
Abstract
Intimate partner violence intervention programs (IPVIPs) are intended to rehabilitate individuals charged with intimate partner violence (IPV) offenses, but these programs evidence high rates of treatment dismissal and recidivism. Applying the risk-needs-responsivity framework to improve IPVIP effectiveness has been suggested, and the Minnesota Multiphasic Personality Inventory-2-Restructured Form (MMPI-2-RF) may be used to inform risk estimates in this context. Past research has evaluated MMPI-2-RF Restructured Clinical scale scores in an IPVIP setting, but the remaining MMPI-2-RF substantive scales have yet to be evaluated. We tested the predictive validity of conceptually relevant MMPI-2-RF Higher-Order, Specific Problems, and Personality Psychopathology Five scale scores among a large sample of men who were court-mandated to treatment. Hierarchical logistic regression analyses indicated that several MMPI-2-RF scores incremented predictions of treatment dismissal and various recidivism variables beyond intake variables. Relative risk ratio analyses demonstrated promising utility of the measure in IPVIP settings.
Keywords
Intimate partner violence intervention programs (IPVIPs) were first developed in the late 1970s to rehabilitate individuals charged with intimate partner violence (IPV) offenses (Gondolf, 1997). Many IPVIPs operate under the Duluth model, which is based on the theory that violence is a product of patriarchal ideology that is often reinforced by social structures (Pence & Paymar, 1993). Treatment under this model primarily consists of group-based psychoeducation from a feminist perspective (Pence & Paymar, 1993). Another prominent approach used by IPVIPs is group-based cognitive-behavioral therapy (CBT), which was developed on the idea that violence may be a learned behavior because it benefits the individual; as such, nonviolence can also be learned (Sonkin et al., 1985). The CBT model relies on developing skills for anger management, communication, and interpersonal functioning. It has been noted that modern IPVIPs tend to draw from both Duluth and CBT models (Babcock et al., 2004).
One issue with the implementation of IPVIPs is that they appear to have notably high attrition rates. Olver et al. (2011) conducted a meta-analysis of predictors of treatment attrition and found that rates were highest among individuals who were charged with IPV offenses (37.8%) relative to individuals charged with sex offenses or general violence offenses and individuals in correctional programs. These authors found that individuals who were least likely to complete such programs appeared to be high-risk high-needs individuals. Moreover, responsivity factors (e.g., treatment attitudes and motivation for change) were strong predictors of program attrition. They also found that many IPV-specific variables, such as type of abusive behaviors (e.g., emotional vs. physical) and controlling tendencies, were not significantly associated with program noncompletion, but prior IPV offenses was a strong predictor of noncompletion. Jewell and Wormith (2010) also conducted a meta-analysis of 30 studies on treatment attrition among men who were charged with IPV offenses. They found that many variables were associated with treatment attrition, including employment, age, income, education, marital status, race, referral source, previous IPV offense, criminal history, and alcohol and drug use. Many of these variables were also significantly associated with IPV recidivism. These authors concluded that demographic, violence, and interpersonal factors should be used to inform assessment of risk for attrition so that individuals with relevant characteristics can receive additional supports. Indeed, programs that appear to be most effective tend to include retention strategies (Babcock et al., 2004).
Evidence of high recidivism rates following IPVIP treatment has also accumulated. A meta-analysis by Babcock et al. (2004) indicated that re-offending after treatment appears to occur at a rate of 21% based on police reports or 35% based on partner reports. These authors reported that effects due to IPVIP treatment were in the small range and noted that these effects may be confounded with effects due to police, probation, and legal system involvement. Considering the limited evidence supporting the effectiveness of IPVIPs, Babcock et al. (2004) called for IPVIP treatment providers and researchers to develop and evaluate alternative techniques and evidence-based practices. Day et al. (2009) noted that program logic is not articulated well, and a better model of change may improve IPVIP effectiveness. These authors suggested that interventions which address individual needs may be more effective.
Some treatment programs for individuals who are convicted for violent offenses assess individuals’ needs using the risk-needs-responsivity (RNR) framework (Andrews et al., 1990). The risk principle is that high-risk individuals should receive proportionately more intensive treatment. The needs principle is that effective treatment programs should target individuals’ criminogenic needs (i.e., psychological, emotional, and interpersonal needs that are related to the cause or maintenance of the problem behavior). The responsivity principle holds that programs should deliver cognitive-behavioral interventions that are tailored to individuals’ motivation levels, abilities, and strengths. Using the RNR framework may help to determine which individuals require additional resources and to allow facility staff to “work constructively with high-risk, high-needs clients and retain them in treatment” (e.g., Olver et al., 2011, p. 16). Some have called for more attention to these principles within IPV-related rehabilitation programs—where attrition is particularly high—noting that the effectiveness of offering more intensive treatment to higher risk individuals has been well-established in the wider rehabilitation field (e.g., Day et al., 2009).
Implementing the RNR framework in IPVIPs would require thorough assessment of RNR factors. Some assessment tools designed to predict treatment noncompletion and various types of recidivism (e.g., general violence, IPV) that operate within the RNR framework exist. For example, the Drop-out Risk Screen (DRS; Nunes et al., 2010) is a five-item assessment of static and dynamic recidivism risk factors as well as motivation designed for use in correctional programs. High scores on this screening tool are intended to trigger more thorough assessment. In addition, the Level of Service Inventory–Revised (LSI-R; Andrews & Bonta, 1995) is a 54-item actuarial tool designed to measure general reoffending among adults and has been shown to predict treatment attrition among some individuals charged with various types of offenses (e.g., Rooney & Hanson, 2001). Moreover, the Spousal Assault Risk Assessment (SARA) guide (Kropp et al., 1994) is a structured professional judgment tool intended to assess imminent threat of general or IPV. Helmus and Bourgon (2011) note that the SARA user manual does not define “imminent,” which is a challenge. These authors also highlight that although the SARA is one of the first widely researched scales developed for use among individuals who perpetrate IPV, some of its items consistently do not predict recidivism. Moreover, the SARA may be of limited utility in settings in which individuals are motivated to present themselves positively (Helmus & Bourgon, 2011).
An assessment tool that could serve as an adjunct to many of these purpose-built measures in IPVIP settings is the Minnesota Multiphasic Personality Inventory-2-Restructured Form (MMPI-2-RF; Ben-Porath & Tellegen, 2008/2011). The MMPI-2-RF is an updated version of one of the most widely used assessment tools in forensic psychology (Archer et al., 2006) and has been linked to current approaches to understanding and assessing personality and psychopathology (see Sellbom, 2019 for a review; Ben-Porath, 2012). This tool includes nine Validity Scales, two of which, Uncommon Virtues (L-r) and Adjustment Validity (K-r), can be used to guide interpretation of other scales if there is evidence that individuals are attempting to portray themselves in a positive light, which meets a need highlighted by Helmus and Bourgon (2011). The MMPI-2-RF also includes 42 scales that measure substantive clinical content and are potentially relevant to individuals’ risk and needs factors. MMPI-2-RF authors Ben-Porath and Tellegen (2008/2011) indicate that when scores on the underreporting scales just mentioned reach designated levels, the absence of elevations on the substantive scales cannot be interpreted as indicating the absence of the problems assessed by these scales. Corey and Ben-Porath (2018) discuss how such levels of underreporting could themselves represent a risk in the context of preemployment evaluations of candidates for public safety positions. These scales could serve a similar function in assessments of IPVIP candidates.
Historically, the MMPI instruments have been used to study IPV. For example, Hale et al. (1988) identified trends in MMPI profiles among men charged with IPV offenses. More recently, Sellbom et al. (2008) examined the utility of the MMPI-2-RF Restructured Clinical (RC) Scales in predicting IPVIP treatment dismissal and IPV recidivism. Point biserial correlations between RC Scale scores and criteria yielded statistically significant correlations between Demoralization (RCd), Dysfunctional Negative Emotions (RC7), and Hypomanic Activation (RC9) scores and conduct problems and violence disinhibition confidence. In addition, Antisocial Behavior (RC4) scores were associated with criminal history, conduct problems, substance use, amount of previous partner violence, and low violence inhibition confidence. The authors reported statistically significant correlations between Cynicism (RC3) and Ideas of Persecution (RC6) scores and blame externalization. Sellbom et al. (2008) also conducted hierarchical regression analyses with background variables in the first block and the RC Scales in the second block to predict treatment dismissal and IPV recidivism. RC9 added 2.2% variance beyond income and substance use in predicting treatment outcome and added 2.4% variance beyond income in predicting IPV recidivism. Finally, Sellbom et al. (2008) conducted relative risk ratio analyses for RC4 and RC9. Elevated scores (>65T) on either scale were more strongly associated with negative outcomes than nonelevated scores, but RC9 was the stronger predictor. Individuals with scores above 65T on this scale were about twice as likely to be dismissed from treatment, and individuals with scores ≥75T were about 2.5 times as likely to be dismissed. Individuals who had elevated scores on either RC4 or RC9 were about 60.0% to 70.0% more likely to recidivate.
The RC Scales were used as part of a previous version of the MMPI, the MMPI-2, at the time of Sellbom et al.’s (2008) investigation. The subsequently published MMPI-2-RF, which was not available when Sellbom et al. conducted their study, incorporated the RC Scales as core measures, complemented hierarchically by both broader and more narrowly focused dimensional psychopathology scales. The current investigation examines the potential for using these additional MMPI-2-RF measures for identifying risk and needs factors related to increased risk of negative outcomes for individuals entering an IPVIP.
The MMPI-2-RF has previously been shown to identify factors relevant to treatment attrition and recidivism in other forensic settings. For example, Mattson, Powers, Halfaker, Akeson, and Ben-Porath (2012) previously studied the utility of MMPI-2-RF scores in predicting drug court treatment completion. They found that higher scores on externalizing (i.e., Behavioral/Externalizing Dysfunction [BXD], Antisocial Behavior [RC4], Juvenile Conduct Problems [JCP], Aggression [AGG], and Disconstraint [DISC-r]) and aberrant experiences (i.e., Aberrant Experiences [RC8]) scales were associated with higher risk of failure to complete treatment. In addition, Tarescavage et al. (2016) found that scores on MMPI-2-RF scales measuring emotion dysregulation and externalizing dysfunction were significantly associated with future violence in a sample of psychiatric inpatients. Furthermore, Tarescavage et al. (2014) found that MMPI-2-RF externalizing scales—including Behavioral/Externalizing Dysfunction (BXD), Antisocial Behavior (RC4), Juvenile Conduct Problems (JCP), Substance Abuse (SUB), Aggression (AGG), Activation (ACT), and Disconstraint-Revised (DISC-r)—predicted probation violations after felonious crimes with moderate to large effect sizes.
This Study
High rates of treatment attrition and recidivism among individuals convicted of IPV have led some to suggest use of the RNR framework within IPVIPs (e.g., Day et al., 2009). Some established scales exist for this purpose. The information they provide may be augmented by using a well-validated measure of personality and psychopathology. Indeed, a widely used assessment of personality and psychopathology, MMPI-2-RF, may be a useful supplement for identifying individuals’ RNR factors. Mattson et al. (2012), Tarescavage, Luna-Jones et al. (2014), Tarescavage et al. (2016), and Sellbom et al. (2008) generally showed that MMPI-2-RF scales that measure emotional and externalizing dysfunction were associated with adverse outcomes, such as failure to complete treatment and recidivism in forensic settings. As such, we expected statistically significant associations with treatment dismissal and various recidivism variables for MMPI-2-RF scores from conceptually relevant externalizing scales (Behavioral/Externalizing Dysfunction [BXD], Family Problems [FML], Juvenile Conduct Problems [JCP], Substance Abuse [SUB], Aggression [AGG], Activation [ACT], Aggressiveness [AGGR-r], and Disconstraint [DISC-r]), emotional dysfunction scales (Emotional/Internalizing Dysfunction [EID], Helplessness/Hopelessness [HLP], Self-Doubt [SFD], Inefficacy [NFC], Stress/Worry [STW], Anxiety [AXY], Anger Proneness [ANP], Behavior-Restricting Fears [BRF], Multiple Specific Fears [MSF], and Negative Emotionality/Neuroticism [NEGE-r]), and an interpersonal scale (Interpersonal Passivity [IPP]), in addition to the RC Scales previously found to be related to these outcomes by Sellbom et al. (2008). We also tested the incremental validity of the MMPI-2-RF scores above intake variables and treatment dismissal in predicting recidivism by conducting hierarchical logistic regression analyses. Finally, we examined the clinical utility of MMPI-2-RF scores by calculating relative risk ratios (RRRs), which indicate the proportional increase in risk for adverse outcomes when MMPI-2-RF scale elevations occur.
Method
Participants
Participants in this study were 596 men who were convicted of IPV for the first time and who were court-mandated to complete treatment at an IPVIP in Northeastern Ohio between September 1997 and August 1998 for actions against female partners. This sample was the same as the one used by Sellbom et al. (2008) to investigate the predictive validity of the RC Scales. Participants with invalid MMPI-2-RF protocols (Cannot Say [CNS] ≥ 18, Variable Response Inconsistency [VRIN-r] or True Response Inconsistency [TRIN-r] T ≥ 80, Infrequent Responding [F-r] T = 120, and Infrequent Psychopathology Responses [Fp-r] T ≥ 100) were excluded from the study (see Ben-Porath & Tellegen, 2008/2011). Of the participants excluded based on invalid MMPI-2-RF protocols, the vast majority were excluded for non-content-based invalid responding (89.0%), while 11.0% were excluded for content-based invalid responding. The final sample consisted of 478 men with an average age of 35.46 (SD = 10.16). The ethnic distribution was 48.3% African American, 40.8% Caucasian, 4.8% Hispanic American, and remaining 6.1% of other or mixed ethnicity. Most participants were never married (35.4%), married (31.0%), or divorced (21.1%). The participants had an average of 11.70 (SD = 1.85) years of education. Participants who produced invalid MMPI-2-RF protocols were significantly younger (t [594] = 2.76, p = .006, d = .28), less educated (t [587] = 3.54, p < .001, d = .37), and more likely to be of minority ethnic status (χ2 [N = 596] = 14.85, p < .001, ω′ = .16), though all effect size estimates were of weak magnitude.
Measures
MMPI-2-RF
The MMPI-2-RF (Ben-Porath & Tellegen, 2008/2011) is a 338-item assessment of personality and psychopathology. Its items aggregate onto nine Validity Scales and 42 scales that measure substantive clinical content. The substantive scales are arranged in a hierarchical order, with three Higher-Order Scales, nine Restructured Clinical Scales, and 23 Specific Problems Scales, complemented by two Interest Scales and five Personality Psychopathology Five Scales. Administration of the MMPI-2-RF is estimated to take 25 to 35 min on a computer (Ben-Porath & Tellegen, 2008/2011). A substantial amount of evidence has accumulated for the reliability and validity of MMPI-2-RF scale scores among several populations (see Sellbom, 2019, for a review).
The MMPI-2 was administered to participants and responses were rescored into MMPI-2-RF scale scores. Past research using a forensic sample has demonstrated comparability of MMPI-2-RF scores from the MMPI-2 and MMPI-2-RF booklets (Tarescavage, Alosco, et al., 2014; Van Der Heijden et al., 2010).
Intake Interview
Historical data were collected in conjunction with intake interviews. This background information included criminal history, current charges, employment information, anger frequency, prior mental health history, and substance use. We compiled three aggregate background variables composed of the mean standardized scores of the following individual items: criminal history (aggregate of number of prior arrests [range = 0–11], number of misdemeanor convictions [range = 0–5], and number of felony convictions [range = 0–8]), substance abuse problems (Diagnostic and Statistical Manual of Mental Disorders, 4th ed.; DSM-IV; American Psychiatric Association, 1994 substance abuse, DSM-IV substance dependence, and alcohol problem; each coded 1 = no and 2 = yes), and conduct problems (juvenile history of running away, stealing, school suspensions, violent behaviors, fire setting, and lying; each coded 1 = never, 2 = sometimes, and 3 = often). Individual variables were also examined, including current mental health treatment (coded 1 = no and 2 = yes), anger frequency (coded 1 = never, 2 = rarely, 3 = sometimes, and 4 = usually), and amount of previous partner violence (range = 7–20 times).
Treatment Dismissal
Data regarding treatment participation and compliance were available for 90.8% of the final sample. Individuals were dismissed from the program if they missed an excessive number of treatment sessions (e.g., two sessions in the 6-week program or three sessions in the 12-week program), failed to submit urine samples for random drug screens, failed to complete a homework assignment or pay a program fee, were arrested, engaged in substance abuse, or failed to pass the final examination covering program material. One hundred forty-four (33.2%) individuals for whom data were available were dismissed from treatment.
New Arrest Data
Follow-up data from participants’ probation files and local police records were collected 1 year after program completion. Data regarding new arrests for any offense during the 1-year follow-up period were available for 84.9% of the final sample. Within the final sample, 147 (36.2%) of individuals for whom data were available had been arrested during this time.
IPV Recidivism Data
Follow-up data regarding IPV recidivism were available for 62.6% of the final sample. We considered participants to have recidivated an IPV offense if they had any further involvement with the legal system specifically related to IPV. Such involvement included being in violation of a no-contact order, having had a new complaint of IPV brought against them, or having had a new arrest or conviction for IPV after intake to the treatment program. Seventy-six (24.4%) participants in the final sample were found to have recidivated an IPV offense within the 1-year follow-up period based on local police records and probation files.
General Recidivism Data
We calculated a broad recidivism variable that includes a new arrest for any offense and any IPV recidivism (as described above). Data needed to score this variable were available for 62.6% of the final sample. Of these individuals, 142 (47.5%) had reoffended (i.e., were arrested or had further involvement in the legal system related to IPV) within the 1-year follow-up period.
Procedures
Participants were men who were convicted of IPV offenses for the first time and who were court-mandated to attend IPVIP treatment. This treatment utilized the Duluth model as well as cognitive-behavioral techniques. Individuals were randomly assigned to an outpatient treatment program of varying lengths (6, 12, or 24 weeks) and attended weekly group treatment sessions. Participants were scheduled for an intake appointment at the treatment facility subsequent to referral to the program. They were administered the MMPI-2 by a trained research assistant. A licensed social worker interviewed the participants and gathered background information. The information was entered into a research database. No staff member had access to the participants’ MMPI-2 scores, and these data were not used to make any decisions regarding participants in this program.
Results
Correlational Analyses
We first investigated the association between treatment dismissal and new arrest (r = .19; n = 388), IPV recidivism (r = .26; n = 299), and general recidivism (r = .27; n = 299), which all evidenced statistically significant associations. We then calculated point biserial correlations between the hypothesized MMPI-2-RF substantive scale scores and the outcome variables (treatment dismissal, new arrest, IPV recidivism, and general recidivism; see Table 1). Although the RC Scales were previously examined by Sellbom et al. (2008) using this sample, we present correlations with the RC Scales because those authors had a more limited set of recidivism outcome variables. In addition, because we calculated a considerable number of correlations, we chose a conservative alpha level of .01 for these analyses. We considered rpb values of .10, .24, and .37 to indicate small, medium, and large effects, respectively, because base rates for outcome variables ranged from 24.4% to 47.5% (see Cohen, 1988; Rice & Harris, 2005). Consistent with our hypotheses, scores on the following scales demonstrated statistically significant associations with treatment dismissal with small effect sizes: Behavioral/Externalizing Dysfunction (BXD), Antisocial Behavior (RC4), Dysfunctional Negative Emotions (RC7), Hypomanic Activation (RC9), Anger Proneness (ANP), Juvenile Conduct Problems (JCP), Aggression (AGG), Family Problems (FML), Behavior-Restricting Fears (BRF), Aggressiveness (AGGR-r), and Disconstraint (DISC-r). These same scale scores (except RC4 and BRF) were also significantly associated with new arrests to a small degree. Interestingly, only RC4 scores were significantly associated with IPV recidivism. General recidivism was significantly associated with scores on BXD, Demoralization (RCd), RC4, RC7, RC9, Anxiety (AXY), ANP, JCP, Substance Abuse (SUB), AGG, FML, DISC-r, and Negative Emotionality/Neuroticism (NEGE-r) to a small degree. Finally, we present correlations between relevant MMPI-2-RF scale scores and the intake variables in Table 2.
MMPI-2-RF Substantive Scale Score Point Biserial Correlations With Treatment Dismissal and Recidivism Variables

Note. MMPI-2-RF = Minnesota Multiphasic Personality Inventory-2-Restructured Form; IPV = intimate partner violence; pb = point biserial; RC = Restructured Clinical.
p < .05. **p < .01.
MMPI-2-RF Substantive Scale Score Correlations With Intake Variables

Note. MMPI-2-RF = Minnesota Multiphasic Personality Inventory-2-Restructured Form; pb = point biserial; RC = Restructured Clinical.
p < .05. **p < .01.
Hierarchical Logistic Regression Analyses
Next, we conducted hierarchical logistic regression analyses to test the incremental validity (over significantly associated intake variables) of the MMPI-2-RF scales that were significantly associated with the outcome variables. To determine which variables to specify in the first block, we calculated point biserial correlations between the intake variables and each outcome variable (see Table 3). Treatment dismissal was significantly associated with substance use problems, so we entered this variable in the first block for analyses predicting treatment dismissal. The new arrests variable and IPV recidivism were significantly associated with conduct problems, so this variable was entered into the first block along with treatment dismissal (to control for whether individuals completed the program) for analyses predicting new arrests and IPV recidivism. General recidivism was significantly associated with substance use problems and conduct problems, so these intake variables were entered into the first block with treatment dismissal for analyses predicting general recidivism.
Correlations Between Intake Variables and Treatment Dismissal and IPV Recidivism, and Between Outcome Variables
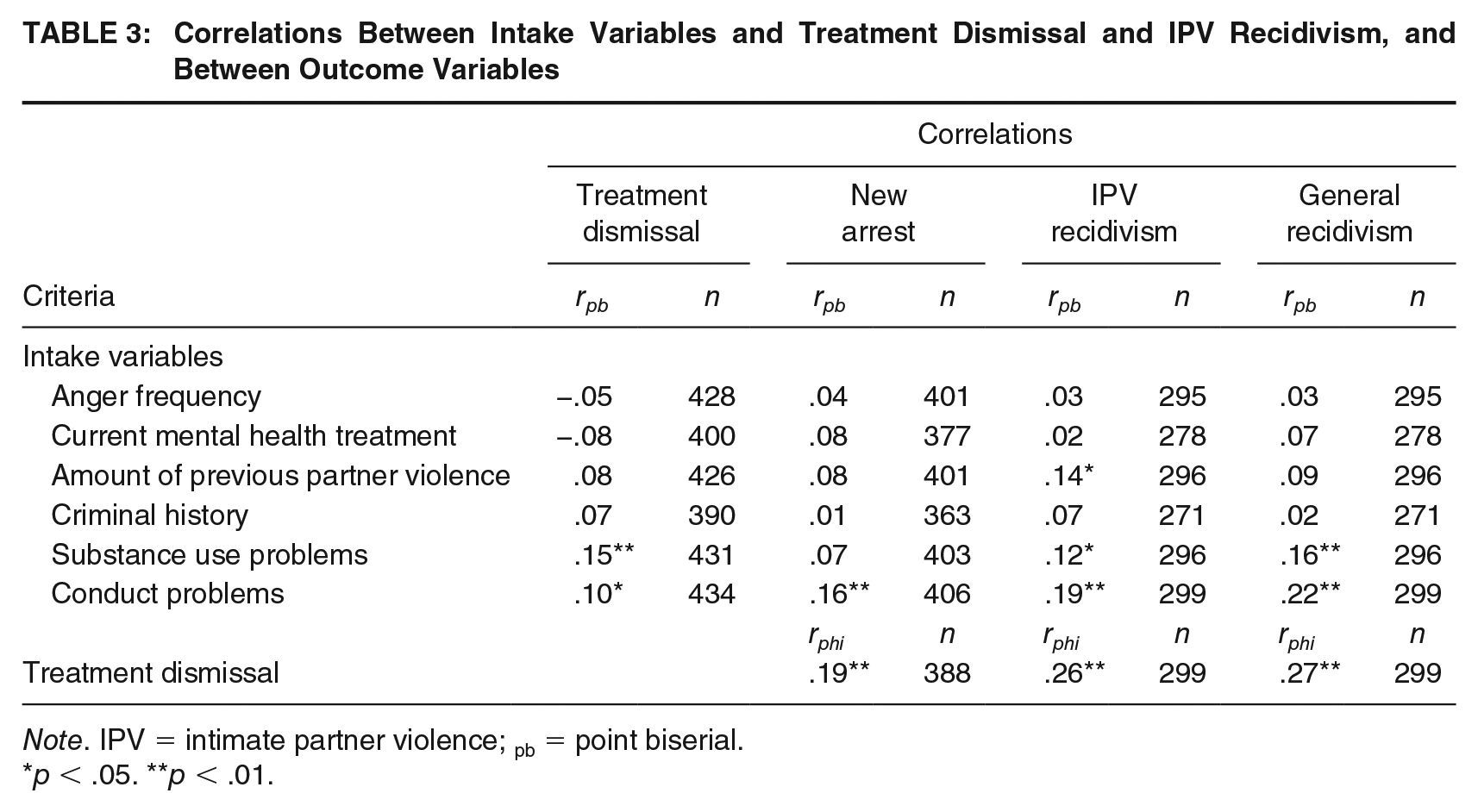
Note. IPV = intimate partner violence; pb = point biserial.
p < .05. **p < .01.
In the second block of the hierarchical regression analyses, we specified individual MMPI-2-RF scales that were significantly associated with the dependent variable. Thus, for predicting treatment dismissal, we calculated 11 hierarchical regression analyses, each with one of the following individual scales in the second block: Behavioral/Externalizing Dysfunction (BXD), Antisocial Behavior (RC4), Dysfunctional Negative Emotions (RC7), Hypomanic Activation (RC9), Anger Proneness (ANP), Juvenile Conduct Problems (JCP), Aggression (AGG), Family Problems (FML), Behavior-Restricting Fears (BRF), Aggressiveness (AGGR-r), and Disconstraint (DISC-r). For predicting new arrests, we examined the incremental validity of BXD, RC7, RC9, ANP, JCP, AGG, FML, AGGR-r, and DISC-r scores in a similar manner, resulting in nine regression analyses. For predicting IPV recidivism, we examined the incremental validity of RC4 scores. Finally, we examined the incremental validity of BXD, Demoralization (RCd), RC4, RC7, RC9, Anxiety (AXY), ANP, JCP, Substance Abuse (SUB), AGG, FML, DISC-r, and Negative Emotionality/Neuroticism (NEGE-r) by entering these scores in the second block for the 13 regression analyses predicting general recidivism. Here too, we present analyses of the RC Scales in the interest of completeness.
Observations were independent as licensed clinical social workers collected intake data, and the treatment team coded outcome variables. Correlations among predictors did not evidence violation of the multicollinearity assumption. The Box and Tidwell (1962) procedure was used to test for linearity of predictors and their natural logs. For predicting treatment dismissal, the interaction term for Disconstraint (DISC-r) scores and their log odds was statistically significant. Thus, associated results should be interpreted with caution.
Each scale score that was significantly associated with treatment dismissal also significantly incremented predictions of treatment dismissal beyond substance use problems. MMPI-2-RF Hypomanic Activation (RC9), Aggressiveness (AGGR-r), and Disconstraint (DISC-r) scores significantly incremented prediction of new arrests over conduct problems and treatment dismissal. Antisocial Behavior (RC4) scores did not significantly increment over treatment dismissal and conduct problems for predicting IPV recidivism. Finally, scores on Dysfunctional Negative Emotions (RC7), Anxiety (AXY), Substance Abuse (SUB), and Family Problems (FML) significantly incremented predictions of general recidivism over treatment dismissal, substance use problems, and conduct problems (see Table 4).
Hierarchical Logistic Regression Analyses for MMPI-2-RF Substantive Scales a Predicting Outcome Variables Above Intake Variables and Treatment Dismissal
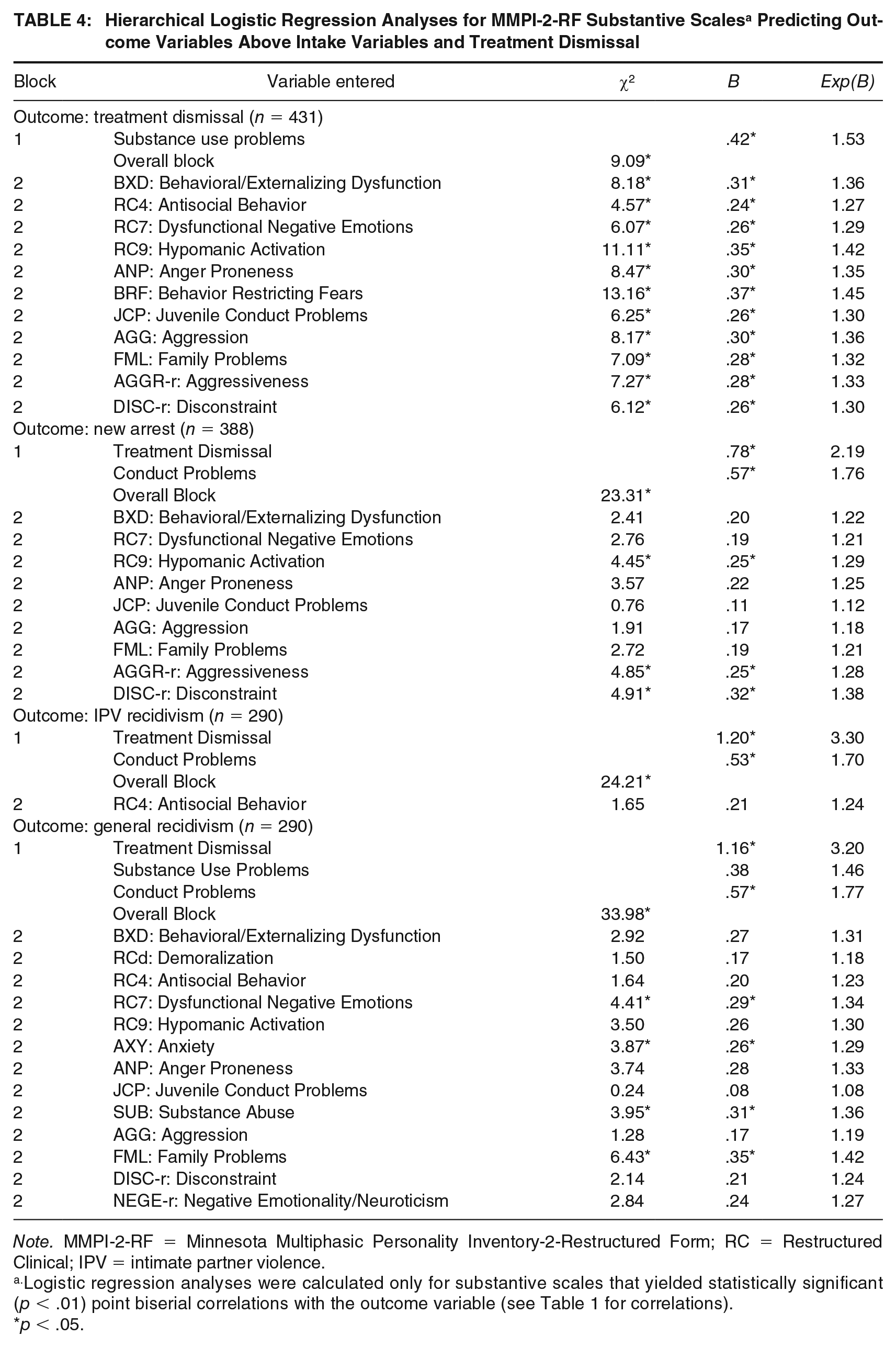
Note. MMPI-2-RF = Minnesota Multiphasic Personality Inventory-2-Restructured Form; RC = Restructured Clinical; IPV = intimate partner violence.
Logistic regression analyses were calculated only for substantive scales that yielded statistically significant (p < .01) point biserial correlations with the outcome variable (see Table 1 for correlations).
p < .05.
Relative Risk Ratios
We calculated RRRs to investigate the clinical utility of the MMPI-2-RF scales for predicting treatment dismissal and each recidivism variable. RRR is the proportion of the risk of a negative outcome for people who scored at or above a cutoff to the risk of that outcome for people who scored below the cutoff. We calculated RRRs at a 65T cutoff only for scales that were both significantly associated with the dependent variable and elevated at this cutoff for at least 2.0% of the sample (i.e., selection ratios ≥ 2.0%) to reduce the likelihood of outliers affecting the results. We calculated 95% confidence intervals for the RRRs, and those that do not overlap with 1.00 indicate significant findings (see Table 5).
RRRs for MMPI-2-RF Substantive Scales a at 65T Cutoffs Predicting Outcomes

Note. Statistically significant (p < .05) findings are bolded; treatment dismissal base rate = 33.2%; IPV recidivism base rate = 46.7%. MMPI-2-RF = Minnesota Multiphasic Personality Inventory-2-Restructured Form; SR = selection ratio; CI = confidence interval; RC = Restructured Clinical; IPV = intimate partner violence.
Relative risk ratios (RRRs) were calculated only for substantive scales that yielded point biserial correlation value of p < .01 with the respective outcome variable and had a selection rate ≥2.0% (see Table 1 for correlates).
To illustrate interpretation of these results, we will describe findings for elevated scores on Behavioral/Externalizing Dysfunction (BXD) at the 65T cutoff in the prediction of treatment dismissal (see the first row of Table 5). The selection ratio indicates that 21.9% of the sample scored at or above the 65T cutoff, and the risk for treatment dismissal in this group is 47.4%. The risk was 29.2% for someone who scored < 65T. Thus, the RRR is 1.62, indicating that individuals with elevations on BXD at 65T are 1.62 times more likely to be dismissed from treatment, as compared to those without elevations. Overall, several RRR analyses yielded statistically significant and clinically meaningful results. For example, those with elevations at 65T on Anger Proneness (ANP) were 1.69 times more likely to be dismissed from treatment. Those with elevations at 65T on Disconstraint (DISC-r) were 1.75 times more likely to be dismissed from treatment and 1.50 times more likely to recidivate any offense within 1 year of IPVIP treatment outset. Individuals with elevations at 65T on Antisocial Behaviors (RC4) were 1.54 times more likely to recidivate an IPV offense and 1.60 times more likely to recidivate any offense. Individuals with 65T scale elevations on Family Problems (FML) were 1.96 times more likely to be arrested and 1.90 times more likely to recidivate any offense within the follow-up period.
Discussion
The purpose of this study was to investigate the predictive validity, incremental validity, and clinical utility of MMPI-2-RF scale scores within the RNR framework in an IPVIP setting. Point biserial correlations between conceptually relevant MMPI-2-RF scale scores and treatment dismissal, new arrests, and general recidivism showed statistically significant associations for several scales. One conceptually relevant MMPI-2-RF scale was significantly associated with IPV recidivism. Hierarchical logistic regression analyses showed that all MMPI-2-RF scale scores that were significantly associated with treatment dismissal also improved upon predictive utility of intake variables in predicting this outcome. Some MMPI-2-RF scale scores incremented intake variables and treatment dismissal for predicting new arrests and general recidivism, but no MMPI-2-RF scale scores significantly improved beyond treatment dismissal and significantly associated intake variables for predicting IPV recidivism. Finally, RRR analyses indicated that individuals were significantly more likely to be dismissed from treatment and reoffend if they had elevations on conceptually relevant MMPI-2-RF scales. Several aspects of these findings warrant further discussion.
Correlation Analyses
First, we investigated the association between treatment dismissal and recidivism variables. Interestingly, not completing IPVIP treatment was meaningfully associated with new arrests within a year (rphi = .19) and—to a greater extent—IPV recidivism (rphi = .26) and general recidivism (rphi = .27). These findings indicate need for greater responsivity to maximize IPVIP retention.
Correlation analyses between MMPI-2-RF scores and treatment dismissal yielded significant findings for several externalizing (Behavioral/Externalizing Dysfunction [BXD], Antisocial Behavior [RC4], Hypomanic Activation [RC9], Juvenile Conduct Problems [JCP], Aggression [AGG], Family Problems [FML], Aggressiveness [AGGR-r], and Disconstraint [DISC-r]) and emotion dysregulation (Dysfunctional Negative Emotions [RC7], Anger Proneness [ANP], Behavior-Restricting Fears [BRF]) scales. These findings generally converge with previous research by Mattson et al. (2012), who found that higher scores on some externalizing scales and the Aberrant Experiences (RC8) scale were associated with higher risk of failure to complete drug court treatment. However, the current findings indicated that emotion dysregulation problems were also associated with attrition from IPVIPs, indicating that individuals with these problems may deserve additional support to maximize their ability to complete treatment.
Several of these same externalizing and emotion dysregulation scales, with the exceptions of Antisocial Behaviors (RC4) and Behavior-Restricting Fears (BRF) scores, were significantly associated with having a new arrest, but only RC4 was significantly associated with IPV recidivism. The correlation findings between new arrests and MMPI-2-RF scores are consistent with Tarescavage et al. (2016), who found that scales measuring emotional and externalizing dysfunction were significantly associated with future violence in a sample of psychiatric inpatients. The current findings indicate that recidivating IPV offenses, however, may be more closely related to a propensity for disobeying rules and authority (i.e., high scores on RC4; Ben-Porath & Tellegen, 2008/2011), rather than emotional and externalizing problems.
Hierarchical Logistic Regression Analyses
We also found that MMPI-2-RF scales that were significantly associated with outcomes incremented predictions of treatment dismissal, new arrests, and general recidivism beyond relevant intake variables, but no MMPI-2-RF scale score significantly incremented intake variables and treatment dismissal in predicting IPV recidivism. These findings are generally consistent with previous research by Tarescavage, Luna-Jones et al. (2014) who identified several externalizing MMPI-2-RF scale scores that predicted probation violation following felonious crimes. However, several internalizing scale scores also predicted treatment dismissal and general recidivism (but not new arrests) in this study. This study may have yielded different results for the prediction of IPV recidivism because IPV is inherently an offense with very specific contextual and interpersonal dynamics, including low reporting rates by victims (Esquivel-Santovena & Dixon, 2012), and official records may be less likely to capture the extent of these behaviors than other felonious crimes for analyses predicting IPV recidivism. Additional research, possibly using victim-report measures for recidivism data, is warranted to determine if this finding replicates.
Relative Risk Ratios
Finally, RRR analyses indicated that MMPI-2-RF scales have promising clinical utility within the RNR framework in an IPVIP setting. Participants with elevated scores on associated scales were 1.16 to 2.34 times more likely to be dismissed from treatment, 1.26 to 1.96 times more likely to be arrested, 1.54 times more likely to recidivate an IPV offense, and 1.25 to 1.90 times more likely to recidivate with general offense(s) within a year of IPVIP treatment. Importantly, the high base rates (BRs) for treatment dismissal and recidivism may have limited the size of the RRRs (treatment dismissal BR = 33.1%, new arrest BR = 36.2%, IPV recidivism BR = 24.4%, general recidivism BR = 47.5%). Therefore, the maximum possible RRRs for treatment dismissal and IPV recidivism are approximately 3.00 and 2.00, respectively. Nevertheless, these findings may be helpful to clinicians conducting intake evaluations to an IPVIP within the RNR framework because they quantify the extent to which certain psychological and emotional needs factors may be related to adverse outcomes. For example, individuals with elevated scores on the Hypomanic Activation (RC9) Scale were 2.34 times more likely to be dismissed from treatment than those who did not have elevations on this scale. Thus, responsive IPVIP facilitators may allocate additional resources or implement pretreatment preparation to individuals with elevations on RC9 to maximize their abilities to fully benefit from the treatment.
MMPI-2-RF Scores in the RNR Framework
MMPI-2-RF scores may be most useful in these settings as adjuncts for mainstay risk assessment tools. MMPI-2-RF scales measure constructs that are strongly aligned with variables frequently included in such risk assessment tools. For example, the LSI-R (Andrews & Bonta, 1995) is a general violence risk assessment tool that operates within the RNR framework. This tool involves ratings on variables such as family and marital problems, alcohol and drug problems, emotional problems, criminal history, and “Authority interactions”—constructs that are measured by MMPI-2-RF Family Problems (FML), Substance Abuse (SUB), Emotional/Internalizing Dysfunction (EID), Behavioral/Externalizing Dysfunction (BXD), and Antisocial Behaviors (RC4) scales, respectively. Thus, the MMPI-2-RF offers well-validated objective measures of personality and psychopathology that may directly inform ratings on the LSI-R and other widely used risk assessment tools within IPVIP settings.
Implementing individual needs assessment within IPVIPs using the MMPI-2-RF could be done in addition to existing risk assessment tools, but may require additional resources—including having a licensed psychologist or another qualified professional on staff to interpret MMPI-2-RF profiles. However, there is meta-analytic evidence that having consistent psychologist involvement and clinical supervision for facilitators in IPVIPs is beneficial to treatment effectiveness (Gannon et al., 2019).
In sum, MMPI-2-RF scores can be directly related to the RNR framework. Men who were at higher risk for recidivism produced higher scores on several expected MMPI-2-RF scales, indicating relevance to the risk principle. Several MMPI-2-RF scale scores significantly incremented intake variables in predicting adverse outcomes and yielded significant RRRs, indicating that these scores identify individual criminogenic needs that could be targets for IPVIP treatment. Finally, men with higher scores on MMPI-2-RF scales were also at greater risk for treatment dismissal, demonstrating the test’s relevance to the responsivity principle. Thus, MMPI-2-RF scores may be especially useful to clinicians seeking to improve IPVIP effectiveness by implementing the RNR framework, especially when administered alongside mainstay RNR forensic risk assessment tools.
Limitations and Future Directions
This study has several limitations that point to future directions in research. First, participants who produced invalid MMPI-2-RF protocols were significantly younger, less educated, and more likely to be of minority ethnic status than those with valid MMPI-2-RF scores. Nevertheless, the final sample of participants who produced valid MMPI-2-RF protocols was diverse, consisting of a majority of African American men (48.3%). Moreover, only males with female partners were included in this study, and results may not generalize to females who perpetrate IPV against male partners or same-sex dyads. Second, these data were collected between 1997 and 1998, when IPVIPs were a relatively new treatment option. Therefore, replication with a newer sample is needed. Third, this study used self-reported data for some variables, such as amount of previous partner violence. The accuracy of such self-reports may be influenced by reporting bias. Fourth, this study relied on local police reports and probation files for information on IPV recidivism. Information from these sources does not consider IPV offenses that were reported in other jurisdictions or offenses that were not reported to law enforcement. Future studies may attempt to gather recidivism data by contacting victims; broader outcomes, such as general violent recidivism may be of interest. In addition, participants in this study were court-mandated to IPVIP treatment following first-time legal involvement related to IPV; future studies should examine the utility of the MMPI-2-RF scales for predicting these outcomes among individuals who have had repeated involvement in the legal system related to IPV. Furthermore, we were unable to control for differential opportunities to reoffend based on subsequent arrest. Future studies should collect such data to control for these differences. Finally, future studies should investigate whether broadband instruments, such as the MMPI-2-RF, may have incremental utility over static risk assessment tools for predicting variables, such as treatment dismissal, recidivism, and future violence.
Notwithstanding these limitations, this study provided evidence for the validity of the MMPI-2-RF scales for identifying individual RNR factors and informing risk estimates within an IPVIP setting. MMPI-2-RF scales were less strongly associated with IPV recidivism than treatment dismissal, but because these outcomes were significantly related, programs that respond to needs factors related to treatment dismissal may also reduce IPV recidivism. These findings support the use of the MMPI-2-RF to inform IPVIP intake and treatment decisions within the RNR framework. Future research is warranted that addresses whether implementing treatment for individuals convicted of IPV within this framework would improve the effectiveness of IPVIPs.
Footnotes
Authors’ Note:
The statements and opinions in this article are those of the authors. This research is grant-funded by the University of Minnesota Press. Regarding conflicts of interest, Anthony Tarescavage, Danielle Burchett, Martin Sellbom, and Yossef Ben-Porath receive research funding from the MMPI-2-RF test publisher, the University of Minnesota Press. Martin Sellbom is a paid consultant to the University of Minnesota Press. He also teaches workshops and webinars on the MMPI-2-RF for remuneration. Yossef Ben-Porath is a paid consultant to the University of Minnesota Press and Pearson. As co-author of the MMPI-2-RF he receives royalties on sales of the test.