
Abstract
The present study examined the relationship between religious capital and depressive symptoms and the moderating role of the Big Five personality constructs in a national sample of African American adults. Data were collected from a national probability sample of 803 African American men and women using a telephone survey including measures of the Big Five personality traits, religious capital, and depressive symptomology. Most interestingly, there was evidence for Personality × Religious Capital interactions on depressive symptomology. Higher religious capital was related to lower depressive symptomology among persons with low conscientiousness or low openness to experience. However, religious capital was less related to depressive symptoms among those with high conscientiousness or high openness. This study reinforces the importance of examining the moderating effects of personality and perceived religious capital in understanding mental health outcomes. This information can be of use to practitioners in designing culturally appropriate interventions, including the use of capital from faith-based organizations.
Introduction
Psychosocial resources such as personality and perceived community support are important to African Americans’ mental health. There is growing evidence of inequalities affecting the mental health of African Americans (Torres, 2013; Utsey & Hook, 2007). Additionally, prior research suggests that religiosity-related variables are associated with health outcomes (George, Ellison, & Larson, 2002; Holt, Schulz, Williams, Clark, & Wang, 2012a, 2012b; Ross, Handal, Clark, & Vander Wal, 2009). For example, George et al. (2002) note that frequent attendance at religious services is related to better physical and mental health; persons who frequently attend religious services have fewer illnesses, recover more quickly from illness, and live longer than those who attend less frequently. Furthermore, they note that persons who rely on religious coping recover more quickly from illness and better tolerate invasive medical procedures. In the current study, we investigate the relationship between personality, religious capital, and depressive symptomology.
The Relationship Between Personality and Mental Health Among African Americans
The Five Factor Model of Personality (Costa & McCrae, 2004) suggests that personality is organized around the following basic dimensions—Openness to Experience (e.g., artistic, curious, imaginative, wide interests), Conscientiousness (e.g., efficient, organized, planful, dependable), Extraversion (e.g., active, energetic, gregarious, talkative), Agreeableness (e.g., appreciative, forgiving, generous, considerate), and Neuroticism (e.g., anxious, self-pitying, emotionally unstable, worrying). Several studies have examined issues related to these personality factors and mental health among African Americans. Savla, Davey, Costa, and Whitfield (2007) found evidence for the five factor personality model in a sample of African American adults and Chan (1997) examined the predictive validity of the five factor model and found no differences in their Black and White samples. Pearson et al. (2014) reported that Black students who were high in neuroticism were more likely to experience intrusive thought, increased negative affect, and less forgiveness in response to a racist incident. They also found that neuroticism moderated the relationship between some coping strategies and distress in response to a racist incident. For example, they found that use of humor as a coping strategy was related to lower negative affect for individuals high in neuroticism but not for those low in neuroticism. A study by Baldwin, Jackson, Okoh, and Cannon (2011) indicated that higher dispositional optimism was related to lower psychological distress and higher resiliency in a sample of Black senior citizens. In addition to personality, religiosity has also been shown to play a role in mental health.
Relationship Between Religion and Mental Health Among African Americans
Several studies indicate the importance of religion among African Americans. Using the National Survey of American Life, Chatters, Taylor, Bullard, and Jackson (2009) found that most African Americans were members of religious worship congregations and reported high levels of other religious activities such as prayer and reading religious texts. Belgrave and Allison (2014) discuss research by the Barna Group showing that African Americans have high levels of reading the Bible in the past week (59%), prayed to God in the past week (91%), and strongly agreed with the inerrancy of the Bible (57%). Belgrave and Allison (2014) further note that for African Americans, church life is often intertwined with family life and that the concept of “church family” indicates the high level of involvement of the church in people’s lives. African American churches include “ministries” to serve the community such as educational (e.g., tutoring), health (e.g., health fairs), counseling/support group (e.g., after death of a spouse), and hunger (e.g., food pantries). These programs help congregation members feel connected to each other and to the community, illustrate their collectivistic orientation, and provide an important source of capital (i.e., social connections that encourage mutual cooperation).
Prior research has examined the relationship between religion and mental health among African Americans. In a national sample of African American adults, Holt, Wang, Clark, Williams, and Schulz (2013) found that perceived religious support mediated the relationship between religious behaviors and depressive symptomology and emotional functioning such that religious behaviors were related to higher religious social support which was, in turn, related to fewer depressive symptoms and better emotional functioning. Grayman-Simpson and Mattis (2012), in a community sample of Black adults, found that subjective religiosity predicted higher levels of helping behavior and higher satisfaction derived from community helping. Taylor, Mattis, and Chatters (1999), using data from five probability samples including Black and White respondents, found that religious comfort and support played an important role in participants’ daily lives and coping strategies. Holt et al. (2009) discussed the importance of understanding the mediators underlying the connection between religion and health among African Americans and highlighted the supportive role that participation in a faith community plays in health-related outcomes.
Religious Capital
As noted above, faith communities, where people gather for worship, foster interpersonal welfare, demonstrate a collectivistic orientation, and provide an important source of social capital. Holt et al. (2012a) define religious capital as the capital derived from one’s relationship with their faith community. This definition is similar to a previous one that defined religious social capital as “social resources available to individuals and groups through their social connections with a religious community” (Maselko, Hughes, & Cheney, 2011, p. 760). The present study used a model of religious capital reported by Holt et al. (2012a) that included three dimensions: social support, interconnectedness, and community participation.
Prior research suggests several benefits of religious capital, including some studies with African American samples. Irwin, LaGory, Ritchey, and Fitzpatrick (2008) found that higher religious social capital predicted less depressive symptomology in a mostly African American sample of homeless men and women. Furthermore, religious social capital was positively correlated with African American 8th- and 10th-grade students’ college ambitions and future goals (Al-Fadhli & Kersen, 2010). Mason, Schmidt, and Mennis (2012) report religious social capital’s positive “spillover” effect in the community in that persons’ close proximity to religious institutions was a protective factor against alcohol use in a largely African American adolescent sample. Wingood et al. (2013) reported on a faith-based HIV prevention program for African American women that, among other outcomes, increased the women’s religious social capital.
In addition to the few studies that have examined the relationship between religious capital and mental health, a considerable number of studies have examined the relationship between social support, a key component of capital, and mental health, including depressive symptomology. Furthermore, some studies have found evidence for moderation involving social support and depressive symptomology. In a sample of Black women, Seawell, Cutrona, and Russell (2014) found evidence for a buffering effect in that tailored support for racial discrimination (but not general social support) protected participants from depressive symptoms when racial discrimination was high but not when discrimination was low. In a sample of African American adolescent boys, Lindsey, Joe, and Nebbit (2010) reported evidence for moderation in that social support was related to lower depressive symptomology, especially among participants experiencing mental health stigma. Bronder, Speight, Witherspoon, and Thomas (2014) found that lower depressive symptomology was related to higher significant other, family, and friend social support in a sample of Black women.
Several additional studies indicate the varying roles of social support. Palmer (2001) reported that African American depressed patients with a history of suicide attempt scored lower on perceived social support than depressed patients with no such history. Brown (2008) observed that receiving racial socialization messages and having high perceived social support predicted higher resiliency. Lincoln (2007) reported that negative social interactions (e.g., others make too many demands, are critical of the individual) were related to lower feelings of mastery, which in turn were related to higher depressive symptomology. Finally, Stevenson (1998) found that adolescents who lived in neighborhoods with high levels of social capital reported less depressive symptomology than those in low social capital neighborhoods. The studies reviewed indicate a well-established relationship between religious capital (and relatedly social support) and its ameliorating effect on depressive symptomology among African Americans.
Personality, Perceived Social Support, and Mental Health: The Complementary Fit Model
Consistent with social cognitive theory (Bandura, 1999), the Person × Environment interactionist approach states that behavioral and attitudinal variables are a function of the relationship between individual and environmental/situational factors (Lewin, 1936; Sansone, Morf, & Panter, 2004). More specifically, we predict that the relationship between an individual’s personality and perceived religious capital in the environment is consistent with the complementary fit model which suggests that the individual’s characteristics “make whole” (Muchinsky & Monahan, 1987, p. 271) the characteristics of the environment or when the environment/situation and the individual contribute to satisfying the needs of the other (Muchinsky & Monahan, 1987; Piasentin & Chapman, 2006; Verquer, Beehr, & Wagner, 2003).
While there is little research examining Personality × Capital interactions, there is extant research exploring Personality × Social Support. Mosher, Prelow, Chen, and Yackel (2006) found that avoidant coping and social support mediated the relationship between optimism and depressive symptoms in a sample of African American college students. In a sample of older adults, McHugh and Lawlor (2012) found that high levels of social support protected against the negative effects of high neuroticism on well-being. Hoth, Christensen, Ehlers, Raichle, and Lawton (2007), in a sample of adults with kidney disease, reported that the personality trait of agreeableness moderated the role of social support in depressive symptom change. Specifically, they found that greater social support among highly agreeable adults with chronic kidney disease was associated with a decrease in depressive symptoms over time, while support had little effect on depressive symptom change for less agreeable patients.
Several other studies have suggested that social support differentially affects individuals who vary on certain personality traits (Hotard, McFatter, McWhirter, & Stegall, 1989; Roberts & Gotlib, 1997; Roos & Cohen, 1987). For example, in a sample of college students, Hotard et al. (1989) found, in their Study 1, that social relationships predicted subjective well-being for introverted, but not extraverted, individuals. In their Study 2, a strong relationship between extraversion and subjective well-being occurred only among persons who were highly neurotic or had poor relationships. Duckitt (1984), in a sample of students at a South African university, found that extraversion moderated the influence of social support such that that social support played a stronger role in reducing distress among those higher in extraversion compared to more introverted participants. Within a group of older patients with some diagnosed with depression, Oddone, Hybels, McQuoid, and Steffens (2011) found that the relationship between both neuroticism and depression varied by level of subjective social support such that those with high subjective social support combined with low neuroticism reported lowered depression. Pai and Carr (2010) examined personality, loss of support from a spouse, and their relationship to depression in a sample of older adults. They found that extraversion and conscientiousness act as protective factors such that depression resulting from a spouse’s anticipated rather than sudden death is lowered as the person’s extraversion or conscientiousness level increases. However, there was no evidence of this effect among continually married individuals. In their study of nurses and burnout, Eastburg, Williamson, Gorsuch, and Ridley (1994) found that compared with introverted nurses, extraverted nurses required more work-related peer support to avoid emotional exhaustion. However, not all research has found synergistic relationships between personality and support on mental health. For example, Emery, Huppert, and Schein (1996), using data from a British national survey, did not find evidence for moderation in which there were no statistically significant interactions between extraversion and support, nor neuroticism and support, in predicting psychological functioning.
In summary, there is ample evidence for the role of religiosity and religious capital in mental health outcomes among African Americans. While there is little, if any, research on the moderation relationship of personality and religious capital on mental health, there is research indicating that personality, especially the Big Five dimensions (e.g., Baldwin et al., 2011; Pearson et al., 2014), and social support (a key dimension of religious capital) are jointly related to mental health (McHugh & Lawlor, 2012; Pai & Carr, 2010). Additionally, there are a variety of studies examining the role of social support and mental health among African Americans (e.g., Mosher et al., 2006). However, there is no research on the relationship between personality, religious capital, and mental health among African Americans.
The Present Study
There is increasing evidence that examining psychosocial resources such as personality and capital can add to our understanding of African Americans’ emotional functioning. The present study explores the possible moderation relationship of personality and religious capital on depressive symptoms in a national sample of African Americans. We examined the Big Five personality characteristics and religious capital since prior work suggests that religious capital is highly important in the African American community. While other studies have jointly examined personality and social support few, if any, have examined personality with religious capital. Furthermore, we could not find any studies that have done so in a sample of African Americans. Given the lack of prior research, we employed a broad approach of examining the five personality dimensions (the Big Five—conscientiousness, extraversion, openness to experience, agreeableness, and neuroticism), religious capital, and their possible moderating relationship to depressive symptomology.
Hypotheses
Based on the complimentary fit model and prior research (e.g., McHugh & Lawlor, 2012; Pai & Carr, 2010), our primary hypotheses involved predicting Personality × Religious Capital interactions such that those reporting high religious capital will report fewer depressive symptoms (compared with those reporting low religious capital) primarily among those with low extraversion, low agreeableness, low conscientiousness, low openness to experience, or high neuroticism. Therefore, high religious capital will help compensate for the detrimental mental health consequences of these patterns of personality traits. However, religious capital will have a smaller relationship (little difference between high and low capital participants) with depressive symptomology for those persons with high extraversion, high agreeableness, high conscientiousness, high openness, or low neuroticism, who will have relatively low levels of depressive symptomology regardless of religious capital levels.
Method
Participants and Telephone Survey
The Religion and Health in African Americans II study (RHIAA II) was a national survey designed to test a theoretical model of the religion-health connection. Professional interviewers dialed telephone numbers from a purchased list of U.S. households, comprising a national representation of census tracts (“cold call” interviews). Gensys, a professional sampling firm, generated the call list by randomly selecting households from a national pool. Eligible participants were African American and 21 years or older. Those who were both interested and eligible were read an informed consent script and asked to provide their assent to participate. On completion of the interview, a $25 gift card was mailed to each participant. The interview took an average of 30 minutes. The study was approved by the University of Maryland Institutional Review Board.
A total of 803 African Americans completed the telephone interview (424 women, 379 men). The average age was 56.01 years (SD = 15.00). Many (40.8%) were married or living with a partner, had a median income of $30,000 to $40,000, most had a high school education (35%) or 1 to 3 years of college (25.8%), worked full-time (33.1%) or were retired (30.1%). The response rate is calculated as the proportion of complete interviews to the total number of eligible individuals. Only 13 individuals who were screened and eligible refused to participate, resulting in an upper bound response rate of 98% (803/816). The overall response rate is 27%, 803 accepted/(803 accepted + 2,195 refused). Another 379 individuals were not eligible for various reasons: 31 were younger than 21 years, 159 refused to provide an age for use in eligibility screening, and 189 were not African American. A total of 3,390 calls were made (summing each of these dispositions). A brief refusal survey was conducted to compare responders to nonresponders (N = 73). Nonresponders were in general older (M = 65.52 years old, SD = 15.28 vs. M = 56.01 years old, SD = 15.00, respectively), more likely to be men (62.0% vs. 47.2%, respectively), less educated in terms of likely to have attended 1 to 3 years of college (14.1% vs. 25.8%, respectively), less likely to have attended a religious service in the past year (70.4% vs. 83.2%, respectively), and less likely to attend religious services four or more times per month (36.6% vs. 47.8%, respectively) than responders.
Measures
The NEO Five-Factor Inventory–Form S was used to assess the five factor model (Big Five) personality dimensions (Costa & McCrae, 2004). The scale assessed Conscientiousness (e.g., “Make plans and stick to them”), Extraversion (e.g., “Make friends easily”), Openness to Experience (e.g., “Enjoy hearing new ideas”), Neuroticism (e.g., “Have frequent mood swings”), and Agreeableness (e.g., “Accept people as they are”). Each of these personality traits was measured by five items. Participants responded on a Likert-type scale (1 = strongly disagree to 5 = strongly agree). Higher scores indicate more of the trait. This is a widely used instrument based on the NEO Personality Inventory with high internal consistency (α = 0.76-0.90). Internal consistencies were also adequate for the current sample: Conscientiousness α = 0.77, Extraversion α = 0.75, Openness to Experience α = 0.67, Neuroticism α = 0.79, and Agreeableness α = 0.75.
Religious capital was operationalized as resources gained through involvement with one’s religious community. Holt et al. (2012a) developed the religious capital scale based on a social capital instrument developed by Perry, Williams, Wallerstein, and Waitzkin (2008). Validation of the religious capital measure is discussed in Holt et al. (2012a). This adaptation involved modifying references to “neighbors” and “people in your community” to “people in my religious/spiritual community” reflecting religious capital. The adaptation was conducted purposively so that items closely mirrored the original social capital instrument. Similar to the social capital measure, religious capital includes a social support dimension (e.g., “If I needed a ride to the doctor, I would be likely to call on someone in my religious/spiritual community for a ride”), an interconnectedness dimension (e.g., “My religious/spiritual community is a good place for kids to grow up”), and a community participation dimension (e.g., “I can influence decisions that affect my religious/spiritual community”). The religious capital scale consisted of nine items assessed in 4-point Likert-type format (1 = strongly disagree to 4 = strongly agree). Higher scores indicate higher levels of these beliefs and the scale demonstrated good internal reliability (α = 0.87).
Depressive symptoms were assessed with the short form of the Center for Epidemiological Studies Depression Scale (Radloff, 1977). The Center for Epidemiological Studies Depression Scale was selected because it has been previously validated with an African American population (Makambi, Williams, Taylor, Rosenberg, & Adams-Campbell, 2009; Roth, Ackerman, Okonkwo, & Burgio, 2008). Participants were asked the frequency in the past week that they experienced depressive symptoms such as “I had crying spells” and “I felt that everything I did was an effort” (rarely/less than 1 day . . . all of the time/5-7 days). Higher scores indicate more depressive symptomology. Test-retest reliability and internal consistency were high in previous normal and patient populations (α = 0.87). Reliability using the current study’s data, using Cronbach’s alpha, was acceptable (α = 0.88).
A standard demographic module assessed participant characteristics including sex, age, relationship status, religious denomination, educational attainment, work status, and household income before taxes.
Results
Overview
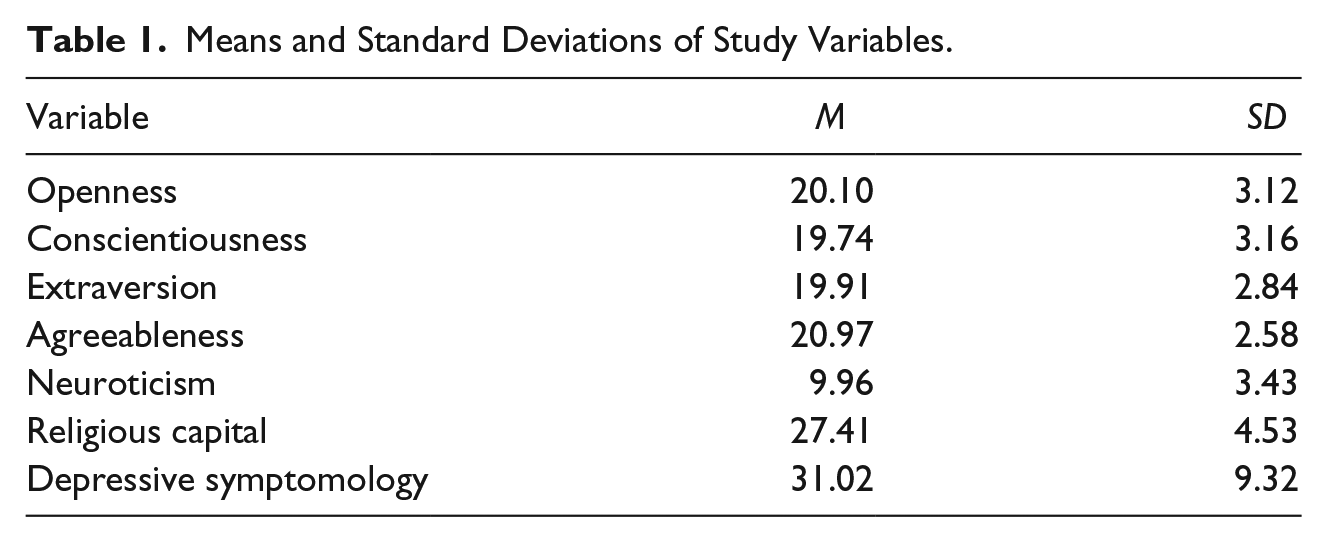
The means and standard deviations for the study variables are reported in Table 1 and the correlation matrix is displayed in Table 2. Due to the very large sample size, all the correlations in Table 2 are significant at the p < .05 level (and as indicated in the note in Table 2, all correlations were significant at the p ≤ .0025 level). Therefore, in Table 2, we omit the asterisks for significant correlations to avoid making the table more cumbersome.
Means and Standard Deviations of Study Variables.
Correlation Matrix of Study Variables.
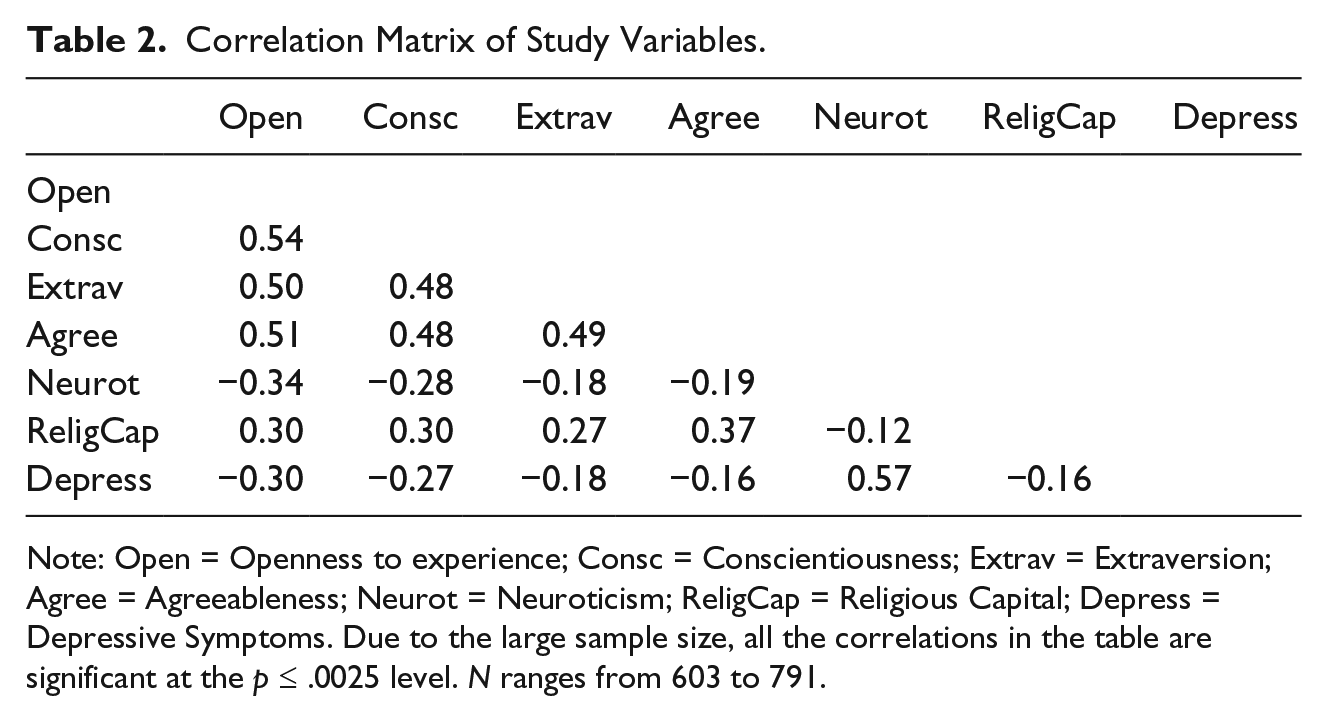
Note: Open = Openness to experience; Consc = Conscientiousness; Extrav = Extraversion; Agree = Agreeableness; Neurot = Neuroticism; ReligCap = Religious Capital; Depress = Depressive Symptoms. Due to the large sample size, all the correlations in the table are significant at the p ≤ .0025 level. N ranges from 603 to 791.
We performed five multiple regressions, one for each personality trait. For each regression, we entered the control variables of age, education, and income, the predictor variables of personality (one of the Big Five), religious capital, and the Personality × Religious Capital interaction. Our outcome variable was depressive symptomology.
Conscientiousness
We found a significant main effect for Conscientiousness (β = −0.79, p < .001) such that higher conscientiousness was related to lower depressive symptoms. We also found a main effect of Religious Capital (β = −0.61, p = .002) in that persons who reported higher religious capital also reported lower depressive symptoms. Finally, there was a significant Conscientiousness × Religious Capital interaction (β = 0.86, p = .006). We performed simple slopes analyses on religious capital using the values of ±1 standard deviations from the means for conscientiousness and religious capital. As shown in Figure 1 and as predicted, among persons low in conscientiousness, those with high religious capital reported lower depressive symptoms than those with low religious capital (b = −1.03, p < .0001). However, among those with high conscientiousness, religious capital was significant but not as strongly related to depressive symptoms (b = −0.48, p = .0021); these high conscientious persons were relatively low in depressive symptoms regardless of their religious capital.
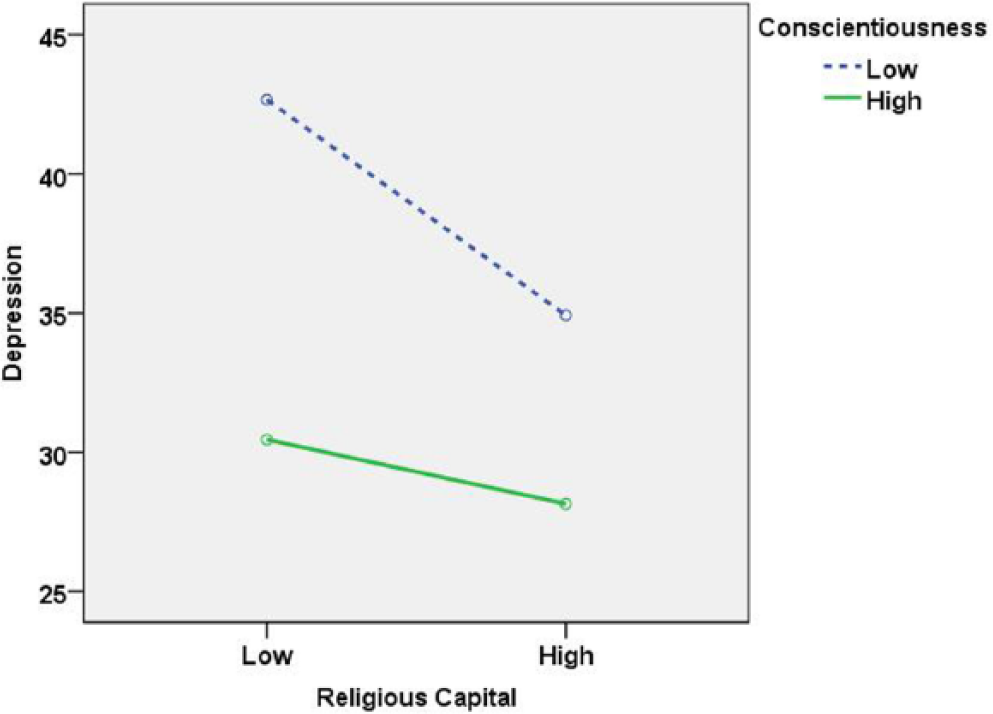
Depressive symptomology as a function conscientiousness and religious capital.
Extraversion
There was a significant main effect for Extraversion (β = −0.60, p = .007) such that those higher in extraversion reported lower depressive symptomology. Again, there was a significant main effect of Religious Capital (β = −0.65, p = .014) such that higher religious capital was related to lower depressive symptomology. There was a significant Extraversion × Religious Capital interaction (β = 0.78, p = .041). However, contrary to our hypotheses, simple slopes analyses using the values ±1 standard deviations from the means for extraversion and religious capital suggested that religious capital was not a significant predictor of depressive symptomology at high or low extraversion levels.
Openness to Experience
The results for Openness were similar to those for Conscientiousness. There was a significant main effect of Openness to Experience (β = −0.73, p = .001) such that those who were higher in openness reported fewer depressive symptoms. Again, there was a main effect of Religious Capital (β = −0.54, p = .012) such that those with higher religious capital reported lower depressive symptoms. There was also a significant Openness × Religious Capital interaction (β = 0.73, p = .024). We performed simple slopes analyses using values ±1 standard deviations from the means for openness and religious capital. As predicted and shown in Figure 2, among persons low in openness, those with high religious capital reported lower depressive symptoms than those with low religious capital (b = −1.08, p < .0001). However, among those with high openness, again those with high religious capital reported lower depressives symptoms than those low on religious capital but the relationship was not as strong (b = −0.58, p < .0007) as for the low openness participants. When openness was high, religious capital was not as strongly related to depressive symptoms as when openness was low; these high openness participants were relatively low in depressive symptoms regardless of their religious capital level.
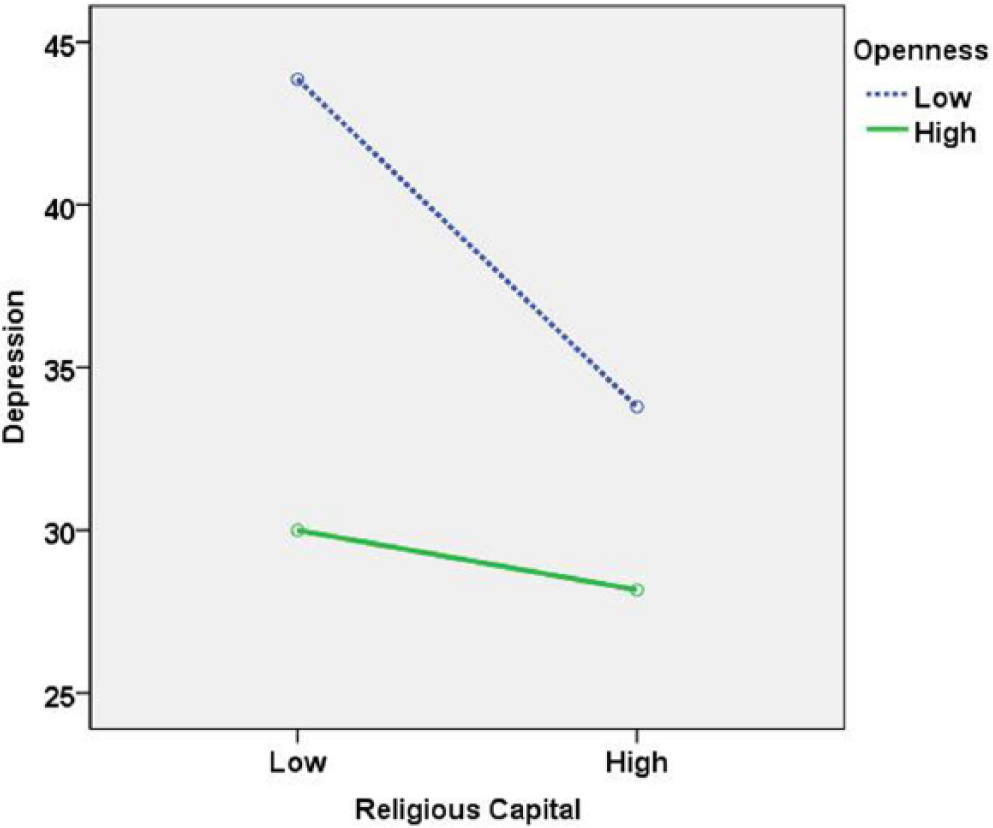
Depressive symptomology as a function of openness to experience and religious capital.
Neuroticism
We found a significant main effect for Neuroticism (β = 1.46, p = .001), such that persons high in neuroticism reported more depressive symptomology than those with low neuroticism. We found a significant Religious Capital main effect such that, inconsistent with prior analyses, those with higher religious capital reported higher depressive symptoms (β = 0.34, p = .001; the reason that religious capital is positively correlated with depressive symptomology instead of negatively correlated as in other analyses is explored below). There was a significant Neuroticism × Religious Capital interaction (β = −0.97, p = .001). We performed simple slopes analyses using the values ±1 standard deviations from the means for neuroticism and religious capital. Contrary to our hypotheses, among those with low neuroticism, those with high religious capital reported higher depressive symptoms than those with low religious capital (b = 1.95, p < .0001). Among persons high in neuroticism, those with high religious capital also reported higher depressive symptoms than those with low religious capital but the relationship was not as strong (b = 1.16, p < .0001). We suspect that the unusual results for the significant Religious Capital main effect and the Neuroticism × Religious Capital interaction are due to suppression effects given the relatively large positive correlation between neuroticism and depressive symptomology (r = 0.57; Table 2). Consistent with the other analyses reported above, religious capital is significantly and negatively correlated with depressive symptomology (r = −0.16; Table 2).
Agreeableness
There was a marginally significant main effect for Agreeableness (β = −0.34, p = .078) such that those with higher agreeableness reported lower depressive symptomology. Neither the main effect for Religious Capital nor the Agreeableness × Religious Capital interaction approached statistical significance, contrary to our hypotheses.
Discussion
Consistent with social cognitive theory (Bandura, 1999), the Person × Environment approach states that behavior is a function of the relationship between the individual and environment (Lewin, 1936; Sansone, Morf, & Panter, 2004). Relatedly, the complementary fit model (Muchinsky & Monahan, 1987; Piasentin & Chapman, 2006; Verquer et al., 2003) suggests that the individual’s characteristics may complement the characteristics of the environment or when the environment and the individual contribute to satisfying the needs of the other. The present study used the complimentary fit model to examine the Big Five personality constructs as moderators of the relationship between religious capital and depressive symptoms in a national sample of African Americans. Given the importance of religious capital and related constructs in the African American community (e.g., K. L. Gilbert, Quinn, Goodman, Butler, & Wallace, 2013; Hosen & Salovey-Hosen, 2003), it is important to examine their roles as well as the contributions of personality characteristics on mental health. In addition, no other studies have examined the moderating role of personality and religious capital.
Personality and religious capital had significant effects on depressive symptomology. Persons who were higher on conscientiousness, extraversion, or openness to experience reported fewer depressive symptoms. The main effect of agreeableness on depressive symptomology was only marginally statistically significant. Furthermore, in most analyses, we found that those with higher religious capital experienced fewer depressive symptoms than those with lower religious capital.
Consistent with the complementary fit model, these significant main effects were qualified by two Personality × Religious Capital interactions—those involving the personality traits of conscientiousness and openness to experience. In general, religious capital had little relationship to depressive symptoms when respondents reported high conscientiousness or high openness to experience. Such persons have relatively low depressive symptoms regardless of religious capital level. Alternatively, when participants were low in conscientiousness or low in openness, then higher religious capital was associated with lower depressive symptoms. It seems that having high religious capital, including high social support, feeling interconnected, and participating in one’s faith community, compensates for low conscientiousness and low openness personality in preventing depressive symptomology. Interestingly, the personality trait of agreeableness did not moderate the influence of religious capital on depressive symptoms, contrary to results found by Hoth et al. (2007). Perhaps this is explained by the correlations displayed in Table 2. Agreeableness is characterized by being appreciative, forgiving, generous, and considerate which are traits that seem especially related to religious capital. Therefore, agreeableness has a higher correlation (more shared variance) with religious capital than some of the other personality variables, in addition to being correlated with depressive symptoms. The Agreeableness scale’s combination of relationships with the other predictor and outcome variables may explain its mostly nonsignificant unique effects in the regression analyses (the main effect for Religious Capital and the Agreeableness × Religious Capital interaction were both nonsignificant).
Additionally, analyses involving extraversion indicated an Extraversion × Religious Capital interaction, but the simple slopes analysis, contrary to our hypotheses, did not confirm different religious capital effects on depressive symptoms at different levels of extraversion, which is somewhat inconsistent with Hotard et al. (1989). Another finding inconsistent with hypotheses was that for the Neuroticism regression analysis only, Religious Capital was positively (not negatively) correlated with depressive symptomology. Furthermore, the Neuroticism × Religious Capital interaction suggested that among those with lower and higher neuroticism, those with higher religious capital reported higher (not lower) depressive symptoms than those with low religious capital (inconsistent with other analyses) and the effect seems slightly larger among those with lower neuroticism. We suspect that this is caused by a suppression effect given the intercorrelations between neuroticism, religious capital, and depressive symptomology. As one would expect, the zero-order correlation between religious capital and depressive symptomology is negative (r = −.16; see Table 2). Additionally, neuroticism (which is characterized by being anxious, self-pitying, emotionally unstable, and worrying) and depressive symptoms, not surprisingly, are positively correlated and share a relatively large amount of variance (r = 0.57; see Table 2). The findings for Extraversion and Neuroticism suggest that there are limits to the complementary fit model. Perhaps personality traits that have somewhat lower or moderate correlations with the environmental variable (religious capital in this study) are the most likely to show the complimentary fit effect. Furthermore, if either the personality trait (in this case, neuroticism) or the environmental variable is too highly correlated with the outcome variable (depressive symptomology), then there is less likely to be a complimentary fit. Examining the moderators of the complimentary fit model is an area for future research.
Limitations of the Present Study
There are several limitations to the present study. First, we rely on self-report data. Participants may have been influenced by social desirability concerns in responding or influenced by inaccurate memory for their depressive symptoms. Second, while our sample cannot be considered representative of the entire African American population, it was chosen using probability-based methods, was a very large national sampling of African Americans and, unlike many other studies, included a large number of African American men. Finally, this was a cross-sectional study so we cannot infer causality.
Future Research and Conclusions
Future research should further explore the applicability as well as the limitations of the complementary fit model. Our data demonstrated that the model predicted results for two of the five personality traits examined. Future research should also examine the mediation relationships between personality, religious capital, and mental health functioning. Some components of religious capital, such as social support, may actually mediate personality effects on mental health. Personality may determine the extent to which people elicit support or capital which in turn may influence health (Amirkhan, Risinger, & Swickert, 1995; Lakey, 1989; Lakey & Dickinson, 1994; Pierce, Lakey, Sarason, Sarason, & Joseph, 1997; Swickert, 2009). Our correlational data are consistent with this view given the significant intercorrelations between personality, religious capital, and depressive symptomology (see Table 2). Another avenue of future research, consistent with social cognitive theory and the person-environment fit model, would be to explore these variables longitudinally, perhaps using a reciprocal determinism approach (Bandura, 1999) to examine how personality, perceived religious capital, and mental health influence one another. Additionally, future research should examine clusters of various personality variables and their relationship to mental health. For example, Vollrath and Torgersen (2002) found that persons with the combination of low conscientiousness and either high extraversion (Impulsives, Hedonists) or high neuroticism (Insecures) were highly likely to engage in risky health behaviors. Our study suggests that examining these personality clusters in combination with variables such as religious capital might improve the prediction of mental health. Finally, the current study was concerned with depressive symptomology, but similar research examining other aspects of mental health (e.g., anxiety) as well as physical health behaviors (e.g., diet, physical activity) could be very beneficial.
In conclusion, this study reinforces the importance of examining the moderation effects of person and contextual variables in understanding mental health outcomes. As with the research on religious coping (e.g., Ross et al., 2009), this information can be of use to practitioners in designing interventions for religious African American clients, including the use of capital related to faith-based organizations. Interventions (e.g., Wingood et al., 2013) that help clients better utilize their religious capital (i.e., seeking out support, forming more connections, increasing participation in one’s faith community) may help lower or prevent depressive symptoms even if the client is lower on conscientious or openness, for example. In addition, interventions that decrease depressive symptomology may improve future religious capital use. Some Africentric interventions for African American youth include activities that focus on religious capital-related constructs, such as religiosity/spirituality, collectivism, and interdependence (D. J. Gilbert, Harvey, & Belgrave, 2009). These types of interventions build on our knowledge of the cultural importance of community and faith-based institutions, as well as personality, which have been demonstrated in prior research on African Americans (Bell-Toliver & Wilkerson, 2011; Gibson, 2007).
Footnotes
Acknowledgements
The team would like to acknowledge the work of Ms. Penny Southward, MPPM, and that of OpinionAmerica, who conducted participant recruitment and data collection activities for the present study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from the Duke University Center for Spirituality, Theology, and Health, through the John Templeton Foundation (#11993) and was approved by the University of Maryland Institutional Review Board (#08-0329).