.98, F(2, 135) = 1.20, p = .304, ηp2 = .02; and those with (n = 111) and without (n = 18) a history of jail incarcerations, Wilk’s Λ = 0.98, F(2, 125) = 1.37, p = .258, ηp2 = .02. In addition, ANCOVA analyses indicated no significant between-group differences on the General Criminal Thinking scale between those in ACT and FACT programs, F(1, 137) = 0.05, p = .830, ηp2 = .00; those with and without a history of arrest, F(1, 136) = 2.37, p = .126, ηp2 = .02; and those with and without a history of jail incarcerations, F(1, 128) = 2.63, p = .108, ηp2 = .02. Taken together, contrary to the hypotheses, criminal thinking did not differ as function of program type or history of CJ involvement.
Hypothesis 3
Linear regression analyses were conducted to evaluate psychiatric symptoms (BSI scores) as predictors of General Criminal Thinking. In addition, the moderating effect of program type (coded ACT = 1 vs. FACT = 0) was examined (Table 3). In each of the following analyses, the PICTS-L-SF General Criminal Thinking scale served as the criterion variable, and all predictors were mean centered prior to analysis. Time in treatment was considered as a potential covariate; however, this was determined to be unnecessary because of its nonsignificant association with General Criminal Thinking (r = −.06, p = .496).
Linear Regression Analyses
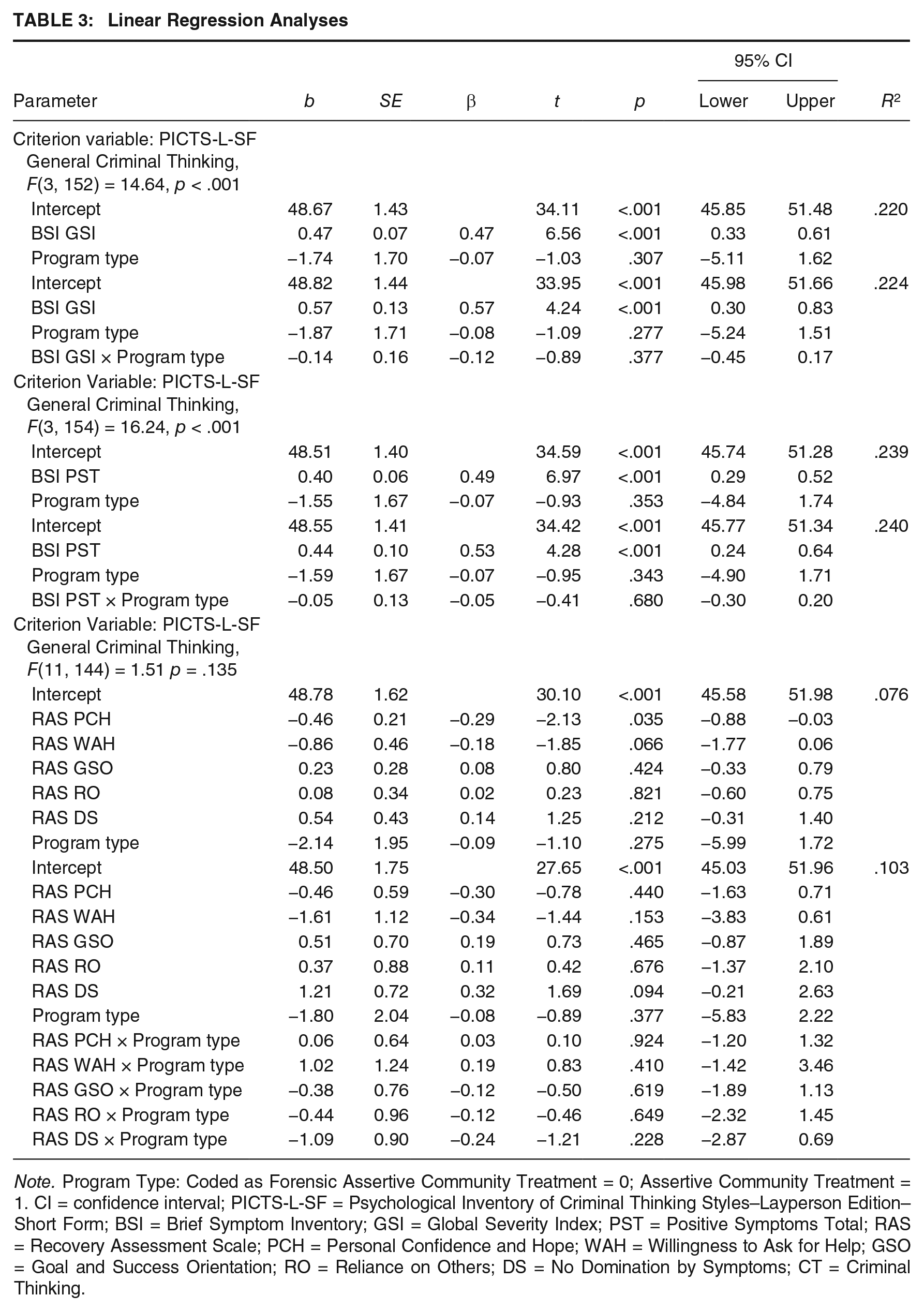
Note. Program Type: Coded as Forensic Assertive Community Treatment = 0; Assertive Community Treatment = 1. CI = confidence interval; PICTS-L-SF = Psychological Inventory of Criminal Thinking Styles–Layperson Edition–Short Form; BSI = Brief Symptom Inventory; GSI = Global Severity Index; PST = Positive Symptoms Total; RAS = Recovery Assessment Scale; PCH = Personal Confidence and Hope; WAH = Willingness to Ask for Help; GSO = Goal and Success Orientation; RO = Reliance on Others; DS = No Domination by Symptoms; CT = Criminal Thinking.
For the first regression analysis, the BSI Global Severity Index and program type were entered as main effects predicting General Criminal Thinking. Subsequently, the interaction between program type and BSI Global Severity Index was added to the model. Due to missing data on the BSI and the PICTS-L-SF profiles that were removed for validity issues, 156 participants were included in this analysis. There were significant main effects of BSI Global Severity Index (b = 0.47, p < .001) but not program type (b = −1.87, p = .307). The main effects accounted for 22% of the variance in General Criminal Thinking. The interaction between program type and BSI Global Severity Index was not significant (b = −0.14, p = .377) and only accounted for an additional 0.4% of the variance in General Criminal Thinking.
To evaluate the relationship between the number of symptoms experienced (without evaluating symptoms severity) and General Criminal Thinking, the BSI Positive Symptoms Total scale and program type were entered as the predictor variables in a linear regression analysis (n = 158). Subsequently, the interaction between program type and BSI Positive Symptoms Total was added to the model. There were significant main effects of BSI Positive Symptoms Total (b = 0.40, p < .001) but not program type (b = −1.55, p = .353). The main effects accounted for 23% of the variance in General Criminal Thinking. The interaction between program type and BSI Positive Symptoms Total was not significant (b = −0.05, p = .680) and only accounted for an additional 0.1% of the variance in General Criminal Thinking. In sum, Hypothesis 3 was partially supported, such that psychiatric symptoms were significantly associated with criminal thinking; however, these associations did not differ by program type.
Hypothesis 4
Linear regression analyses were conducted to evaluate recovery attitudes (RAS scores) as predictors of General Criminal Thinking (n = 156). In addition, the moderating effect of program type (coded ACT = 1 vs. FACT = 0) was examined (Table 3). All predictors were mean centered prior to analysis. First, the five RAS subscales and the program type were simultaneously included as main effects predicting General Criminal Thinking; subsequently, the interactions between program type and the RAS subscales were added to the model. There was a significant main effect of the Personal Confidence and Hope RAS scale (b = −0.46, p = .035); however, all main effects accounted for only 7.6% of the variance in General Criminal Thinking. The interactions between program type and the RAS subscales were not significant and only accounted for an additional 2.7% of the variance in General Criminal Thinking.
Hypotheses 5 and 6
Negative binomial regressions were conducted to examine the associations between General Criminal Thinking and the number of lifetime arrests and psychiatric hospitalizations. In addition, the moderating effects of program type (coded ACT = 1 vs. FACT = 0) were examined. 1 All predictors were mean centered prior to analysis. To determine the most appropriate fitting regression model for the count data (i.e., number of lifetime arrests, number of lifetime psychiatric hospitalizations), the dispersion of the data was examined. The mean number of lifetime arrests was 11.48 with a variance of 169.34 (SD = 13.01), and the mean number of lifetime psychiatric hospitalizations was 7.94 with a variance of 87.24 (SD = 9.34). For both variables, the variance exceeded the mean, and the dispersion coefficient exceeded zero, suggesting overdispersion. Furthermore, a comparison of the log likelihood fit statistics for the Poisson and negative binomial models indicated that the negative binomial models yielded significantly better fit (p < .001).
The first negative binomial regression examined the main effects of program type (coded ACT = 1 vs. FACT = 0) and General Criminal Thinking on the number of lifetime arrests; subsequently, the interaction between program type and General Criminal Thinking was added to the model (Table 4). The negative binomial regression model that included the main effects was statistically significant, Likelihood Ratio χ2(2, N = 132) = 22.38, p < .001. Program type was a significant predictor of the number of lifetime arrests, such that individuals in the ACT program evidenced .66 fewer lifetime arrests than those in the FACT program when holding General Criminal Thinking constant. General Criminal Thinking was also a significant predictor of the number of lifetime arrests, such that among individuals in the FACT program, a one-point increase in General Criminal Thinking was associated with a 1.03 increase in the number of lifetime arrests. The model that included the interaction between program type and General Criminal Thinking was also significant, Likelihood Ratio χ2(3, N = 132) = 26.33, p < .001; however, the interaction term was not.
Negative Binomial Regression Results With Number of Lifetime Arrests as the Outcome Variable

Note. Program Type: Coded as Forensic Assertive Community Treatment = 0; Assertive Community Treatment = 1. CI = confidence interval; GCT = General Criminal Thinking.
The second negative binomial regression examined the main effects of program type (coded ACT = 1 vs. FACT = 0) and General Criminal Thinking on the number of lifetime psychiatric hospitalizations; subsequently, the interaction between program type and General Criminal Thinking was added to the model (Table 5). The negative binomial regression model that included the main effects was statistically significant, Likelihood Ratio χ2(2, N = 120) = 14.04, p = .001. Program type was a significant predictor of the number of lifetime psychiatric hospitalizations, such that individuals in the ACT programs had 1.97 more lifetime psychiatric hospitalizations than those in the FACT programs when holding General Criminal Thinking constant. General Criminal Thinking was not a significant predictor when holding program type constant. The model that included the interaction between program type and General Criminal Thinking was also significant, Likelihood Ratio χ2(3, N = 120) = 14.07, p = .003; however, the interaction term was not.
Negative Binomial Regression Results With Number of Lifetime Psychiatric Hospitalizations as the Outcome Variable
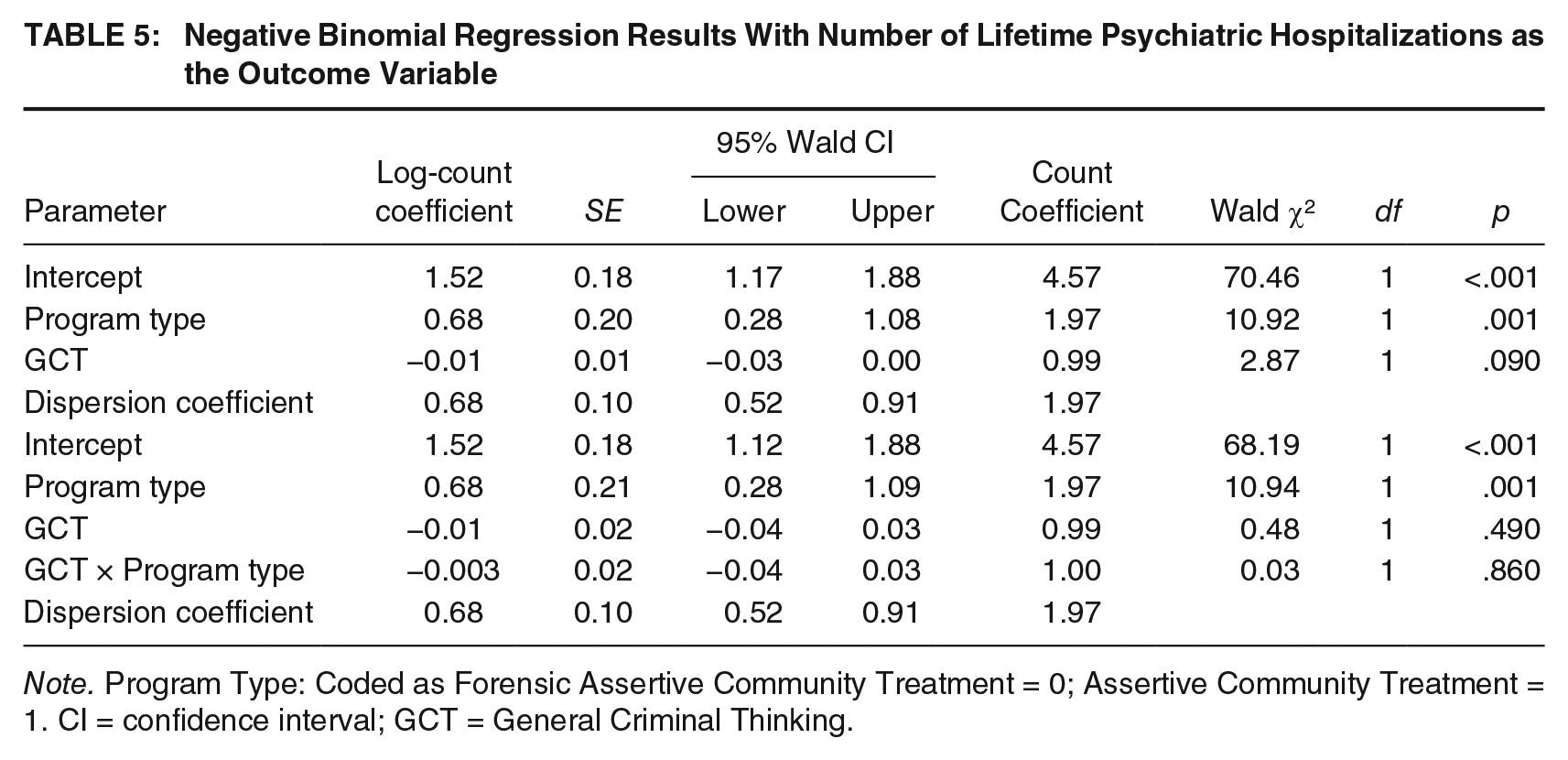
Note. Program Type: Coded as Forensic Assertive Community Treatment = 0; Assertive Community Treatment = 1. CI = confidence interval; GCT = General Criminal Thinking.
Discussion
The aim of this study was to establish the presence and severity of criminal thinking, assess for differences between consumers based on mental health program type (ACT vs. FACT) and CJ involvement, and to examine the relations between criminal thinking and CJ involvement, mental health, and recovery attitudes in a community mental health sample. Although the average scores across the criminal thinking scales on the PICTS-L-SF did not exceed the threshold to be determined as “high,” a majority of the participants who produced a valid PICTS-L-SF profile elevated at least one criminal thinking scale (n = 116, 69.5%).
Contrary to our hypotheses, General Criminal Thinking, Reactive Criminal Thinking, or Proactive Criminal Thinking did not significantly differ by program type, nor CJ history. Regarding psychiatric symptomology, results indicated significant positive associations between psychiatric symptoms (both severity of distress and number of symptoms) and General Criminal Thinking, as hypothesized. Regarding recovery attitudes, the personal confidence and hope scales of the RAS were significantly negatively associated with General Criminal Thinking, which was also consistent with our hypotheses. However, contrary to our hypotheses, these associations did not vary between ACT and FACT program participants. As expected, General Criminal Thinking was positively associated with the number of lifetime arrests, but this association did not differ by program type; although, individuals in ACT programs reported fewer lifetime arrests than those in the FACT programs. Last, individuals in the ACT programs had a larger number of lifetime hospitalizations than those in the FACT program; however, the association between General Criminal Thinking and number of lifetime hospitalizations was not significant and did not vary by program type.
The positive relationship found between psychiatric symptomatology (i.e., level of distress, number of symptoms) and criminal thinking supports the assertion that criminal thinking and psychiatric symptomatology should be conceptualized as comorbid, yet distinct, disorders and treated concurrently (Draine et al., 2002; Hodgins et al., 2007; Morgan et al., 2010). Treatment needs, both psychiatric and criminogenic, become increasingly important with elevated criminal thinking or increased psychiatric symptomatology. Community mental health consumers should be screened for criminogenic treatment needs (e.g., criminal thinking), regardless of CJ involvement and program involvement, as consumers with greater psychiatric symptomatology simultaneously evidenced greater criminal thinking.
Consequently, individuals who report comorbid mental health and criminogenic treatment needs would necessitate treatment that integrates criminal risk factors as treatment foci, in addition to the mental health programs currently in place (Epperson et al., 2011). Furthermore, previous research has advocated for a more integrated approach, such that treatment focused on both the criminogenic (e.g., substance abuse, emotions management, criminal attitudes, criminal associates) and psychiatric (e.g., medication compliance, mental illness awareness, social skills, problem-solving) needs of PMI at risk for CJ involvement will likely be most efficacious (Moran & Hodgins, 2004; Morgan et al., 2010). This concept is demonstrated in the fact that ACT programs are empirically supported and have been shown to improve mental health functioning, but minimal improvements in CJ outcomes are achieved (Calsyn, Yonker, Lemming, Morse, & Klinkenberg, 2005; Morrissey, Meyer, & Cuddeback, 2007).
Increased criminal thinking was associated not only with increased psychiatric symptomatology, but also with increased contact with the CJ system via arrests, and individuals in the FACT program had significantly more lifetime arrests compared with those in the ACT program when holding criminal thinking constant. Although this difference was statistically significant, the practical significance of this finding may be limited given that this finding indicates a difference of less than one lifetime arrest between the two treatment groups. Generally, this positive association is problematic, as arrest can interfere with recovery and mental health functioning by disrupting the continuity of care (Adair et al., 2005; Brekke, Ansel, Long, Slade, & Weinstein, 1999; Greenberg & Rosenheck, 2005). Furthermore, frequent CJ contact provides greater opportunities to commit additional criminal acts (e.g., assault on a public servant, resisting arrest) and may increase the likelihood of incarceration, which can subsequently increase the risk for mental health decompensation (Bauer, 2012) and victimization (Blitz, Wolff, & Shi, 2008).
In addition, criminal thinking was not associated with the number of lifetime hospitalizations; however, ACT consumers reported a greater number of lifetime hospitalizations. This suggests that criminal thinking may result in behaviors that are more likely to result in illegal behavior (e.g., violating the rights of others) versus behavior that would indicate mental health decompensation (e.g., suicidality, poor self-care) and warrant hospitalization. It is also possible that first responders are most commonly law enforcement officers and not mental health professionals. Law enforcement may be more likely to view illegal behavior as a manifestation of underlying criminal thinking or other criminal dispositions versus psychiatric symptomatology. For example, it is possible that PMI with increased criminal thinking are more verbally abusive or threatening toward law enforcement officers resulting in the decision by CJ officials for PMI to be processed through the CJ system versus being deferred to mental health services (e.g., hospitalization in lieu of arrest).
Given that participants rarely had no contact with the CJ system and that criminal thinking was positively associated with the number of lifetime arrests, the results of this study suggest most PMI will have multiple contacts with the CJ system throughout their lifetime. To enhance continuity of care in the transition from incarceration to the community, integrated treatment approaches should be present in correctional treatment programs as well. Once diversion opportunities are created within the community, joint partnerships between the CJ and community mental health system should be fostered. Creating positive working relationships and developing an integrated mental health and CJ database accessible by both systems could facilitate identification of PMI who become involved in the CJ system that may benefit from community-based diversion programs. In addition, this partnership could increase the continuity of care when PMI are initially incarcerated and when they are released back into the community to assist with reentry and increase the likelihood of successful reintegration.
Enhanced services and improved CJ responses for PMI would require program funding to hire additional staff, train preexisting staff, and develop new treatment programs in an already strained local, state, and federal budget. However, it may prove fruitful to advocate for funding based on evidence that programming saves money. For example, it has been shown that appropriate treatment programs that address the needs of persons involved in the CJ system result in treatment gains that decrease financial (e.g., cost of incarceration) and societal (e.g., community safety) costs (Romani, Morgan, Gross, & McDonald, 2012).
Focusing on the mental health of consumers, those with higher psychiatric symptomatology reported higher criminal thinking. In addition, consumers who reported having more personal confidence and hope also reported less criminal thinking. It is possible that individuals with greater criminal thinking are more pessimistic about their mental health recovery. Treatment providers should be aware that consumers’ perception of their recovery may not be realistic or accurate and should consider building confidence and hope about mental health recovery (e.g., challenging negative automatic thoughts about recovery failure and highlighting treatment progress). Ensuring that consumers’ perception of their recovery is accurate allows treatment providers to increase the likelihood that appropriate interventions are delivered with appropriate intensity.
No significant differences in criminal thinking were found between the consumers in ACT and FACT programs and those with and without a history of CJ involvement. These findings were contradictory to the hypotheses, which could be due to no differences existing between the populations or because the analyses lacked sufficient power. However, with regard to the lack of significant differences in criminal thinking, a more likely explanation for this finding is that the general lack of availability of FACT programs in most community settings may result in individuals with high criminal risk (e.g., a significant history of CJ involvement) being assigned to ACT when no FACT programs are available. As previously mentioned, a vast majority of the consumers in this study reported a history of CJ involvement (83.3%), which suggests that consumers with criminogenic needs were placed in FACT and ACT programs. In most cases, individuals with high criminal thinking only have ACT programs available. This may result in their mental health treatment needs being addressed without concurrent treatment to address their criminogenic needs. This is problematic given that mental health treatment that makes positive psychiatric gains fails to improve CJ outcomes (Calsyn et al., 2005; Morrissey et al., 2007). Results of this study suggest that ACT and FACT programs are composed of similar consumers with regard to mental health functioning and criminal risk.
Despite the important findings of this research, it is not without limitations. The data in the current study are cross-sectional, which precludes any conclusions about causal relationships. Future research should consider employing longitudinal designs to better understand the temporal associations between the variables of interest. In addition, the current study utilized a short form of the PICTS-L (35 items), and it is possible that the using of the full-length PICTS-L (80 items) could yield different conclusions. Thus, replication of the current study using the full-length PICTS-L is warranted. An analytical procedure (i.e., cell weighting based on unequal sample sizes) was utilized to allow for the multivariate analyses to be conducted with unequal sample sizes across groups. Analyses with relatively equal sample sizes are preferred as they retain greater power (Tabachnick & Fidell, 2007), and the power to detect potential differences in this study may have been compromised as one of the groups (i.e., no CJ involvement, FACT participant) during each comparison was relatively small (less than 50 in some cases). Moreover, given the number of analyses conducted it is possible that the probability of Type I error was inflated; therefore, we encourage replication of our results. Last, generalizability may also be limited in that the participation rate of programs was quite low, and programmatic variables (e.g., funding, staff support, treatment interventions) could differ across sites, and it was not possible to ensure that our samples were representative of the programs’ populations. Similarly, it is possible that the participants with missing data who were excluded from the analyses were a unique population and our findings do not apply to them, which limits the generalizability of our findings to all community mental health clientele. Therefore, it is important that the current study is replicated with programs in other geographic areas and with verifying resources to increase the generalizability findings of the current study.
The results of this study suggest that as PMI’s psychiatric symptoms worsen, criminal thinking increases as well; thus, demonstrating a relationship between these two variables. Increasing our understanding of this relationship is important and warrants further investigation to determine if one precedes the other or if the relationship is bidirectional. In addition, other measures of psychiatric decompensation/health and criminal risk could provide greater insight into the relationship between criminal thinking, criminal behavior, and mental health.
Footnotes
Opinions expressed in this article are those of the authors and do not necessarily represent the opinions of the Federal Bureau of Prisons or the Department of Justice.
This project was funded by the Center for Behavioral Health Services & Criminal Justice Research.