
Abstract
Recent anecdotal reports have suggested that disciplinary segregation in prison is disproportionately used against mentally ill inmates. To date, little research has examined this phenomenon empirically. This study analyzes the impact of a prediagnosed mental illness on the likelihood an inmate is sentenced to segregation following an institutional misconduct in state facilities. Findings suggest that inmates with a mental illness have a higher likelihood of being sentenced to segregation compared with inmates without a mental illness (odds ratio [OR] = 1.36), net of other factors. Further analyses indicate that mentally ill inmates are more likely to receive segregation compared with a range of other less serious disciplinary actions. Practical implications and directions for future research are explored.
Keywords
Introduction
Despite a recent decrease in the overall U.S. correctional population, almost 7 million men and women were incarcerated as of yearend 2015 (Kaeble & Glaze, 2016). Prisoners who have been previously diagnosed with a mental illness make up an estimated 37% of prison inmates and 44% of jail inmates, ranging from anxiety or depression to severe psychotic disorders (Bronson & Berzofsky, 2017). Indeed, individuals with mental illnesses are disproportionately represented in the inmate population at roughly 3 times the rate in the general population (Prins & Draper, 2009). Correctional facilities have become one of the largest mental health service providers in the country (Al-Rousan, Rubenstein, Sieleni, Deol, & Wallace, 2017), as U.S. prisons and jails in some states housed almost 10 times more individuals with mental illnesses than mental hospitals in 2004 (Torrey, Kennard, Eslinger, Lamb, & Pavle, 2010).
This is concerning for correctional facility operators, as those with mental illnesses require special consideration; mental illness symptoms can result in violent or risk-taking behavior including self-harm (Bersot & Arrigo, 2010), and those with mental illnesses are more likely to be charged with misconduct (Al-Rousan et al., 2017; Toch & Adams, 1986), be victimized in prison (Blitz, Wolff, & Shi, 2008), and recidivate once released (O’Keefe, Klebe, Stucker, Sturm, & Leggett, 2010). Further complicating the situation, correctional institutions have limited resources to treat and handle inmates (Adams & Ferrandino, 2008), with complaints of mistreatment by prison officials recently spilling into the public sphere through a number of high-profile cases. Since 2014, inmates have filed lawsuits against several jurisdictions alleging systematic abuse of inmates by officers (e.g., Cook County, Illinois; Denver County, Colorado; Floyd County, Indiana; LA County, California; and the state of Alabama), including excessive use of force (Bauer, 2014; A. Cohen, 2014) and corruption (Rucke, 2014). Especially troubling, the now-settled lawsuit in LA County alleged that correctional officers would target mentally ill inmates for abuse (Rosas v. Baca, 2013; Winter & Eliasberg, 2014), while the judge in the case against Alabama ruled that the state provided “horrendously inadequate” mental health care that “start[ed] at the door” (Braggs v. Dunn, 2017, pp. 17, 299). Indeed, the judge’s opinion goes on to cite alarming problems of understaffing, inadequate care and treatment, and the inappropriate use of disciplinary actions and segregation (Braggs v. Dunn, 2017). This includes keeping mentally ill inmates in segregation in response to suicide attempts (Ford, 2017) or left in suicide-watch cells for months at a time (Elliott, 2017; Southern Poverty Law Center, 2016).
Although inmates who act out as a result of their mental illness may indeed violate institutional rules, several studies have demonstrated that isolation (i.e., solitary confinement or segregation) can have deleterious psychological effects, including insomnia, hallucinations, and paranoia (e.g., Abramsky & Fellner, 2003; Bersot & Arrigo, 2010; Metzner & Fellner, 2010; Steinbuch, 2014; see Smith, 2006, and Haney, 2003, for a brief review), which may be exacerbated by or exacerbate a preexisting mental condition (Adams & Ferrandino, 2008; Glancy & Murray, 2006). 1 In addition, mental illnesses can be considered a disability, where segregation as a punishment for actions caused by an illness is a violation of the American With Disabilities Act (Martin, 2014).
Although anecdotal evidence indicates that mentally ill prisoners are being placed in solitary confinement in response to their mental illness alone (Ford, 2017), there is little empirical analysis considering how mental illness may influence the disciplinary action given to an inmate after a misconduct violation, net of other factors. Seeking a more valid estimate of the unique effect of mental illness on segregation use, this study utilizes a sample from the 2004 Survey of Inmates in State and Federal Correctional Facilities (SISFCF) while minimizing the confounding effect of selection bias with propensity score weighting to control for a range of covariates that predict mental illness (Rosenbaum & Rubin, 1983; Shadish, Cook, & Campbell, 2002). Here, if those with a mental illness are significantly more likely to be assigned to segregation after weighting, there is empirical evidence that segregation is used in response to a mental illness alone.
Literature Review
Mental Illness and Prison Misconduct
The link between mental health problems and institutional misconduct has been explored by number of studies (e.g., Adams, 1983; Houser & Belenko, 2015; Houser, Belenko, & Brennan, 2012; Matejkowski, 2017; McCorkle, 1995; O’Keefe & Schnell, 2007), with the majority indicating a significant, positive relationship between the two covariates (Steiner, Butler, & Ellison, 2014). Indeed, in their review of the literature on misconduct, Steiner and colleagues (2014) found that nearly two thirds of models examining mental health problems and misconduct showed a positive relationship (46 out of 73 models), with the remaining third indicating a null relationship. These findings align with an importation perspective of explaining inmate misconduct, where inmate adjustment is based on preprison characteristics (Irwin, 1980; Irwin & Cressey, 1962), which has found support in past research (Cao, Zhao, & Van Dine, 1997; Houser et al., 2012; Jiang & Fisher-Giorlando, 2002; Steiner et al., 2014; Wooldredge, Griffin, & Pratt, 2001). Mentally ill inmates may not be able to adjust to the prison environment because of their preexisting conditions, where symptoms can manifest into behavior that is considered a violation of rules, such as aggression, refusing to follow orders, or self-mutilation (Fellner, 2006). Those with mental health problems may have less developed coping abilities, such as the ability to follow commands or adjust to a rigid schedule, ultimately affecting their ability to assimilate into the prison (Houser & Belenko, 2015; O’Keefe & Schnell, 2007; Toch & Adams, 1986).
To date, a number of studies have shown that mentally ill offenders are more likely to commit misconduct while imprisoned. Adams (1986) determined that offenders who were referred to mental health units were more likely to be charged with a disciplinary violation, which is often characteristic of a mental illness (i.e., self-injurious behavior). More recent research has found that seriously mentally ill inmates have higher rates of both violent and nonviolent misconducts (Felson, Silver, & Remster, 2012; Matejkowski, 2017; Steiner & Meade, 2016). In studies utilizing the 2004 SISFCF, those with preincarceration mental illnesses committed more assaults and substance violations (Steiner & Meade, 2016), whereas inmates with the specific diagnoses of depression and psychosis were more likely to engage in violence against inmates as well as nonviolent misconducts (Felson et al., 2012). When restricting the sample to only female inmates, Houser and colleagues (2012) found that those with a mental illness had higher odds of committing a serious infraction compared with those without (170% higher compared with no infraction, and 8% higher compared with a minor infraction).
Empirical evidence also shows that institutional context is an important factor in inmate misconduct (Camp, Gaes, Langan, & Saylor, 2003; Huebner, 2003; Steiner et al., 2014; Steiner & Meade, 2016; Steiner & Wooldredge, 2013, 2014). In their 2014 review of the literature, Steiner et al. (2014) found that a security level of maximum was the most reliable prison-level predictor of misconduct, with 78% of the models included showing a positive relationship and only 11% reporting an insignificant relationship between the covariates. Similarly, Steiner and Wooldredge (2013) and Huebner (2003) reported that higher levels of misconduct were observed in higher security facilities. Camp et al. (2003) also found that the average security level of inmates housed in institutions was significantly related to violent and drug misconduct; however, the authors note the problematic definitions of security levels in prisons (i.e., medium security may mix high- and low security–level inmates). Furthermore, the variations between state and federal institutional environments, such as differences in operations, inmate populations, or culture, may influence levels of misconduct (Butler & Steiner, 2017; Steiner et al., 2014; Steiner & Meade, 2016).
Misconduct violations are a costly concern for prison administrators, as a single misconduct costs an average of US$970, and mentally ill inmates have been found to commit the majority of misconduct infractions within institutions (Lovell & Jemelka, 1996). These inmates may most benefit from treatment of their illness, which can alleviate symptoms leading to misbehavior (Adams & Ferrandino, 2008). Despite this, correctional officers often have minimal mental health training, making it difficult to identify differences between intentional misconduct and symptomatic manifestations (Fellner, 2006; O’Keefe & Schnell, 2007).
Mental Illness and Disciplinary Actions
Balancing treatment and control of mentally ill inmates can be difficult for prison administrators (Adams & Ferrandino, 2008), who are responsible for treating rather than punishing individuals for disruptive behavior that is a result of their mental illness (Bersot & Arrigo, 2010; Faiver, 1998). However, with scarce resources for treatment and the primacy of safety and order, it can be difficult to reconcile the long-term needs of the mentally ill with the short-term needs of institutional control (Fellner, 2006). This can often push treatment and rehabilitation into a secondary position where mentally ill inmates may be controlled using isolation or segregation (O’Keefe, 2007), with past research showing that there is a disproportionate amount of mentally ill inmates in segregation units (Houser & Belenko, 2015; Lovell & Jemelka, 1996; O’Keefe, 2007; Stewart & Wilton, 2014; Wexler, 2003).
When an inmate is charged with a rule violation, a disciplinary process begins to determine his or her sanction. Similar to the initial charges of misconduct, the prison administration has considerable discretion in its disciplinary decisions with a myriad of punishments available, ranging in severity from a warning to solitary confinement (American Civil Liberties Union, 2005). Although prisoners have been guaranteed certain due process rights in these hearings by the Supreme Court, such as the ability to call witnesses and present evidence (Krelstein, 2002), administrators have considerable latitude in the disciplinary action assigned (Butler & Steiner, 2017; Fellner, 2006). Furthermore, although these hearings allow for competency assessments, inmates are not able to claim an insanity defense (F. Cohen, 2008). In his national survey on the role of mental health in prison disciplinary processes, Krelstein (2002) found a wide range of policies regarding mental health in these hearings. For instance, the majority of states have no formal policy regarding the consideration of mental health in the disciplinary process, whereas some (e.g., New York and Texas) do not allow mental health professionals to determine prisoner culpability or formally testify in disciplinary hearings (Krelstein, 2002).
Mental Illness and Segregation
Although state regulations vary regarding the role of mental health in the disciplinary process, multiple reports have shown that inmates with mental illnesses are disproportionately represented in segregation units (e.g., Abramsky & Fellner, 2003; Fellner, 2006; Lovell & Jemelka, 2007; O’Keefe et al., 2010; O’Keefe, 2007). Indeed, based on reports from the late 1990s and early 2000s, Abramsky and Fellner (2003) found that roughly a quarter of those in segregation in New York had mental health problems, and their time in segregation was 6 times longer than those who did not have mental health issues. Similarly, in Indiana, Iowa, Oregon, and Washington between roughly 30% and 50% of the inmates in segregation were mentally ill (Abramsky & Fellner, 2003). A more recent 2010 audit indicated that between 55% and 77% of inmates in segregation in Wisconsin had a mental illness (O’Keefe et al., 2010). However, in their empirical study of female offenders, Houser and colleagues (2012) observed a null relationship between mental illness and level of disciplinary action; only the level of prison misconduct (minor or serious) affected the type of disciplinary action taken. They also observed a null relationship between disorder type and the level of disciplinary action (Houser et al., 2012).
Segregation is used in correctional facilities for a variety of reasons, most notably for institutional safety (i.e., disciplinary segregation) or for the safety of a specific inmate (i.e., administrative segregation; Adams & Ferrandino, 2008). Although both types of segregation aim to ensure the safety of individuals and the order of the institution, only disciplinary segregation is considered a punitive sanction (Federal Bureau of Prisons, 2016), as prisoners are placed in disciplinary segregation as a result of a disciplinary action. Also known as special housing units (SHUs), segregation generally consists of isolation cells (Adams & Ferrandino, 2008) where inmates are kept in their cells up to 24 hr per day with little human interaction (Fellner, 2006). 2
Although segregation remains a popular method of discipline in U.S. prisons (Abramsky & Fellner, 2003; Steinbuch, 2014), multiple studies point to possible detrimental psychological effects of isolation on inmates, both on those with and without preexisting mental conditions (e.g., Andersen et al., 2000; Grassian, 1983; Haney, 2003; see Smith, 2006, for an in-depth review). Here, many studies have associated this type of isolation with negative psychological outcomes, including hallucinations, anxiety, depression, and paranoia (e.g., Abramsky & Fellner, 2003; Bersot & Arrigo, 2010; Metzner & Fellner, 2010; Steinbuch, 2014). In their review of the literature, Glancy and Murray (2006) concluded that although some of these findings have been methodologically criticized, the general consensus among past research shows that certain inmates experience negative effects from segregation, particularly those who have preexisting mental disorders. Segregation has been shown to worsen mental disorder symptoms (Metzner & Fellner, 2010) through stress, isolation, and a lack of structure (Abramsky & Fellner, 2003).
That being said, it should be noted that at least two studies focused on administrative segregation showed isolated inmates did not experience mental health declines at a significantly different rate than those not in isolation (O’Keefe et al., 2010; Zinger, Wichmann, & Andrews, 2001); however, both of these studies have been criticized due to data collection methods and sampling procedures (O’Keefe, 2007; Smith, 2006). Because of these concerns, solitary confinement of those with a mental disorder has been widely criticized on the basis of human rights, with experts arguing that it is at least unethical (Metzner & Fellner, 2010) and at most a violation of the Americans With Disabilities Act (Martin, 2014).
Recent research examines the allocation of disciplinary segregation based on inmate characteristics (Butler & Steiner, 2017; Olson, 2016). These studies align with the focal concerns perspective in judicial decision making, where officials rely on both legal and extralegal factors to determine an offender’s blameworthiness, risk, and consequences of punishment to allocate sanctions (Steffensmeier, Ulmer, & Kramer, 1998). Although the bulk of research on focal concerns looks at traditional court proceedings and sentencing decisions (e.g., Demuth & Steffensmeier, 2004; Freiburger, 2009; Harris, 2009; Kramer & Ulmer, 1996), Butler and Steiner (2017) and Olson (2016) found support for this perspective in the prison disciplinary context. Using data from the 2004 SISFCF, these studies determined that extralegal factors, including age and race, were associated with the assignment to segregation (Butler & Steiner, 2017; Olson, 2016). That being said, Butler and Steiner (2017) did not find a significant relationship between segregation and mental health; however their operationalization did not include those who indicated a mental illness that had been previously diagnosed by a mental health professional.
Current Inquiry
Despite multiple reports detailing the use of solitary confinement for mentally ill offenders (e.g., Braggs v. Dunn, 2017; Ford, 2017; Winter & Eliasberg, 2014), there has been little direct empirical study of the role of mental illness in levels of disciplinary action. Of the studies that exist, generalizable results are difficult to obtain as there is a focus on only one type of offender (Houser & Belenko, 2015; Houser et al., 2012) or certain types of mental disorder, such as those with serious mental illnesses (Matejkowski, 2017). Furthermore, although these studies control for potential selection bias through regression, there is little direct consideration of potentially impactful differences between those with a mental disorder and those without (Houser et al., 2012; O’Keefe, 2007). To address these gaps, this study employs a nationally representative sample including multiple categories of offender characteristics and propensity score weighting methods to equate those with and without a mental illness. Based on the past body of literature, this study explores the following research questions:
To address these questions, this research utilizes data from the SISFCF (2004; ICPSR 4572) to compare the disciplinary actions given to those with a mental illness and a weighted comparison group following a misconduct violation (Bureau of Justice Statistics, 2004). 3
Method
Data
The SISFCF is a nationally representative survey conducted by the U.S. Census Bureau, which employs a probability sample of inmates within federal and state institutions (Bureau of Justice Statistics, 2004). The survey is administered to inmates through computer-assisted personal interviewing, with almost 18,000 inmates participating in 2004, covering a wide range of topics including inmate behavior, criminal histories, personal backgrounds, and experiences within and outside of incarceration. The sample was restricted to only state inmates due to possible unmeasured factors in federal facilities that may affect their use of segregation, such as institutional structures (Butler & Steiner, 2017; Steiner & Wooldredge, 2013). The sample was further restricted to those who committed at least one misconduct during their incarceration and were not missing data for a mental illness or a disciplinary action (N = 5,823; mental illness = 1,904, no mental illness = 3,919).
Dependent Variable
The dependent variable under analysis is the most recent disciplinary action that the inmate received. Although segregation is the primary disciplinary action under consideration, the SISFCF asks inmates about a range of possible disciplinary actions (listed from least serious to most serious): none, other punishment, reprimand, lose privileges, lose work assignment, given extra work, lose good time/gain bad time, given new sentence, transfer to another facility, higher custody within same facility, confinement to own cell, or solitary confinement/segregation. The dependent variable is measured as a dichotomous outcome for logistic regression models (1 = solitary confinement/segregation, 0 = other disciplinary action) and a multinomial outcome for multinomial logistic regression (reference = solitary confinement/segregation). For the multinomial outcome, if the inmate reported multiple disciplinary actions, he or she was included in the most serious disciplinary category.
Independent Variable
For the purposes of this study, being diagnosed with a mental illness prior to incarceration is the independent variable. 4 The survey specifically asks inmates whether they have been diagnosed by a medical professional prior to incarceration with various mental disorders: depressive, psychotic, personality, manic/bipolar, posttraumatic stress disorder (PTSD), anxiety, or any other disorder. Because of low levels of certain reported disorders, mental illness is measured dichotomously (reference = no mental illness) for all regression models. Thus, inmates with a mental illness are compared with those who have not reported a mental illness diagnosis prior to incarceration.
Weighting Variables
To reduce possible selection bias between those with and without a mental illness, the propensity score weighting method used here considers covariates that are predictors of mental illness. Put another way, the covariates included estimate the probability that the offender would have a mental illness. Based on past studies focused on predictors of mental illness, especially those related to individuals involved in the criminal justice system, this model includes demographic and criminal history covariates that have been shown to be correlated to mental illness. Specifically, in terms of criminality, those with mental illnesses have been found to engage in more violent and nonviolent misconducts (Felson et al., 2012; Steiner & Meade, 2016), have a higher number of prior arrests and incarcerations (Baillargeon, Binswanger, Penn, Williams, & Murray, 2009; Bronson & Berzofsky, 2017; O’Keefe et al., 2010), be more likely to engage in substance use (Cain, Steiner, Wright, & Meade, 2016; Diamond, Wang, Holzer, & Thomas, 2001; Houser et al., 2012), and be incarcerated for specific instant offense types (Bronson & Berzofsky, 2017; Cain et al., 2016; Lamb & Weinberger, 1998).
Demographically, mental illness has been associated most notably with age, race/ethnicity, and sex (see Diamond et al., 2001, for a brief discussion). Additional studies have also reported a link between mental illness and a number of other demographic factors, specifically marital status (Bronson & Berzofsky, 2017; Coombs, 1991), learning disabilities (Deb, Thomas, & Bright, 2001; Diamond et al., 2001), educational attainment (Diamond et al., 2001; P. White, Chant, Edwards, Townsend, & Waghorn, 2005), past employment (Ditton, 1999; Stuart, 2006), prior homelessness (Bersot & Arrigo, 2010; O’Keefe & Schnell, 2007; Prins & Draper, 2009), and a history of sexual and/or physical abuse (Cain et al., 2016; Mulder, Beautrais, Joyce, & Fergusson, 1998). Table 1 describes each covariate included in the propensity score estimation.
Description of Propensity Score Estimation Covariates
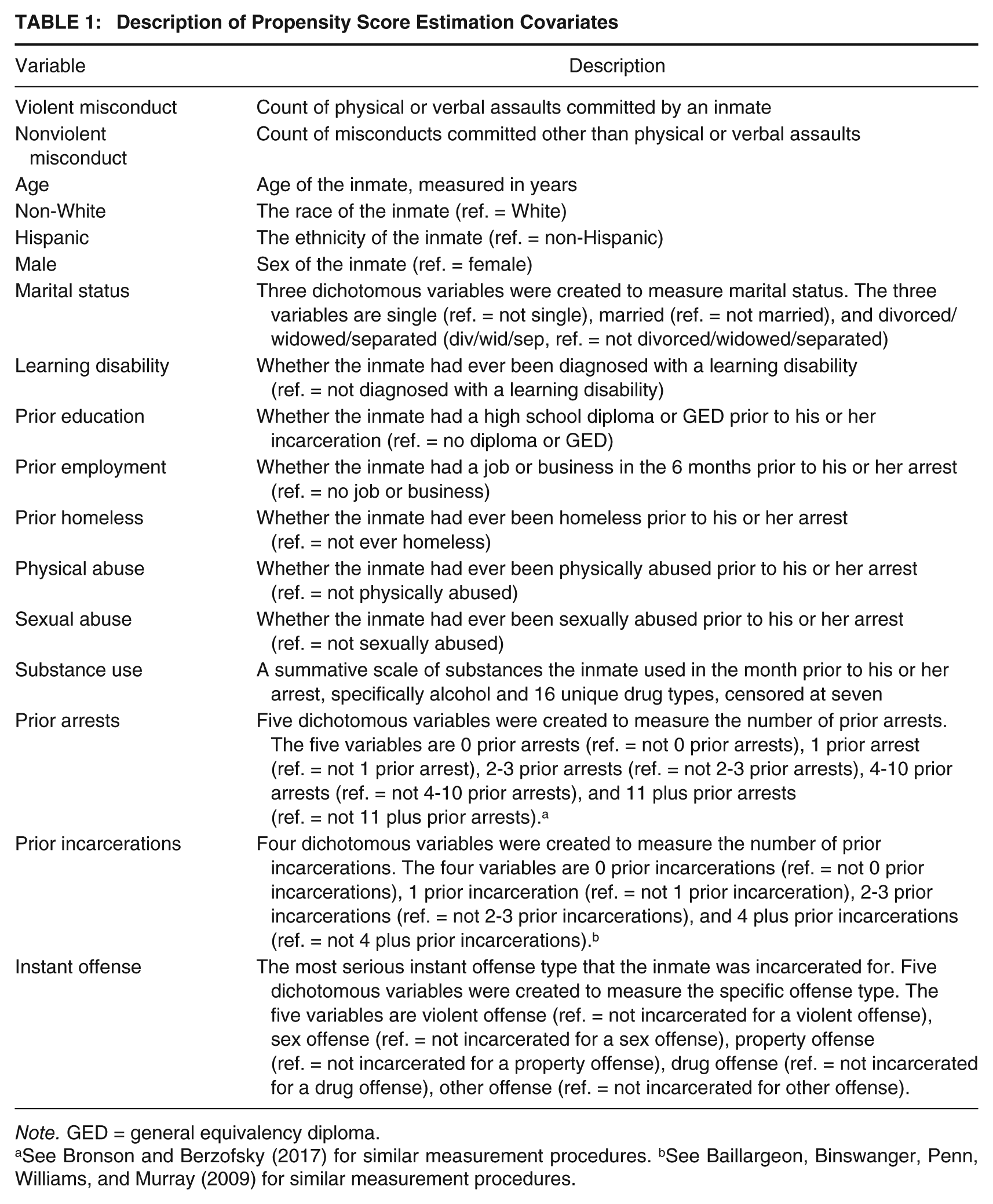
Note. GED = general equivalency diploma.
See Bronson and Berzofsky (2017) for similar measurement procedures. bSee Baillargeon, Binswanger, Penn, Williams, and Murray (2009) for similar measurement procedures.
Missing Data
Despite the initial data reductions previously described, several cases contained missing data on the control variables listed above. In total, 5,216 of the cases contained complete data (90%), with the bulk of the remaining cases missing data on only one control variable (432 cases) and the rest missing data for between two and five control variables (175 cases). To utilize as much data as possible, multiple imputation of missing values was employed through the “Amelia” package in R, which uses an expectation maximum algorithm for the prediction of plausible values (Honaker, King, & Blackwell, 2014; R Core Team, 2015). A total of 20 data sets were imputed and combined for all estimates. Table 2 presents descriptive statistics for the analysis groups as well as the results of imputation.
Univariate Descriptive Statistics, Missing Data, Multiply Imputed Data
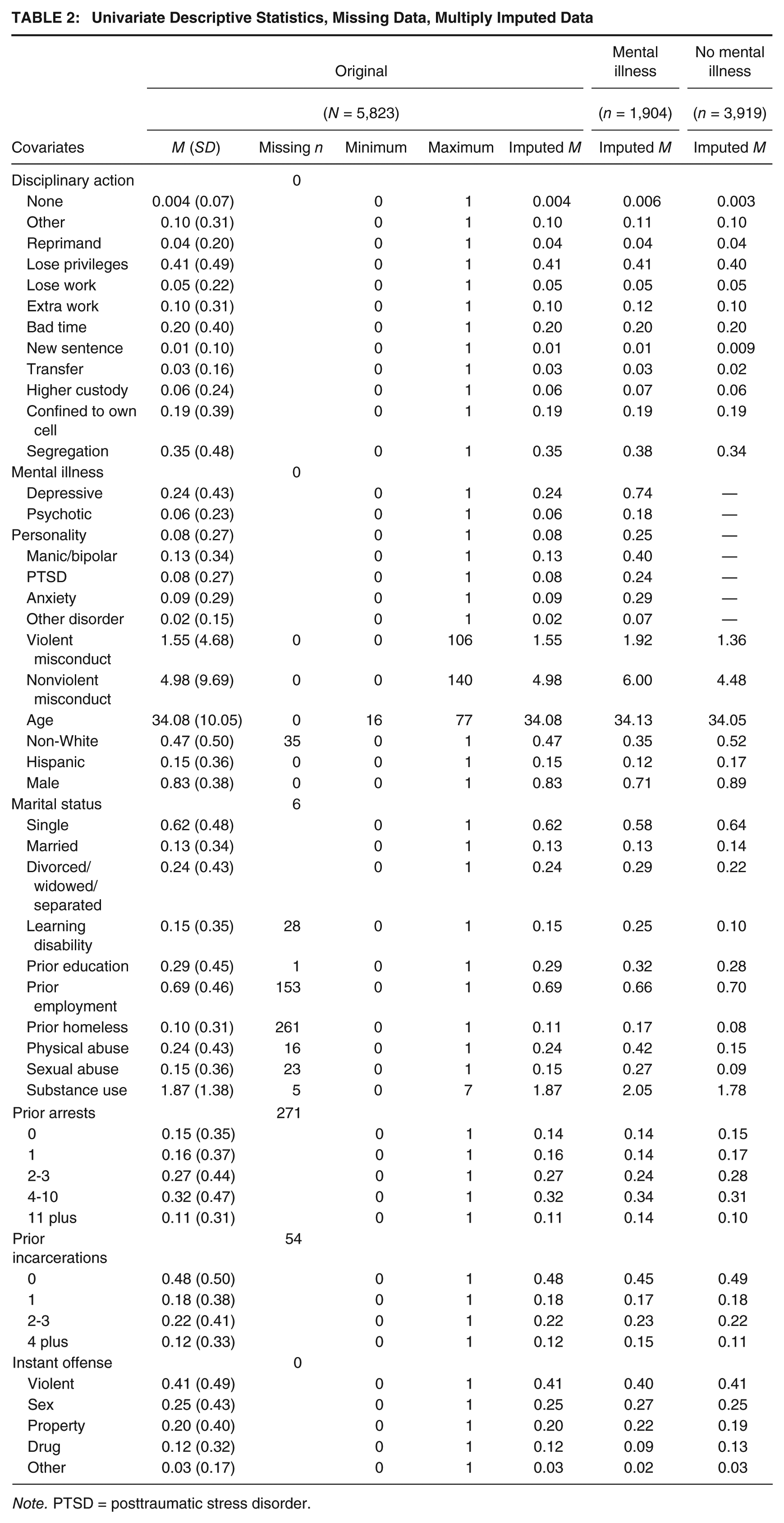
Note. PTSD = posttraumatic stress disorder.
Propensity Score Weighting
It is possible that selection bias may affect the analyses presented here (Shadish et al., 2002), as there may be important differences between those with a mental illness and those without that could confound the assessment of any effects. For example, an inmate with a mental illness may have a higher number of misconduct infractions, which would increase his or her chances of being placed in segregation compared with those without a mental illness. Thus, it is necessary to employ a propensity score technique to minimize the threats of selection bias by better equating the groups prior to the estimation of effects (Rosenbaum & Rubin, 1983).
Propensity scores were first estimated using a covariate balance propensity score (CBPS), an estimation method that maximizes covariate balance between groups (Imai & Ratkovic, 2014). Using the “CBPS” package in R (Fong, Ratkovic, & Imai, 2014), the CBPS weights the nonmentally ill inmates so that they resemble the mentally ill, reflecting the average treatment effect on the treated (ATT). Once the scores were derived, the sample was weighted using marginal mean weighting through stratification (MMW-S), which first splits the sample into strata based on the CBPS and then weights comparison units based on their strata membership, ultimately reducing differences to approximate random assignment on the observables (Hong & Hong, 2009; Leite, 2017). Furthermore, this method reduces the sample to only cases that have propensity scores that are found in both groups, eliminating any case that does not have common support. The MMW-S weighting procedure eliminated 16 cases (0.3%). These methods have been shown to be successful in past criminological research (Clark & Rydberg, 2016; Grommon, Rydberg, & Carter, 2017; Rydberg & Clark, 2016).
Covariate imbalance is assessed using a standard difference measure that estimates the imbalances between the two groups on the given covariate, with a score above 0.2 considered imbalanced (Austin, 2011). As shown in Table 3, there were several imbalanced covariates between the groups prior to weighting, with the overall average standard difference exceeding the imbalance threshold, thereby supporting the use of a propensity score weighting method. After weighting, all included covariates are below the 0.2 threshold with many large reductions in imbalance.
Covariate Balance Before and After MMW-S Weighting
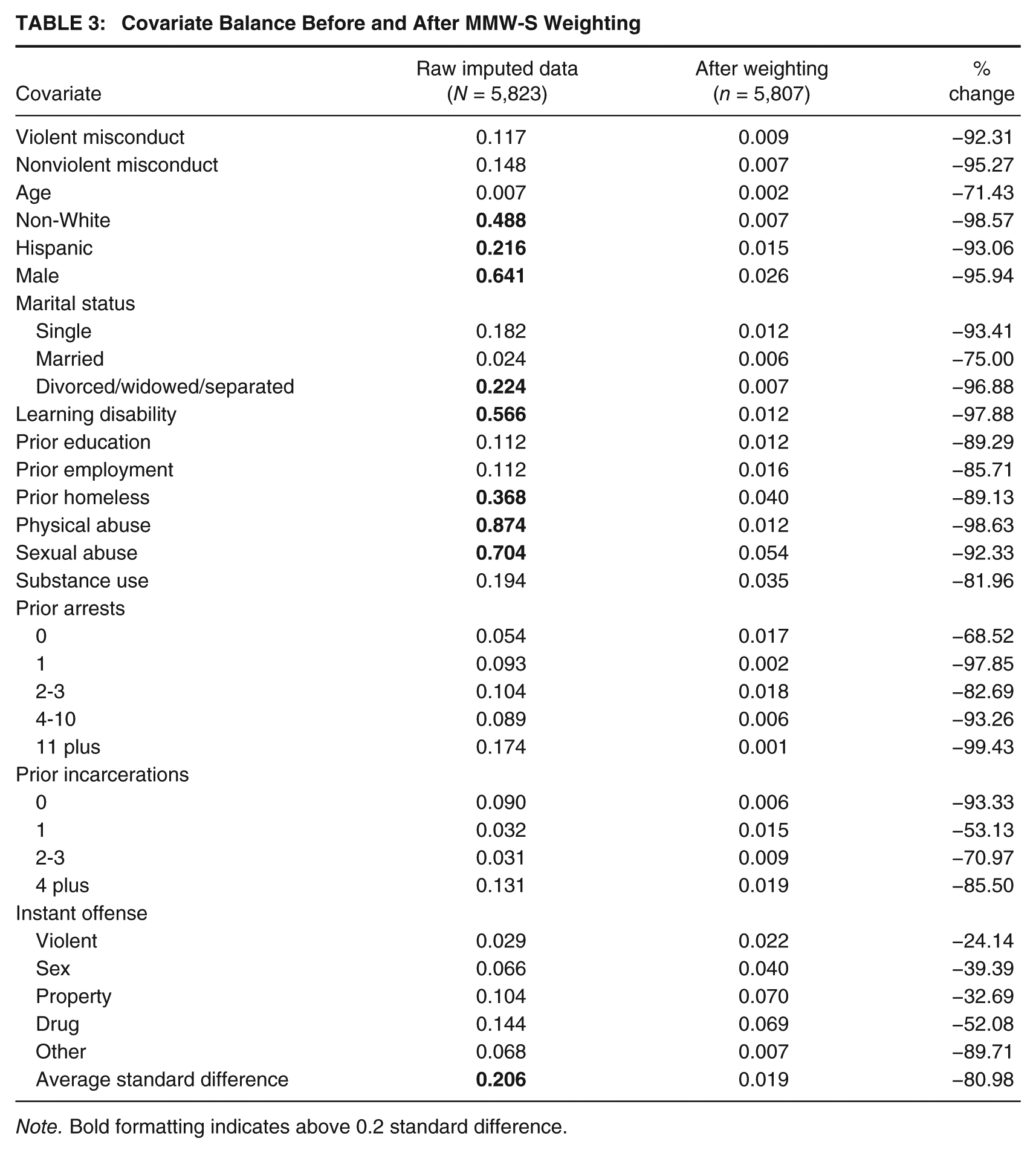
Note. Bold formatting indicates above 0.2 standard difference.
Analytical Strategy
After the sample was weighted, two analyses were carried out to assess the relationship between mental illness and disciplinary action. First, a weighted logistic regression model was estimated using the dichotomous outcome of segregation compared with other disciplinary actions. Second, a weighted multinomial logistic regression was estimated using segregation as the reference, to determine how segregation is utilized compared with each other individual category of disciplinary action. 5 All results presented represent pooled estimates from the imputed data sets. Each analysis uses robust estimation to control for remaining differences beyond the weights by including all covariates in the regression equation. To account for the possibility of correlated errors within institutions, all standard errors have been estimated using clustered robust estimation. 6 For ease of interpretation, only effects for mental illness on segregation are presented here; however, full results are available upon request.
Results
Tables 2 and 3 illustrate some important observations about inmates with and without a mental illness, which should be considered before results are estimated. As shown in Table 2, many of the univariate statistics are fairly consistent between those with and without a mental illness, with a similar average age (roughly 34 years), number of prior arrests (most commonly four to 10), and most often being a violent offender (roughly 41%). In terms of disciplinary actions, both groups most often lose privileges (roughly 41%), although segregation is a close second (roughly 35%), and least often are given no disciplinary action (less than 1%). However, there are also differences, some of which may affect the analysis if uncontrolled. Those with a mental illness have a statistically significant higher average number of nonviolent misconducts (6.00 compared with 4.48; t = 4.08, p ≤.001) and violent misconducts (1.92 compared with 1.36; t = 5.02, p ≤ .001). When comparing these groups, Table 3 indicates that indeed some covariates are imbalanced between the groups, including being female, race/ethnicity, and a history of abuse. After weighting, all covariates are balanced according to the 0.2 threshold, with many large reductions in imbalance (Austin, 2011).
After the covariates were balanced using the MMW-S weights, the results of the weighted logistic regressions indicate that inmates with a mental illness are statistically significantly more likely to be given segregation as a punitive sanction compared with the aggregated other disciplinary actions in state institutions (odds ratio [OR] = 1.36, SE = 0.07, p ≤ .001, Nagelkerke R2 = .05). Here, the odds of those with a mental illness being put into segregation following a misconduct are 36% higher than those without a mental illness. This shows a positive relationship between having a prediagnosed mental illness and being given segregation as a punishment, net of other covariates.
Weighted multinomial logistic regressions were then estimated to determine whether those with a prediagnosed mental illness are more likely to be placed in segregation compared with the other disciplinary actions. These results are presented in Figure 1, with each disciplinary action being compared with segregation; these can be interpreted as separate logistic regressions, with the disciplinary action as the measured (1) category and segregation as the reference (0) category. Those with a mental illness are consistently less likely to be given the presented disciplinary actions compared with segregation, with no ORs exceeding 1.0. In terms of the statistically significant findings, those with a mental illness in state institutions are 40% less likely to be given other disciplinary action, 27% less likely to lose privileges, 23% less likely to be given extra work, 19% less likely to be given bad time, and 27% less likely to be confined to their own cell, all compared with segregation. In other words, these results show that inmates with a mental illness are more likely than those without to be given a severe punishment (segregation) compared with certain other less severe disciplinary actions.
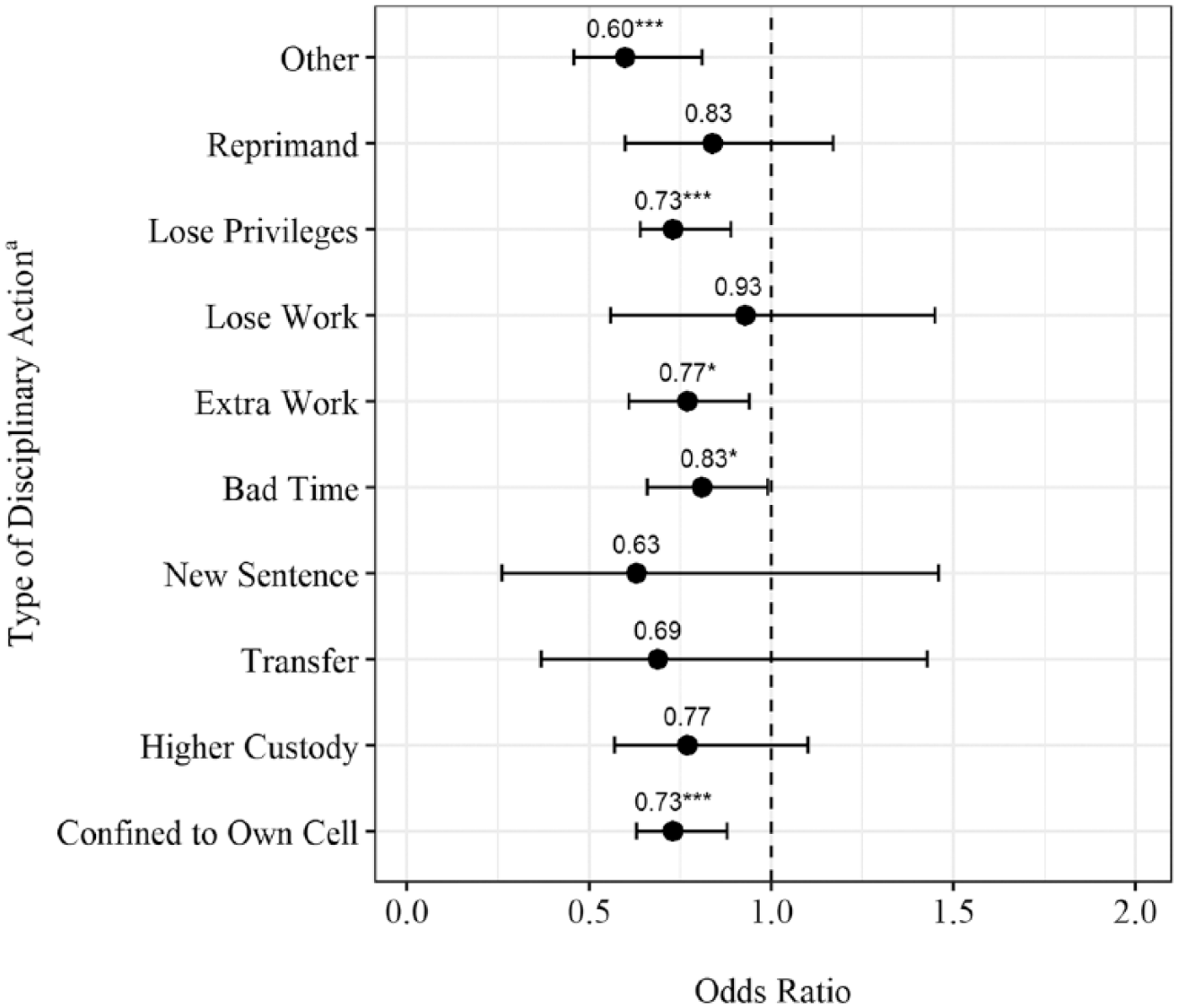
Weighted Multinomial Logistic Regression Model on Type of Disciplinary Action (N = 5,807)
Discussion and Conclusion
Despite news stories outlining the problematic use of isolation for mentally ill inmates, little empirical consideration has been given to this important issue for correctional practice. This study aimed to explore the relationship between mental illness and disciplinary action, specifically solitary confinement, by analyzing the following research questions:
Utilizing the 2004 SISFCF, this study adds to the literature with a nationally representative sample of various inmate types and attempting to control for selection bias beyond the regression framework using a propensity score weighting method to equate those with a mental illness to those without a mental illness to the extent possible.
The findings illustrate important considerations for practice and policy going forward. Inmates with a mental illness were found to engage in more violent and nonviolent misconduct than their counterparts without a prediagnosed mental illness. Mental illness was also found to affect the likelihood of being disciplined using segregation as those with a mental illness were more likely to be placed in segregation when compared with the aggregate of all other disciplinary options. Here, an inmate with a mental illness is 1.36 times as likely to be placed in segregation compared with those without a mental illness. Because the nonmentally ill group has been weighted to resemble the mentally ill group, the only observable difference between groups is the presence of a mental illness; thus, there is evidence that these inmates are being segregated for their mental illness alone, rather than their misconduct record.
Those with a mental illness are also more likely to receive a sanction of segregation following a misconduct compared with a range of less serious disciplinary actions. Specifically, those with a mental illness are between 0.60 and 0.81 times as likely to be punished with being confined to their own cell, given extra work or bad time, lose privileges, or be given other disciplinary action compared with segregation. However, there are some disciplinary categories that have a null relationship when compared with segregation, namely, reprimand, loss of work, a new sentence, or being generally transferred or transferred to higher custody. Thus, segregation is a more likely option when compared with certain disciplinary actions, however, not when compared with all other disciplinary actions. Although a number of states restrict the use of solitary confinement as a reaction to mental illness alone (Krelstein, 2002), the findings indicate that this is likely occurring.
There are a number of possible explanations for these observed relationships. Consistent with past research, the findings support the importation theory of inmate misconduct (Adams, 1986; Felson et al., 2012; Houser et al., 2012; Matejkowski, 2017; Steiner et al., 2014; Steiner & Meade, 2016). Here, higher levels of misconduct may be explained by mentally ill inmates acting out due to symptomatic behaviors of a mental illness (i.e., their preprison characteristics affect their ability to assimilate into the prison culture), such as aggressive behavior or reduced coping abilities (Fellner, 2006; Houser et al., 2012). Extending this to segregation, prison management may be paying more attention to those with mental illnesses, or more attention to the actions of those with mental illnesses (Cao et al., 1997), ultimately resulting in more infractions and harsher punishments.
Relatedly, administrators may be using segregation to control those with a mental illness based on motivations not measured in the SISFCF. Because many institutions suffer from a lack of resources, space, and staffing, isolation of mentally ill prisoners can be seen as the only viable option in dealing with these inmates (Office of the Inspector General, 2017). In this case, segregation may be disproportionately used for those with a mental illness because they are seen as especially dangerous to themselves or others, which warrants the use of solitary confinement as a disciplinary tactic (Smith, 2006). Similarly, the result of a disciplinary action does not exist in a vacuum, and the disciplinary hearing process may be a crucial mechanism linking mental illness to segregation, net of other factors. Indeed, there is little research on the decision-making process in these hearings, so there is a lack of clarity in how they function between correctional institutions (Butler & Steiner, 2017; Krelstein, 2002). Officials are given broad power to determine a sanction (Fellner, 2006), aimed at punishing, deterring, and protecting the prison community (Bersot & Arrigo, 2010); reviews that consider a range of characteristics (i.e., not only misconduct history) are the norm (Steinbuch, 2014). This is further complicated by the lack of mental health integration in these hearings, where, in many cases, mental health professionals are not allowed to testify and inmates are not permitted to use an insanity defense regarding their culpability for misbehavior (Fellner, 2006).
Although these motivations and processes are not directly measured in the survey, mentally ill offenders are often seen as dangerous and uncontrollable by the public (Carroll, Wiener, Coates, Galegher, & Alibrio, 1982; Link, 2008; Rabkin, 1980), a stigma that can extend to prison officials (Adams, 1986; Matejkowski, Caplan, & Wiesel Cullen, 2010; Prins & Draper, 2009). Thus, the findings also support the focal concerns perspective, where punishments are based on concerns regarding those with a mental illness. Here, the mentally ill may be perceived as more blameworthy when they commit misconduct, resulting in harsher punishments. In addition, the stigma associated with mental illness can lead officials to want to protect the prison community from such behavior by using segregation (B. D. Johnson, 2006; Steffensmeier et al., 1998). Although the focal concerns perspective has largely been applied to traditional court systems, Butler and Steiner (2017) and Huebner and Bynum (2006) found support for the perspective in segregation and parole decisions, respectively, with both legal and extralegal factors influencing decision making in these contexts.
Correctional administrators may also be under pressure to utilize their solitary confinement to control overcrowding and costs, which may adversely affect those with a mental illness (Steinbuch, 2014). Recent data show that solitary confinement units are expensive to maintain (C. Johnson & Chappell, 2014), which may drive administrators to keep them full to justify their existence. In addition, overcrowding may motivate administrators to disproportionately use solitary confinement to ease strain on the general population (Hresko, 2006). Here, the mentally ill again may be more vulnerable to punishment using segregation, as prison administrators subconsciously (or overtly) view these inmates as particularly problematic due to their characteristics, ultimately using their diagnosis as a justification to use solitary confinement and, thereby, reducing administrative pressures (Steinbuch, 2014).
Limitations
There are some limitations to the current research that should be discussed, particularly those related to the use of the SISFCF and secondary data analysis. The survey data are limited by the questions asked, lacking possibly important contextual information that would aid in the identification of mechanisms explaining the observed relationships. Notably, the survey does not measure the security level of state institutions, which has been shown to be an important factor in misconduct (Huebner, 2003; Steiner et al., 2014), the handling of mentally ill inmates (McCorkle, 1995; T. W. White, Schimmel, & Frickey, 2002), and disciplinary actions (Butler & Steiner, 2017). However, a large number of covariates have been included in the weighting procedures to help account for characteristics that may affect these processes regardless of security level, which is an improvement over past research. That being said, the technique is only as good as the variables that are used to weight cases, meaning there may be unobserved differences between the groups. It is also unclear in the survey how inmates are defining segregation or solitary confinement (e.g., are they considering administrative segregation a type of segregation), which may be an important distinction. However, because the survey specifically asks about punishment following disciplinary action, it can be reasonably assumed that the inmates are only reporting disciplinary segregation.
Conclusion
Overall, the analyses presented here have generated empirical evidence that mental illness is a unique predictor of assignment to disciplinary segregation. The limitations notwithstanding, there are some important points of consideration for future research and policy. First, future research should drill down into the meaning of segregation and solitary confinement. Solitary confinement comes in many forms, all of which utilize isolation in different ways and for different means. To truly understand how mental illness affects segregation and vice versa, it is necessary to consider each of these variations of segregation (Adams & Ferrandino, 2008). Second, future research should attempt to focus on the black box of disciplinary hearings; here, it would be beneficial to examine the specific role of mental illness in the disciplinary process. There is little information on the mechanisms at work in handing out disciplinary punishments within institutions (Krelstein, 2002). A deeper understanding of the discretion exercised by officials in these hearings would help to explain the relationships seen in this research, especially as it relates to the focal concerns perspective.
Although administrators may see isolation as a way to effectively deal with this special population of inmates, when considering the effects of solitary confinement on mental health, this solution is counterproductive. Multiple studies have shown that those with mental health problems may be more susceptible to the negative effects of solitary confinement, thereby creating a cycle in which mentally ill offenders are put in solitary confinement due to their mental illness, which is made worse by isolation, leading to further or worsening symptomatic behavior (Fellner, 2006; Metzner & Fellner, 2010).
Although solitary confinement may be considered a more economical or practical choice for containing these inmates, better mental health care can be more cost effective in treating their behavior (Smith, 2006). Indeed, recent studies have pointed to the importance of mental health care for those in the general population and, more importantly, in solitary confinement (Abramsky & Fellner, 2003). This includes recommendations for regular mental health checkups (Office of the Inspector General, 2017) and the integration of mental health professionals in the entire disciplinary process (Krelstein, 2002). A number of states are already attempting to incorporate new mental health policies, such as restrictions on time in solitary confinement (A. Cohen, 2014) and the use of therapeutic communities for those with a mental illness (Adams & Ferrandino, 2008). Although this is an important step, systematic change will be necessary to ensure public safety, given the possible deleterious effects of solitary confinement coupled with the increased likelihood of recidivism of those with a mental illness.