
Abstract
The prison-based Therapeutic Community (TC) is a promising substance use treatment program that emphasizes peer influence. Although program evaluations demonstrate positive results, the cognitive, behavioral, and social processes that define the prison-based TC are largely unknown. The TC model presumes that residents increase their treatment engagement and willingness to change through peer interactions and role modeling, but this process has received virtually no research attention. This study explores these peer-driven mechanisms by examining self, reflected, and peer appraisals of willingness to change of 177 male TC residents, predicting within-person changes in treatment engagement by changes in appraisal measures. Results suggest that self, peer, and reflected appraisals converge over time in treatment. In addition, fixed effects models demonstrate that changes in reflected appraisals are most predictive of changes in treatment engagement. Such results, consistent with symbolic interactionist perspectives, inform prison-based programming and contribute to research on individual-level trajectories of desistance and recovery.
In 2017, more than 620,000 individuals left state and federal prisons and reentered their communities, a number that will persist or even grow as America exits the recent era of mass incarceration (Bronson & Carson, 2019). It is estimated that approximately three quarters of these released individuals will recidivate within 5 years, and that substance use disorders (SUDs) contribute significantly to this recidivism (Durose et al., 2014). The prevalence of SUDs is significantly higher among incarcerated populations, at approximately 65% (The National Center on Addiction and Substance Abuse at Columbia University, 2010), than among the general American population, at approximately 8.4% (Center for Behavioral Health Statistics and Quality, 2015). Yet it is estimated that less than a quarter of those incarcerated who need SUD treatment receive any during their incarceration (Belenko & Peugh, 2005; Taxman et al., 2007). Repairing this detrimental gap in services is fundamental for reducing recidivism and facilitating successful community reentry.
The inadequate attention given to SUDs in prison-based programming is reflected in program evaluation, with sparse research on drug treatment among incarcerated individuals (Travis et al., 2014). When program evaluations and meta-analyses are conducted, findings do not necessarily translate into prison practice, as surveys indicate that few correctional facilities utilize evidence-based drug treatment programs (Chandler et al., 2009). In addition, a more thorough understanding of processes of desistance from crime and substance use is needed to better tailor in-prison treatment programs to the needs of individuals and to reduce recidivism rates. Although some evaluations of programs work toward this aim, the mechanisms of individual change that are pertinent for desistance, and if and how such mechanisms are present in various treatment programs, have not been adequately parsed out.
For example, the prison-based Therapeutic Community (TC) is a widely used substance abuse treatment program that evaluations have consistently found to be effective at reducing recidivism (Mitchell et al., 2012). Despite promising evidence, research has not adequately explored the mechanisms underlying this treatment modality. Without such research, it is difficult to evaluate which elements of treatment are effective and how to improve the program to further reduce relapse and recidivism. George De Leon (2000), a preeminent expert in TCs, states the following in his seminal monograph on TC philosophy:
Although much is known about whether TCs work in terms of successful outcomes, less is understood as to why and how TCs work. The link between treatment elements, treatment experiences, and treatment outcomes must be established to firmly substantiate the specific contribution of the TC to long-term recoveries. (p. 5, emphasis in original)
The current study addresses this recognized gap by utilizing 10 waves of longitudinal data to analyze within-person change in various appraisals of resident willingness to change across 4 months of prison-based TC treatment. In addition to assessing the mechanisms of individual change, this research contributes to discussions of theories of desistance, parsing out the elements of internal change or external support that are crucial in cessation of criminal behavior and substance use. This study examines life course theories of desistance and concepts rooted in symbolic interactionism through the lens of individual processes of recovery. An innovative longitudinal dataset collected over 10 months in a prison-based TC enables a more thorough understanding of individual-level and unit-level changes and a more accurate picture of the social dynamics of the TC unit.
The Therapeutic Community
The TC is an intensive inpatient program that utilizes a community-as-method approach (De Leon, 2000). Residents are expected to become embedded within the community over time and, throughout the course of their own recovery, assist in the recovery processes of their peers (De Leon, 2000). The TC model relies heavily on social learning mechanisms, specifically peer influence, which are mechanisms of particular interest when considering the model within a prison context. The confined nature of a prison TC, and the resulting elevated levels of peer interaction, increases the accuracy and usefulness of peer appraisals as a measure of resident change. These features also increase the potential strength of peer influence, which could contribute to a well-functioning TC or, alternatively, to negative social learning as predicted by the “school of crime” hypothesis (Miller & Ohlin, 1985; Nguyen et al., 2017). The composition of the TC unit, that is the behaviors and attitudes of the current residents, determines which of these disparate pathways social learning effects will follow. Assessment of the treatment engagement and motivation for change among TC residents can predict the pathway of social learning effects.
George De Leon (2000), author of the comprehensive TC resource handbook The Therapeutic Community: Theory, Model, and Method, argues that genuine participant engagement in TC treatment is essential for both success in treatment and long-term sobriety (De Leon, 2000). Prison-based TCs have been evaluated and participant engagement measured using scales such as the Client Assessment Summary (CAS; Kressel & De Leon, 1997) and the Staff Assessment Summary (SAS; De Leon & Kressel, 1997). Self-reported treatment engagement measures are undoubtedly useful, but the potential effects of social desirability are inflated within a prison-based TC, especially considering successful program completion is often a requirement for parole. Staff assessments are more objective, but still do not capture the most accurate measures of individual participant engagement within the community-as-method approach of the TC.
In the community-as-method model, TC residents are intended to be the primary source of feedback for their peers throughout treatment, affirming and correcting peer behaviors and attitudes. Residents are expected to transition into leaders and role models within the community over time as they replace antisocial thoughts and behaviors with prosocial ones. Through countless daily interactions between residents, program-necessitated evaluations of peer behavior, and group treatment experiences, peer evaluations of participant engagement are arguably the most accurate measure within a prison-based TC due to the community-as-method model. Peer evaluations also result in multiple points of data per resident, reducing the impact of any single biased appraisal and allowing trends to emerge through aligning peer perceptions.
While many TC graduates exemplify the success of the program with criminal desistance and sobriety upon reentry, there are at least an equal number of participants who do not experience such successes (see Welsh & Zajac, 2013). A more thorough understanding of the cognitive, behavioral, and social processes that transpire within the prison-based TC, and the differences between desisting and relapsing TC graduates, enables better tailoring to the strengths and needs of participants. George De Leon (2000) asserts:
Illuminating the treatment process is essential for improving the TC treatment itself. Thus, wise modification of the approach must be guided by an understanding of the active “ingredients” in the treatment model, the course of recovery, and the complexity of individual change. (p. 5)
Despite a lack of understanding regarding precisely how TCs foster recovery and desistance, evaluations of their aggregate effectiveness have been largely positive (Sacks et al., 2012; Welsh & Zajac, 2013). Bahr et al. (2012) discuss the results of eight evaluations of TCs in various states, concluding that well-executed TCs can be “effective in reducing the risk of drug relapse and rearrest” (p. 160). Similarly, a comprehensive meta-analytic review of incarceration-based drug treatment programs found that TCs most consistently reduced relapse and recidivism (Mitchell et al., 2012). These evaluations demonstrate the promise of prison-based TCs, yet a gap in research exists regarding what mechanisms are benefiting TC participants, increasing their engagement, and fostering positive long-term outcomes.
The mechanisms underlying effective TC treatment can be uncovered through evaluation of one’s self-reported “willingness to change” as they progress through treatment, and whether that perception matches peer evaluations. Such an evaluation can assess if expected increases in self-awareness and positive role modeling are coming into fruition through engagement in treatment. In addition to self-reported and peer-evaluated willingness to change, a reflected appraisal measure is included to further parse out mechanisms of individual change and peer influence. Reflected appraisals, or how an individual perceives the actual appraisals of others, enable evaluation of processes of peer influence that affect self-concept or identity. Determining the relationship between three appraisals of willingness to change sheds light on processes of within-person longitudinal change and peer influence within the TC treatment model.
Symbolic Interactionism and Identity Change
Given its embeddedness in peer influence, the TC relies on processes of learning and change rooted in symbolic interactionism. Symbolic interactionism asserts that humans live in symbolic environments as well as physical environments, influenced by “symbols” or stimuli with learned meanings and values (Mead, 1934; Rose, 1962). Individuals learn meanings, values, and ways of acting from others through symbolic communication and gestures. The conceptualization of one’s identity or sense of self as arising from iterations of social learning is highly relevant within the context and philosophy of a prison-based TC.
Reflected appraisals represent one pivotal way in which society shapes the “self.” The concept of reflected appraisals can be traced to 1902 with Cooley’s “looking-glass self,” in which individuals imagine how they appear to others, react to the imagined judgment of that appearance, and shape their identity through that perceived judgment. Scholars in various fields have evaluated reflected appraisals since Cooley’s work, finding that while our perceptions of how others see us are not necessarily accurate, they nevertheless influence behavior (Alvarez & Helms, 2001; Bouchey & Harter, 2005; Matsueda, 1992).
Asencio’s (2011) research within a medium-security prison demonstrated that reflected appraisals from family members and incarcerated peers have a significant influence on an individual’s self-appraisal of their criminality. Asencio (2013) additionally explains how self-esteem moderates reflected appraisals within incarcerated populations, with those measuring high on self-esteem reporting reflected appraisals that more closely align with actual peer appraisals than those with low self-esteem. These findings suggest that the progression of a TC participant’s reflected appraisal of willingness to change throughout treatment influences their self-appraisal and overall identity. As participants progress through the TC, the transformation of antisocial tendencies should be reflected in increased self-esteem and, subsequently, closer alignment of reflected and peer appraisals (Asencio, 2013). Additional individual-level changes that should result from active engagement in TC treatment, such as increased self-awareness and community cohesion, should contribute to this alignment over time. As such, residents for whom reflected and peer appraisals do align throughout treatment are predicted to be more engaged in TC treatment and to experience greater success both in the program and post-release.
The Therapeutic Community as a Life Course Turning Point
Sampson and Laub (2003) consider social role transitions, such as entrance into marriage or parenthood, and how becoming socially embedded with prosocial peers can encourage desistance. Although these role transitions often result in desistance, they are typically beyond the control of policy intervention, which makes the prison-based TC an important area of research. For Sampson and Laub, participation in a prison-based TC would be a turning point, providing stability and support while the individual becomes socially embedded with prosocial peers. Within their age-graded theory of informal social control, TC participation alone should set residents on a path to desistance, providing there is community support and prosocial peers. While agency is taken into consideration in later iterations of their theory, the primary impetuses of change are external sources of informal social control when assessing social role transitions. Agency and internal cognitive changes are not necessary or sufficient impetuses of desistance for Sampson and Laub, and these processes are framed as responses to entrance into prosocial roles.
Sampson and Laub (2003) hypothesize that life course transitions are exogenous to individuals, which suggests that success for TC residents hinges on experiencing a prison-based TC as a turning point. Other theories of desistance emphasize the importance of agency in the process of identity transformation (Giordano et al., 2002; Maruna, 2001). Giordano et al.’s (2002) theory of cognitive transformation, a symbolic interactionist approach to desistance, would consider participation in a prison-based treatment program as a “hook for change,” or a prosocial catalyst for change. In this perspective, desistance rests upon the actor’s role in latching onto such a catalyst by being receptive to change and perceiving the hook as salient. Only with such a combination of factors can the individual begin to envision a “replacement self,” leaving behind a now irrelevant deviant self, and moving forward as their envisioned self. Giordano et al.’s (2002) theory predicts improved treatment engagement and long-term success for individuals who develop into self-aware, positive community members during TC treatment.
While these theories of desistance are, of course, relevant to the residents of the prison-based TC, the presence of SUDs and criminal behavior in tandem complicates evaluation of behavioral change. Desistance and recovery are complex processes individually, and are even more complex when occurring together (Colman & Vander Laenen, 2012; Ti et al., 2014). Recovery is a gradual process that, when attained, takes years or even decades to stably achieve (Dennis et al., 2014; Hser et al., 2015; McLellan et al., 2000). The mechanisms of change underlying effective treatment and successful recovery are difficult to pinpoint (Black & Chung, 2014; Kazdin, 2007), yet prior research has emphasized the fundamental role of social processes and peer-based mechanisms, including social learning, social control, and prosocial peer networks (Best et al., 2016; Litt et al., 2009; Moos, 2007).
Recognizing the complexity of behavioral change and the difficulty in measuring such processes, longitudinal measures from TC residents contribute to the disentangling of social processes of treatment within a prison-based TC. This study presents an innovative approach to tracing social and cognitive paths to desistance, measuring what changes emerge in prison-based treatment for residents at varying levels of engagement. To determine whether expected increases in self-awareness and decreases in antisocial traits transpire through engagement in TC treatment, these desistance processes are illuminated through a longitudinal measure of one’s perceived willingness to change as they progress through the TC, and whether that perception matches peer evaluations of willingness to change. When linked to treatment engagement, these longitudinal measures shed light on the individualized process between a hook for change and post-release outcomes.
The Present Study
The Therapeutic Community Prison Inmate Networks Study (TC-PINS: PI Kreager) data collected over 10 months in a prison TC enable the comparison of self, reflected, and peer appraisals of individual residents’ willingness to change as those residents progress through 4 months of TC treatment. Participants who become more invested and embedded in the community throughout their time in the program, as is required of effective TC treatment, should have self and reflected appraisals that more closely align with the evaluations of their peers. As TC residents progress through their months of treatment, they are intended to recognize and alter their antisocial personality traits, become more self-aware, and develop higher self-esteem. These processes, in tandem with the community cohesion of the TC unit, should contribute to bringing self-appraisal and reflected appraisal measures into alignment with peer appraisals. In addition, the community-as-method approach should foster self-disclosure and bonding between residents, enabling them to evaluate one another more accurately over time.
In addition to the logistical aspects of the unit that contribute to the usefulness and accuracy of peer appraisals, such appraisals reflect the intended model of the TC. The community-as-method model hinges on peer influence processes, with participation measured by “whether members provide, as well as use, peer observation and feedback” (De Leon, 2000, p. 96). Residents are expected to engage with their peers, identify their attitudes and behaviors that conflict with recovery and right living, and grow in their own recovery through responsible concern for others. This process requires interaction with peers and awareness of peer progress in recovery, which implies appraisal alignment over time.
Hypothesis 1: Self-appraisals, reflected appraisals, and peer appraisals of willingness to change will converge over 4 months of TC treatment as residents gain deeper understanding of their peers.
An intensive prosocial community environment is the most suitable context for evaluating these individual trajectories, especially in attempting to overcome potential self-report biases within a prison-based treatment context due to parole requirements. Consistent with symbolic interactionism, peer evaluations and peer-influenced perceptions (i.e., reflected appraisals) will be more accurate and more predictive of long-term desistance in a small, intensive treatment setting, such as a prison-based TC.
Determining which of these three appraisals best predict changes in treatment engagement informs our understanding of social, behavioral, and cognitive processes transpiring within the prison-based TC. Taking previous research on reflected appraisals and the isolated and intensive nature of the prison-based TC into consideration, it is predicted that reflected appraisals will have a significant impact on self-concept and behavior in a program based on community-as-method, resulting in reflected appraisals being more predictive of self-reported treatment engagement than self-appraisals. Reflected appraisals represent a blending of self and peer appraisals, capturing elements of both individual agency and social context. Despite isolation of the prison-based TC unit and high levels of daily social interaction, TC peers cannot fully know a fellow resident (e.g., their mind-set, experiences, motivation); therefore, individual agency limits the accuracy of peer appraisals. Self-appraisals, on the other hand, tend to present an idealistic representation of desire to change, an impulsive affirmation of hope for recovery that lacks the realism introduced by considering the more cynical views presented by TC peers, other sources of external identity formation (e.g., family and friends), and society in general. With this lack of realism, self-appraisals are typically high throughout treatment, resulting in minimal variation and low predictive power. Reflected appraisals require the consideration of perceptions from external sources while still allowing room for individual agency, presenting a more conservative and realistic appraisal of willingness to change, accounting for complex social dynamics that shape identity (Asencio, 2011; Asencio & Burke, 2011; Burke, 1991).
Hypothesis 2: Reflected appraisals of willingness to change will be most predictive of self-reported treatment engagement measures.
Conversely, if the community-as-method model is not functioning as intended, it is possible that peer influence mechanisms do not predict within-person changes in treatment engagement and that differences in treatment engagement result from pre-existing individual characteristics and not endogenous treatment effects. If selection drives the treatment process in this unit, minimal change will be observed in the appraisal sources for residents over their 4 months of treatment and peer-influenced appraisals (i.e., reflected and peer) will not have significant predictive power for treatment engagement.
Data and Sample
Data for the National Institutes of Health (NIH)–funded TC-PINS was collected monthly from August 2016 to May 2017 at a medium-security state correctional institution (SCI) in Pennsylvania with five TC units. After approval from the Pennsylvania State University Institutional Review Board (IRB), computer-assisted personal interviews (CAPI) were conducted monthly with residents of one of the TC units (n = 62). Residents who chose to participate completed the CAPI in a confidential setting with the author or another interviewer who read all questions and answer choices to the respondents and provided clarification when necessary. The response rates per wave ranged from 73% to 82% of the unit, combining to a total sample response rate of 84% of eligible respondents completing at least one CAPI.
Over 10 months of data collection, 470 CAPI surveys were administered to 177 respondents. Variable missingness is relatively low (3.8%, n = 18 observations) and is mostly accounted for by missing peer appraisals due to new TC residents not being known by their peers. Missing peer appraisals account for 72% of the missingness (n = 13), with missing reflected appraisals accounting for the remaining 28% (n = 5). Due to the modest amount of missingness, listwise deletion is used in all analyses.
At intake into the state prison system in Pennsylvania, those who score six or above on the TCU Drug Screen II (Institute of Behavioral Research, 2014) are parole-mandated to complete the prison-based TC program. In an attempt to maximum the benefit of the treatment effects on reentry outcomes, the TC program is timed at the end of an individual’s sentence, with minimal time, or often no time, in general population before release. If an individual declines to participate or “signs out” of the TC, they are required to sign their maximum sentence papers, agreeing to serve their maximum sentence instead of being eligible for parole at their minimum sentence. Therefore, the majority of those mandated to the TC agree to participate, whether or not they have any interest in the program, to be eligible for parole at their minimum sentence date. This creates a dynamic of coercion into treatment and removes much of the selection bias potentially resulting from only highly motivated individuals joining the TC unit. Individuals with a score of six or above on their drug screen intake are placed in the TC, creating a respondent sample with ample variation in motivation for recovery and willingness to change.
In Pennsylvania state prisons, the TC program is currently 4 months long, shortened from a longer TC program (i.e., 12 months) of the past. Those 4 months of TC treatment are separated into three phases: Phase 1 (“induction”) lasts 1 month, Phase 2 (“primary treatment”) last 2 months, and Phase 3 (“reentry”) compromises the fourth and final month. Residents enter the unit on a rolling admission system (i.e., residents do not enter as cohorts) and “phase up” based on their entry date. However, many treatment groups are conducted within phase, so residents spend more time with the residents in their phase than those in other phases.
Residents of this prison-based TC unit are isolated from those in general population for the majority of their 4 months on the unit. The TC unit studied houses approximately 62 residents at a time who maintain a high level of interaction in a small space, spending many hours per day in treatment groups, moving to and from meals together, attending the same daily yards, and spending all of their downtime on the TC unit with other residents. Unit residents attend meetings and treatment groups Monday through Friday from 9 a.m. to 4 p.m., with a few breaks for meals and institution-wide counts. Considering the isolation of the unit and the intensity of daily treatment, peer dynamics should be particularly influential in this unit.
Over 10 waves of data collection, a total of 210 residents were on the TC unit during days the CAPI was administered. Of those 210 potential respondents, 177 residents completed at least one CAPI. Unit and sample demographics are described in Table 1. Participation in multiple treatment waves declined per wave: 144 residents participated at two treatment waves, 97 participated at three treatment waves, and 52 completed all four possible treatment waves. Much of this decline across waves was due to the timing of resident treatment (e.g., some were partway through treatment when data collection started or ended), residents being transferred to other TC units before program completion, or discharge from the unit by request or for behavioral reasons. As a result of these factors, only 41% of residents in the sample had all four of their months of treatment overlap with the data collection window.
Unit and Sample Descriptive Statistics
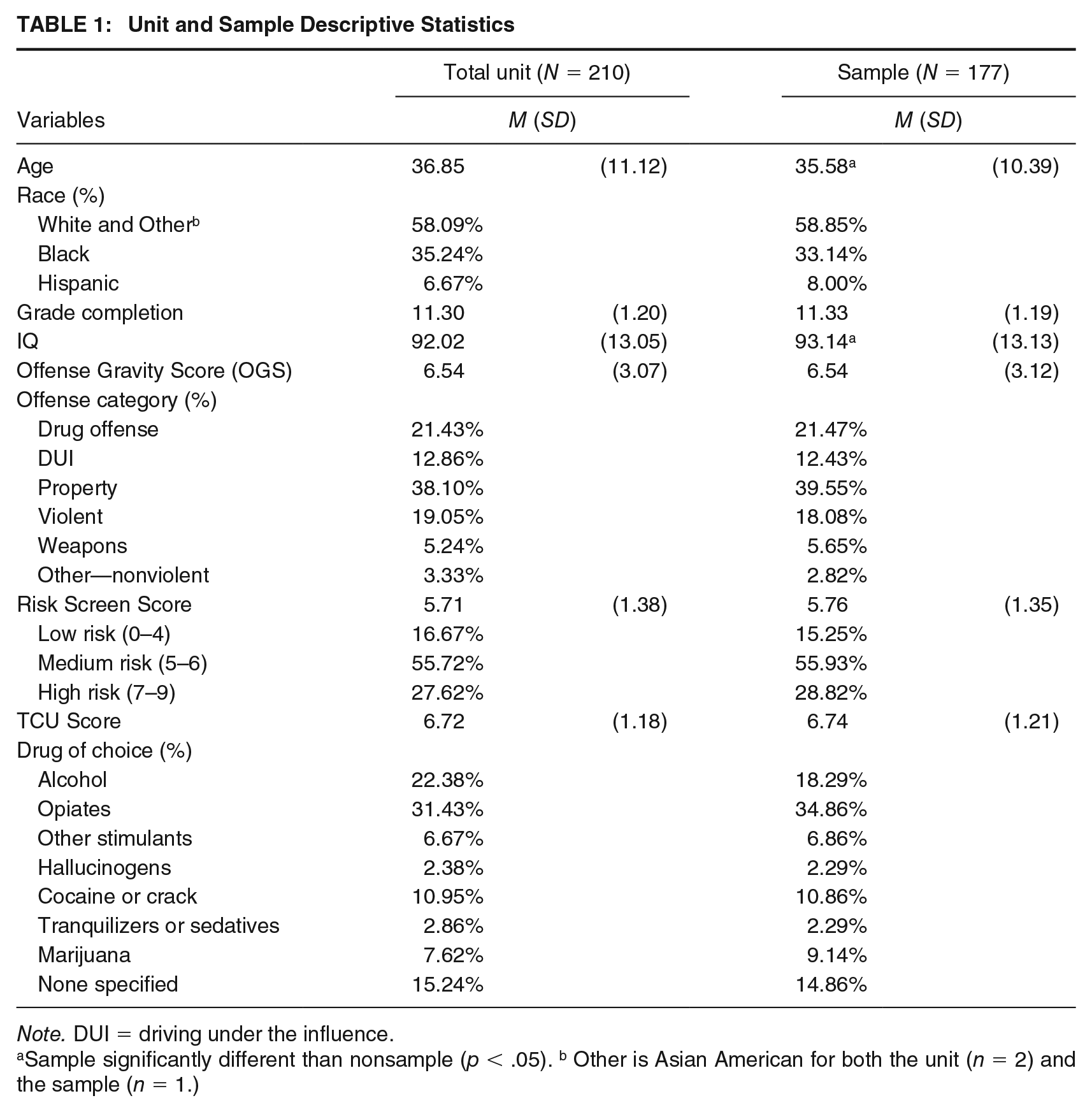
Note. DUI = driving under the influence.
Sample significantly different than nonsample (p < .05). b Other is Asian American for both the unit (n = 2) and the sample (n = 1.)
The race distribution of the TC unit studied is significantly different than the statewide distribution, with a higher percentage of White residents in this unit and in the sample than in all SCIs (Pennsylvania Department of Corrections, 2016). This is possibly a product of the opioid epidemic affecting rural areas of America in recent years, which is reflected in rates of prison admittances from rural Pennsylvania counties over the past several years (Pennsylvania Department of Corrections, 2016). Across all Pennsylvania SCIs, 48% of incarcerated males are Black, 41% are White, and 10% are Hispanic. In contrast, the sampled TC is predominantly White (see Table 1).
The majority of the unit and sample are assessed as medium risk on the Risk Screen Tool used by Pennsylvania Department of Corrections. Nearly 40% of the unit and sample were incarcerated for property offenses, approximately 34% for drug offenses or DUIs, and the remainder for violent, weapons, or other offenses. Drug of choice is measured with the TCU Drug Screen II (Institute of Behavioral Research, 2014), which asks individuals to indicate the substance that is the primary source of their disorder. The largest drug use group in both the unit and the sample is opiates, an unsurprising statistic given the widely acknowledged opioid epidemic. Approximately 15% of the unit and the sample do not specify a primary drug, which may indicate multi-drug use or denial that any single drug is a source of disruption to their daily life and functioning.
Measures
The dependent variable in these analyses is treatment engagement, measured with the CAS, a validated self-reported TC treatment engagement scale developed by TC experts (Kressel & De Leon, 1997; see the Supplemental Appendix, available in the online version of this article). Responses are averaged to create a treatment engagement score with a minimum score of 1.0 to maximum score of 5.0 (α = .86). Self-appraisals, reflected appraisals, and peer appraisals of willingness to change are the primary independent variables and were collected from each TC resident who took the CAPI. Readiness or willingness to change is an important predictor of engagement in substance use treatment (Morgen & Kressel, 2010; Welsh & McGrain, 2008). However, given the frequent use of the phrase “readiness to change” among treatment professionals and TC materials, a more conventional phrasing of willingness or desire to change was used to avoid conflation with engagement in the TC. While “readiness to change” may be equated with commitment to the TC program itself, “want to change” encompasses a broader orientation to change. Thus, the following questions were asked of respondents at every way in which they participated:
Self-appraisal: “On a scale of 0 to 10, how much do you really want to change?
0 = I do not want to change; 10 = I really want to change”
Reflected appraisal: “On a scale of 0 to 10, how much do you think others in the unit believe that you want to change?”
Given concerns about respondent burden due to a lengthy CAPI survey, these items were limited to one item, but this single-item method of measuring reflected appraisals has been established in prior literature (Asencio, 2013; Asencio & Burke, 2011; Matsueda, 1992). These questions, including the peer appraisal question listed below, are worded identically with the exception of the source of the appraisal, as is standard in comparisons of appraisal types (e.g., comparison of self to reflected appraisals, comparison of reflected to actual appraisals) (see Asencio & Burke, 2011; Matsueda, 1992).
The peer-based appraisal measure utilized is derived within phase, with respondents evaluating only the residents in their same phase (i.e., Phase 1, Phase 2, or Phase 3), making these peer appraisal measures less burdensome on respondents and more accurate due to heightened intra-phase interaction. Interaction levels are higher between TC residents within the same phase as treatment groups are often split up by phase. Thus, within the CAPI survey, respondents were asked to rate the peers within their phase on their willingness to change. These ratings were combined across appraisals to create one peer appraisal score per TC participant per wave. With a minimum of 10 within-phase peers to provide an appraisal, and a maximum of over 30 within-phase peers, there is confidence in the validity of this aggregate measure of peer appraisals.
Peer appraisals: “This is a list of the residents in your phase. On a scale of 0 to 10, how much do the residents in your phase really want to change?”
Demographic variables from official Department of Corrections (DOC) data include age, race/ethnicity, highest completed grade, IQ, TCU Drug Screen Score (scale from 1 to 9), drug of choice, and Offense Gravity Score (scale from 1 to 18). These demographic variables are utilized to determine whether the dynamics of these three appraisals and their relationship to changes in treatment engagement vary by time-stable characteristics. Given previous literature on race effects of TC treatment (Kerrison, 2018), it is possible that such characteristics influence the mechanisms underlying TC treatment.
Analytic Strategy
First, the trends of these three appraisals (self, reflected, and peer) are assessed across Treatment Wave, or each month of TC treatment (1–4), to test Hypothesis 1. The alignment of appraisals for those residents who completed a CAPI survey in each month of their TC treatment (i.e., completed four CAPIs) are analyzed for convergence across treatment months. Second, to test Hypothesis 2, the three appraisal sources are used to predict treatment engagement within fixed effects models to determine which processes of change best predict engagement in treatment over time. Fixed effects models account for the influence of unobserved time-invariant selection variables. By focusing only on within-person variation in independent and dependent variables across time, fixed effects models eliminate bias introduced by time-stable unobserved individual-level factors that are related to observed variables. In these models, fixed effects account for unobserved variables that could potentially bias appraisal sources and treatment measures such as personality characteristics (e.g., gregariousness, malleability) and historical personal experiences (e.g., participation in other treatment programs, childhood trauma).
Results
Due to the community-as-method model of the TC, the three appraisal sources should align throughout 4 months of treatment, reflecting unit-level community cohesion and individual-level increases in self-esteem and self-awareness. To test Hypothesis 1, the aggregate appraisal trends are evaluated across Treatment Wave (see Table 2).
Variable Means by Treatment Wave
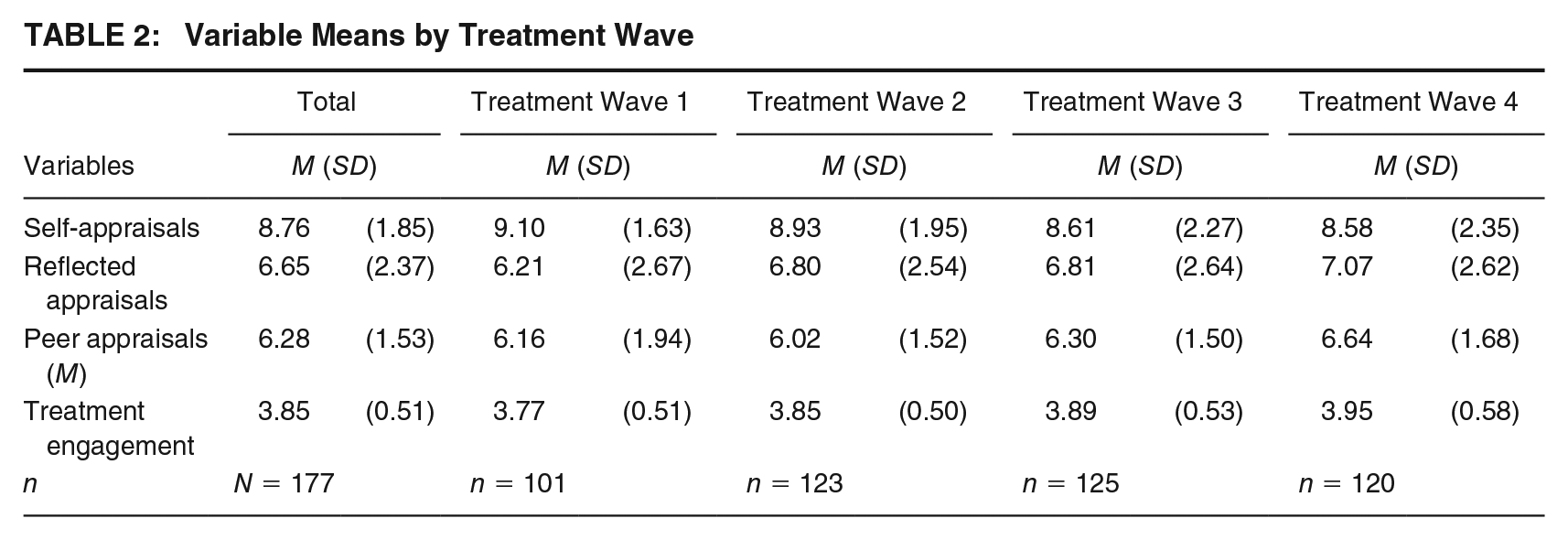
In the observed data, self-appraisals decline across each Treatment Wave, while reflected appraisals increase in each Treatment Wave. As residents progress through the TC, they rate their own willingness to change more conservatively while simultaneously seeing their recovery identity more positively from the assumed perspective of their TC peers. Declining self-appraisals may seem counterintuitive to TC treatment aims, but in reality this trajectory is likely a positive result of residents becoming more self-aware and developing more realistic expectations regarding their recovery timeline and long-term goals through TC curriculum. TC groups include themes of realistic expectations, and residents are encouraged to recognize the enduring and challenging work required to maintain sobriety. In addition, TC treatment emphasizes the broad scale changes in behavior and identity that are required for success in recovery long-term. Internalization of these treatment themes would result in more conservative appraisals of one’s own willingness to change.
On an aggregate level, TC residents perceive their peers to be more willing to change as they phase up and complete the program, which suggests that residents are demonstrating attitudes and behaviors more aligned with recovery over time in treatment. In combination, these sample-level appraisal trajectories result in self, reflected, and peer appraisals converging across each Treatment Wave (1–4), offering support for Hypothesis 1. Figure 1 shows longitudinal mean values of the appraisal variables for those respondents who completed a CAPI during all four of their Treatment Waves (n = 52). Treatment engagement is included in Figure 1 to assess whether this validated measure of engagement coincides with trends in willingness to change appraisals across waves. Average treatment engagement increases over time in treatment, which does coincide with the general trends of both peer and reflected appraisals (self-appraisals decrease over time in treatment, as previously discussed). The increase in treatment engagement, peer, and reflected appraisals across waves illustrates that residents become more engaged in the TC over time in treatment and demonstrate observable progress, which is recognized by their peers.
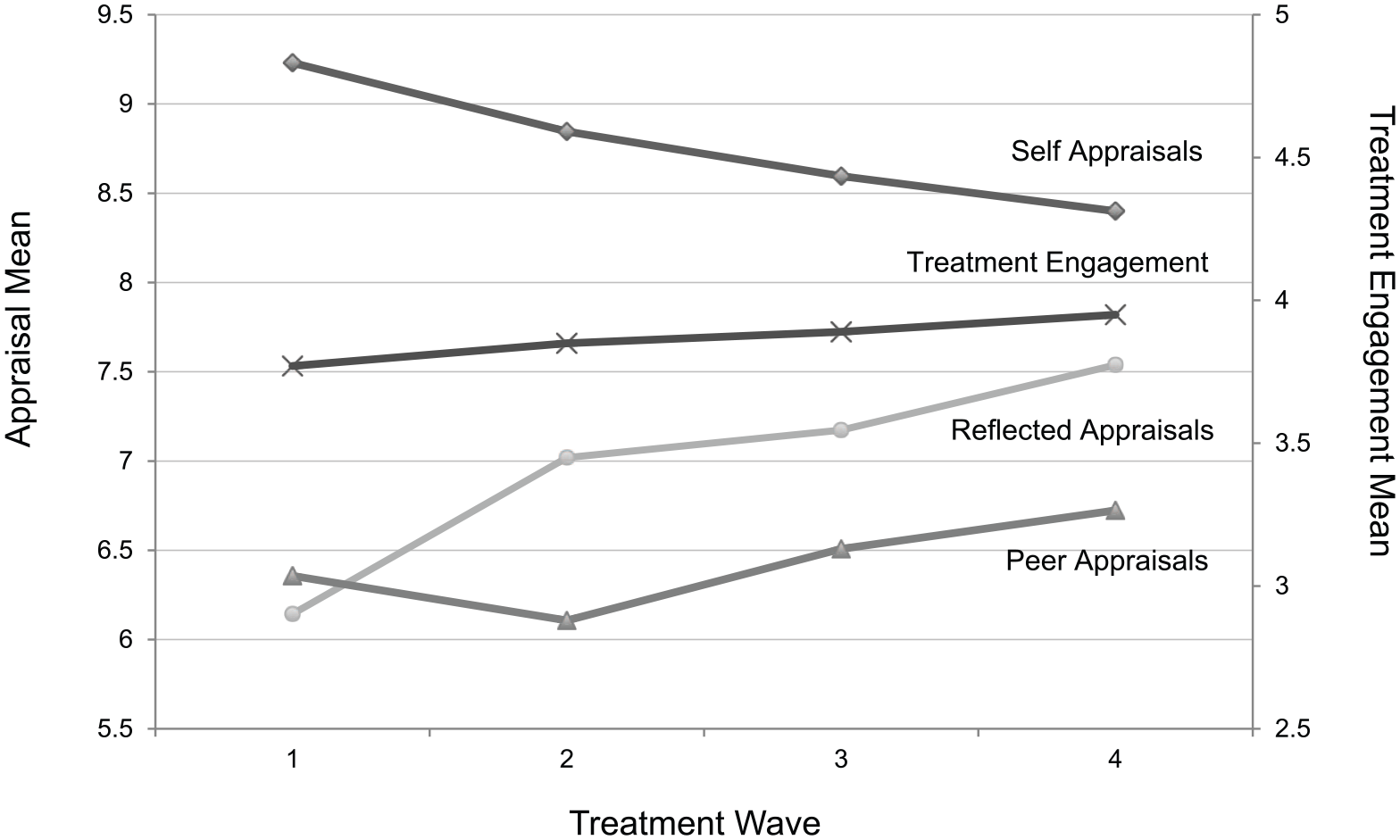
Appraisal Alignment and Treatment Engagement Across Treatment Waves (n = 52)
Table 3 lists estimates from fixed effects models of the bivariate associations between the three appraisal variables and treatment engagement before estimating a full model that includes all three appraisals. To account for time trends, the measure of Treatment Wave is included. Its coefficient is significant and positive, suggesting that treatment engagement tends to increase over resident time in the program. When all three appraisals are included in the model, only changes in reflected appraisals maintain statistical significance in predicting changes in treatment engagement over time, supporting Hypothesis 2.
Fixed Effects Regressions of Appraisals on Treatment Engagement (N = 452)
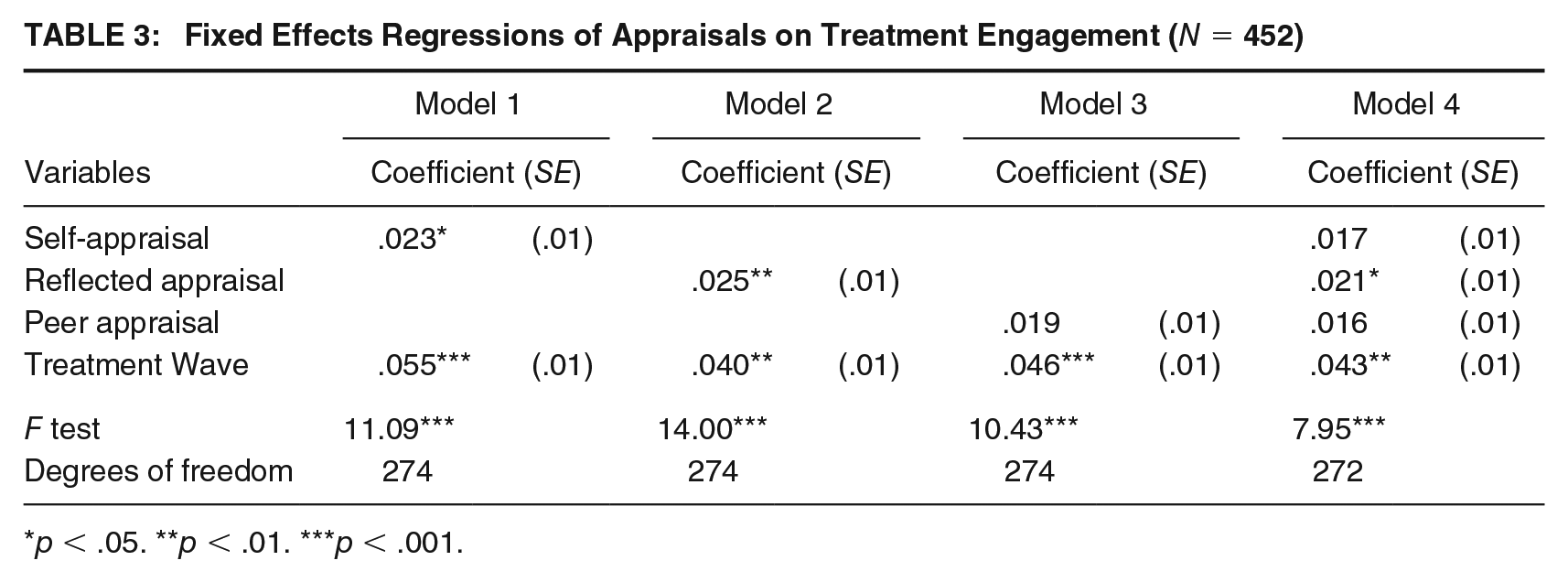
p < .05. **p < .01. ***p < .001.
A purely selection-driven process of recovery, as opposed to the presence of at least some elements of the community-as-method approach, would result in null estimates in fixed effects models. Baseline measures would be fully predictive of treatment engagement, and within-person changes would be statistically nonsignificant. Significant reflected appraisal estimates indicate that individual-level change in this TC unit is not entirely fueled by selection.
Treatment Wave interaction terms were included in additional analyses to determine whether the effects of any appraisal type varied across time in treatment. Given the community-as-method model of the TC, it would be unsurprising if peer-based appraisal measures became more strongly predictive of treatment engagement over 4 months of treatment. However, these terms were nonsignificant in all models (results available upon request). In addition, interactions between the appraisal variables and time-invariant variables, including age, race/ethnicity, drug of choice, TCU score, and Offense Gravity Score, were estimated and none reached statistical significance (results available upon request). Separate fixed effects models were also estimated with the following unit subsets: White versus non-White residents, younger versus older residents, those with less than a high school degree versus those with high school or more, and those with TCU scores below seven versus those at seven or above (results available upon request). In all separated demographic models, z tests indicate that the differences between coefficients are not statistically significant (see Paternoster et al., 1998).
The possibility of reverse causality also exists within these fixed effects models, as changes in treatment engagement may influence changes in appraisals. Fixed effects models with lagged independent variables were examined to determine time-order (results available upon request). As expected, the coefficients for all three appraisal sources decreased in magnitude and significance, but the relative pattern among the variables held across all models. Further analyses are needed to better parse out these time-dependent effects.
Discussion
Prison-based TCs are utilized in approximately 30% of prisons nationwide (Taxman et al., 2007), yet the mechanisms that separate TC participants who benefit from treatment and progress in recovery from those who do not are not understood. This study takes steps toward a better understanding of processes of change within a prison-based TC to enable improved program implementation and greater success for participants. The traditional TC program is at least 12 months long (De Leon, 2000), and many evaluations of prison-based TCs assessed programs of that length (Welsh & Zajac, 2013). Many states are trending toward shorter TCs, often to reduce treatment costs; a growing percentage of prison-based TCs are 4 months long or even shorter. In 2007, Taxman et al. reported that a third of prison-based TC programs were 90 days or shorter and additional programs have been shortened since then, including those in Pennsylvania prisons. The effects of these modifications have not been adequately evaluated, but there is evidence that inconsistencies across treatment programs result in variant effects in reentry outcomes (Jensen & Kane, 2012; Zhang et al., 2011).
The results of this study indicate that peer influence processes are driving factors within prison-based TC treatment, both directly (i.e., peer appraisals) and when filtered through resident perceptions (i.e., reflected appraisals). These processes change within person over time in the treatment program. In addition, prison-based TC treatment does not appear to be fueled entirely by selection, which indicates that this form of treatment intervention can alter individual attitudes and likely affect trajectories of desistance. Considering the coercive nature of this TC, given that parole eligibility hinges on participation, a purely selection-driven pattern would not have been surprising. There is mixed evidence regarding the effectiveness of coercion into treatment in existing literature (Parhar et al., 2008; Zhang et al., 2013), and more research attention should be devoted to understanding the effects of mandated treatment. Although participation in this TC was largely fueled by the threat of serving maximum sentences, these results illustrate that the peer-driven TC model impacted participants despite their coercion into treatment.
Given the current nationwide drug epidemic and high rates of recidivism, a better understanding of processes of recovery and desistance for individuals with SUDs is an important step toward improving programming and fostering greater success in reentry. This research works to fill that gap by illuminating core, and previously unmeasured, aspects of the TC philosophy. These results contribute to George De Leon’s call for a better understanding of how and why the TC model can be effective for participants (De Leon, 2000). Fixed effects models indicate that concepts rooted in symbolic interactionism, such as reflected appraisals, are important when evaluating changes in attitudes, behaviors, and identity that accompany processes of recovery and desistance. The self develops through social interaction and identities exist within contexts, which makes the evaluation of peer influence on changing identities in treatment and recovery processes important in reducing rates of recidivism and relapse.
These results are also supportive of cognitive theories of desistance, such as cognitive transformation, which is rooted in symbolic interactionist principles. The exogenous appraisal source (i.e., peer appraisals) was not significantly predictive of change in treatment engagement in these fixed effects models. Instead it was reflected appraisals, which blend agentic thinking with an externally imposed treatment community or “hook for change,” that were most predictive of within-person change over time in treatment. This illustrates that the process of recognizing a hook for change, internalizing it to some degree, and allowing external influence to shape self-concept is an important element of within-person change in this TC unit.
While the mechanisms underlying any TC treatment are expected to be similar across prison units and across states, generalizability of findings is a limitation of this research. This calls for replication of this research in TC units in other states, especially states with substantial differences in programming and longer TC programs. De Leon (2000) outlines the recommended 12-month TC program, and it is probable that the shorter TC program is not as effective, particularly when analyzing change in treatment investment, identity, prosocial attitudes and behaviors, and self-awareness. Indeed, George De Leon conducted a fidelity assessment of the unit studied, reporting low-medium fidelity and citing institutional barriers and staff training as detriments to the intended model (Kreager et al., 2018).
Due to administrative data restrictions and respondent burden concerns, the descriptive measures for the sample are somewhat two-dimensional, lacking more holistic measures of the TC participants like cultural affiliation, which would certainly affect the manner in which TC residents engage with their peers and their treatment. Psychological assessment measures were also unavailable due to Health Insurance Portability and Accountability Act (HIPAA) laws, which is a limitation given the high rates of comorbidity of SUDs and mental health diagnoses (Ross & Peselow, 2012). However, the use of fixed effects tempers these concerns, as the models account for unobserved, individual-level measures that are time-invariant. Bias from unobserved measures, such as mental health diagnoses and cultural affiliation, is eliminated (assuming that these factors are stable across a resident’s 4 months of prison-based TC treatment, which is a reasonable assumption).
Nonrespondents in this study were, on average, older residents who had slightly lower IQs, potentially affecting the generalizability of these findings. However, survey respondents were able to appraise willingness to change for all TC residents, not just those who completed the CAPI, minimizing the detriment of these missing data. In addition, official DOC data will provide measures of contact with the criminal justice system post-release, providing measures of post-release success. These longer term trajectories will be evaluated in future analyses, connecting patterns observed during TC treatment with reentry outcomes, further illuminating processes of desistance or recidivism for individuals with histories of SUDs.
Given that the outcome of interest is self-reported, it would not be surprising if self-appraisals were the best predictor of self-reported treatment engagement, yet this is not the case in the fixed effects models. It is logical to assume that residents would rate their treatment engagement according to their internalized sense of dedication to change and recovery. However, despite the challenges a prison-based treatment environment poses in terms of encouraging resident vulnerability and personal disclosure (Davidson & Young, 2019), peer-based effects appear to be present and statistically significant in a prosocial direction in this particular TC unit.
Despite these environmental hurdles and research limitations, this research is an important step toward a better understanding of the mechanisms of prison-based TC treatment, and why some residents have higher engagement and experience more progress in their recovery than others. Many differences exist in prison-based TCs across correctional facilities and across states. Determining how specific “treatment elements” (De Leon, 2000, p. 5) are impacting prison-based TC residents opens the door for improvement in prison-based TC implementation and greater rates of long-term success for graduates. Processes of behavioral change are gradual and complex, making evaluation of treatment program mechanisms and individual-level progress particularly challenging. This research begins to uncover the mechanisms underlying effective prison-based TC treatment, illuminating the intertwining processes of peer influence and within-person trajectories of change.
Supplemental Material
Appendix – Supplemental material for Testing an Interactionist Theory of Treatment Engagement in a Pennsylvania Prison-Based Therapeutic Community
Supplemental material, Appendix for Testing an Interactionist Theory of Treatment Engagement in a Pennsylvania Prison-Based Therapeutic Community by Kimberly M. Davidson in Criminal Justice and Behavior
Footnotes
Author’s Note:
The author would like to thank the Criminal Justice Research Center at the Pennsylvania State University (PSU) for support and Dr. Derek Kreager and anonymous reviewers for their helpful suggestions. The Therapeutic Community Prison Inmate Networks Study (TC-PINS) is funded by the National Institutes of Health (PI: Derek Kreager; Award Number R21AA023210).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.