
Abstract
A growing body of research supports the use of mindfulness-based interventions (MBIs) in incarcerated populations; however, treatment effectiveness remains unclear. This meta-analysis of 22 studies (N = 2,265, 75% male) quantified the effectiveness of MBIs in incarcerated populations on key psychological outcomes and criminogenic needs. Results from pre–post studies indicated MBIs had a small to moderate effect on all outcomes, but this was not supported by controlled studies. Studies with older participants, more females, and longer treatment length demonstrated slightly greater effects. Results from pre–post analyses demonstrated significant reductions in psychological outcomes (depression, anxiety, and stress) and criminogenic needs (impulsivity, self-dysregulation, anger, substance use behavior, and attitude). However, only depression and anxiety were significantly reduced in controlled studies. Although findings offer preliminary support of the efficacy of MBIs in targeting psychological health in incarcerated populations, further controlled studies are required to examine criminogenic outcomes and recidivism rates after treatment.
Introduction
Background
Incarcerated youth and adults experience significant psychological difficulties, including higher levels of stress, anxiety, and depression compared with the general population (Diamond et al., 2001; Johnson & Zlotnick, 2012; Trestman et al., 2007). Approximately two out of three incarcerated individuals meet the criteria for a psychiatric diagnosis in both adult and adolescent populations (Teplin et al., 2002; Trestman et al., 2007). Although mental health problems are considered the most significant cause of mortality in prison, they remain undertreated (Birmingham, 2003). Furthermore, the social and health costs of incarcerated populations include high rates of recidivism (e.g., Freudenberg et al., 2008), suicide (e.g., Abram et al., 2008), violence (e.g., Binswanger et al., 2007), and substance abuse (e.g., Abram et al., 2008).
An expanding body of research has established dynamic psychological risk factors that predict criminal behavior. Dynamic psychological risk factors are potentially changeable compared with static risk factors, which are fixed, such as age, ethnicity, or gender. Thus, dynamic risk factors serve as appropriate targets for intervention and are considered “criminogenic needs” (Andrews & Bonta, 2014). These well-established risk factors include, but are not limited to, deficits in impulsivity, anger, substance misuse, and self-regulation (Andrews & Bonta, 2014; Dafoe & Stermac, 2013; Gottfredson & Hirschi, 1990; Hanson, 2009). Evidently, larger social determinants of health need to be addressed to prevent youth and adult offending and reoffending; nevertheless, group- and individual-level interventions are necessary to assist those currently incarcerated (Simpson et al., 2018).
In response to the concerns outlined above, numerous mindfulness-based interventions (MBIs) intended for the general population have been adapted for both adult and youth incarcerated populations to support their mental health and reduce their recidivism rates (e.g., Himelstein et al., 2015; Samuelson et al., 2007; Suarez et al., 2014). However, the effectiveness of MBIs remains unclear and has yet to be quantified. In addition, there is little evidence examining whether trial characteristics (e.g., pre–post or control), program characteristics (e.g., type of intervention, length of treatment or study quality), and participant characteristics (e.g., gender or age) can affect the usefulness of and incarcerated individuals’ response to MBIs. An examination of these potential contributing factors is required to support prison staff in providing MBIs that are targeted and effective at meeting the behavioral needs and mental health of incarcerated populations, as well as potentially reducing their recidivism rates.
MBIs and Incarcerated Populations
Within the context of Western science, mindfulness has been operationalized as deliberate, nonjudgmental awareness of the present moment (Kabat-Zinn, 2003). Mindfulness can be described as a trait, state, and process, and has been found to be a successful intervention in both clinical and nonclinical populations (Khoury, Lecomte, Fortin, et al., 2013; Vago & David, 2012). Mindfulness-based techniques have also been incorporated into intervention programs, such as mindfulness-based stress reduction (MBSR; Kabat-Zinn, 1990), mindfulness-based cognitive therapy (MBCT; Teasdale et al., 2000), and mindfulness-based relapse prevention (MBRP; Bowen et al., 2014). Both historical and recent models of mindfulness aim to enhance positive emotions and reduce suffering (Bishop et al., 2004; Teasdale et al., 1995).
The positive impacts of MBIs for those experiencing mental and/or physical ailments are well documented (Allen et al., 2006; Bishop et al., 2004; Khoury, Lecomte, Fortin, et al., 2013). For instance, MBIs have been found to be helpful in the treatment of major depressive disorder (Piet & Hougaard, 2011; Segal et al., 2010), anxiety disorders (Grossman et al., 2004), bipolar disorder (Chiesa & Serretti, 2011), and substance use disorders (Bowen et al., 2006; Zgierska et al., 2009). Additional benefits of mindfulness include reducing risky behavior, as well as improving emotion regulation and overall well-being, and, therefore, may be particularly useful for incarcerated individuals (Baer, 2003; Chiesa & Serretti, 2009; Luberto et al., 2014).
In the past two decades, many studies have evaluated the utility of mindfulness-based programs in prison settings, supporting the potential efficacy of these interventions for people in custody with a range of psychological and behavioral outcomes (see Shonin et al., 2013, for review). The literature provides compelling evidence that mindfulness training may offer a healthy coping mechanism for incarcerated populations allowing them to better manage the stressful environment of prison life. MBIs have demonstrated efficacy in targeting and treating criminogenic needs, such as self-regulation and negative affect (Dafoe & Stermac, 2013). In a paper by Howells and colleagues (2010), mindfulness training was suggested as a beneficial tool for reducing the risk of recidivism as mindfulness targets key criminogenic needs such as poor affective self-regulation, anger control, and impulsivity (Day, 2009; Wright et al., 2009). Similarly, MBIs have contributed to significant improvements in hostility, self-esteem, and mood disturbance in people in custody, as they are able to gain new strategies for managing their negative emotions (Samuelson et al., 2007). MBIs and other Buddhist-derived interventions have been shown to have positive effects on psychological well-being, quality of life, and substance abuse rates in incarcerated populations (Auty et al., 2017; Dafoe & Stermac, 2013; Himelstein, 2011a). It is important to note that these studies are not without limitations (see Shonin et al., 2013, for review). Sample sizes were consistently small with attrition being a frequent problem in this population. In addition, these studies tended not to randomly assign participants to research conditions and some were not controlled (Himelstein, 2011a).
Intervention Characteristics
With an increasing number of studies examining the impacts of different types of MBIs in incarcerated settings, researchers have begun to investigate the pooled impact of MBIs on mental health and well-being outcomes in correctional settings (Auty et al., 2017; Dafoe & Stermac, 2013; Day, 2009; Lyons & Cantrell, 2016; Shonin et al., 2013; Witharana & Adshead, 2013). However, there has yet to be a published meta-analysis examining the quantifiable effects of MBIs in this population. In addition, previous reviews have focused on other Buddhist practices such as meditation and yoga programs, or provided narrative reviews (Auty et al., 2017; Himelstein, 2011a; Shonin et al., 2013). As such, it is important to investigate whether different types of MBIs have differential effects on incarcerated populations.
Individual Differences
The developmental contemplative science (DCS) framework suggests that the effectiveness of mindfulness programs and reaction to mindfulness training will change across developmental periods (Roeser & Pinela, 2014). As such, it is reasonable to assume that this framework may hold in the correctional context when examining the effectiveness of mindfulness training in incarcerated adults compared with adolescents; however, to our knowledge, no existing research has examined the influence of age on the effectiveness of mindfulness training in incarcerated populations. An examination of chronological age in incarcerated settings is warranted to determine whether this factor affects response to mindfulness training. In addition to the potential influence of age on MBIs in incarcerated settings, there is limited understanding of whether gender affects the effectiveness of mindfulness programs for incarcerated individuals. An investigation of potential gender differences in the efficacy of MBIs in incarceration settings would inform both researchers and practitioners on the appropriateness of mindfulness training for males and females in custody.
Objectives
A comprehensive meta-analysis was conducted to elucidate the effects of MBIs on certain criminogenic needs and psychological outcomes in incarcerated populations, as well as enhance our current understanding of how MBIs may confer their benefits upon incarcerated persons. The first objective of this meta-analysis was to quantify the influence of MBIs on psychological outcomes (depression, anxiety, and stress) and key criminogenic needs (anger, self-regulation, impulsivity, substance use behavior, and attitude toward substance use) for people in custody. In accordance with Borenstein et al. (2011), multiple outcomes were grouped into broad outcomes for our meta-analysis. Thus, our outcome groups of criminogenic needs and psychological outcomes are based on previous literature. Our second objective was to investigate the process outcome of trait mindfulness. The final objective was to explore the impact of intervention type and examine moderator variables (age, study quality, length of treatment, and proportion of females). The current meta-analysis will provide pertinent information on the role of intervention characteristics and individual differences in the effectiveness of MBIs in incarcerated settings.
Method
Eligibility Criteria
Pre–post and control studies were eligible for inclusion in the review if (a) mindfulness-meditation was the primary intervention and (b) the population was in a jail, prison, or an inpatient correctional facility setting. Studies were excluded if (a) they did not evaluate the intervention or implemented a qualitative design, (b) mindfulness was not the primary treatment (e.g., dialectical behavioral therapy, acceptance and commitment therapy) or meditation was the only intervention, (c) data were insufficient to compute an effect size, (d) they were published in a format other than a peer-reviewed journal article or dissertation, (e) the reported data overlapped with existing data already included in the analyses, or (f) the article was published in a language other than English or French. This meta-analysis was registered on PROSPERO (CRD42019125210).
Search Strategy
Electronic databases (PsycINFO, PubMed, MEDLINE, ProQuest Dissertations, and Theses Global) were searched from the first available date until March 19, 2019. We used the following search terms: (mindful* or stress reduction or MBCT or MBSR or mindfulness-based cognitive therapy or mindfulness-based relapse prevention or MBRP) AND (incarcerat* or prison* or inmate* or offender*). The search was limited to abstract and title for PubMed, ProQuest Dissertations, and Theses Global. PsycINFO and MEDLINE searches were limited to title, abstract, and subject heading. Reference sections of the included papers and review articles were also manually examined to obtain additional articles, which were accessed through Google Scholar.
Study Selection
Duplicates were removed using Endnote X8.2 and exported to Rayyan, an online screening tool (Ouzzani et al., 2016). A nonblinded, standardized protocol was used to determine inclusion eligibility using the aforementioned criteria by the first (M.P.) and second (C.S.) authors. M.P. and C.S. separately assessed 10% of the same articles following duplication removal (k = 26) and compared reasons for inclusion and exclusion criteria. An interrater agreement of 96% was achieved initially. After discussing their rationale for inclusion or exclusion, consensus was reached through discussion. Thereafter, M.P. and C.S. independently assessed half of the remaining articles. Any disagreements between reviewers about whether a study should be included were resolved through consultation with the last author, B.K. Two authors of the original studies were contacted to request missing data to compute effect sizes. Both authors responded, and their studies were included. The selection process is outlined in Figure 1. The following information was extracted from each included article: (a) trial characteristics (including the year of publication, pre–post or control trial, randomization, outcome measures, study quality, and qualifications of therapist), (b) intervention characteristics (including group or individual, treatment length, treatment type, and treatment homework), (c) participant characteristics (including target population, M age, percentage of females participants, and attrition rate).

PRISMA Flow Diagram of Search Results and Publication Exclusion Process
Synthesis of Results
The meta-analysis was performed by computing standardized differences in means. All analyses were conducted with Comprehensive Meta-Analysis, Version 3.070 (Borenstein et al., 2014). Effect sizes were computed using means and standard deviations when available. For the studies in which means and standard deviations were not available, other statistics were included (e.g., t). If correlations between pre- and postintervention measures were unavailable, the conservative estimate of r = .7 was used (Rosenthal, 1991). Hedges’s g was used to measure the effect size for all studies for discreet data (noncontinuous measures, such as number of events). We calculated effect sizes using odds ratios (ORs) for discreet data (e.g., noncontinuous variable) such as number of events (used also in suicide, hospitalization, and recidivism) and reported them separately. In addition, 95% confidence intervals (95% CIs), and the associated z and p values were calculated for each study. To calculate the mean effect size for groups of studies, a random effects model was used as it is more conservative and resilient to heterogeneity (Khoury, Lecomte, Fortin, et al., 2013). Heterogeneity among studies was systematically assessed using I2, which measures the portion of the total observed dispersion not affected by low statistical power and the chi-square statistic (Q). To interpret the I2 values, 25% may be considered low, 50% moderate, and 75% may be considered high (Higgins et al., 2003).
Risk of Bias Across and Within Studies
A fail-safe N (Orwin, 1983) and funnel plot were computed to assess publication bias for across studies. These analyses provide information regarding the number of studies needed to invalidate findings. For risk of bias within studies, controlled studies were assessed using the Cochrane tool as reported in the Cochrane Collaboration handbook (Higgins et al., 2011). This tool enables researchers to assign a quality score of high, low, or unclear risk based on seven factors that might cause the effect of treatment in individual studies to be over- or underestimated. Risk of bias was assessed in the following domains: (a) selection bias (e.g., random sequence generation and allocation concealment), (b) detection bias (e.g., blinding of outcome assessment), (c) performance bias (e.g., blinding of participants), (d) attrition bias (e.g., incomplete outcome data), (e) reporting bias (e.g., selective reporting), and (f) other biases. Risk of bias assessment was carried out independently by the first (M.P.) and second (C.S.) authors on controlled studies and any disagreements were resolved through discussion.
Outcome Measures
The primary outcome measures were three psychological outcomes: stress, depression, and anxiety. The following criminogenic needs were also examined: impulsivity, anger, self-regulation, substance use behavior, and attitude toward substance use. Finally, we investigated the process outcome of trait mindfulness.
Additional Analyses
Subgroup analyses were conducted to compare the mean effect sizes of the different MBIs (e.g., MBRP vs. MBSR-modified). Comparisons were made using a z test and a pooled estimate of I2. Meta-regression analyses were conducted with the goal of investigating how outcomes were affected by the following potential moderators: specifically, participants’ mean age, session length, the proportion of females in the studies’ samples, and study quality.
Results
Study Selection
Three hundred eighty-eight articles were retrieved from the initial search on March 19, 2019. Removal of duplicates resulted in 258 articles. The first and second authors carefully screened the identified publications through the title and/or abstract and applied the exclusion criteria. The full text of the potentially eligible studies was independently assessed for eligibility by the first and second author. Discrepancies were resolved through discussion between reviewers. A total of 21 studies (19 different articles with two including two different studies each with distinct participant samples) met the eligibility criteria. An additional study was identified through an article’s reference list. Data collected from three of the studies were reported in more than one article (e.g., a thesis and a published article). Data were extracted from all these articles as they reported complementary data (An et al., 2019; Himelstein, 2010; Himelstein et al., 2012; Leonard et al., 2013; Umbach et al., 2018; Xu et al., 2016). A detailed illustration of the study selection process is portrayed in Figure 1.
Study Characteristics
The total number of participants included in the meta-analysis was 2,265. Half of the studies focused on youth in incarcerated settings (k = 11; Mage = 16.955 years) and the remaining half on adults (k = 11; Mage = 36.652 years). Sixteen out of the 22 studies (73%) focused solely on incarcerated males, and five studies (23%) exclusively targeted individuals with a history of substance abuse. Intervention was most commonly delivered by trained professionals (k = 12; e.g., MBSR instructor), followed by students (k = 2; e.g., clinical doctoral student), and through electronics (k = 1). Seven studies did not specify the training of the facilitator. Fourteen of the included studies (64%) used a pre–post design, whereas the remaining eight (36%) used a controlled design. Of the controlled studies, half of the studies compared treatment with wait-list or treatment as usual, and the remaining half used an active control group. One study used a quasi-wait-list control, but their control group was not included as there were insufficient data to compute effect size (Samuelson et al., 2007).
A wide range of MBIs were used. Interventions consisted of modified versions of MBSR (MBSR-modified; k = 4), which is a well-established treatment that broadly consists of training in formal mindfulness practices such as body scans and sitting meditation (Kabat-Zinn, 1990); the mind–body awareness intervention (MBA; k = 4), which is a mindfulness-based curriculum developed for incarcerated youth (Himelstein, 2011a); mindfulness-based relapse prevention–modified (MBRP-modified; k = 2), which combines cognitive behavioral intervention with mindfulness practices to target substance abuse; mindfulness-based programs with a cognitive–behavioral component (MB/CBT; k = 2); mindfulness-based substance abuse treatment (MBSAT; k = 2), which is a novel group-based intervention consisting of mindfulness, self-awareness, and substance-abuse strategies; and other MBIs (MBIs-O; k = 13). MBIs-O were any other MBI that integrated mindfulness and meditation, such as the Re-Entry Values and Mindfulness program (REVAMP; Youman et al., 2010), which is grounded in several MBIs and employs key elements of mindfulness and associated proximal outcomes to reduce risky behavior of incarcerated individuals. A modified version of dialectal behavior therapy (DBT) was included in the MBIs-O as the authors only implemented the mindfulness module of DBT over the course of the intervention. Detailed characteristics of individual studies can be found in Table 1.
Characteristics of Individual Studies
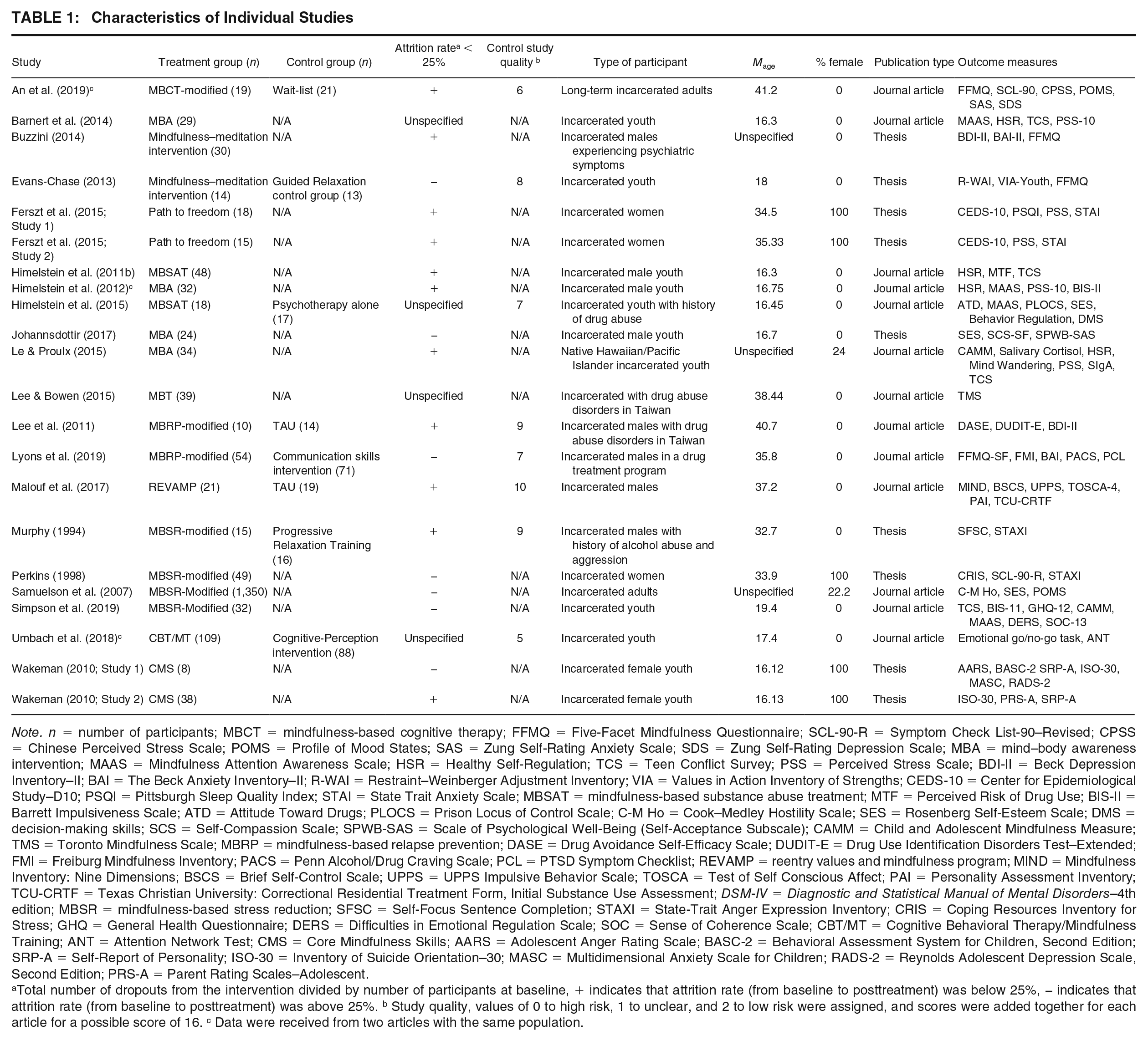
Note. n = number of participants; MBCT = mindfulness-based cognitive therapy; FFMQ = Five-Facet Mindfulness Questionnaire; SCL-90-R = Symptom Check List-90–Revised; CPSS = Chinese Perceived Stress Scale; POMS = Profile of Mood States; SAS = Zung Self-Rating Anxiety Scale; SDS = Zung Self-Rating Depression Scale; MBA = mind–body awareness intervention; MAAS = Mindfulness Attention Awareness Scale; HSR = Healthy Self-Regulation; TCS = Teen Conflict Survey; PSS = Perceived Stress Scale; BDI-II = Beck Depression Inventory–II; BAI = The Beck Anxiety Inventory–II; R-WAI = Restraint–Weinberger Adjustment Inventory; VIA = Values in Action Inventory of Strengths; CEDS-10 = Center for Epidemiological Study–D10; PSQI = Pittsburgh Sleep Quality Index; STAI = State Trait Anxiety Scale; MBSAT = mindfulness-based substance abuse treatment; MTF = Perceived Risk of Drug Use; BIS-II = Barrett Impulsiveness Scale; ATD = Attitude Toward Drugs; PLOCS = Prison Locus of Control Scale; C-M Ho = Cook–Medley Hostility Scale; SES = Rosenberg Self-Esteem Scale; DMS = decision-making skills; SCS = Self-Compassion Scale; SPWB-SAS = Scale of Psychological Well-Being (Self-Acceptance Subscale); CAMM = Child and Adolescent Mindfulness Measure; TMS = Toronto Mindfulness Scale; MBRP = mindfulness-based relapse prevention; DASE = Drug Avoidance Self-Efficacy Scale; DUDIT-E = Drug Use Identification Disorders Test–Extended; FMI = Freiburg Mindfulness Inventory; PACS = Penn Alcohol/Drug Craving Scale; PCL = PTSD Symptom Checklist; REVAMP = reentry values and mindfulness program; MIND = Mindfulness Inventory: Nine Dimensions; BSCS = Brief Self-Control Scale; UPPS = UPPS Impulsive Behavior Scale; TOSCA = Test of Self Conscious Affect; PAI = Personality Assessment Inventory; TCU-CRTF = Texas Christian University: Correctional Residential Treatment Form, Initial Substance Use Assessment; DSM-IV = Diagnostic and Statistical Manual of Mental Disorders–4th edition; MBSR = mindfulness-based stress reduction; SFSC = Self-Focus Sentence Completion; STAXI = State-Trait Anger Expression Inventory; CRIS = Coping Resources Inventory for Stress; GHQ = General Health Questionnaire; DERS = Difficulties in Emotional Regulation Scale; SOC = Sense of Coherence Scale; CBT/MT = Cognitive Behavioral Therapy/Mindfulness Training; ANT = Attention Network Test; CMS = Core Mindfulness Skills; AARS = Adolescent Anger Rating Scale; BASC-2 = Behavioral Assessment System for Children, Second Edition; SRP-A = Self-Report of Personality; ISO-30 = Inventory of Suicide Orientation–30; MASC = Multidimensional Anxiety Scale for Children; RADS-2 = Reynolds Adolescent Depression Scale, Second Edition; PRS-A = Parent Rating Scales–Adolescent.
Total number of dropouts from the intervention divided by number of participants at baseline, + indicates that attrition rate (from baseline to posttreatment) was below 25%, − indicates that attrition rate (from baseline to posttreatment) was above 25%. b Study quality, values of 0 to high risk, 1 to unclear, and 2 to low risk were assigned, and scores were added together for each article for a possible score of 16. c Data were received from two articles with the same population.
Synthesis of Results
Results suggest moderate-to-small effects on all outcome measures combined for all pre–post studies (k = 22; Hedges’s g = 0.309, 95% CI = [0.185, 0.433], p < .001), with high heterogeneity (I2 = 80.276, Q = 106.469). However, results suggest that overall effects for controlled studies (k = 8) were nonsignificant (Hedges’s g = 0.144, 95% CI = [−0.080, 0.368], p = .208, ns). Thus, caution should be exercised before drawing definite conclusions. Only one study examined recidivism and results were nonsignificant for 3-month postrelease (OR = 3.046, 95% CI = [0.618, 14.923], p = .172, ns) and 3 years postrelease for arrest frequency (Hedges’s g = 0.704, 95% CI = [−0.004, 1.412], p = .051, ns). Results were nonsignificant for individuals arrested in the mindfulness relative to the controlled group (OR = 2.984, 95% CI = [0.681, 13.073], p = .147, ns).
Psychological Outcomes
Results from pre–post analyses demonstrated an overall large effect on combined psychological outcomes (e.g., depression, anxiety, and stress; k = 13; Hedges’s g = 0.761, 95% CI = [0.484, 1.038], p < .001), with high heterogeneity (I2 = 86.813, Q = 90.999). Results suggest very large effects on stress (k = 7; Hedges’s g = 1.020, 95% CI = [0.573, 1.467], p < .001), with high heterogeneity (I2 = 89.402, Q = 56.614), and very large effects on depression (k = 7; Hedges’s g = 1.296, 95% CI = [0.672, 1.919], p < .001), with high heterogeneity as well (I2 = 92.546, Q = 80.499). Results suggest medium-to-large effects on anxiety (k = 8; Hedges’s g = 0.600, 95% CI = [0.183, 1.016], p = .005), with high heterogeneity (I2 = 90.898, Q = 76.904). Results from controlled studies analyses suggest a small-to-medium effect of MBIs on anxiety (k = 3; Hedges’s g = 0.357, 95% CI = [0.002, 0.711], p = .049), with low heterogeneity (I2 = 26.456, Q = 2.719), and a large effect on depression (k = 1; Hedges’s g = 0.757, 95% CI = [0.125, 1.389], p = .019). Stress was not investigated in controlled studies. Studies did not report follow-up data on psychological outcomes.
Criminogenic Needs Outcomes
Results from pre–post analyses demonstrated an overall small-to-moderate effect on combined criminogenic needs (e.g., substance use behavior and attitude, impulsivity, anger, and self-regulation; k = 15; Hedges’s g = 0.309, 95% CI = [0.206, 0.411], p < .001), with low-to-moderate heterogeneity (I2 = 35.979%, Q = 21.868). Results suggest a moderate effect of MBIs on anger (k = 5; Hedges’s g = 0.407, 95% CI = [0.222, 0.592], p < .001), with low-to-moderate heterogeneity (I2 = 38.828%, Q = 6.539); results suggest small effects on self-regulation (k = 5; Hedges’s g = 0.265, 95% CI = [0.106, 0.423], p = .001), with low heterogeneity (I2 = 24.217, Q = 5.278). A small effect was found on impulsivity (k = 6; Hedges’s g = 0.241, 95% CI = [0.083, 0.399], p = .003), with low-to-moderate heterogeneity (I2 = 37.024%, Q = 7.940), and substance use behavior and attitude (k = 4; Hedges’s g = 0.281, 95% CI = [0.032, 0.530], p = .027) with moderate heterogeneity (I2 = 61.683%, Q = 7.829). Only one study reported follow-up data on impulsivity and substance use, demonstrating an overall medium-to-large effect (k = 1; Hedges’s g = 0.659, 95% CI = [0.184, 1.134], p = .007). No significant effects were found for combined criminogenic needs in controlled studies (k = 7; Hedges’s g = −0.019, 95% CI = [−0.503, 0.466], p = .940, ns); therefore, limiting any definitive conclusions regarding the effects of MBIs on criminogenic needs.
Mindfulness
Small effects were found on mindfulness in pre–post studies (k = 11, Hedges’s g = 0.211, 95% CI = [0.027, 0.396], p = .025), with high heterogeneity (I2 = 75.009, Q = 40.014). No significant effects were found on mindfulness in controlled studies (k = 5, Hedges’s g = 0.162, 95% CI = [−0.081, 0.406], p = .192, ns). A complete list of effect sizes grouped by outcome measure for pre–post studies is presented in Table 2.
Effects of MBIs Grouped by Type of Outcome Measure for Pre–Post Studies Within Group Effects

Note. The table shows effect size estimates (Hedges’s g), the 95% CIs, and the outcome category effects from before to after administration of the MBI in an incarcerated population. k = number of studies; MBI = mindfulness-based intervention; CI = confidence interval.
p < .05. **p < .01. ***p < .001.
Effects Grouped by Type of Treatment
In pre–post studies, MBRP demonstrated a moderate effect on all outcomes (k = 2; Hedges’s g = 0.477, p < .001), followed by a small-to-moderate effect with MBIs-O (k = 8; Hedges’s g = 0.393, p = .030), MBSR-modified (k = 4; Hedges’s g = 0.381, p < .001), and MBSAT (k = 2; Hedges’s g = 0.330, p = .001). MBA demonstrated a small effect (k = 4; Hedges’s g = 0.200, p = .014). However, no significant overall effects were found with MB/CBT (k = 2; Hedges’s g = 0.272, p = .509, ns). A full description of the effects for each type of treatment group can be found in Table 3.
Effects Grouped by Type of Treatment

Note. The table shows effect size estimates (Hedges’s g), the 95% CIs, and the outcome category effects from before to after administration of the MBI in an incarcerated population. k = number of studies; SE = standard error; CI = confidence interval; MB/CBT = Mindfulness-Based Intervention with a Cognitive Behavioral Component; MBA = mind–body awareness intervention; MBIs-O = other mindfulness-based interventions; MBRP = mindfulness-based relapse prevention; MBSAT = mindfulness-based substance abuse treatment; MBSR = mindfulness-based stress reduction.
p < .05. **p < .01. ***p < .001.
Additional Analyses
Risk of Bias Across and Within Studies
For the risk of bias across studies, the effect sizes for all pre–post studies corresponded to a z value of 10.603 (p < .001), indicating that a minimum of 622 studies with null results would be needed to nullify the results of the current study. The funnel plot for pre–post studies was symmetrical indicating low risk of publication bias and robust results (Figure 2). Risk of bias within studies were evaluated using the Cochrane Collaboration’s tool for assessing risk of bias (Higgins et al., 2011) for controlled studies (k = 8). For each article, values of 0 to high risk, 1 to unclear, and 2 to low risk were assigned and summed. This allowed for examination of the impact of study quality with scores ranging from 5 to 10 out of a possible 14 points (M = 7.625, SD = 1.685). For random sequence generation, the majority of studies were rated as unclear (50%) risk, followed by low (37.5%), and high risk (12.5%). All the studies were rated as unclear for allocation concealment. Most of the controlled studies were rated as low risk of detection bias (87.5%), either because outcome assessors were blind or studies used solely self-report questionnaires. Conversely, all the included controlled studies were rated high risk on performance bias. This was expected for the types of interventions in this study as it is not typical to blind study participants or personnel. The majority of studies (62.5%) were rated as high risk of attrition bias, followed by low risk (37.5%). For reporting bias, studies were either unclear (87.5%) or high (12.5%). Most studies were identified as low risk (87.5%) of other biases, although 12.5% were deemed high risk. See Figure 3 for a complete description of Cochrane ratings.
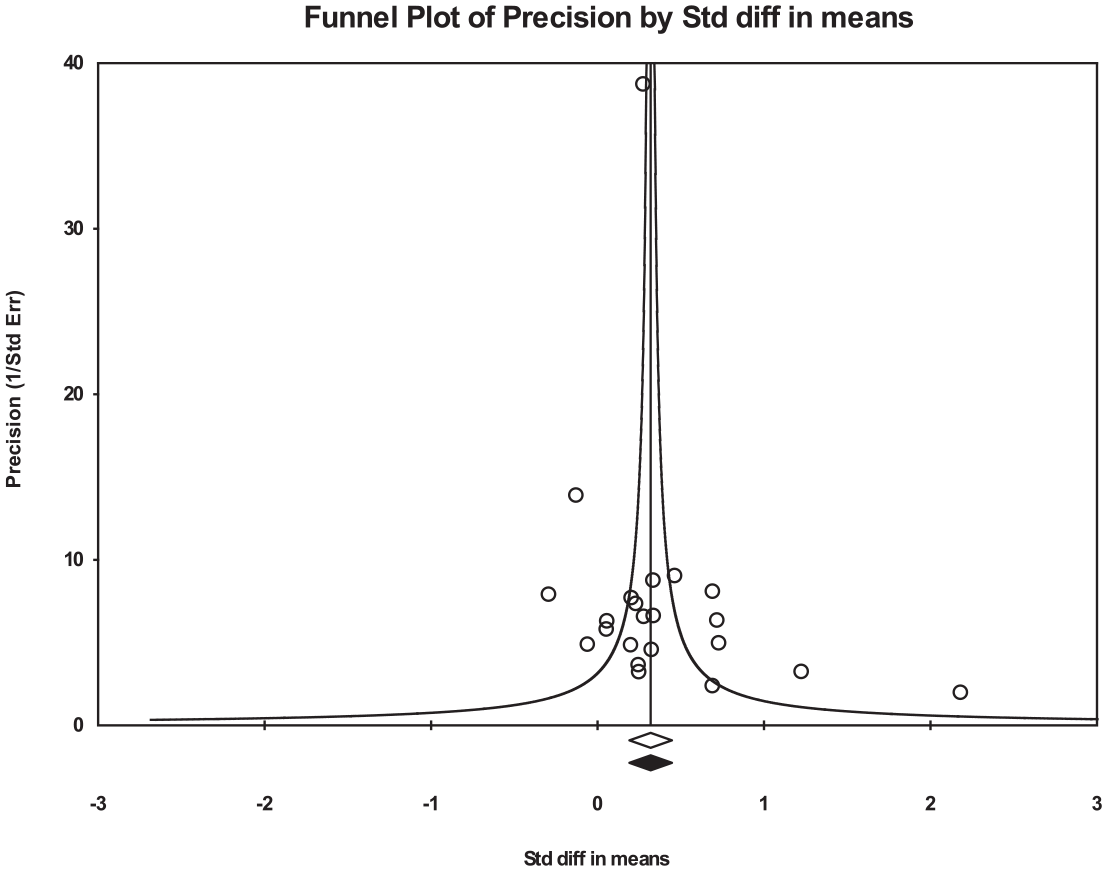
Funnel Plot of Precision by Hedges’s g for Controlled Data
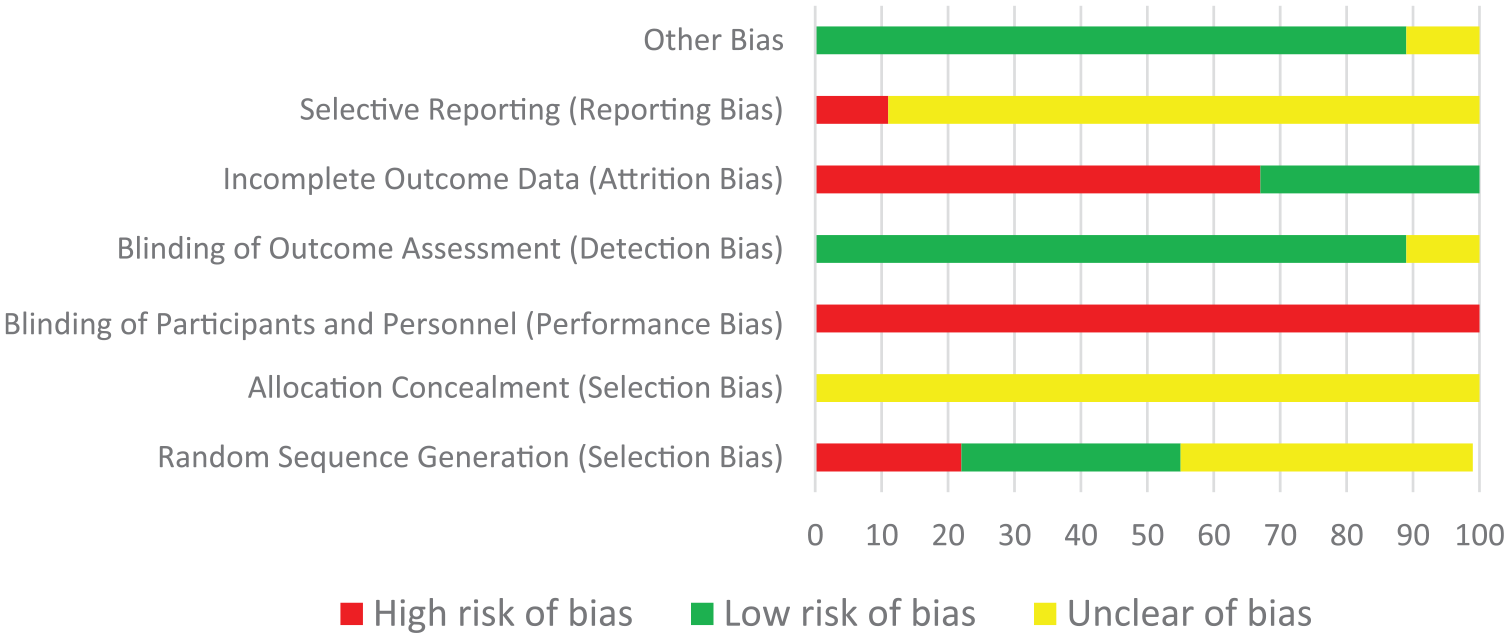
Cochrane Risk of Bias for Individual Studies
Meta-Regression
Meta-regression analyses were conducted on effect results from pre–post studies. Total outcomes were positively but weakly moderated by the percentage of females in the sample (k = 22; β = .007, SE = 0.002, p < .001), mean age (k = 19; β = .012, SE = 0.003, p < .001), and total length of treatment (k = 22; β = .022, SE = 0.005, p < .001). Study quality did not significantly moderate total outcomes (p = .308, ns).
Discussion
Summary of Evidence
This meta-analysis examined 20 articles (22 total studies) using MBIs in a correctional setting. The results suggest that from pre- to posttreatment, MBIs significantly reduced certain dynamic risk factors and improved psychological health outcomes. However, the controlled studies present an important caveat to the pre- to postfindings, as significant results were only found in reducing anxiety and depression. Results from our moderator analyses revealed that when the population was female, older, or when the treatment duration was longer, there was a weak, yet significant and positive effect on overall outcomes. These findings must be interpreted cautiously, given the weak impact of these moderators. In a larger meta-analysis examining the impact of mindfulness across different populations, a moderating effect of age was not found (Khoury, Lecomte, Fortin, et al., 2013). In addition, a recent meta-analysis found MBIs for youth to be effective (Zoogman et al., 2015). Thus, future research is needed to examine differing needs of adolescent versus adult incarcerated populations when engaging in MBIs. The impact of treatment duration on outcome is consistent with previous research (Auty et al., 2017) as cultivating and practicing mindfulness skills is time consuming. With repeated instructions and meditation practices in session, participants may be more equipped to practice mindfulness on their own and may experience more benefits. Future studies should elucidate this effect by comparing different lengths of treatment (e.g., 1- vs. 2-hr-long weekly sessions or four vs. six weekly sessions).
We found that MBIs contributed to large reductions in psychological outcomes of stress, anxiety, and depression in participants in pre–post studies. MBIs yielded the largest effects for attenuating levels of stress and depression. Findings were supported by the controlled studies, which found small-to-medium effects on anxiety and large effects on depression. These results are in line with the current literature demonstrating that MBIs can significantly enhance emotional health (Grossman et al., 2004; Piet & Hougaard, 2011). The implications of these findings are significant, given that incarcerated populations face a disproportionately higher prevalence of psychiatric diagnoses and consequently face additional barriers that may hinder their treatment success (Lamb & Weinberger, 1998; Teplin et al., 2002). These findings may be explained by the cognitive tools offered in mindfulness training, which could serve to decrease emotion-based drives and assist in the management of prison-related stress (Chiesa & Serretti, 2011). However, the included studies failed to investigate follow-up data on psychological outcomes; thus, future research is needed to explore long-term effects of these interventions. In sum, these findings suggest that mindfulness may have the potential to enable higher overall psychological functioning in incarcerated adolescents and adults.
Pre–post treatment results found small-to-moderate improvements on combined criminogenic needs (e.g., self-regulation, impulsivity, anger, substance use behavior, and attitude toward substance use) and MBIs had the largest impact on decreasing anger with a moderate effect. However, when solely targeting controlled studies, the results were insignificant. This suggests that the impact of MBIs on criminogenic outcomes is inconclusive. It is widely accepted that (a) an important intervention goal for incarcerated populations is to manage the risk of reoffending and (b) anger, impulsivity, self-regulation, and drug misuse are significant predictors of reoffending (Wright et al., 2009). The ability to regulate emotions (e.g., anger) requires a high degree of executive control, and mindfulness has been demonstrated to improve emotional regulation. Thus, mindfulness may facilitate a process through which individuals can gain cognitive control over behavior (Baumeister et al., 1994; Shapiro & Schwartz, 2000). Given the importance of these outcomes, their proposed relationship with mindfulness, and the shortage of controlled studies examining them, it is highly recommended that any future research on mindfulness interventions investigates these factors and utilizes a randomized controlled trial (RCT) design.
There was a wide range of included interventions and all, with the exception of MB/CBT, had significant effects on overall outcomes. The findings revealed that MBRP appeared to have the largest effect on overall outcomes with a moderate effect size, followed by MBIs-O and MBSR-modified. Although MBRP yielded the strongest results, these two studies examined individuals with a history of substance use, which may not be generalizable to the incarcerated population as a whole. However, these results demonstrate important findings due to the high prevalence of substance abuse in incarcerated settings. Notably, treatment targeting substance abuse in incarcerated settings has been linked to a reduction in crime-related behaviors (National Center on Addiction and Substance Abuse, 2010; Rempel et al., 2003). The positive effects of MBIs-O highlight how standardized treatments may not be necessary to yield a positive effect in incarcerated settings; thus, incorporation of basic mindfulness and meditation principles may be just as effective.
Interestingly, while mindfulness had a significant yet small effect in pre–post interventions, this was not significant in controlled studies. This may be due to the lack of studies reporting mindfulness outcomes, as only half of the included studies measured and reported mindfulness. The lack of measurement of dispositional mindfulness is a common criticism of the mindfulness literature (Jamieson & Tuckey, 2017; Simpson et al., 2018). Another possible explanation for the small effect is that the mindfulness measures used may not be appropriate for incarcerated populations. According to Himelstein and colleagues (2015), the Mindfulness Attention Awareness Scale (MAAS) item “I find myself preoccupied in the future or past” is considered insensitive toward the intense trauma common in incarcerated populations (Steiner et al., 1997). Future studies warrant pre–post measurements of mindfulness to ascertain validity in changes in mindfulness levels.
The included controlled studies were not found to have significant effects when examining all outcomes combined. Potential explanations are the small number of selected studies, which may have decreased the power of the analysis, and methodological issues, as the majority of controlled studies were not high-quality RCTs. However, we found that study quality was not a significant moderator to overall outcomes. We acknowledge that the nonsignificant findings in controlled studies may limit the interpretations of MBI’s effectiveness in prison populations. To confirm our findings or otherwise, the limited number of studies, their small sample sizes, and general low study quality signal a need for rigorously designed RCTs with high internal validity to investigate the magnitude of MBIs’ effects on incarcerated individuals. Previous research has encountered similar findings regarding study quality (e.g., Hofmann et al., 2010; Klainin-Yobas et al., 2012; Piet & Hougaard, 2011), which is likely due to the lack of RCTs examining MBIs.
Limitations and Future Directions
Important limitations must be considered when examining the results of this meta-analysis. First, there was a high degree of variability in treatment protocols and quantitative outcome measures used to assess criminogenic needs and psychological outcomes. Although all included studies used mindfulness as the main intervention component, there was significant diversity among the treatment protocols. Although some used standardized treatments, other studies used a modified version of existing standardized treatments that varied in terms of protocol and treatment length. Similarly, studies used a wide variety of measures to assess outcomes. For example, among the seven studies that measured depression, multiple measures were used. The high degree of heterogeneity in this analysis suggests that these interventions may not be comparable with each other and limits the generalizability of our findings to different MBIs. The high degree of variability is consistent with prior scoping reviews and meta-analyses on MBIs in incarcerated populations (Auty et al., 2017; Simpson et al., 2018).
Second, despite the potential for MBIs to reduce certain criminogenic needs, risk factors are diverse across participants and are ultimately difficult to generalize. A proposed goal for future research is to investigate the influence of mindfulness on other criminogenic needs, such as negative affect or procriminal attitudes. There is a strong need for follow-up data within longitudinal research as only one study directly investigated recidivism after release (Malouf et al., 2017).
We encourage future research to explore whether positive psychological outcomes, such as self-esteem, mindfulness, and self-compassion, serve as mediators of important factors such as recidivism or clinical outcomes. Some research has found that self-esteem mediates the relationship between mindfulness and both depression and anxiety (Bajaj et al., 2016; Rasmussen & Pidgeon, 2011). Thus, individuals who have high levels of dispositional mindfulness may have higher self-esteem, which consequently contributes to a decrease in anxiety and depression. A better understanding of whether the changes in incarcerated participants’ self-esteem, hope, or self-compassion are significant contributors to these positive outcomes is warranted. Future research should explore the potential pathway through which mindfulness exerts a positive effect on incarcerated individuals, as this was beyond the scope of these analyses.
Finally, the development of well-designed RCTs is needed to truly elucidate the benefits and limitations of MBIs. As demonstrated by our analyses, there is a danger in relying solely on pre–post outcomes as indicators of treatment effectiveness. Although pre–post studies showed significant effects of mindfulness when examining all outcomes combined, results were not supported by controlled studies alone. We make the following recommendations for future researchers: (a) utilize an active control (e.g., psychoeducation about emotion regulation, relaxation intervention) rather than an inactive control (e.g., wait-list), (b) take measures of mindfulness across the entire intervention (e.g., at baseline and postintervention) and between sessions (e.g., before and after each meeting), (c) quantify and qualify mindfulness practice by asking participants to log how long they practiced and how well they were able to engage in the practice (on a daily basis), (d) include a 3-month or longer follow-up postrelease to obtain information about recidivism, (e) obtain qualitative feedback on the intervention to accurately assess feasibility and satisfaction with the MBI, and (f) the use of the Cochrane handbook (Higgins et al., 2011) to avoid potential sources of bias for RCTs (e.g., allocation concealment, blinding of participants). Furthermore, we encourage facilitators to have personal experience with and professional training in mindfulness. It will be important to adapt therapy according to the severity of clients’ concerns, such as cognitive distortions, to avoid overwhelming or harming the client (Gaudiano et al., 2013; Khoury, Lecomte, Gaudiano, & Paquin, 2013). For example, a previous study that investigated case studies revealed that intensive meditation techniques may exacerbate psychosis (Sethi & Bhargava, 2003). Ultimately, we acknowledge the challenges faced when implementing an intervention in a prison setting such as the high rates of attrition due to individuals being released and transferred.
Conclusion
The results of this meta-analysis indicate that MBIs may be a potentially promising intervention for incarcerated populations for enhancing emotional health; however, results were inconclusive regarding criminogenic outcomes. MBIs require minimal resources and are relatively easy to implement in existing adjunct correctional programs. Continued research on the long-term effects of MBIs is needed to evaluate the effectiveness of these treatments and to identify the mechanisms that facilitate change.
Footnotes
Authors’ Note:
The opinions expressed herein are those of the authors.