
Abstract
A large body of research links both a lack of self-control and adverse childhood experiences (ACEs) to a variety of negative health and behavior outcomes, including delinquent and criminal behavior. To date, relatively little research considers whether experiencing a greater variety of ACEs is associated with lower self-control. We advance this area of research by first articulating potential mechanisms through which ACEs may impact self-control. We then investigate whether experiencing more ACEs is inversely associated with self-control in separate samples of youth from Michigan and Florida. For both samples, results indicate that experiencing a greater variety of ACEs is negatively associated with self-control. Exploratory analyses also indicate that ACEs reflecting interpersonal maltreatment are more strongly associated with deficits in self-control than ACEs pertaining to aspects of household dysfunction.
Keywords
Introduction
Gottfredson and Hirschi’s (1990) general theory of crime, which emphasizes deficits in self-control as the primary cause of antisocial behavior, stands as one of the most prominent theories in the field of criminology. According to Gottfredson and Hirschi, a lack of self-control is characterized by six dimensions: impulsivity, risk-seeking, a preference for simple (as opposed to complex) tasks, a preference for physical (as opposed to mental) activities, self-centeredness, and anger. In support of the theory, multiple meta-analyses identify a lack of self-control as one of the strongest correlates of delinquency and crime (Pratt & Cullen, 2000; Vazsonyi, Mikuška, & Kelley, 2017). In addition, deficits in self-control are associated with a myriad of other negative outcomes across the life course, including poor health, reduced educational attainment, criminal victimization, and illicit substance use (Hay & Meldrum, 2016; Miller, Barnes, & Beaver, 2011; Moffitt et al., 2011; Pratt, Turanovic, Fox, & Wright, 2014).
Given the predictive value of self-control, researchers are keenly interested in causal paths associated with a lack of self-control. Many studies test Gottfredson and Hirschi’s (1990) hypothesis that ineffective parenting (i.e., a lack of parent–child attachment, inadequate supervision, and erratic discipline) contributes to poor self-control. On this point, several studies support this prediction (Botchkovar, Marshall, Rocque, & Posick, 2015; Burt, Simons, & Simons, 2006), though others do not (Vera & Moon, 2013; Wright & Beaver, 2005). Furthermore, many studies reveal key nonparenting sources of variation in self-control, including peer associations (Meldrum, Young, & Weerman, 2012), neighborhood and school contexts (Teasdale & Silver, 2009; Turner, Piquero, & Pratt, 2005), and heritability (Willems, Boesen, Li, Finkenauer, & Bartels, 2019).
These nonparenting causes of self-control illuminate the need to consider other sources of self-control variation, and fields of study outside criminology offer fruitful possibilities. Indeed, as criminologists were paying attention to self-control, health sciences researchers directed attention to adverse childhood experiences (ACEs). Attention to ACEs is based on the idea that life struggles during adolescence and adulthood are associated with adversities in childhood that have lasting influences on how individuals think, act, and relate with others. Driven by the work of Felitti and colleagues (1998), ACEs reflect experiences with the types of interpersonal maltreatment (e.g., abuse and neglect) and household dysfunction (e.g., family mental illness, parental incarceration) expected to be most consequential during childhood. Since the original ACEs study (Felitti et al., 1998), a growing body of research links ACEs with chronic disease, mental illness, risky behaviors, and poor socioeconomic outcomes (e.g., Hughes et al., 2017; Metzler, Merrick, Klevens, Ports, & Ford, 2017). Recent studies also link ACEs with delinquent behavior (e.g., Baglivio, Wolff, Piquero, & Epps, 2015).
Despite research focused on (a) the causes and consequences of a lack of self-control and (b) the varied outcomes of ACEs, these two strands of research have largely developed in isolation. Only recently have researchers started to consider the possibility that ACEs and self-control might be linked, such that experiencing a greater variety of ACEs could reduce self-control. For example, research links ACEs to the impulsivity dimension of (low) self-control (Perez, Jennings, & Baglivio, 2018) and a lack of future orientation (Craig, 2019). Other studies report that individually measured ACEs, including child abuse, family substance abuse, and family violence, are associated with reduced self-control (e.g., Bunch, Iratzoqui, & Watts, 2018; Hallquist, Hipwell, & Stepp, 2015; Meldrum, Trucco, Cope, Zucker, & Heitzeg, 2018).
Although these studies offer initial evidence that ACEs may reduce self-control, this association remains neglected in criminological research. If such an association exists, there are important implications for prevention and intervention efforts aimed at ensuring proper child and adolescent development. Central to this is the possibility that these two consequential risk factors—ACEs and deficits in self-control—may co-occur because one increases the likelihood of the other. Such a pattern would increase the need to identify programming to prevent the occurrence of both. But beyond prevention, this pattern would also prompt the need to intervene with youth encountering a high number of ACEs in ways that attend to the problems with low self-control that they may also possess. As we will discuss, there are compelling reasons to believe that ACEs may contribute to deficits in self-control, and we seek to bridge the ACEs and self-control literature in this study in two ways. First, we draw on arguments from social science and neuroscience lines of theory and research to describe the possible mechanisms through which ACEs might reduce self-control. Second, we investigate the association between ACEs and self-control by analyzing data collected from two large, independent samples of adolescents—one a community-based sample of youth from the Detroit Metro area in Michigan and the other a high-risk sample of youth detained in juvenile justice facilities in Florida.
ACEs and Associated Outcomes
Formulated by Felitti and colleagues (1998), the ACE inventory was developed in a primary-care health setting to assess the association between childhood adversity and later adult health-related outcomes. The ACEs self-report inventory is composed of items that capture experiences of abuse (physical, psychological, and sexual), neglect (physical and psychological), family violence, family substance abuse, family mental illness, parental incarceration, and parental separation/divorce (Centers for Disease Control and Prevention, 2016). In the original ACE study, Felitti and colleagues (1998) found that experiencing a greater variety of ACEs is linked to chronic disease and other health risk factors, including smoking, alcoholism, illicit drug use, obesity, and depressive symptoms. For example, relative to participants with zero reported ACEs, those with four or more ACEs were 7.4 times more likely to be an alcoholic and 10.3 times more likely to have injected illicit drugs (Felitti et al., 1998).
Advancement of the ACE literature has focused on evaluating whether ACEs impact other outcomes across diverse populations. For example, studies report that ACEs are associated with problematic drinking (Rothman, Edwards, Heeren, & Hingson, 2008), teenage pregnancy (Hillis et al., 2004), teenage paternity (Anda et al., 2002), and perceived well-being (Nurius, Green, Logan-Greene, & Borja, 2015). Other studies report that ACEs are associated with the risk of high school noncompletion, unemployment, and below-poverty household incomes (Metzler et al., 2017). 1 More pertinent to the field of criminology, several studies report an association between ACEs and antisocial behavior. For example, Baglivio and colleagues (2015) found that each additional ACE increases the likelihood of becoming a serious, violent, and chronic (SVC) offender by 35%. In line with Baglivio et al. (2015), earlier research reported a cumulative effect of ACEs on violence perpetration (Duke, Pettingell, McMorris, & Borowski, 2010). Additional research finds that SVC young offenders have higher ACE scores compared with youthful offenders who committed less serious offenses (Fox, Perez, Cass, Baglivio, & Epps, 2015).
However, the relationship between ACEs and deficits in self-control has been less scrutinized. This is a noteworthy omission given the known linkages between low self-control and delinquent behavior (Pratt & Cullen, 2000) and the potential that ACEs could retard the development of self-control. Although direct evidence linking ACEs to deficits in self-control (as conceptualized by Gottfredson & Hirschi, 1990) is absent from the literature, a small body of research reports that ACEs are associated with variation in concepts tangentially related to self-control. This includes externalizing behaviors (Hunt, Slack, & Berger, 2017; Muniz et al., 2019), impulsivity (Perez et al., 2018), a lack of future orientation (Craig, 2019), negative emotionality (Wolff & Baglivio, 2017), and poor delay of gratification (Evans, Fuller-Rowell, & Doan, 2012). Hunt and colleagues (2017), for example, found that children with two ACEs were 3.4 times more likely to display externalizing behaviors that called for professional attention, relative to children with zero ACEs. Likewise, Evans and colleagues (2012) examined the mediating role of self-regulation in the link between ACEs and body mass index, finding that the relationship between ACEs and childhood obesity was mediated by the ability to delay gratification. Wolff and Baglivio (2017) also report a substantial portion of the effect of ACEs on juvenile re-offending operates indirectly through negative emotionality.
Studies also link individually measured ACEs with low self-control. Using data drawn from the Add Health study, Bunch et al. (2018) found a positive association between experiencing abuse as a child and reduced self-control. Other studies link family violence with greater impulsivity (e.g., Hallquist et al., 2015; Monahan, King, Shulman, Cauffman, & Chassin, 2015; Shin, McDonald, & Conley, 2018). More recently, Meldrum and colleagues (2018) reported that family alcohol use disorder was prospectively associated with low self-control among a high-risk sample of adolescents in the Michigan Longitudinal Study.
Possible Mechanisms Linking ACEs to Deficits in Self-Control
Research indicates that both ACEs and low self-control are associated with similar outcomes. Likewise, evidence, albeit indirect, points to the possible association between ACEs and deficits in self-control. Given these observations, more direct investigation into the association between ACEs and self-control is warranted. Equally important is the need to describe the possible mechanisms through which such an association might operate. In the following sections, we draw from both the social science and neuroscience literature to inform this discussion.
Social Mechanisms
ACEs could reduce self-control through several processes. One involves arguments directly made in self-control theory (Gottfredson & Hirschi, 1990). According to the theory, the primary cause of low self-control is ineffective parenting marked by deficits in attachment, rule-setting, supervision, and discipline. Certain ACEs could undermine these aspects of parenting. For example, parents with substance abuse problems might inadequately monitor their children, use discipline inconsistently, and have lower quality parent–child interactions (e.g., Dishion, Capaldi, & Yoerger, 1999; El-Sheikh & Flanagan, 2001). Similarly, family violence likely reduces family warmth (e.g., expressing love and affection and spending leisure time with one another) and also might be correlated with parents’ ineffective and harsh discipline (Chiesa et al., 2018). Parental marital discord, a common feature of divorced or separated families, is also linked to ineffective parenting (Chapple, 2003; Fauber, Forehand, Thomas, & Wierson, 1990). Effective parenting also may be undermined by parental incarceration (Turney & Goodsell, 2018) or parental mental illness, as parents become withdrawn, unpredictable, or self-preoccupied (Berg-Nielsen, Vikan, & Dahl, 2002; Duncan & Reder, 2000; Smith, 2004). In sum, several of the adverse experiences included in the ACEs index are linked to poor parenting practices that, in turn, may influence self-control.
Importantly, however, even when accounting for the correlation between ACEs and parental socialization, an effect of ACEs on self-control would persist if ACEs operate through other important mechanisms. One possibility is that ACEs encourage low self-control through social learning mechanisms such as imitation, modeling, and reinforcement (Akers, 1998). Although control perspectives tend to focus on aspects of parenting that are lacking (e.g., supervision and discipline), social learning approaches conceptualize parents as a key source of social learning that could influence self-control (Giordano, 2010). For example, many dynamics included in the ACEs index (e.g., family substance abuse, mental health problems, and violence) likely expose children to stressful circumstances in which family members model negative emotional reactions and unproductive and erratic methods of coping (e.g., yelling, destroying household items, and physical and verbal aggression). Over time, children may internalize related strategies of responding to stress and adversity and further solidify their own deficits in self-control. Through these social learning mechanisms, children exposed to ACEs may develop deficits in self-control because certain ACEs present them with role models who are low in self-control.
Another possibility is that the uncertain and unreliable attention to child needs that is implicit in many ACEs, especially physical and psychological neglect, leaves children less invested in exercising self-control toward the pursuit of long-term goals and needs. This possibility rests on the idea that uncertain and unreliable satisfaction of needs—which likely follows from the “chaotic home environments” that ACEs produce (Jones, Worthen, Sharp, & McLeod, 2018, p. 68)—leads children to discount the value of future rewards (because those rewards may seem unreachable). Under such circumstances, seizing upon immediate and more certain gratification may be more rewarding than exercising self-control. Indeed, this pattern has been observed in experimental research showing that children are less likely to delay gratification when confronted with unreliable circumstances (Kidd, Palmeri, & Aslin, 2013).
Brain-Based Mechanisms
There is also reason to suspect that ACEs might influence self-control by contributing to changes in the structure and functioning of brain regions known to govern self-control, particularly the prefrontal cortex (PFC; Barkley, 1997; Beaver, Wright, & DeLisi, 2007). This view is consistent with arguments from criminologists who conceptualize self-control as an executive function of the brain (e.g., Beaver et al., 2007; Cauffman, Steinberg, & Piquero, 2005; DeLisi, 2014; Jackson & Beaver, 2013), and many studies document the negative effects that trauma and toxic stress early in life have on the developing brain (e.g., Blair & Raver, 2012; Shonkoff et al., 2012; Teicher, Samson, Anderson, & Ohashi, 2016; Twardosz & Lutzker, 2010).
An exhaustive review of the literature linking childhood adversity with alterations in brain structure and functioning is beyond the scope of this study, but we can draw attention to studies that support the contention that such alterations might explain why ACEs are detrimental for self-control. For example, Tomoda and colleagues (2009) found that repeated exposure to harsh corporal punishment during childhood was associated with volumetric reductions in multiple regions of the PFC (see also Eiland & Romeo, 2013). Similar results were observed by Andersen and colleagues (2008) when focusing on the effects of childhood sexual abuse among a sample of females in early adulthood. More directly relevant to the current focus, research by Fava and colleagues (2019) found that experiencing more ACEs prior to age 11 was negatively associated with activity in the anterior cingulate cortex (ACC), a sub-region of the PFC known to govern executive functioning and self-regulation (e.g., Posner, Rothbart, Sheese, & Tang, 2007). Furthermore, Meldrum and colleagues (2018) reported that reduced ACC activity at age 12 was inversely associated with self-control measured approximately 1 year later.
This Study
Our review of prior theory and research makes evident there is good reason to believe that an association between ACEs and reduced self-control exists and that it could operate through a number of different mechanisms. Although previous studies offer some initial support for a link between ACEs and deficits in self-control, we will help to shed additional light on this association in two important ways. First, whereas prior research is often limited to a focus on certain dimensions of low self-control as outcomes of ACEs (i.e., Perez et al., 2018), or, alternatively, limited to a focus on individually measured ACEs as potential causes of poor self-control (e.g., Bunch et al., 2018; Meldrum et al., 2018), we examine the association between the 10-item ACEs inventory and measures of self-control that reflect the multiple dimensions emphasized by Gottfredson and Hirschi (e.g., the Grasmick, Tittle, Bursik, & Arneklev, 1993, scale). Second, we test the hypothesis of an inverse association between ACEs and self-control in two large, independent samples of youth that are different in terms of geographical location, risk profile, and demographics, enabling us to assess the robustness of the association between ACEs and self-control across different methodological specifications.
Method
Data
Data for this study are drawn from two sources. The first is data collected during the first wave of the Supporting Healthy Adolescent Relationships and Environments (SHARE) study, a Centers for Disease Control and Prevention-funded study of 1,236 adolescents that began in 2012. The SHARE study was conducted over four annual waves via an accelerated longitudinal design. Data were captured at Wave 1 relevant to neighborhood and family contexts, teen dating relationships, and, most relevant to the current focus, ACEs (retrospectively) and self-control. SHARE study participants were recruited from six school districts in the Detroit Metro area in southeast Michigan. The school districts were selected based on community risk factors developed from a composite rating of publicly available community data, including crime rates, poverty rates, minority composition, and percent rental properties. Two school districts were recruited across low-, medium-, and high-risk strata, totaling six districts. All middle and high schools in each of the six districts participated in the SHARE study, totaling 13 schools.
Within each participating school, youth were randomly selected using a stratified sampling procedure by grade level (sixth and ninth grades only) and gender; a passive parental consent procedure was employed. Prior to survey administration, all participants also provided oral or written assent, depending on age (assent was read aloud to those less than 13 years of age), and were informed of their right to withdraw from the study or skip questions at any time. The response rate across the 13 schools was 95%. Of the 1,236 adolescents who participated in the first wave of the SHARE study (the focus of our analysis), complete data for this study were available for 1,145 (93%) of the participants.
The second data source is derived from the Florida Department of Juvenile Justice’s (FDJJ) archival data records. FDJJ maintains a database on youths’ offending history and two risk assessment tools: The Residential Positive Achievement Change Tool (RPACT) and the Community Positive Achievement Change Tool (CPACT). The RPACT and CPACT evaluate risk and protective factors related to things such as family background, social relationships, and prosocial attitudes. Most relevant to our current focus, these tools enable the construction of measures of ACEs and self-control. Both the RPACT and CPACT are administered by FDJJ case managers, who conduct a semi-structured interview with youth, but also receive feedback from probation or residential staff who have worked with the youth in question. Official records also are used where possible to complete the assessments. The CPACT is administered to all youth upon first entering the system, so CPACT data are collected prior to any confinement. The RPACT, on the contrary, is administered only with youth who are placed in residential confinement; the first RPACT assessment occurs within 30 days of admission. Importantly, the administration of the CPACT occurs prior to the administration of the RPACT, which helps establish correct temporal ordering between ACEs and self-control, given that the CPACT is the basis for the ACEs index, whereas the RPACT is the basis for the measure of self-control.
We use these data for youth who completed a residential placement in a juvenile residential facility between July 1, 2010, and June 30, 2015. Although we began with 17,782 cases, 8,316 cases were excluded because they lacked necessary CPACT data to measure ACEs. This sometimes was because available CPACT data were insufficiently up to date (we excluded cases with CPACTs administered more than 60 days prior to the placement), but the most common exclusion stemmed from limiting the analysis to cases receiving the “full-screen” CPACT rather than the shorter “pre-screen” CPACT. 2 Second, to ensure that all youth appear only once in the dataset, 969 cases were excluded for youth who had experienced an earlier residential completion. Finally, 201 cases were excluded due to missing data on covariates, resulting in a final analytic sample of 8,296 cases of FDJJ youth placed into residential confinement. 3
Measures
Dependent Variable: Self-Control
For the Michigan sample, we measure self-control using the 24-item Grasmick et al. (1993) scale. Adolescents responded to each of the items with options ranging on a 4-point scale from strongly disagree (= 1) to strongly agree (= 4). The direction of the coding of the items was reversed so that higher scores indicate greater self-control. For the analyses, the 24 items were averaged together to form a global measure of self-control, a method supported by recent research (Ward, Nobles, & Fox, 2015). The internal consistency of the 24-item measure was in line with prior research (α = .86).
For the Florida sample, we measure self-control using three items from the RPACT, selected because they reflect the impulsivity, anger, and self-centeredness dimensions of low self-control emphasized by Gottfredson and Hirschi (1990). Unlike the self-reports of self-control in the Michigan sample, each of the three items in the Florida sample is based on responses provided by staff members who worked in the facility in which the youth was confined. The impulsivity item was measured on a 4-point scale based on the facility staff member’s perception of whether the youth is impulsive or acts before thinking: uses self-control, usually thinks before acting (= 1); some self-control, sometimes thinks before acting (= 2); impulsive, often acts before thinking (= 3); or highly impulsive, usually acts before thinking (= 4). The anger item was also measured on a 4-point scale based on the facility staff member’s perception of whether the youth has a poor tolerance for frustration: never gets upset over small things or has temper tantrums (= 1), rarely gets upset over small things or has temper tantrums (= 2), sometimes gets upset over small things or has temper tantrums (= 3), or often gets upset over small things or has temper tantrums (= 4). The self-centeredness item was measured on a 3-point scale based on the facility staff member’s perception of whether the youth has empathy, remorse, or sympathy for the victims of his or her delinquent behavior: has empathy for his or her victim(s) (= 1), has some empathy for his or her victim(s) (= 2), or does not have empathy for his or her victim(s) (= 3). Given that the response options for each of the three items were different, scores for each of the items were first standardized. Following this, the items were reverse-coded and averaged so that higher values for the three-item measure reflected greater self-control (α = .65; average inter-item correlation = .39). 4
Independent Variable: ACEs
Using the ACEs inventory developed by Felitti and colleagues (1998) as a guide, we created 10-item variety indices of ACEs for both the Michigan and Florida samples. These indices reflect a count of how many of the 10 different ACEs each youth experienced in his or her lifetime prior to data collection. For the Michigan sample, this information was based on self-reports, whereas for the Florida sample information was drawn from the CPACT semi-structured interviews. One difference between the Michigan and Florida items to note is that the “family violence” ACE in the Michigan data refers to having witnessed violence against a parent(s), whereas in the Florida data this item reflected witnessing violence against family members or having been physically hurt by a family member. The internal consistency of the 10-item ACEs index in the Michigan data was .82, whereas in the Florida data it was .60. For a complete listing of the items used to construct the variety indices in both the Michigan and Florida samples, see the Supplemental Appendices (available in the online version of this article).
Covariates
To better isolate the association between ACEs and self-control, and to guard against the potential that other factors might account for any association between the two constructs, we included a number of covariates in the multivariate models. In the Michigan sample, we included the following six covariates for the analysis: age, sex, race, effective parental socialization, family support, and neighborhood problems. Age was measured continuously to two decimal places based on self-reports of birth date and year. Sex and race were both coded dichotomously (male = 1, female = 0; White, non-Hispanic = 1, non-White = 0). Effective parental socialization was measured as an average of eight items (α = .81). Example items include “When I am not at home, one of my parents knows when I am and who I am with,” and “The rules in my family are clear.” For each of the items, response options were NO! (= 1), no (= 2), yes (= 3), and YES! (= 4). Family support was measured as an average of three items (α = .76). An example item is “There are people in my family I can talk to, who care about my feelings and what happens to me.” For each of the three items, response options were not at all (= 1), some (= 2), and a lot (= 3). Neighborhood problems were measured as an average of 17 items (α = .95). For each of the items, youth were asked, “Thinking about your neighborhood, how much of a problem is. . . .” Items included abandoned buildings, street gangs, and vandalism. For each item, response options were not a problem (= 1), sort of a problem (= 2), and a big problem (= 3). 5
For the Florida sample, the following six covariates were included in the analysis: age, sex, race, effective parental socialization, family support, and family income. Age was measured continuously and captures the youth’s age at admission to the FDJJ residential facility. Sex and race were measured dichotomously (male = 1, female = 0; White, non-Hispanic = 1, non-white = 0). Effective parental socialization was measured using four items reflecting parental: supervision, disapproval of antisocial behavior, consistency of punishment, and consistency of rewards. The four items were first standardized given differences in scaling and then averaged for the analysis (α = .75); higher scores represent more effective socialization practices. For detailed information on the wording of these items, see the Supplemental Appendices (available in the online version of this article). Family support was a single-item, ordinal measure created using two RPACT items: (a) whether a youth reported feeling close to either his or her parent (mother or father) and (b) whether a youth had parents who were consistently willing to support them. A score of 0 was assigned for the family support variable if youth said neither of these two aforementioned conditions applied to them, 1 if they affirmed one or the other, and 2 if they affirmed both. Family income was measured as an ordinal variable with values ranging from 1 to 4: less than US$15,000 (= 1), US$15,000 to US$34,999 (= 2), US$35,000 to US$49,999 (= 3), and ≥US$50,000 (= 4).
Analytic Plan
The analysis unfolded in three stages. First, we present and discuss descriptive statistics for each of the two samples of youth, drawing attention to differences between each with regard to ACEs and demographics. Second, we present parallel sets of ordinary least squares (OLS) regressions for each sample to test the hypothesis of an inverse association between ACEs and self-control. OLS regression was employed given that the values for self-control in each of the two samples approximated normal distributions (Michigan sample: skew = −0.04, kurtosis = 3.75; Florida sample: skew = 0.07, kurtosis = 2.59). 6 Third, we present the results of exploratory analyses to investigate the possibility that certain types of ACEs are more strongly associated with variation in self-control than others. Specifically, we consider whether ACEs related to maltreatment exert a stronger effect on self-control than ACEs related to household dysfunction. Although not the primary focus of the study, these exploratory models add important nuance that merits attention given the paucity of research investigating the association between ACEs and self-control. 7
Results
Bivariate Statistics
Table 1 presents descriptive statistics for the sample of youth from Michigan (Panel A) and the sample of youth from Florida (Panel B); correlation matrices for each sample can be found in the Supplemental Appendices (available in the online version of this article). Given the measure of self-control in each sample is based on different items with different response options, we do not make a direct comparison of the mean values for self-control between the two samples. Comparisons can be made, however, with regard to ACEs and demographics. First, the mean value for ACEs among the youth in the Michigan sample of 2.22 is lower than the mean value of 3.40 among youth in the Florida sample (t = −19.10, p < .001). The higher mean value in the Florida sample of youth makes intuitive sense given (a) the higher-risk nature of this sample and (b) the mean age for the Florida sample of 16.39 is greater than the Michigan sample of 13.65 (t = 65.77, p < .001); the Florida sample of youth has had more time to experience ACEs. The two samples also are different with regard to sex and race composition. Specifically, the Florida sample of youth is predominately male (87.1%), whereas the Michigan sample of youth is much more balanced (47.8% male). In addition, the majority of the Michigan sample of youth is White (61.1%), whereas approximately one-third of the Florida sample of youth is White (35.1%). 8
Descriptive Statistics
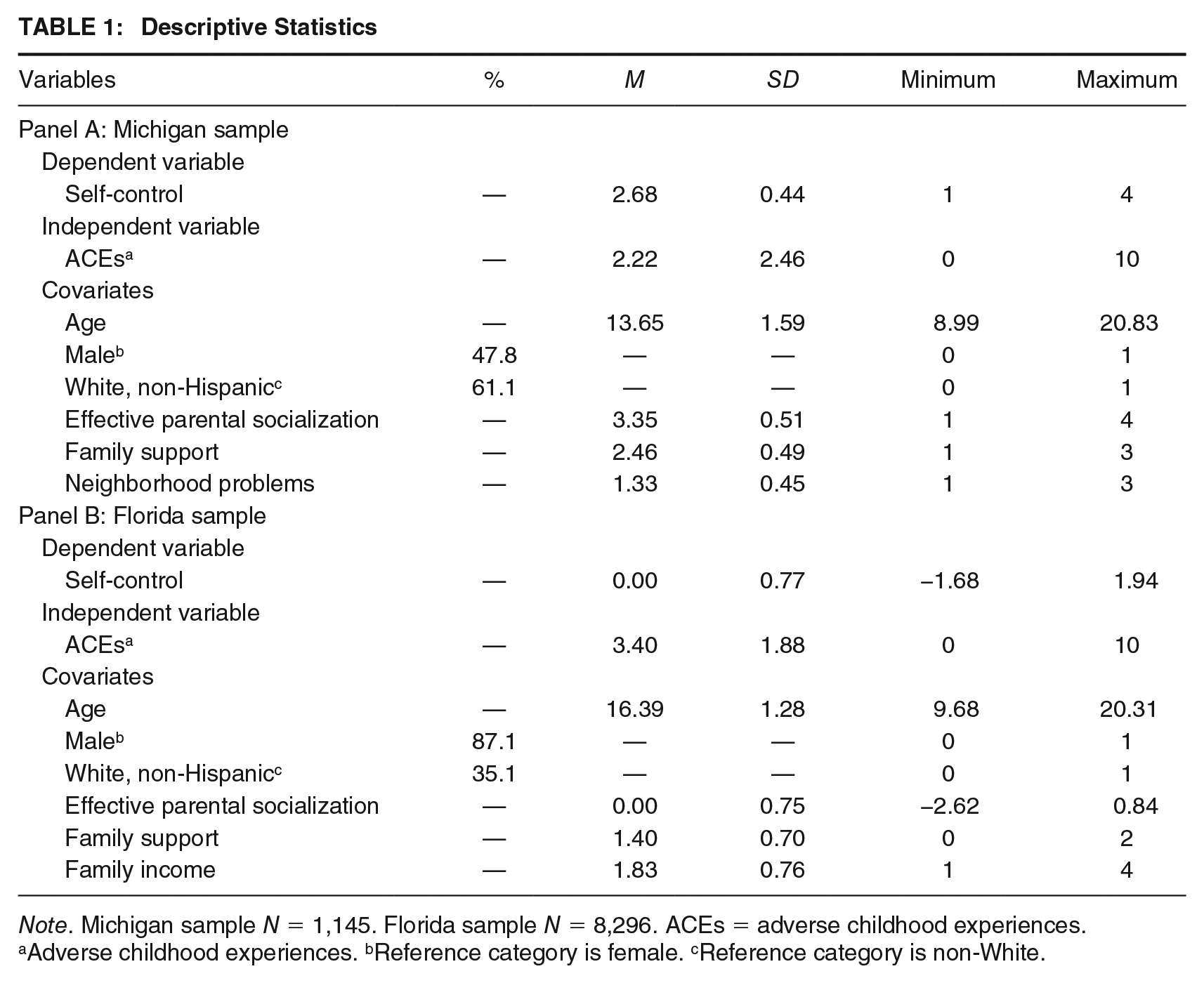
Note. Michigan sample N = 1,145. Florida sample N = 8,296. ACEs = adverse childhood experiences.
Adverse childhood experiences. bReference category is female. cReference category is non-White.
Regression Models
We then turned attention to testing our primary hypothesis that youth who experience a greater variety of ACEs will score lower in self-control. Panel A of Table 2 presents the results of two OLS regressions estimated for the Michigan sample of youth. In Model 1, a bivariate regression is estimated, revealing a negative, statistically significant association between ACEs and self-control. Described in terms of standardized effects, a one standard deviation (SD) increase in ACEs is associated with a 0.26 SD decrease in self-control. As indicated by the adjusted R2 value, the measure of ACEs accounts for 7% of the variation in self-control.
OLS Regressions of Self-Control
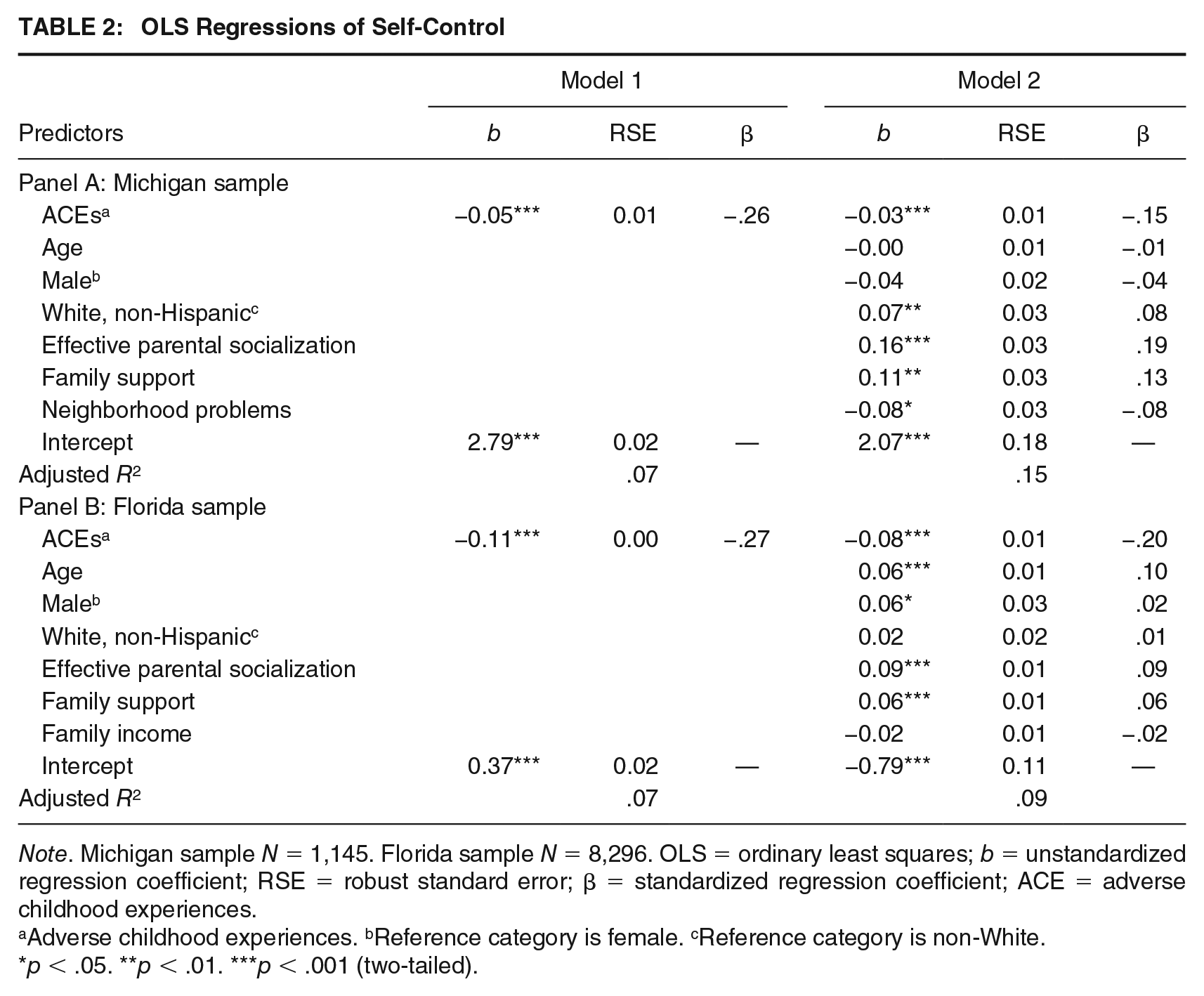
Note. Michigan sample N = 1,145. Florida sample N = 8,296. OLS = ordinary least squares; b = unstandardized regression coefficient; RSE = robust standard error; β = standardized regression coefficient; ACE = adverse childhood experiences.
Adverse childhood experiences. bReference category is female. cReference category is non-White.
p < .05. **p < .01. ***p < .001 (two-tailed).
Model 2 adds the covariates. As shown, a negative, statistically significant association between ACEs and self-control remains, though the magnitude of the effect is attenuated by approximately 40% (b = −0.03, p < .001, β = −.15). Model 2 also indicates that Whites have higher self-control (β = .08). Furthermore, youth reporting more effective parental socialization (β = .19) and greater family support (β = .13) have higher self-control, whereas living in a neighborhood with greater problems is negatively associated with self-control (β = −.08). The addition of the covariates to Model 2 more than doubles the amount of variation in self-control accounted for relative to Model 1 (15% in Model 2 relative to 7% in Model 1).
Panel B of Table 2 presents the results of two OLS regressions for the Florida sample of youth. In Model 1, the bivariate regression reveals a negative, statistically significant association between ACEs and self-control (β = −.27). As indicated by the adjusted R2 value, the ACEs measure accounts for 7% of the variation in self-control. Model 2 adds the covariates. As shown, the association between ACEs and self-control remains when accounting for the covariates (b = −0.08, p < .001, β = −.20). Model 2 also indicates that older youth (β = .10) and males (β = .02) are higher in self-control, though the magnitude of the latter effect is very small. Furthermore, youth in the Florida sample reporting more effective parental socialization and greater family support have higher self-control (β = .09 and .06, respectively). The addition of the covariates to Model 2 increases the amount of variation in self-control accounted for relative to Model 1 (9% in Model 2; 7% in Model 1). 9
Exploratory Analyses
Results from both the Michigan and Florida samples support the hypothesis that experiencing a greater variety of ACEs is inversely associated with self-control. Given this, we explored the potential that some ACEs could be more strongly associated with variation in self-control than others. Specifically, in considering the 10 different ACEs, a distinction appears evident when contrasting ACEs reflecting abuse, neglect, and family violence against ACEs concerning family substance abuse, family incarceration, family mental illness, and parental separation. Specifically, the former set of ACEs relates to some form of interpersonal maltreatment having occurred that youth either experienced or were aware of (perhaps witnessing). In contrast, the latter set of ACEs captures aspects of general household dysfunction.
It is possible that ACEs reflecting maltreatment could have a greater impact on self-control than those pertaining to household dysfunction given that the former may pose a more immediate threat to a child’s physical and psychological well-being. To explore this potential, we disaggregated the 10-item ACEs index into a six-item maltreatment ACEs measure and a four-item household dysfunction ACEs measure. Panel A of Table 3 presents results for the Michigan sample of youth using these two measures in place of the full ACEs measure. Model 1 presents the results using the maltreatment ACEs measure as the primary predictor variable, whereas Model 2 presents the results using the household dysfunction ACEs measure. As shown, there is a stronger association between maltreatment ACEs and self-control (Model 1: b = −0.05, p < .001, β = −.17) than between household dysfunction ACEs and self-control (Model 2: b = −0.03, p = .022, β = −.07); the difference in the magnitude of effect sizes is greater than a factor of two.
Effect of Maltreatment Versus Household Dysfunction ACEs on Self-Control
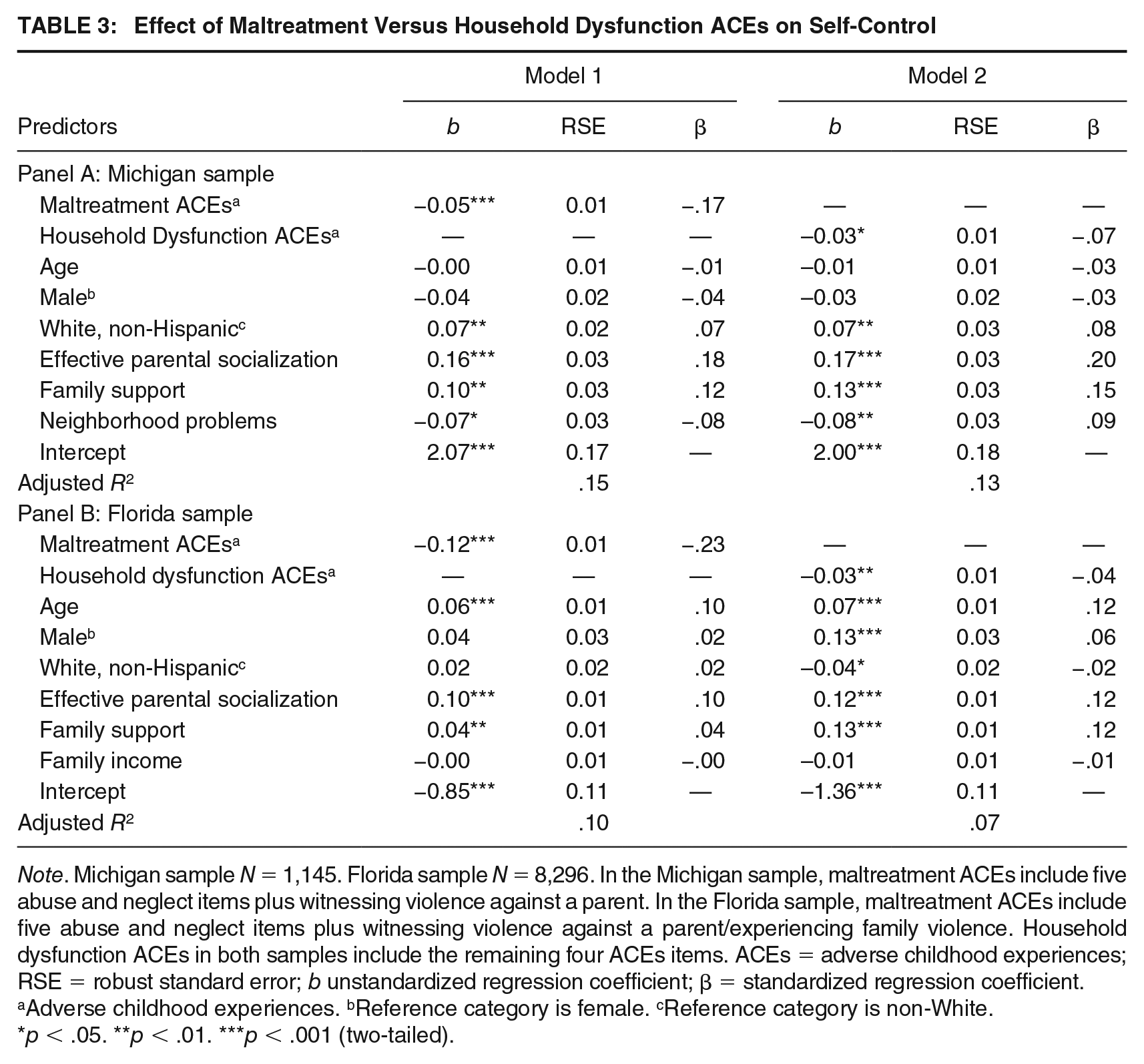
Note. Michigan sample N = 1,145. Florida sample N = 8,296. In the Michigan sample, maltreatment ACEs include five abuse and neglect items plus witnessing violence against a parent. In the Florida sample, maltreatment ACEs include five abuse and neglect items plus witnessing violence against a parent/experiencing family violence. Household dysfunction ACEs in both samples include the remaining four ACEs items. ACEs = adverse childhood experiences; RSE = robust standard error; b unstandardized regression coefficient; β = standardized regression coefficient.
Adverse childhood experiences. bReference category is female. cReference category is non-White.
p < .05. **p < .01. ***p < .001 (two-tailed).
Panel B of Table 3 presents results pertaining to the Florida sample of youth. Once again, Model 1 presents results using the maltreatment ACEs measure as the primary predictor variable, whereas Model 2 presents the results using the household dysfunction ACEs measure. As indicated, a stronger association is again observed between maltreatment ACEs and self-control (Model 1: b = −0.12, p < .001, β = −.23) than between household dysfunction ACEs and self-control (Model 2: b = −0.03, p = .002, β = −.04); the difference in the magnitude of effect sizes is greater than a factor of five. Thus, in both samples, we find evidence that maltreatment ACEs are more strongly associated with self-control than household dysfunction ACEs. 10
Discussion
In the quest to identify the causes of delinquency and crime, low self-control has emerged as one of the strongest predictors (Pratt & Cullen, 2000; Vazsonyi et al., 2017). Naturally, this has led to considerable interest in the etiology of self-control. In this study, we have provided evidence that cumulative childhood adversity, in the form of ACEs, may play an important role in contributing to deficits in self-control. In this final section, we draw attention to the key findings, noting their implications for both theory and policy. Following this, we describe the strengths and limitations of this study and highlight important directions for future research.
The primary finding of this study is that experiencing a greater variety of ACEs is inversely associated with self-control, a pattern we observed in two large, independent samples of youth that are very different from one another with regard to demographic makeup, risk profile, measurement of self-control, and reporting source. This finding is consistent with recent work linking ACEs to certain dimensions of self-control (i.e., impulsivity, Perez et al., 2018) and constructs akin to reduced self-control (i.e., lack of future orientation, Craig, 2019; poor delay of gratification, Evans et al., 2012), as well as work linking individually measured ACEs to deficits in self-control (e.g., Bunch et al., 2018; Hallquist et al., 2015). The second finding of this study is that maltreatment ACEs are more strongly associated with deficits in self-control than household dysfunction ACEs, a pattern observed in each of the two samples analyzed. Although our consideration of this issue was exploratory, it nonetheless adds importance nuance to our understanding of the nature of the association between ACEs and self-control, which is important given how little attention has been directed at this issue in the criminological literature.
In considering the importance of these findings, at least two observations merit attention. First, although there were differences in the two samples with regard to the measurement of self-control and demographic characteristics, we observed a negative association between ACEs and self-control in each sample, particularly when the focus was maltreatment ACEs. This suggests that the influence of ACEs on self-control may apply to a wide range of adolescents, though replication of our findings is warranted. Second, the magnitude of the association between the full ACEs measure and self-control was comparable with that of the association between the parenting/family variables and self-control in the Michigan sample (and exceeded the association in the Florida sample). This finding is inconsistent with theoretical arguments made by Gottfredson and Hirschi (1990), yet fits with a growing body of research identifying factors other than parenting that impacts self-control (e.g., Beaver et al., 2007; Burt et al., 2006; Meldrum et al., 2012).
The finding that ACEs reduce self-control also has important policy implications. Most notably, it reveals a daunting pattern in which these two consequential risk factors often co-occur. This gives priority to identifying and expanding evidence-based programs that can prevent them both. Early prevention efforts with at-risk families are promising in this regard—these programs are emphasized in the dialogue on prevention for both ACEs (Fortson, Klevens, Merrick, Gilbert, & Alexander, 2016) and low self-control (Hay & Meldrum, 2016). Illustrative programs include nurse–family partnerships (Olds et al., 2007), which are used in the prenatal period to prevent an array of problems—ACEs and child self-control deficits included—that can follow from struggles experienced by new parents. Similarly, Triple P—the Positive Parenting Program—is a cognitive behavioral therapy that helps parents constructively interpret and manage stressors and complications that commonly emerge in family life (Sanders & Mazzucchelli, 2013). This helps to build the habits and skills parents need to keep their lives on track, potentially reducing a wide variety of ACEs. In the process, this can also prevent problems with self-control.
Beyond prevention, policy efforts also must confront instances where ACEs have already occurred and produced harmful consequences for children. Early identification is critical, and this calls for expanded ACEs screening in schools, medical practices, and juvenile justice and social welfare agencies (McKelvey, Whiteside-Mansell, Conners-Burrow, Swindle, & Fitzgerald, 2016). Once such cases are identified, the programs most likely to be effective are cognitive behavioral interventions that not only reduce the occurrence of future ACEs in the household but also address trauma already experienced (Cohen & Mannarino, 2008; Saywitz, Mannarino, Berliner, & Cohen, 2000). As Finkelhor (2018) emphasizes, the challenges here are notable—much is unknown about what treatments should be triggered by different varieties and combinations of ACEs. Moreover, because the effects of ACEs on low self-control have been minimally studied, there has been little recognition of a key treatment implication following from the results presented here. Most notably, youth high in ACEs will enter treatment not just with heightened levels of such things as depression or anxiety but also perhaps with notable deficits in self-control. Successful intervention requires that this pattern receive attention in treatment efforts.
Strengths and Limitations
The findings of this study are noteworthy given they were observed in two independent samples of youth that are geographically and demographically diverse. Furthermore, for the Florida sample in particular, the fact that the measures of ACEs and self-control were drawn from different reporting sources reduces concerns that the finding is a result of shared method variance. Despite such strengths, there are limitations of the study that should be acknowledged. First, as is the case with much criminological research, the study was observational. Although we took steps to include important covariates in the analyses, particularly parenting-related variables and socioeconomic variables, the possibility exists for unmeasured sources of confounding. More robust measures of socioeconomic status, such as parental education, could attenuate the observed association between ACEs and self-control, as could indicators of parental self-control. Furthermore, there is the potential that heritability, something which could not be accounted for in this study, could also account for a portion of the observed association between ACEs and self-control, as recent work indicates accounting for genetic confounding attenuates the association between childhood adversity and delinquency (Connolly & Kavish, 2019). Future research should therefore attempt to replicate our findings when utilizing samples of siblings or twins that can aid in better ruling out genetic confounds.
Additional limitations merit discussion. First, the internal consistency of the ACEs measure for the Florida sample was lower than desired. Yet, it is worth emphasizing that it correlated with self-control and several of the covariates in ways that would be expected. Second, for both samples a retrospective research design was employed, whereby ACEs were measured based on self-reports of past experiences and self-control was measured using contemporaneous reports. This raises questions about the timing of the different ACEs, and it is possible that more recent ACEs could be more strongly associated with self-control. The stress literature generally indicates that recent stresses are more consequential for well-being (Dunn et al., 2018). Thus, replicating this study using a prospective research design would enable such a consideration. Third, the dichotomous measurement of each ACE, particularly those pertaining to abuse, neglect, and family violence, fails to take into account the frequency or severity of these ACEs. Participants who might have experienced repeated instances of abuse, neglect, and family violence were treated, for analytical purposes, the same as participants who only experienced these ACEs in a single instance. To the extent that the frequency of these ACEs is more consequential for self-control than just mere prevalence, our findings may underestimate the magnitude of the association between ACEs and self-control. Given this, future research might consider measuring the frequency or severity of different ACEs.
We should also point out that neither of the samples analyzed is nationally representative, and replication of our findings using samples of youth that better reflect the demographic profile of youth at a national level is warranted. Furthermore, the measures of self-control employed in the study, although consistent with Gottfredson and Hirschi’s (1990) conceptualization of self-control, are not without flaws. This is particularly true of the more limited three-item measure of self-control used for the Florida sample of youth. Along this line of thought, future research might consider examining the association between ACEs and self-control using alternative operationalizations, such as that provided by the Tangney, Baumeister, and Boone (2004) brief self-control scale.
A final limitation is that we did not test for mediating mechanisms between ACEs and self-control. As we discussed earlier, many such mechanisms may be relevant, and this possibility is consistent with previous research indicating the complex etiology of self-control (Hay, 2001; Jackson & Beaver, 2013). As one example, a recent study reported that ACEs are negatively associated with ACC activity (Fava et al., 2019), and another reported that reduced ACC activity is negatively associated with self-control (Meldrum et al., 2018). In combination, these two studies point to the possibility that ACC activity could mediate the association between ACEs and deficits in self-control. Future research that explicitly tests for such mediation, however, is needed, not only for assessing variation in ACC activity as a potential mediating mechanism but also the potential social mechanisms described earlier in the article.
Directions for Future Research
We see several directions for future research on the association between ACEs and self-control in addition to those implied in our discussion of limitations. First, given that we only evaluated this association when measuring self-control at a single point in time, it would be informative to assess whether ACEs are related to trajectories of self-control. Likewise, investigating how exposure to ACEs across time shapes the development of self-control is an equally important consideration. Second, it will be useful to examine whether the association between ACEs and self-control is conditioned by other factors. For example, the effect of ACEs on self-control might be gendered. Effects may also vary according to other risk and protective factors that could amplify or diminish the association. Third, given the known consequences of deficits in self-control, particularly involvement in delinquency and crime, future research should investigate the extent to which variation in self-control mediates the association between ACEs and delinquency/crime (Wolff & Baglivio, 2017).
Conclusion
Studies on the causes of self-control (e.g., Jackson & Beaver, 2013; Meldrum et al., 2012) have advanced well beyond a focus on parenting practices emphasized by Gottfredson and Hirschi (1990). Likewise, research into the consequences of ACEs has extended outside of initial foci on health-related behaviors. In this article, we argued that a marriage of these two literature is warranted. In support of this, analysis of data from two separate samples indicated that exposure to ACEs is associated with reduced self-control. We view our effort, however, as merely a first step. Important avenues for future research remain in light of alternative approaches to sampling and measurement that could be employed. Such efforts could shine greater light on how early adversity harms child and adolescent development, including the development of self-control. Such research ultimately may help promote healthy physical, social, and cognitive development.
Supplemental Material
Online_Supplementary_Appendix_A – Supplemental material for Are Adverse Childhood Experiences Associated With Deficits in Self-Control? A Test Among Two Independent Samples of Youth
Supplemental material, Online_Supplementary_Appendix_A for Are Adverse Childhood Experiences Associated With Deficits in Self-Control? A Test Among Two Independent Samples of Youth by Ryan C. Meldrum, Brae Campion Young, Sadhika Soor, Carter Hay, Jennifer E. Copp, Madison Trace, Joanne P. Smith-Darden and Poco D. Kernsmith in Criminal Justice and Behavior
Footnotes
Authors’ Note:
This research is partially supported by a grant from the Centers for Disease Control and Prevention (Grant Number U01-CE002115). Opinions expressed are those of the authors and do not represent the position of the CDCP or the Florida Department of Juvenile Justice.
Supplemental Material
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.