
Abstract
Psychopathy and borderline personality disorder (BPD) are commonly associated with an increased propensity toward substance use. However, few studies have accounted for shared variance between psychopathy and BPD when examining relationships with unique forms of substance use, particularly in justice-involved females. This study investigated psychopathic and BPD traits in relation to alcohol and drug use in a sample of 274 incarcerated adult females. Results revealed that psychopathic and BPD traits were differentially related to alcohol and drug use. Specifically, unique variance in BPD traits was related to alcohol use, whereas unique variance in lifestyle-antisocial psychopathic traits was related to drug use. Findings support unique relationships between psychopathic and BPD traits and problematic and prolonged alcohol and drug use in incarcerated adult females. Results may inform methods of tailoring specific substance use treatments for use in females with distinct personality profiles.
Substance use is estimated to cost the United States $740 billion dollars annually (National Drug Intelligence Center, 2011; National Institute on Drug Abuse, 2017). It places significant burden on the criminal justice system, with roughly 85% of incarcerated persons having histories of substance use and/or being imprisoned for a substance-related reason (The National Center on Addiction and Substance Abuse at Columbia University, 2010). Drug policy changes have led to drastic increases in substance-related offending. Despite consequences across gender, these changes have disproportionately affected females, causing some to describe the “War on Drugs” as the “War on Women” (Chesney-Lind & Pasko, 2004; Javdani et al., 2011b). In fact, in 2017, the most serious offense for 28% of incarcerated females was substance-related, while the same was true for only 15% of incarcerated males (Carson, 2020). Accordingly, research on risk factors for substance use in females holds notable implications for the criminal justice system.
Substance use is commonly implicated in female pathways to offending (Bloom et al., 2004; Broidy et al., 2018). The feminist pathways literature has shown that relative to males, females likely have distinct paths to offending and recidivism (Chesney-Lind & Pasko, 2013). This work sheds light on interacting psychosocial factors (e.g., trauma, mental illness, substance use, relational dysfunction) that are particularly relevant to female involvement in the system (Chesney-Lind & Pasko, 2013). Specifically, the pathways perspective posits that early trauma indirectly relates to offending via status offenses, psychopathology, and substance use (Benedini & Fagan, 2020; Bozzay et al., 2020). Accordingly, substance use likely plays a more integral role in understanding offending in females than males, as females may engage in substance use to cope with trauma and psychopathology (Chesney-Lind & Pasko, 2013; Moe, 2006). Substance use reflects direct and indirect routes into the system. As for the latter, females report being under the influence of substance(s) during offenses and/or engaging in crime (e.g., prostitution) to support their use (Carson, 2015; Young & Boyd, 2000). Substance use also contributes to high recidivism rates, also referred to as a revolving prison door, in females (Scott et al., 2014).
Researchers have expanded their view of female pathways to offending to include other individual-level features, including pathological personality traits, as risk factors (Javdani et al., 2011a). In particular, studies have implicated psychopathy and Cluster B personality disorders, most notably borderline personality disorder (BPD), as pertinent to substance use and antisocial outcomes in females (Edwards, Carre, et al., 2019). Aligning with female pathways literature, early trauma has been linked to behavioral and emotional dysregulation in females, and elevated dysregulation has been associated with personality pathology, including psychopathy and BPD, substance use, and antisocial outcomes in females (Chapman, 2019; Edwards, Carre, et al., 2019; Hicks et al., 2010; Hien et al., 2005). Interpersonal contexts are also key to understanding antisociality in females, and females are more likely than males to express psychopathic and BPD traits in interpersonal contexts (e.g., sex work, partner/child aggression; Javdani et al., 2011a; Lazarus et al., 2014). Given the relevance of substance use to female offending, studies testing individual-level risk factors for substance use is deserving of further empirical attention.
Psychopathy and BPD have traditionally been conceptualized as distinct. However, evidence of their comorbidity, along with emerging dimensional models of personality, has shifted focus from unique symptoms in each to shared traits between them (e.g., disinhibition; Edwards et al., 2017; Miller et al., 2010). Dimensional personality models have been proposed as more informative than traditional diagnostic categories in understanding behavioral outcomes (e.g., substance use) and advancing clinical decision-making (Kotov et al., 2018; Lowe & Widiger, 2009). In line with this, shared trait vulnerabilities between psychopathy and BPD (e.g., disinhibition) may help to explain relationships with substance use (Jones et al., 2013; Krueger et al., 2007). However, studies often continue to conceptualize psychopathy and BPD as distinct based on the traditional categorical model (Trull & Durrett, 2005; Trull et al., 2007). To inform this debate, this study utilizes a sample of incarcerated females to explore the extent to which unique versus shared variance in psychopathy and BPD help to account for relationships with substance use. This study holds important treatment and criminal justice implications for females, such that incorporation of interventions designed to target distinct personality pathology may be useful in also reducing substance use and recidivism in this population.
Psychopathy and Substance Use
Psychopathy is characterized by a collection of interpersonal-affective and dysfunctional behavioral traits (Hare, 2003). Psychopathy is commonly assessed using the expert-rated Hare Psychopathy Checklist–Revised (PCL-R; Hare, 2003). PCL-R factor analyses have revealed two distinct, yet related dimensions. Factor 1 reflects interpersonal-affective traits (i.e., glibness, callousness) and Factor 2 reflects developmental-lifestyle-antisocial traits (i.e., child, adolescent, adult behavioral problems, impulsivity, poor decision-making; Hare & Neumann, 2006). Individuals with elevated psychopathic traits tend to display heightened patterns of alcohol and drug use, along with earlier onset of use, compared to those with lower trait levels (Corrado et al., 2004; Hemphill et al., 1994; Smith & Newman, 1990; Taylor & Lang, 2006; Walsh et al., 2007). Studies in males have observed positive relationships between PCL-R Factor 2 (lifestyle-antisocial traits) and drug use (Brennan et al., 2017; Dargis et al., 2017; Hemphill et al., 1994; Mailloux et al., 1997; Smith & Newman, 1990; Walsh et al., 2007). However, relationships between psychopathy and alcohol use in males have been somewhat mixed. Whereas a few studies have associated PCL-R Factor 2 (lifestyle-antisocial traits) with higher alcohol use in males (Mailloux et al., 1997; Smith & Newman, 1990; Walsh et al., 2007), one study failed to observe this relationship (Hemphill et al., 1994).
Despite relevance to female offending, relationships between psychopathy and drug and alcohol use in females have been infrequently studied. In female studies that have used expert-rater measures of psychopathy, results align with those in males. Female studies using the PCL-R and Psychopathy Checklist–Screening Version (PCL-SV; Hart et al., 1995) suggest associations between psychopathy and alcohol and drug use are driven by Factor 2 (lifestyle-antisocial traits), rather than Factor 1 (interpersonal-affective traits; Hicks et al., 2010; Kennealy et al., 2007; Schulz et al., 2016). Similarly, when using the Psychopathy Checklist–Youth Version (PCL-YV; Forth et al., 2003), Factor 2 psychopathic traits in mid-adolescence have been shown to predict alcohol and drug use 5 years later in male and female youth (Hemphälä & Hodgins, 2014), particularly for males. In addition, Schulz et al. (2016) found that while PCL-SV Factor 2 (lifestyle-antisocial) was related to increased drug use in justice-involved males and females, gender moderated the relationship between Factor 1 (interpersonal-affective) and age of first drug use. Specifically, these traits were related to later onset in females, but not males, suggesting that while lifestyle-antisocial traits may increase risk for drug use across gender, interpersonal-affective traits may protect against early drug use in females (Schulz et al., 2016). Given that substance use is a salient factor in female pathways to offending and interpersonal-affective traits may protect against early drug use in females, results suggest early drug use may contribute less to offending in females high in interpersonal-affective psychopathic traits.
BPD and Substance Use
BPD is characterized by impulsivity, along with difficulties in affect regulation and interpersonal function (American Psychiatric Association [APA], 2013). Studies have shown that BPD is prevalent among incarcerated females (Edwards, Carre, et al., 2019). Like psychopathy, BPD has also been related to substance use, such that BPD is often comorbid with alcohol and drug use disorders in females (Feske et al., 2006; Grant et al., 2008; Lee et al., 2015; Trull et al., 2000, 2018). While impulsive-behavioral features of BPD are more often implicated in substance use (Bornovalova et al., 2005), BPD traits marked by affect instability and sensitivity to abandonment may also be important for understanding relationships, as they may contribute to substance use for reasons related to coping with emotional lability and feelings of emptiness and rejection (Jahng et al., 2011; Mikolajewski et al., 2011). This aligns with relational-cultural theory (RCT), which posits that female growth and development centers around a drive for meaningful interpersonal connections with others (Jordan, 2008). Thus, RCT and related explanations of BPD and substance use in females suggest that psychological distress and maladaptive coping strategies may be related to feelings of social isolation and interpersonal disconnection (Covington, 2008).
Psychopathy, BPD, and Substance Use
Studies have shown positive associations and overlap between psychopathic and BPD traits in justice-involved females (Blonigen et al., 2012; de Vogel & Lancel, 2016; Rogers et al., 2007; Warren et al., 2002). Psychopathy and BPD show similar prevalence rates (~1%–2% of general population), traits (e.g., disinhibition), and behavioral correlates (e.g., substance use; Hare, 2003; Lieb et al., 2004). Researchers testing their overlap have shown associations between BPD and Factor 2 or lifestyle-antisocial psychopathic traits, in particular (Miller et al., 2010; Taylor & Lang, 2006). In fact, BPD and PCL-R Factor 2 have shown trait and genetic overlap with each other and externalizing disorders more broadly, likely reflecting a shared propensity toward disinhibition (Blonigen et al., 2005; Hunt et al., 2015). BPD and PCL-R Factor 2, together with vulnerable narcissism (reflective of defensive and hypersensitive aspects of narcissism), have been shown to coalesce and represent overlapping traits with shared inclination toward disinhibition and negative affect (Edwards et al., 2017). Thus, it may be that individuals high in these traits may impulsively use substances to cope with negative affect (Elkins et al., 2006; Trull et al., 2018). Aligning with this, Edwards et al. (2017) found that this trait constellation (i.e., BPD, Factor 2, vulnerable narcissism) was associated with drug-related criminal activity (e.g., drug possession) in adult males and females.
While psychopathy and BPD comprise similar pathological traits (e.g., disinhibition), they exhibit differences in affect dysfunction. Specifically, studies have associated BPD with an exaggerated emotional response or affect hyperactivity, whereas PCL-R Factor 1 (interpersonal-affective traits) has been related to muted affective response and emotional detachment (Edwards, Carre, et al., 2019). While some work has shown insignificant (or negative) relationships between BPD and Factor 1 (Miller et al., 2010; Warren et al., 2003), other work has suggested that BPD and Factor 1 traits are related, but only in the presence of high Factor 2 traits (Sprague et al., 2012). Studies on the etiological overlap between BPD and psychopathy have focused primarily on overlap between BPD and Factor 2, opposed to Factor 1, although one study found that genetic variance related to narcissistic, insensitive, and dominant aspects of Factor 1 traits may actually protect against BPD in male and female twins (Hunt et al., 2015).
Studies suggest that BPD and PCL-R Factor 2 (lifestyle-antisocial traits) relate to substance use in females, and that relationships may be (at least in part) accounted for by shared vulnerabilities (e.g., disinhibition, negative affect). However, it is unclear the extent to which unique variance in BPD and psychopathy may also inform substance use in females. Given that researchers continue to examine BPD and psychopathy separately in relation to externalizing outcomes, including substance use, it is useful to explore whether relationships with substance use change when accounting for shared variance. Despite this, only one study has controlled for shared variance with BPD when examining effects of psychopathy on drug use (excluding alcohol; Schulz et al., 2016). Results showed that across justice-involved males and females, Factor 2 (lifestyle-antisocial traits) was related to drug use, above the influence of BPD. Thus, results from Schulz et al. (2016) suggest that unique variance associated with Factor 2 traits may be important in understanding drug use. That said, further research is necessary to better understand whether unique variance in both BPD and psychopathy informs distinct substance use patterns in justice-involved females. By accounting for their shared variance in studying substance use outcomes, this work may inform tailored treatment with incarcerated females based on the presence of personality features unique to BPD or psychopathy.
Present Study
This study examined relationships between psychopathic and BPD traits and alcohol and drug use in a sample of 274 incarcerated females. Given that prior work suggests PCL-R Factor 2 (lifestyle-antisocial) and BPD traits share underlying processes that likely promote substance use (e.g., disinhibition, negative emotion), it was expected that without controlling for their shared variance, both would be positively related to alcohol and drug use in incarcerated females. Prior research suggests that in addition to impulsive-behavioral features of BPD, traits unique to BPD, including those marked by affect instability, interpersonal distress, and rejection sensitivity, are conceptually related to substance use (e.g., Mikolajewski et al., 2011; Trull et al., 2018). Moreover, one study to date has suggested unique variance associated with Factor 2 traits may be related to drug use outcomes in justice-involved adults (Schulz et al., 2016). Thus, of particular interest in this study, we hypothesized that while shared variance between BPD and PCL-R Factor 2 may partially account for relationships with substance use outcomes, it would not fully account for these relationships. In other words, we hypothesized that unique variance in both BPD and PCL-R Factor 2 would also be related to alcohol and drug use in incarcerated females.
Method
Participants
Participants were 274 incarcerated females housed in a medium- and maximum-security correctional facility in the United States. This study involved secondary data analyses from data collected as part of a larger set of studies supported by three National Institute of Health R01 awards. Participants ranged from 21 to 56 years of age (M = 34.27; SD = 7.71), and ethnicity was self-identified as Hispanic/Latina (n = 142; 51.8%) or not Hispanic/Latina (n = 132; 48.2%). Race was primarily self-identified as Caucasian (n = 218; 79.6%), followed by Black/African American (n = 29; 10.6%), American Indian/Alaska Native (n = 22; 8.0%), and Native Hawaiian/Other Pacific Islander (n = 2; 0.7%). A total of 1.1% (n = 3) self-identified as Other or chose not to self-identify race.
Participants were excluded if they had an estimated intelligence quotient (IQ) below 70, nonfluency in English and/or a reading level below the fourth grade, lifetime history of psychosis, current antipsychotic medication, and history of traumatic brain injury with loss of consciousness exceeding 30 min. 1 A lifetime history of bipolar disorder was exclusionary, given that such a diagnosis often involves a history of symptoms (e.g., mood lability, impulsivity) that overlap with BPD (Fornaro et al., 2016). To aid in the interpretability of results, participants were also excluded if they met criteria for a current Axis I disorder (Structured Clinical Interview for the Diagnostic and Statistical Manual of Mental Disorders [DSM-IV-TR; APA, 2000] [SCID-I/P]; First et al., 2002), given similar vulnerabilities evident in psychopathy and BPD (e.g., affect dysfunction, impulsivity/reactivity) have been associated with other Axis I disorders common in justice-involved females (de Vogel & Nicholls, 2016; Sakiris & Berle, 2019). Finally, two participants were excluded for a current substance use disorder, considering active substance use may affect reliable assessment of BPD and psychopathy. An ethical review board approved the study, and a certificate of confidentiality was obtained prior to data collection to further protect participant confidentiality. All participants provided written consent prior to participation and were paid at a rate consistent with the facility wage.
Assessments
Alcohol and Drug Use
As a measure of problematic substance use, alcohol and drug dependence were assessed by trained research staff using the SCID-I/P (First et al., 2002). 2 Participants were evaluated on a scale ranging from 0 (absent) to 2 (present) for seven dependence criteria for alcohol (α = .90) and each of six drug categories, including sedative-hypnotics (α = .86), cannabis (α = .74), stimulants (α = .94), opioids (α = .96), cocaine (α = .94), and hallucinogens (α = .77). Dependence was obtained if at least three criteria were scored at threshold. Most participants had at least one dependence diagnosis (n = 247; 90.1%), and participants were frequently diagnosed with more than one dependence type (M = 2.06; SD = 1.28). Due to the high prevalence of dependence diagnoses in the current sample, dimensional scores, reflective of problematic alcohol and drug use, were computed to allow for a larger range and more variability in resulting scores. Specifically, alcohol dependence scores were computed by summing ratings across the seven criteria (M = 6.00; SD = 5.02), with scores ranging from 0 to 14. Similarly, drug dependence scores were computed by summing ratings across the six drug categories (M = 21.71; SD = 11.40), with scores ranging from 0 to 59. See Table 1 (top panel) for descriptive statistics for all variables of interest. Prior work has pointed to distinct etiological mechanisms underlying alcohol and drug use, as well as genetic and shared environmental risk factors for drug abuse/dependence that are nonspecific to drug type (Kendler et al., 2003; Ystrom et al., 2014); thus, drug dependence was collapsed across categories.
Descriptive Statistics for BPD, Psychopathy, and Substance Use
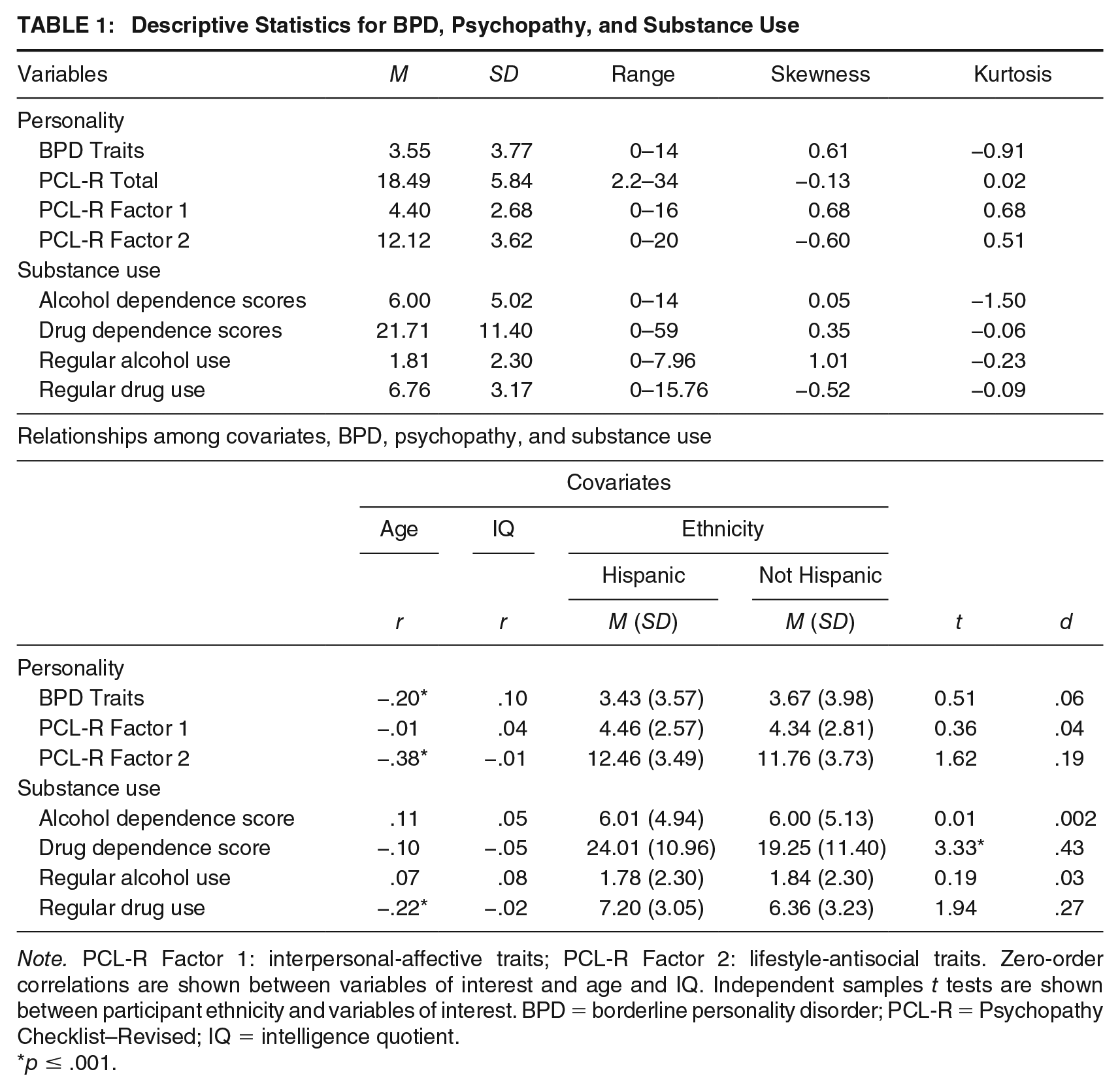
Note. PCL-R Factor 1: interpersonal-affective traits; PCL-R Factor 2: lifestyle-antisocial traits. Zero-order correlations are shown between variables of interest and age and IQ. Independent samples t tests are shown between participant ethnicity and variables of interest. BPD = borderline personality disorder; PCL-R = Psychopathy Checklist–Revised; IQ = intelligence quotient.
p ≤ .001.
In addition to alcohol and drug dependence, duration of lifetime alcohol and drug use was collected for a subsample of participants (n = 212) using a modified version of the Addiction Severity Index (ASI; McLellan et al., 1992). 3 Duration of lifetime alcohol and drug use was included as an additional outcome variable reflective of prolonged substance use across a participant’s lifetime. In other words, while correlated with dependence scores described above (see Table 2), this variable is distinct in that it does not provide information on problems associated with use. Regular use was defined as having used three or more times per week for at least 1 month. Years of regular use was determined for alcohol (i.e., five or more drinks at a time 4 ) and nine drug categories, including cannabis, heroin, cocaine/crack, methamphetamine, other amphetamines (e.g., Adderall), hallucinogens, inhalants, methadone/levo-alpha-acetylmethadol (LAAM), and other opiates/analgesics (e.g., OxyContin). Total years of regular use was computed by summing years of regular use across alcohol and the nine drug categories. Using a similar method as in Ermer et al. (2012), total years of regular use was then divided by participants’ age to control for opportunity and multiplied by 100, and a square root transformation was applied. Scores for regular alcohol use ranged from 0 to 7.96 (M = 1.81; SD = 2.30), and scores for regular drug use ranged from 0 to 15.76 (M = 6.76; SD = 3.17).
Zero-Order Correlations Among BPD, Psychopathy, and Substance Use
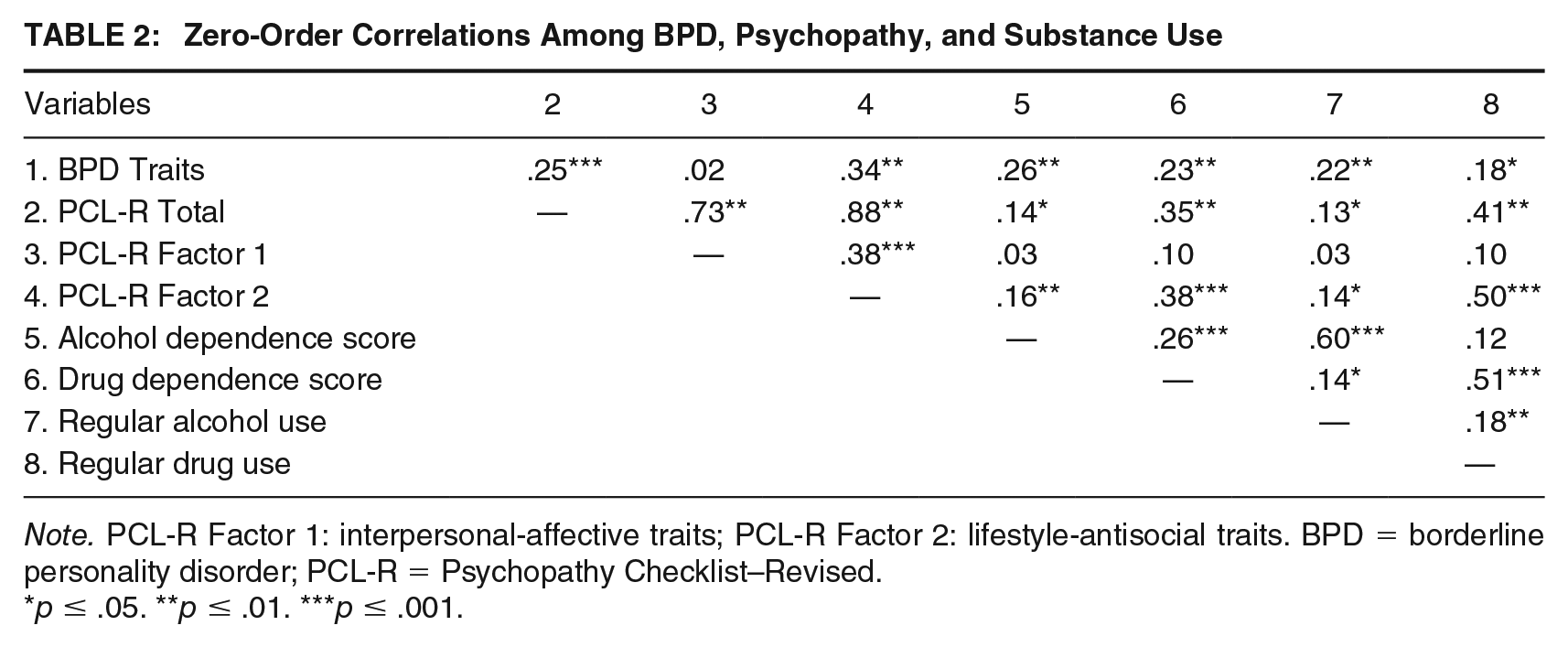
Note. PCL-R Factor 1: interpersonal-affective traits; PCL-R Factor 2: lifestyle-antisocial traits. BPD = borderline personality disorder; PCL-R = Psychopathy Checklist–Revised.
p ≤ .05. **p ≤ .01. ***p ≤ .001.
Psychopathy
Psychopathic traits were assessed using the Hare PCL-R (Hare, 2003), a semi-structured interview consisting of 20 items (α = .76; n = 274) and completed via evaluation of participants’ school, employment, relationship, and criminal history, along with a review of institutional files. Participants received a score on a scale ranging from 0 to 2 for each of the 20 items, with potential PCL-R Total scores ranging from 0 to 40. PCL-R Total scores in the current sample ranged from 2.2 to 34 (M = 18.49; SD = 5.84). Factor 1 (M = 4.40; SD = 2.68) and Factor 2 (M = 12.12; SD = 3.62) scores were positively correlated (r = .38, p < .001). Trained staff completed PCL-R interviews, and double ratings were conducted on 15.7% (n = 43) of interviews (intraclass correlation coefficient [ICC] = .95, p < .001).
BPD
BPD traits were assessed using the Structured Clinical Interview for Axis II Personality Disorders (SCID-II; First et al., 1997). Participants first completed the SCID-II screening form, consisting of 15 items designed to measure BPD traits. Seven (2.6%) participants did not complete the screening form and, therefore, were excluded from analyses involving the BPD variable. Participants who endorsed five or more screening items were then administered the SCID-II BPD interview by trained research staff, which included nine items (α = .80; n = 262). Each item was scored on a scale ranging from 0 (absent) to 2 (threshold). Dimensional BPD scores were calculated by summing scores across the nine items (M = 3.55; SD = 3.77), with scores ranging from 0 to 14. Participants who completed the screening form, but did not endorse a minimum of five screening criteria (n = 111, 41.6%), received a dimensional value of zero. Whereas few participants met full criteria for a BPD diagnosis (i.e., scored at threshold on ≥5 [of 9] criteria), the sample exhibited adequate range of dimensional BPD scores.
Data Analysis
Given high prevalence of substance use in the current sample, this construct was examined by way of two outcome variables assessing both problematic use (i.e., alcohol and drug dependence scores) and prolonged use (i.e., years of regular alcohol and drug use in lifetime). To test study hypotheses, associations between psychopathy factor scores, BPD score, and substance use variables were first tested by way of zero-order correlations. In addition, linear hierarchical regressions were run separately with alcohol and drug dependence scores, as well as regular alcohol and drug use, entered as dependent measures. For each hierarchical regression, demographic covariates (e.g., age, ethnicity) were entered first, PCL-R Factor 1 and Factor 2 scores (or BPD score) were entered second, and BPD scores (or PCL-R Factor 1 and Factor 2 scores) were entered third. Regression models were run in this manner to examine unique variance associated with each of the psychopathy factors, as well as BPD, in relation to alcohol and drug outcomes. All continuous variables included in regression analyses were first mean centered. A modified Bonferroni adjustment employed in prior work was used to account for multiple comparisons (i.e., α divided by the number of dependent variables tested across regression analyses (p ≤ .05 / 4 = .0125; Edwards, Ermer, et al., 2019).
Results
Descriptive statistics for all variables of interest are shown in Table 1 (top panel). Although few participants met the standard PCL-R cutoff for high psychopathy (i.e., PCL-R Total ≥30, n = 10) and/or full criteria for a BPD diagnosis (i.e., ≥5 threshold criteria; n = 9), the sample showed an adequate range of both psychopathic and BPD traits. Participants with a BPD diagnosis had a higher mean PCL-R Factor 2 score (M = 14.61; SD = 2.86) relative to those without a BPD diagnosis (M = 11.97; SD = 3.62), t(264) = 2.17, p = .03, d = .74. However, participants scoring high on PCL-R Total (≥30; M = 4.70; SD = 3.74) did not differ from those scoring below 30 (M = 3.50; SD = 3.77) in terms of mean BPD traits, t(260) = 0.98, p = .33, d = .32. Finally, 100% of participants scoring high on PCL-R Total (≥30) met criteria for at least one substance dependence diagnosis, as did 100% of participants with a lifetime BPD diagnosis. Relationships among demographic covariates (i.e., age, IQ, ethnicity) and variables of interest are shown in Table 1 (bottom panel). Given that age was negatively related to BPD, PCL-R Factor 2, and regular drug use, it was included as a covariate in regression analyses. Females who self-identified as Hispanic showed significantly higher drug dependence scores relative to females who self-identified as non-Hispanic; thus, ethnicity was also included as a covariate in regression models examining relationships with drug dependence.
Zero-order correlations among variables of interest are presented in Table 2. With respect to alcohol-related outcomes in females, BPD and PCL-R Factor 2 were positively related to alcohol dependence scores, as well as regular alcohol use. Linear hierarchical regressions revealed main effects of BPD for both alcohol dependence scores (β = .29, p < .001) and regular alcohol use (β = .23, p = .001; see Table 3, top panel). BPD also remained significantly related to alcohol dependence scores (β = .24, p < .001) after accounting for shared variance with psychopathic traits. Whereas there was a main effect of PCL-R Factor 2 for alcohol dependence scores (β = .25, p = .001) and regular alcohol use (β = .22, p = .01), these effects were no longer significant after controlling for shared variance with BPD (p = .03–.10).
Linear Hierarchical Regressions Among BPD, PCL-R Factors, and Alcohol Use Outcomes
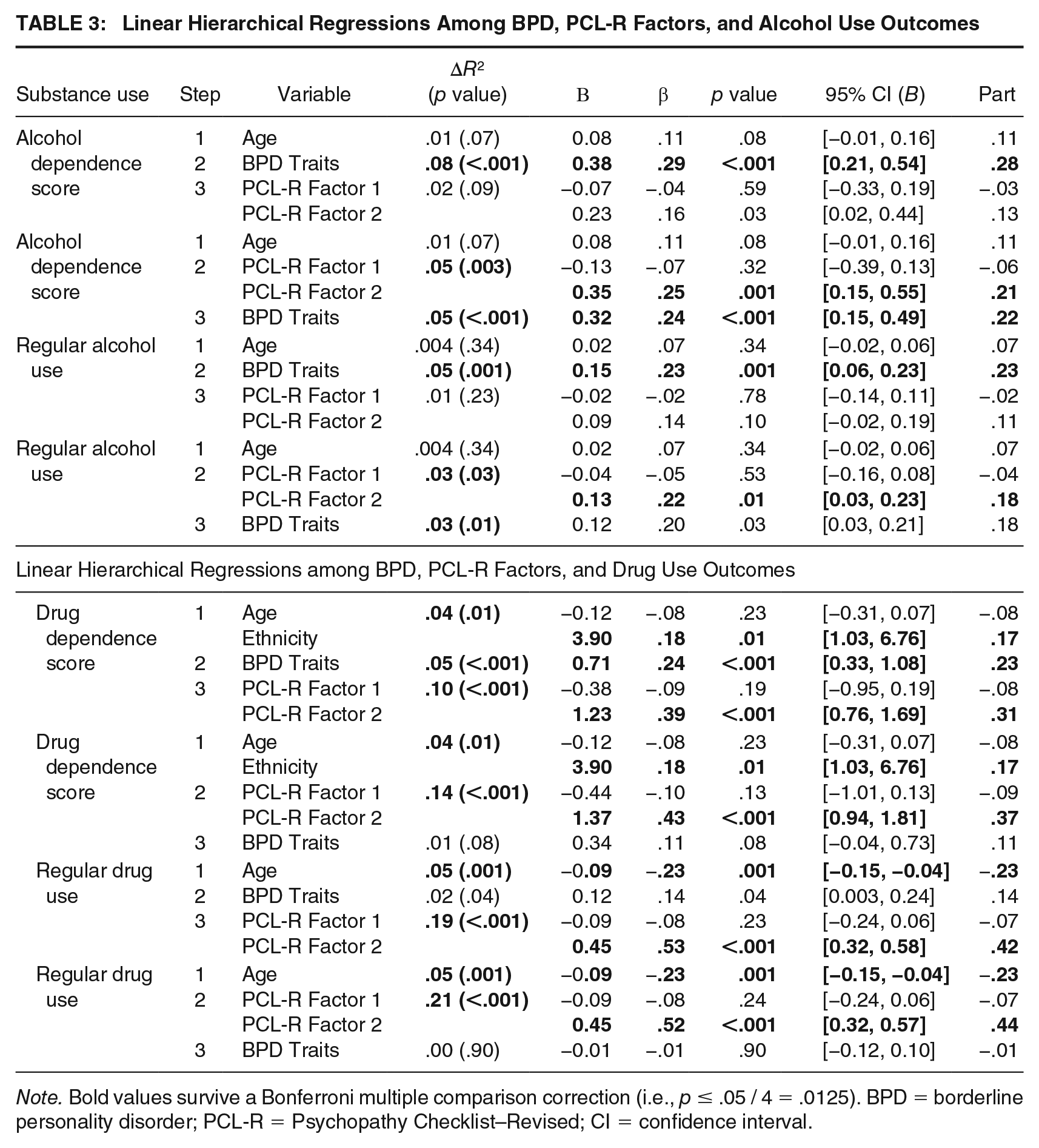
Note. Bold values survive a Bonferroni multiple comparison correction (i.e., p ≤ .05 / 4 = .0125). BPD = borderline personality disorder; PCL-R = Psychopathy Checklist–Revised; CI = confidence interval.
Regarding drug outcomes in females, BPD and PCL-R Factor 2 were positively associated with drug dependence scores and regular drug use. Linear hierarchical regressions revealed main effects of age for regular drug use, as well as ethnicity for drug dependence scores (see Table 3, bottom panel). In addition, there were main effects for PCL-R Factor 2 for drug dependence scores (β = .43, p < .001) and regular drug use (β = .52, p < .001), both of which remained significant when accounting for shared variance with BPD (drug dependence scores: β = .39, p < .001; regular drug use: β = .53, p < .001). While there was a main effect of BPD for drug dependence scores (β = .24, p < .001), this effect was no longer significant after controlling for shared variance with psychopathic traits (p = .08). BPD was not related to regular drug use in regression models (p = .04), after correcting for multiple comparisons. Post hoc zero-order and partial correlations (covarying BPD traits) were run to further examine specific psychopathic traits driving observed relationships between PCL-R Factor 2 scores and drug dependence and regular drug use. Results revealed positive partial correlations between PCL-R Facet 3 (impulsive/lifestyle; r = .25, p ≤ .001) and Facet 4 (developmental/antisocial; r = .25, p ≤ .001) traits and drug dependence scores, as well as PCL-R Facet 3 (r = .34, p ≤ .001) and Facet 4 (r = .44, p ≤ .001) and regular drug use.
Discussion
This study examined relationships between psychopathic and BPD traits and both alcohol and drug use in a sample of incarcerated females. Building on prior work, this study accounted for shared variance between psychopathic and BPD traits in relation to both alcohol and drug use in incarcerated females, and thus, results inform the extent to which unique variance in psychopathy and BPD may relate to distinct substance use outcomes in this population. In line with hypotheses, before accounting for shared variance, both PCL-R Factor 2 (developmental-lifestyle-antisocial) and BPD traits were related to measures of alcohol and drug use. As PCL-R Factor 2 and BPD share similar etiological underpinnings and both have been previously related to heightened genetic risk for externalizing psychopathology (Hunt et al., 2015), these results further point to a general externalizing proneness as important in understanding prolonged and diagnostically relevant substance use in high-risk females.
In support of our hypothesis, BPD traits were related to alcohol dependence scores, above the influence of psychopathic traits, suggesting unique variance in BPD may be relevant to alcohol dependence in incarcerated females. However, unique variance in BPD traits was not related to regular alcohol use. Moreover, after accounting for shared variance with BPD, PCL-R Factor 2 (lifestyle-antisocial) traits were not related to alcohol use in the current sample. Taken together, these results suggest that unique variance in BPD, or that not shared with PCL-R Factor 2, may be relevant to understanding problematic alcohol use in incarcerated females. While both BPD and PCL-R Factor 2 (lifestyle-antisocial) are linked to elevated negative affect (Hicks & Patrick, 2006; Miller et al., 2010), within BPD specifically, these features often manifest as interpersonal dysfunction, including feelings of rejection, abandonment, and isolation (Liebke et al., 2017). Relative to drug use, alcohol is more prevalent in various social contexts and is legal to purchase. Therefore, females presenting with BPD traits may use alcohol to cope with negative affect related to interpersonal and social distress. Relatedly, BPD is characterized by mood fluctuations to subjective interpersonal distress, and it has been suggested that females with BPD traits may use alcohol for stress-dampening effects (Levenson et al., 1980). These results align with a relational-cultural view that social bonds are a fundamental female need (Jordan, 2008) and accordingly, support gender-responsive substance use treatments that promote fostering interpersonal connectedness (Covington, 2008; Salisbury & Van Voorhis, 2009). The finding that unique variance in BPD was related to alcohol dependence, but not regular alcohol use, may also reflect significant interpersonal dysfunction as a specific symptom of alcohol dependence.
Aligning with hypotheses, PCL-R Factor 2 (lifestyle-antisocial traits) was related to drug use outcomes, above the influence of BPD traits. However, contrary to hypotheses, unique variance in Factor 2 was not related to alcohol use. Findings support work in females with psychopathic traits (Hicks et al., 2010; Kennealy et al., 2007), such that PCL-R Factor 2 was related to both problematic and prolonged drug use. In fact, as in Schulz et al. (2016), unique variance in PCL-R Factor 2 was related to drug use, suggesting something specific to Factor 2 may be relevant to drug (and not alcohol) use, at least in incarcerated females. Although PCL-R Factor 2 and BPD traits have been similarly linked to externalizing, evidenced by comparable patterns of impulsive and irresponsible behavior, Factor 2 traits also specifically encompass criminal activity. While criminality may be present in females with BPD traits, it is not a specific feature of BPD as it is for PCL-R Factor 2. It may be that proneness to criminality, evident in females scoring high on Factor 2, helps distinguish those with more serious drug use. That said, criminality and drug use are related, such that each influences the other. For instance, living a criminal lifestyle and/or affiliating with criminal associates likely provides contexts promotive of drug use. Alternatively, in line with theories on female offending, drug use may contribute to and exacerbate criminality in females via drug-related crime (e.g., possession) or crime which helps finance drug use (e.g., theft, prostitution; McClellan et al., 1997). In fact, the former reflects a gendered institutional influence, as drug policy changes have disproportionately affected females and their involvement in the criminal justice system (Javdani et al., 2011b).
This study has several strengths. It included females with varying levels of psychopathic and BPD traits and substance use. As psychopathic and BPD traits were both assessed, this study could examine relationships between their unique variance and alcohol versus drug use. Substance use was also examined via two approaches, given the high prevalence of alcohol and drug use. There are also some limitations. First, few participants met the standard PCL-R cutoff for high psychopathy (i.e., PCL-R Total ≥30, n = 10; Hare, 2003). However, studies show that females likely exhibit lower rates of psychopathy than males (Vitale et al., 2002). Relatedly, although most participants were considered medium-security, a few participants may have been considered maximum-security, but not housed in segregation, and thus, security level may have had an effect on PCL-R scores. Second, few females met full diagnostic criteria for BPD (i.e., ≥5 threshold criteria, n = 9). The low BPD diagnostic rate may be due in part to ethnic composition, as lower BPD prevalence has been observed in Hispanic individuals compared with other ethnicities (Grant et al., 2008). Females in this study may also have been hesitant to endorse certain BPD traits (e.g., suicidality) that may result in unwanted consequences (e.g., suicide watch). Regardless, the sample had an adequate range of BPD traits. Third, females with a current Axis I disorder were excluded, and thus, results may not generalize to those with current Axis I diagnoses or those who may use substances to cope with current Axis I symptoms. However, this exclusion criteria likely aided our ability to understand the extent to which unique variance in BPD or psychopathy (opposed to comorbid current Axis I symptoms) related to substance use. Including cannabis may limit generalizability of results, as this drug has been growing in its legalization (Hall & Lynskey, 2016). Substance use also likely contributed to personality trait scoring, and thus, circularity may partially account for relationships. Finally, race was not included in models and its inclusion may have influenced results. In light of controversy on conceptualizations of race (e.g., biological, social) and its use in research on health outcomes (Corbie-Smith et al., 2008), testing race in relation to substance use appeared to fall outside the scope of this study. It would be useful for future work to explore the role of race and/or ethnicity in understanding relationships among psychopathy, BPD, and substance use.
This study holds important treatment and criminal justice implications. Given high rates of substance use in justice-involved females, findings suggest that assessment of distinct personality traits may help to determine appropriate substance use treatments for females in the criminal justice system. Our results also suggest that when tailoring treatment in incarcerated females, it may be worthwhile to incorporate interventions effective in targeting personality pathology, such as dialectical behavior therapy (DBT; Linehan, 2015). For example, DBT skills in emotion regulation, distress tolerance, and interpersonal effectiveness may be useful in treating females with comorbid alcohol use (Jahng et al., 2011). In addition, given unique variance in BPD was related to alcohol use, incorporating significant others (e.g., family, romantic partners) and emphasizing common BPD feelings of rejection and social isolation in BPD treatment with females may be beneficial in addressing issues related to interpersonal distress, as well as those relevant to alcohol use (Fitzpatrick et al., 2019). Results also suggest that proneness to criminality (i.e., unique variance in PCL-R Factor 2) might help distinguish females with more versus less severe drug use. While criminality and drug use are likely mutually related, research has shown that relative to non-drug users, odds of criminal offending are 3 to 4 times higher for drug users (Bennett et al., 2008). It may also be that in drug-using populations, odds of offending are even greater for females than males, consistent with work highlighting drug use as central in female offending (Bennett et al., 2008; McClellan et al., 1997). Drug use is a dynamic risk factor that can be targeted with treatment to reduce criminal risk, and thus, substance use treatment is likely useful in females high in Factor 2 (lifestyle-antisocial traits) and drug use. Beyond targeting drug use itself, drug treatment may also help to break cyclic relationships between criminality and drug use that contribute to female recidivism.
In conclusion, results provide further support for positive relationships between PCL-R psychopathic traits, as well as BPD traits, and substance use outcomes in incarcerated females. Specifically, this study observed relationships between unique variance in psychopathy and BPD and distinct types of substance use (i.e., lifestyle-antisocial psychopathic traits and drug use and BPD traits and alcohol use). These results shed light on unique personality vulnerabilities that may contribute to alcohol versus drug use in incarcerated females. Finally, results hold critical implications for tailoring substance use treatments based on distinct personality traits.
Footnotes
Acknowledgements
We would like to thank the New Mexico Corrections Department for their support in making this research possible. Data collection for this project was funded in part by the National Institutes of Health across R01MH085010, R01DA026964, and R01DA020870 (PI: Kent A. Kiehl).
The National Institute of Health has provided stipend support for Bethany G. Edwards (F31DA047048). The content in this manuscript is the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.