
Abstract
Often cited as a developmental and cultural resource, religion has been widely studied. However, few studies have explored the relationship between nonorganizational religious involvement (NRI) and psychosocial well-being among Black youth or within ethnic groups of Black youth. This study examined this relationship among 1,170 African American and Caribbean Black youth who participated in the National Survey of American Life–Adolescent Supplement study. Moderated hierarchical regression results showed significant main effects of NRI on life satisfaction, self-esteem, coping, and depressive symptoms after accounting for study covariates (i.e., age, gender, family income, denomination, ethnicity, religious service attendance, and religious socialization). No significant interaction effects were observed between NRI and ethnicity on any of the psychosocial well-being outcomes. Results illuminate a promotive effect of NRI in this sample. Though no significant ethnicity and religiosity interaction effects were observed, findings suggest the importance of NRI as a key intervention target to support better psychosocial well-being among Black youth, in an effort to promote overall youth development.
Religious involvement plays an important role in the lives of Black Americans. For over 300 years, religious institutions, such as the Black church, have provided practical, civic, and spiritual support to congregants and the surrounding community at large. Subsequently, 93% of African American and 89% of Caribbean Black adults have reported religion and spirituality as important factors in their lives (Taylor & Chatters, 2010). Also, Black youth have ascribed higher levels of importance to their faith compared with other racial or ethnic subgroups of adolescents (i.e., Hispanic, Asian American, Native American, and White; Wallace et al., 2016). As such, religion may function as a developmental and cultural resource that promotes positive adjustment, and researchers have only recently begun to address the diverse modicums through which Black youth experience religion (Gooden & McMahon, 2016). Black youth may attend religious services and participate in youth-oriented religious programming and activities (e.g., youth groups). Many also have opportunities to be active participants in religious services (e.g., sacred dance, choir, mime; Streaty Wimberly, 2014). Being involved in a religious community creates opportunities for adolescents to receive and provide church support (Hope, Taylor, et al., 2019). Furthermore, Black churches often foster youth resilience by reducing the harmful effects of high-risk activities that jeopardize future thriving (see e.g., Kim et al., 2017).
Broadly, religious involvement has corresponded with a wide range of well-being outcomes for Black adolescents (Butler-Barnes et al., 2016; Kim et al., 2017), including greater psychosocial well-being (Rose et al., 2014) and positive self-concept (Toldson & Anderson, 2010). Black adolescents with higher levels of religiosity have tended to report lower levels of subjective stigmatization—that is, the extent to which adolescents internalized negative messages about the group(s) with which they identified and more positive racial identity (Brega & Coleman, 1999; Taggart et al., 2019). Adolescent participation in religious services may create spaces for adolescents to thrive. For example, one Black youth observed the meaningfulness of involvement in dance ministry as while observing the positive response from others (Streaty Wimberly, 2014). Furthermore, African American adolescents with greater religious beliefs tended to exhibit fewer high-risk behaviors (e.g., delinquency; Kim et al., 2017). Organizational religious involvement and natural mentorship were also found to buffer the effects of community violence on African American adolescent girls’ future sexual risk behaviors (Hope, Lee, et al., 2019). Much of the scholarship on Black adolescents has addressed organizational religious involvement (e.g., service attendance) and has emphasized the interpersonal and corporate aspects of religious attitudes, beliefs, and practices (Breland-Noble et al., 2015). The beliefs and traditions acquired in organizational settings may, however, be used in other contexts or practiced independently. The current study explores the influence of nonorganizational religious involvement (NRI) on psychosocial well-being among African American and Caribbean Black youth.
Nonorganizational Religious Involvement
NRI reflects internalized religious beliefs, devotional practices (e.g., prayer, reading religious texts), and other religious practices independent of others (e.g., memorizing scriptures and the tenets of faith; Chatters et al., 2009; Salas-Wright et al., 2012). However, the ways in which scholars have operationalized NRI vary. For example, NRI has been measured by some as the subjective importance of religion (i.e., how important a role religion plays in life) or the frequency of praying (Burdette & Hill, 2009; Nonnemaker et al., 2003). Other scholars measure NRI as the degree to which religious beliefs are important and influence decision making (Salas-Wright et al., 2017). In addition, items and scales assessing prayer and/or other forms of NRI may be included within comprehensive measures of overall or general religious involvement (Cole-Lewis et al., 2016; Rew & Wong, 2006). In turn, this approach may obscure the specific and direct effects of NRI on well-being and other outcomes.
Theoretical Frameworks
Faith development theory (Fowler, 1981) and psychosocial theory (Erikson, 1968) guided the current study. Faith development theory proposes that faith is central to the development of an individual’s principles and beliefs, which in turn provide life guidance, connect individuals to others, root individual standards within a greater framework, and equip individuals to handle life challenges. Inevitably, as faith develops and youth are increasingly exposed to religion, a greater connection to God is nurtured (Fowler & Dell, 2006). Of the eight stages of faith, during adolescence the synthetic-conventional stage of faith emerges and can produce expansion of cognitive functioning, which facilitates adolescents’ critical thinking, meaning making, and abstract thought, generally (Piaget, 1976) and with regard to religious development (Fowler & Dell, 2006; Markstrom et al., 2010). The growth of cognitive functioning can shape youth religious involvement both in and out of religious settings (Salas-Wright et al., 2012) and, importantly, facilitate attitudes, beliefs, rituals, and practices (e.g., NRI activities) that may help youth navigate and cope with stressors (Bryant-Davis et al., 2012).
Concurrently, adolescence is a time of identity development. Psychosocial theory posits eight stages of development across the life span (Erikson, 1968). Each stage includes psychosocial crises that when resolved produce a sense of competence and self-esteem (Erikson & Erikson, 1998). Youth are tasked with managing the psychosocial crisis of identity versus role confusion, which involves their exploration of personal values and beliefs in comparison with those of their peers (Erikson & Erikson, 1998). Identity may also include religious identity, which could comprise pursuing sanctification, understanding and accepting love, and attachment to beliefs and values consistent with or different from others they consider significant (Haley, 2014; Hardy et al., 2011). As such, increasingly independent youth might explore their personal relationship with God through NRI, engaging in individualized activities such as praying, reading sacred text, or other personal expressions of faith.
Taken together, during adolescence, growth in cognitive functioning and an enhanced sense of meaning making, along with a developing sense of identity, specifically religious identity, can result in the development of cognitive and behavioral resources such as those specific to NRI (e.g., prayer). In turn, these resources, in the form of NRI, may help youth address emotional challenges as well as promote positive experiences that undergird thriving. For example, NRI, through prayer, may produce faith that God provides strength and understands what the believer is experiencing (Levin, 2010). Similarly, interactions with God may empower adolescents by increasing efficacy (Bryant-Davis et al., 2012). Concomitantly, some effects of religious involvement function therapeutically: Adolescents may experience “salutary emotions” after praying to God (Levin, 2010), which may be used to address emotional problems and challenging circumstances (Lee et al., 2018). Similarly, internalized religious principles (e.g., messages from sermons) and beliefs could promote social development; as such, adolescents may better manage interpersonal conflicts, which could reduce stress and improve well-being (Shepperd et al., 2015; Smith et al., 2003). Overall, behavioral, cognitive, and social processes could help shape Black adolescents’ use of NRI activities, with subsequent salubrious benefit, such as improved psychosocial well-being and positive development. Resultantly, NRI may be reflective of and supported by the ongoing developmental tasks of adolescence.
NRI and Black Youth Outcomes
When scholars have explored NRI among Black youth, they have tended to primarily focus on prayer. Found across many faith traditions, prayer encompasses various modes of communication with God or another higher power (Levin, 2016). In the United States, Black adolescents have prayed frequently (Lee & Neblett, 2019) and more often compared with their counterparts in other racial and ethnic groups (Smith et al., 2003). For example, African American adolescent boys reported praying privately at least once a week (Bruce et al., 2016). Many reported praying for divine help and intervention to support academic achievement (Butler-Barnes et al., 2012). Additionally, some Black adolescents viewed prayer and reading the Bible as hope-promoting activities (Harley & Hunn, 2015). However, prayer is not the only way through which NRI may manifest. In one study, Black college students reported that listening to gospel music empowered them to integrate religious values into daily life and decision making, and provided them with security and comfort during stressful times (Williams & Banjo, 2013).
NRI may also be influenced by religious affiliation. For example, approximately 79% of Black Americans in the United States identified as Christian, and the majority of those reported attending predominantly Black churches (Masci, 2018). Subsequently, involvement in these settings may shape how adolescents approach NRI. For example, some adolescents involved in Black churches reported that they were counseled to use prayer as the primary way to deal with mental health issues, instead of seeking out mental health professionals (e.g., therapists; Breland-Noble et al., 2015). In other contexts, demographic factors (e.g., age, educational attainment) for Black adolescents may increase the likelihood of clergy referring congregants to outside mental health treatment and resources (Allen et al., 2010). Furthermore, Black adolescents are affiliated and involved with other religious traditions outside Christianity (Johnson, 2015) or may consider themselves spiritual but not religious (e.g., Cooper & Mitra, 2018). As such, NRI activities may function differently across affiliations and faiths and inevitably shape how adolescents integrate NRI into their lives.
Few studies have linked NRI to well-being outcomes for Black youth. Having a relationship with God has been shown to promote psychological well-being for African American adolescent girls (Butler-Barnes et al., 2018). Exploring ethnic group differences, Butler-Barnes et al. (2016) found a positive correlation between prayer and self-esteem for African American youth, whereas, further analyses showed that prayer buffered the negative effect of discrimination on depression for Caribbean Black youth. Furthermore, Shannon et al. (2013) reported significant positive correlations between religious coping and daily spiritual experiences, and life satisfaction among African American youth. Other scholars have documented the direct and indirect effects of NRI on substance use (Fletcher & Kumar, 2014; Salas-Wright et al., 2017). Some African American adolescents and emerging adults harness prayer as a coping strategy to process and navigate adversity (Dill, 2017; Molock & Barksdale, 2013). Other youth may utilize multiple NRI activities concurrently. In one study, African American emerging adult women reported that praying and reading the Bible helped them address stressful academic experiences (Patton & McClure, 2009). Going forward, more information is needed regarding the multifaceted roles of different types of NRI in supporting and promoting Black youth well-being.
A Focus on Psychosocial Well-Being
Recent empirical trends suggest that the absence of a mental health disorder alone does not equate to positive well-being (Stewart-Brown, 2016; Suldo & Shaffer, 2008) and both should be measured to comprehensively assess mental health (e.g., Antaramian et al., 2010; Suldo & Shaffer, 2008). Concomitantly, the World Health Organization (2018) defines mental health as a state of well-being in which an individual realizes his or her own abilities, can cope with the normal stresses of life, can work productively and is able to make a contribution to his or her own community. (para. 2)
Consistent with recent conceptualizations, our study explores both positive and negative aspects of psychosocial well-being. Positive aspects include life satisfaction (overall cognitive evaluation of one’s life; Diener, 2000; Driscoll et al., 2015), self-esteem (e.g., appreciation of self; Lanier et al., 2017), mastery (perception about control in life; Benson et al., 1999; Rose et al., 2017), and active coping (heightened determination to succeed; Blackmon et al., 2016). Negative aspects include perceived stress (e.g., Greer et al., 2015) and depressive symptoms (Substance Abuse and Mental Health Services Administration, 2018). Although each respective indicator has been extensively explored in the youth well-being literature, our study endeavors to generate a more comprehensive and holistic understanding of psychosocial well-being among Black adolescents.
Prospective Ethnic Group Differences
Religious differences between African American and Caribbean Blacks may be rooted in cultural and historical contexts, immigration experiences, and socialization messages (Butler-Barnes et al., 2016; Chatters et al., 2009). For example, the Black church in African American narratives maintains a historic and ongoing role in community activism and commitment to education (e.g., Jordan & Wilson, 2017). Conversely, within the United States, intersections of Blackness and immigration status for Caribbean Blacks may undergird religious affiliation and shape congregants’ involvement, (e.g., religious involvement in faith settings with a substantial immigrant population; A. W. Nguyen et al., 2016; Waters, 1999). In these settings, aspects of religious involvement (and subsequent NRI) of Black youth may remain similar or vary across ethnic groups. For example, Black immigrant youth may participate in communities that host culturally specific activities for congregants and noncongregants alike. In addition, the function of religious involvement may differ by ethnicity. Indeed, service attendance and prayer have functioned protectively against the effects of discrimination on depressive symptoms in Caribbean Black youth but not for African American youth (Butler-Barnes et al., 2016). Furthermore, Hope, Taylor, et al. (2019) found that young Caribbean Black adolescents tended to provide more church support whereas African American youth tended to receive more support.
The Current Study
Our study explores the influence of NRI on psychosocial well-being outcomes among African American and Caribbean Black adolescents (ages 13-17 years) in the United States. Often, when aspects of NRI are explored in relation to well-being, only one aspect of NRI is addressed. Also, the majority of NRI research conducted among Black samples has focused on adults (Hays & Lincoln, 2017; Taylor et al., 2011), and the extant research on psychosocial outcomes among African American and Caribbean Black adolescents who utilize NRI has been minimal. Accordingly, we assess NRI with five indicators (prayer, requesting prayer, watching or listening to religious programs, listening to religious music, reading religious materials). Given the few studies that have shown significant positive associations between prayer and well-being in both Black youth and Black adult samples, we hypothesize that Black youth, regardless of ethnicity, with greater NRI will report greater psychosocial well-being. Based on previous studies, we expect that there will be a moderating role of ethnicity for the association between NRI and psychosocial well-being. However, given the limited information on this subject, this hypothesis is exploratory.
Method
Study Design and Sample
Data for this study are from the National Survey of American Life–Adolescent Supplement (NSAL-A). This sample is based on the NSAL (2001-2003), which is the largest and most comprehensive study on mental disorders and mental health among Black Americans (Jackson et al., 2004). Using a cross-sectional survey design and stratified and clustered sampling approach, the nationally representative sample included 3,570 African Americans (AAs), 1,621 Blacks of Caribbean descent (CBs), and 1,006 non-Hispanic Whites, aged 18 years and older (see Jackson et al., 2004).
All AA and CB households with an adult participant in the NSAL were screened for eligible AA and CB adolescents. A randomized procedure was used to select adolescents (Joe et al., 2009). The NSAL-A sample was weighted to adjust for variation in the probabilities of selection within households and nonresponse rates of adolescents and households. The weighted data were poststratified to approximate the national population distributions for gender (male and female subjects) and age (13-, 14-, 15-, 16-, and 17-year-olds) subgroups among Black youth (Joe et al., 2009). This weighting design allowed for accurate inferences about the national population of Black youth, and the sample design and weight characteristics classified the NSAL-A as a complex sample survey. The original adolescent sample was 1,193 cases; 23 cases were removed because of age at interview (18+). Given missing data, the current study’s analytic sample comprised AAs (n = 777) and CBs (n = 342) aged 13 to 17 years, with 536 (48%) boys and 583 (52%) girls.
Measures
Nonorganizational Religious Involvement
Five items from the National Survey of Black Americans assessed the frequency of adolescents’ NRI (Jackson & Neighbors, 1997). Using 4-point responses scaled from 1 = never to 4 = very often, the participants answered how frequently they read religious books or other religious materials, watched or listened to religious programs on TV or radio, listened to religious music, prayed, and requested prayer from someone else. Responses were averaged, with higher scores indicating greater frequency of NRI activities. Missing items were excluded from both the numerator and the denominator (Schafer & Graham, 2002). The reliability estimate of the NRI scores was .72. Exploratory factor analysis was conducted to test the structural validity of the NRI construct, using the principal axis factor method with no rotation. Results of the factor analysis indicated one factor—with an eigenvalue greater than 1—that explained most of the unique variance. Factor coefficients ranged from .46 to .69 for the five items. This evidence supported the use of a one-factor structure for this sample. The variable was centered at the mean (
Psychosocial Well-Being
Six indicators (self-esteem, active coping, mastery, life satisfaction, depression, and perceived stress) represented psychosocial well-being.
Life satisfaction
A single-item question—“How satisfied with your life as a whole would you say you are these days?”—assessed adolescents’ level of life satisfaction, conceptualized as an overall cognitive evaluation of one’s life (Diener, 2000). Responses to items ranged from 1 = very satisfied to 4 = very dissatisfied. The item was reverse coded such that higher mean scores indicated greater life satisfaction.
Self-esteem
Self-esteem was measured by the Rosenberg Self-Esteem Scale (RSES), originally designed to measure the self-esteem of high school students (Rosenberg, 1965). The 10-item scale assesses global self-esteem, a subjective evaluation of personal worth, by measuring both positive and negative feelings about oneself (e.g., “On the whole, I am satisfied with myself”). As such, this Likert-type scale includes five positively worded and five negatively worded items, scaled on 4-point responses ranging from 1 = strongly agree to 4 = strongly disagree. The positively worded items were reverse scored and averaged, so that higher mean scores indicated better self-esteem. Prior research has demonstrated RSES scores to be internally consistent with alpha estimates ranging from .80 to .84 (Lockett & Harrell, 2003; Moses, 2009; Tynes et al., 2012). Furthermore, the research has provided support for the construct validity of the RSES. For example, RSES scores were correlated in positive directions with other self-esteem measures, such as the Single Item Self-Esteem Measure (median r = .73-.80, p < .01), and similar constructs such as optimism (r = .48, p < .01; Robins et al., 2001). Similarly, Hatcher and Hall (2009) reported negative correlations between the RSES and depression (r = −.67, p < .01) as well as negative thinking (r = −.79, p < .01). In this sample, the alpha estimate for the RSES scores was .72.
Mastery
Mastery was measured by Pearlin’s Mastery Scale (Pearlin & Schooler, 1978). This seven-item Likert-type scale measures individuals’ perception of control over their own life chances. The adolescents completed items (e.g., “I can do just about anything I set my mind to”) scaled on 4-point responses ranging from 1 = strongly agree to 4 = strongly disagree. Positively worded items were reverse-scored and a mean calculated such that higher mean scores indicated a greater sense of mastery. Previous research has indicated that mastery scores were reliable, with alpha estimates ranging from .70 to .77 (Grossman et al., 2011; Moses, 2009). There is a paucity of research on the validity of Pearlin’s Mastery Scale despite its common use in studies (Eklund et al., 2012). However, Marshall and Lang (1990) found the scale to have good construct validity via a positive correlation with dispositional optimism (favorable expectations for life outcomes; r = .71, p < .001) and a negative correlation with depression (r = −.61, p < .001). Marshall and Lang (1990) also reported predictive validity due to mastery having a unique significant influence on depression (β = −.53, p < .001). In this study’s sample, the alpha estimate for the mastery scores was .68.
Active coping
Coping was assessed using the John Henryism scale (James, 1994). The 12-item Likert-type scale was developed for AAs and assesses active coping, conceptualized as efficacious mental and physical vigor, a strong commitment to hard work, and a single-minded determination to succeed (James, 1994). A sample item from the scale was “Hard work has really helped me to get ahead in life.” The items were scaled on 4-point responses ranging from 1 = completely true to 4 = completely false. Each item was reverse coded and summed, with higher scores indicating higher levels of active coping. Results of previous studies provided support for internal consistency reliability, with alpha estimates ranging from .70 to .84 (e.g., Brenner et al., 2013; Wright et al., 1996). Furthermore, Wright et al. (1996) provided evidence of construct validity through reported moderate correlations between the John Henryism scale and self-esteem scores (r = .40, p < .001) as well as the Anger Reflection subscale score (r = .36, p < .001) but not the Anger In (r = −.02, p > .05) or Out (r = −.11, p > .05) subscale scores of the Spielberger Anger Expression Scale (Spielberger et al., 1985). In this study’s sample, the alpha estimate for the John Henryism scores was .71.
Perceived stress
Perceived stress was measured by Cohen’s Perceived Stress Scale (PSS; Cohen et al., 1983). This 14-item Likert-type scale assessed the level at which adolescents evaluate life situations as stressful (e.g., “In the last month, how often have you felt nervous and stressed out?”). Items were scaled on 5-point responses ranging from 1 = never to 5 = very often. Positively worded items were reverse scored and summed to produce a total score; higher scores indicated greater perceived stress. Across previous research, alpha estimates for PSS scores ranged from .82 to .87 (Cohen et al., 1983; Greer et al., 2015; Mahon et al., 2007). Furthermore, Cohen at al. (1983) reported small to moderate correlations between the PSS and life events scores (r = .20-.39, p < .01), providing evidence of concurrent validity. Additionally, PSS scores have predicted depressive symptom scores (rs = .65 and .76, p < .001) and social anxiety scores (rs = .37 and .48, p < .001), indicating predictive validity (Cohen et al., 1983). In this study’s sample, the alpha estimate for the PSS scores was .77.
Depressive symptoms
A 12-item version of the Center for Epidemiologic Studies–Depression Scale (CES-D; Radloff, 1977) assessed the adolescents’ depressive symptoms in the past week (e.g., “I felt depressed”). Responses ranged from 0 = rarely or none of the time; less than 1 day to 3 = most or all of the time; 5 to 7 days. Positively worded items were reverse coded and summed such that higher scores reflected greater depressive symptoms. Internal consistency estimates obtained from previous research on the 12-item CES-D ranged from .64 to .83 (H. Nguyen et al., 2011; Prelow et al., 2006; Roberts & Sobhan, 1992). Roberts and Sobhan (1992) reported high reliability estimates between scores on the 12-item and 20-item CES-D (.96). Additionally, concurrent reliability was evidenced via correlations between scores on the CES-D and other measures of depressive symptoms (r = .37, p < .05) and general psychopathology (r = .54, p < .05). Similarly, CES-D scores discriminated between general and psychiatric inpatient populations, providing evidence of known-groups validity (Radloff, 1977). In this study’s sample, the alpha estimate for the CES-D scores was .68.
Covariates
Demographic covariates included age (continuous), gender (male = 0 or female = 1), family income in US$ (0-17,999, 18,000-31,999, 32,000-54,999, ≥55,000), denomination (Protestant, Pentecostal, Baptist, Catholic, other, or no religion [reference]), and ethnicity (AA = 0 or CB = 1). Adolescent ethnicity was based on the adult household from which the youth were sampled; these adults were participants in the NSAL (Sweetman et al., 2009). For the NSAL, AAs self-identified as Black but did not identify ancestral ties to the Caribbean. CBs self-identified as Black and endorsed Caribbean ancestral ties through identifying (a) they were of Caribbean or West Indian descent or (b) the Caribbean country they came from based on an interviewer-provided list (Heeringa et al., 2004; Jackson et al., 2004).
Two religious socialization questions and one question about organized religious involvement were used as additional covariates. The religious socialization questions were “About how often do your parents or the people who raised you talk with you about religion?” and “Not including parents or those who raised you, how often do other close relatives such as brothers, sisters, aunts, uncles, and grandparents talk with you about religion?” For both questions, responses ranged from 1 = very true to 5 = never. Both variables were recoded to 0 (never, rarely, sometimes) or 1 (often, very often). Religious attendance was a single-item question: “How often do you usually attend religious services?” Responses were 1 = nearly every day, 2 = at least once a week, 3 = a few times a month, 4 = a few times a year, 5 = less than once a year, and 6 = never. These responses were reverse coded and entered as four dummy variables with responses for never and less than once a year as the reference condition.
Procedures
Before the interview, informed consent and assent were obtained from the adolescent’s legal guardian and the adolescent, respectively. Most of the interviews were conducted in the adolescents’ homes by trained interviewers using a computer-assisted instrument, and 18% of the interviews were conducted either in part or fully by telephone. Respondents were paid $50 for their participation in the study; the overall response rate was 80.6% (80.4% for AAs and 83.5% for CBs). The appropriate institutional review board approved the study.
Data Analysis
All analyses were conducted using STATA/SE (16.0; StataCorp, 2019). Descriptive analyses means and standard errors, and bivariate correlations were calculated for the sample and by ethnicity. With NRI as our study predictor, six moderated hierarchical regression analyses were performed and reported using ordinary least squares and ordered logistic regression models conducted in three steps: (a) covariates only, (b) covariates plus NRI, and (c) covariates, NRI, and the interaction of NRI and ethnicity. Ordered logistic regression was used to explore the life satisfaction outcome given its ordinal level of measurement; results are presented as odds ratios (ORs) with 95% confidence intervals (CIs), based on the proportional odds assumption. Linear regression was used to examine the other five outcomes: self-esteem, mastery, coping, perceived stress, and depressive symptoms.
To estimate properly weighted coefficients and appropriate variance adjustments in the context of the complex survey design (cluster, weight, and stratum), Stata’s svy command was used. An a priori alpha of .05 was used for this study. Furthermore, effect sizes (represented by sr2 for each variable and also by ΔR2 for NRI) were expected to be in the low range (.02, small effect; Cohen, 1992), given the effects for NRI in prior studies (.01–.10; Butler-Barnes et al., 2018; Hills et al., 2006; Maltby et al., 1999). Finally, given the number of tests conducted, we used the Benjamini-Hochberg (1995) false discovery rate (FDR) adjustment. Rather than directly adjusting the significance level (i.e., the Bonferroni adjustment), the FDR adjustment controls for the expected rate of false rejection, leading to a higher level of power while addressing the problem of multiple testing. The method requires first ranking the p values from the multiple tests (in this case, six p values) from lowest to highest, dividing the rank by the total number of tests (rank ratio), and then multiplying this ratio by the FDR to calculate a new threshold (Benjamini-Hochberg, 1995). The p value from each test is then compared with this new adjusted p-value threshold. We assumed an FDR of 10%, meaning a 10% chance of finding at least one spurious statistically significant finding.
For each linear model, appropriate diagnostics pertaining to normality (normal probability plot) and homoskedasticity (scatterplot of residuals by NRI) were conducted. Transformations were undertaken for the outcome variables that deviated from normality to improve residual normality; none of these transformations resulted in substantively different findings. None of the results were sufficiently heteroskedastic to merit remediation. Outlier diagnostics were used to remove influential observations, resulting in substantive differences only for depressive symptoms. Finally, there were 51 missing values (about 4% of the sample), and to address this, all of the models were rerun using multiple imputation (of 10 data sets; Schafer & Graham, 2002). None of the models examined in this study were substantively different after imputation, and we reported the complete case analysis.
Results
Preliminary Analyses
Descriptive statistics of the study sample, and means and standard errors of the continuous variables, by ethnicity are presented in Table 1. Correlations of NRI and the six well-being outcomes are presented in Table 2. NRI was significantly correlated with life satisfaction (r = .11, p < .01), self-esteem (r = .13, p = .01), and coping (r = .21, p < .001) for AA youth. For CB youth, NRI was significantly correlated with life satisfaction (r = .15, p < .01) and coping (r = .23, p = .01).
Descriptive Statistics of the Sample and Main Study Variables by Ethnicity.
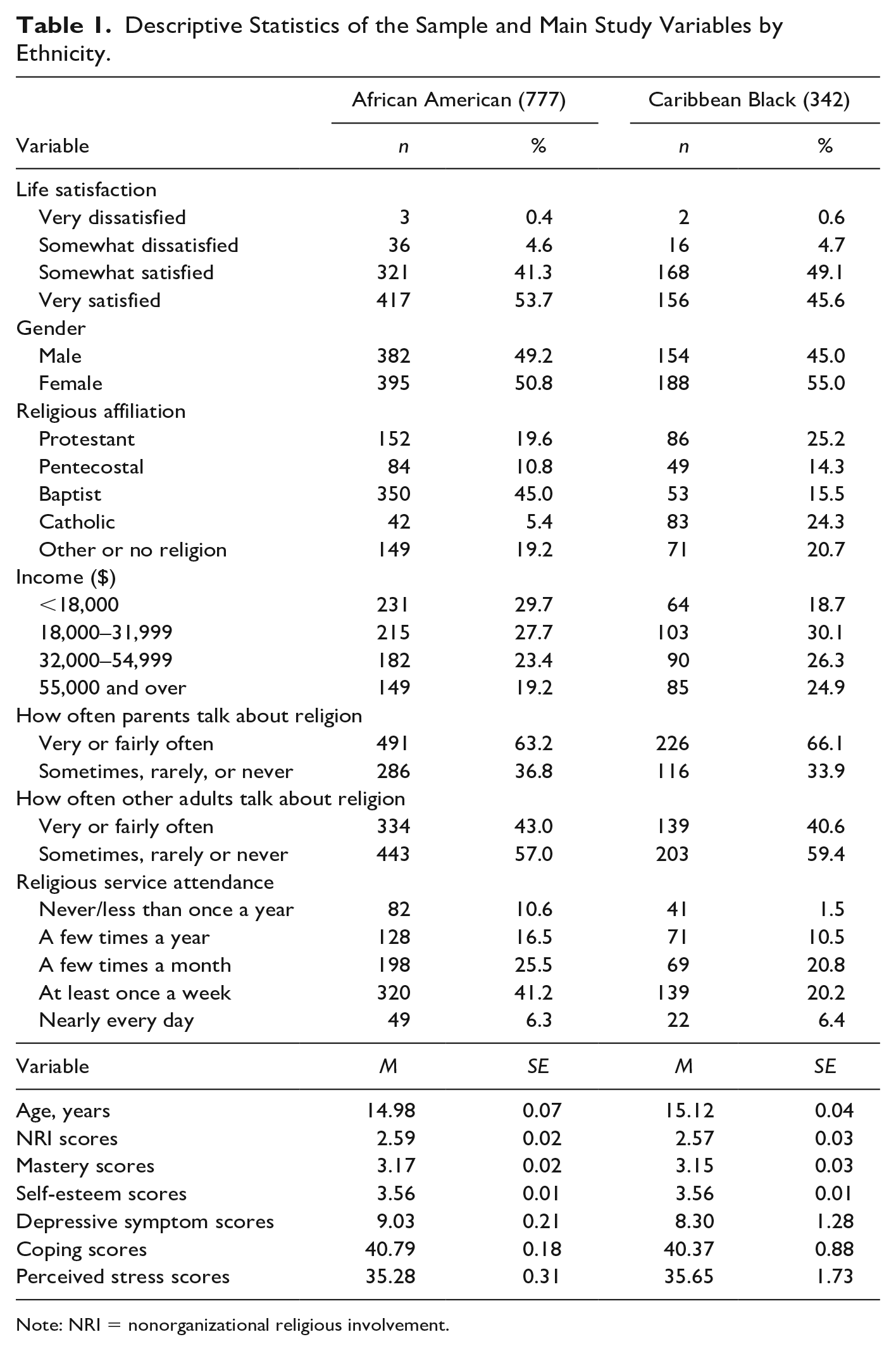
Note: NRI = nonorganizational religious involvement.
Pearson’s Correlation Coefficients for NRI and Well-Being Outcomes by Ethnicity.
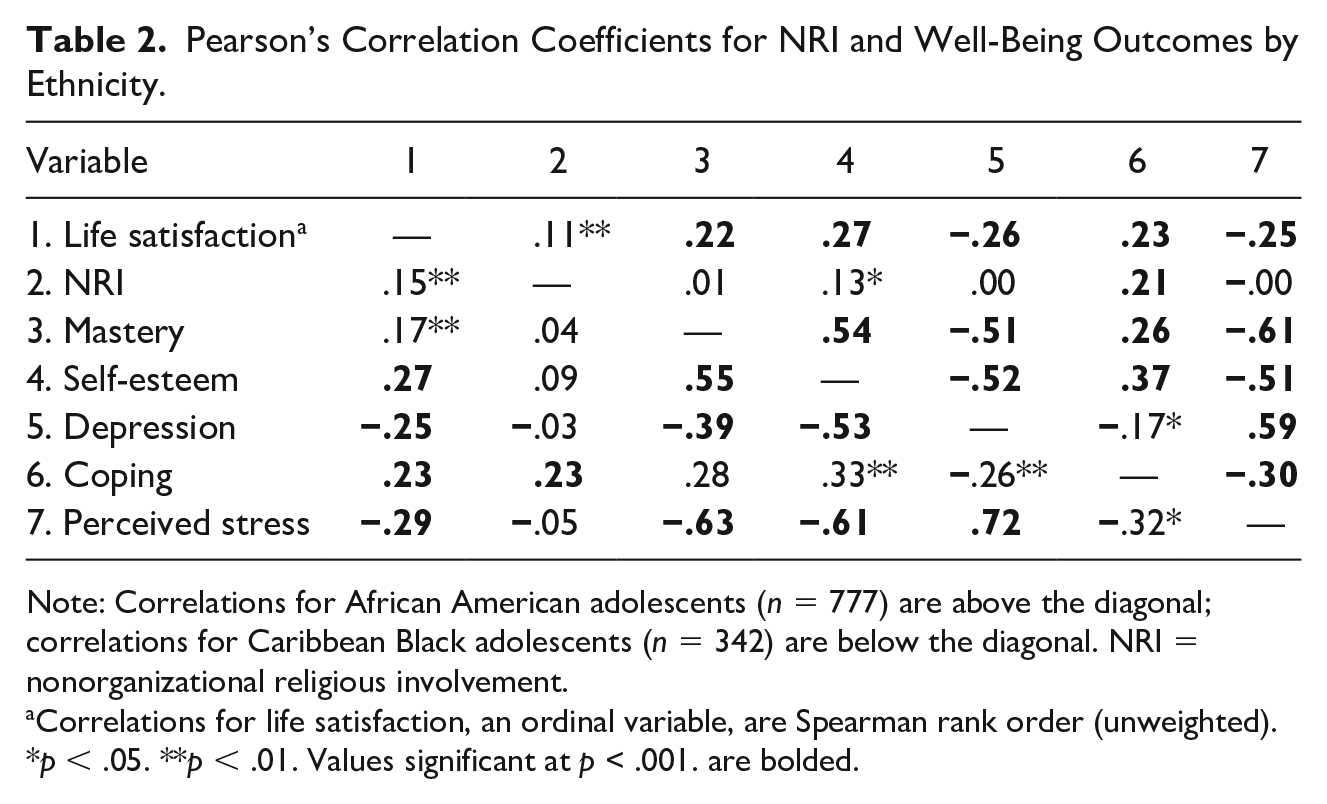
Note: Correlations for African American adolescents (n = 777) are above the diagonal; correlations for Caribbean Black adolescents (n = 342) are below the diagonal. NRI = nonorganizational religious involvement.
Correlations for life satisfaction, an ordinal variable, are Spearman rank order (unweighted).
p < .05. **p < .01. Values significant at p < .001. are bolded.
Moderated Regression Analyses
As noted, six moderated regressions were conducted, one for each of the following outcome variables: life satisfaction, self-esteem, mastery, coping, perceived stress, and depressive symptoms. In Block 1, the covariates entered were age, gender, family income, ethnicity, organized religious involvement, and religious socialization. In Block 2, NRI was entered, and in Block 3 the interaction effect of NRI by ethnicity was entered.
None of the moderation (interaction) terms were statistically significant, indicating that there was no statistically significant difference in the association between NRI and each outcome by ethnicity. Below, and in the following tables, we have reported the findings from Blocks 1 and 2. The tables also include Block 3. Notably, the tables are reported without reference to the Benjamini-Hochberg FDR adjustment, which, as we will discuss afterward, did not change any of the significant findings.
Life satisfaction
Ordered logistic regression results (Table 3) showed that NRI for life satisfaction after controlling for the other variables was statistically significant (OR = 1.38; 95% CI [1.09, 1.76], p = .01); every 1-point increase in NRI score was associated with a 38% increase in odds of being in a higher versus lower satisfaction group.
Hierarchical Logistic Regression Predicting Life Satisfaction.

Note: N = 1,081; OR = odds ratio; CI = confidence interval; NRI = nonorganizational religious involvement.
Reference categories: a <$18,000. b No religious affiliation. c Never or less than once a year.
p < .05. **p < .01. ***p < .001.
Self-esteem
For self-esteem (Table 4), covariates alone explained 3.6% of the variance. After adding NRI in Block 2, the model explained 4.3% of the variance. Higher levels of NRI were significantly associated with higher levels of self-esteem (b = .06, 95% CI [0.01, 0.11], p = .03, ΔR2 = .01).
Hierarchical Linear Regression Analysis Predicting Self-Esteem.
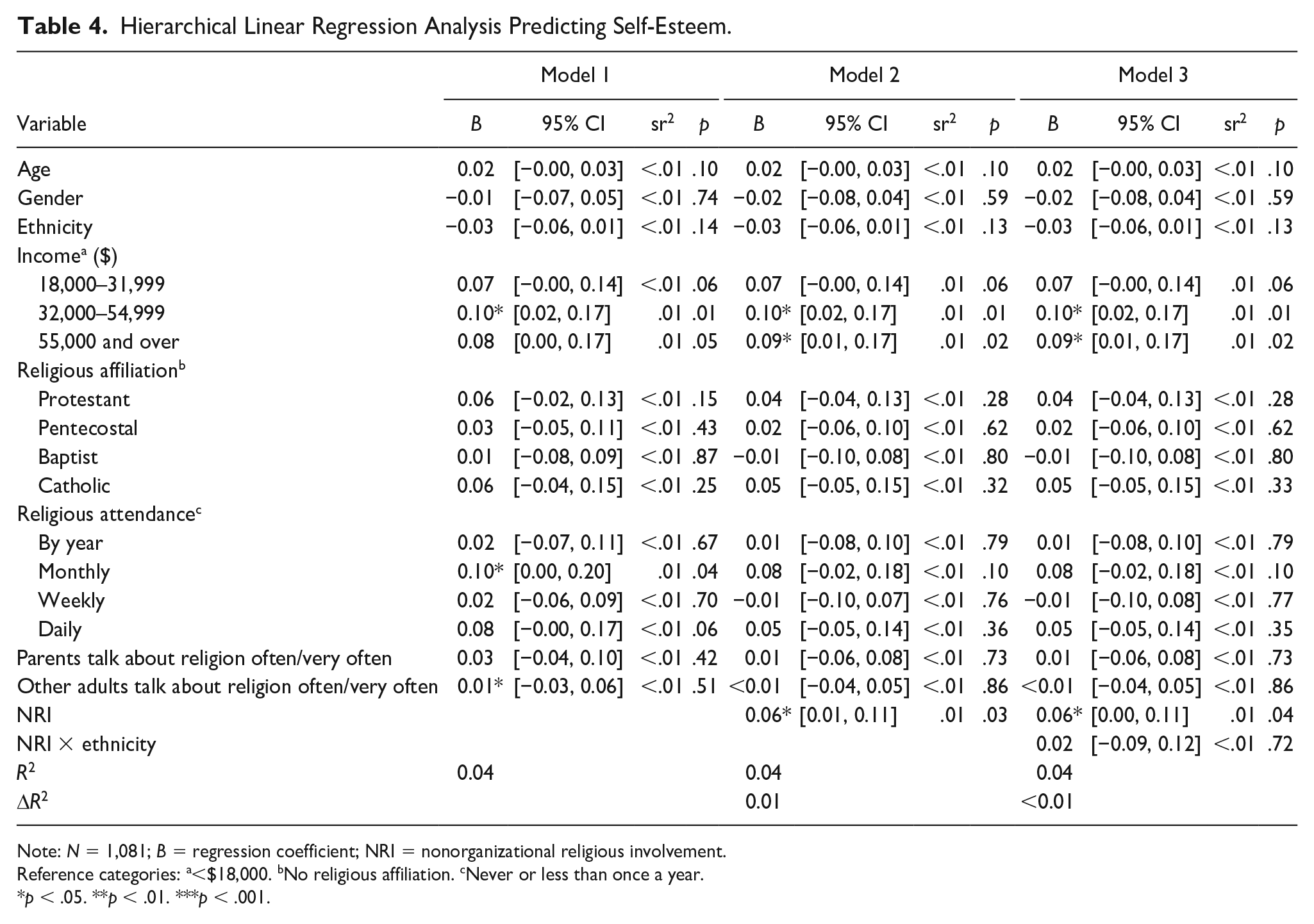
Note: N = 1,081; B = regression coefficient; NRI = nonorganizational religious involvement.
Reference categories: a<$18,000. bNo religious affiliation. cNever or less than once a year.
p < .05. **p < .01. ***p < .001.
Mastery
Covariates explained 6.1% of the variance in mastery in Block 1; after adding NRI in Block 2, this increased to 6.4% (ΔR2 = .002). NRI was not statistically significant in the final model (b = .04, 95% CI [−.04, .12], p = .27, ΔR2 < .01).
Coping
For coping (Table 5), covariates alone accounted for 3% of the variance. In Block 2, NRI explained an additional 5.5% of the variance. NRI was significantly associated with coping (b = 1.7, 95% CI [1.1, 2.4], p < .001, ΔR2 = .06).
Hierarchical Linear Regression Analysis Predicting Coping.
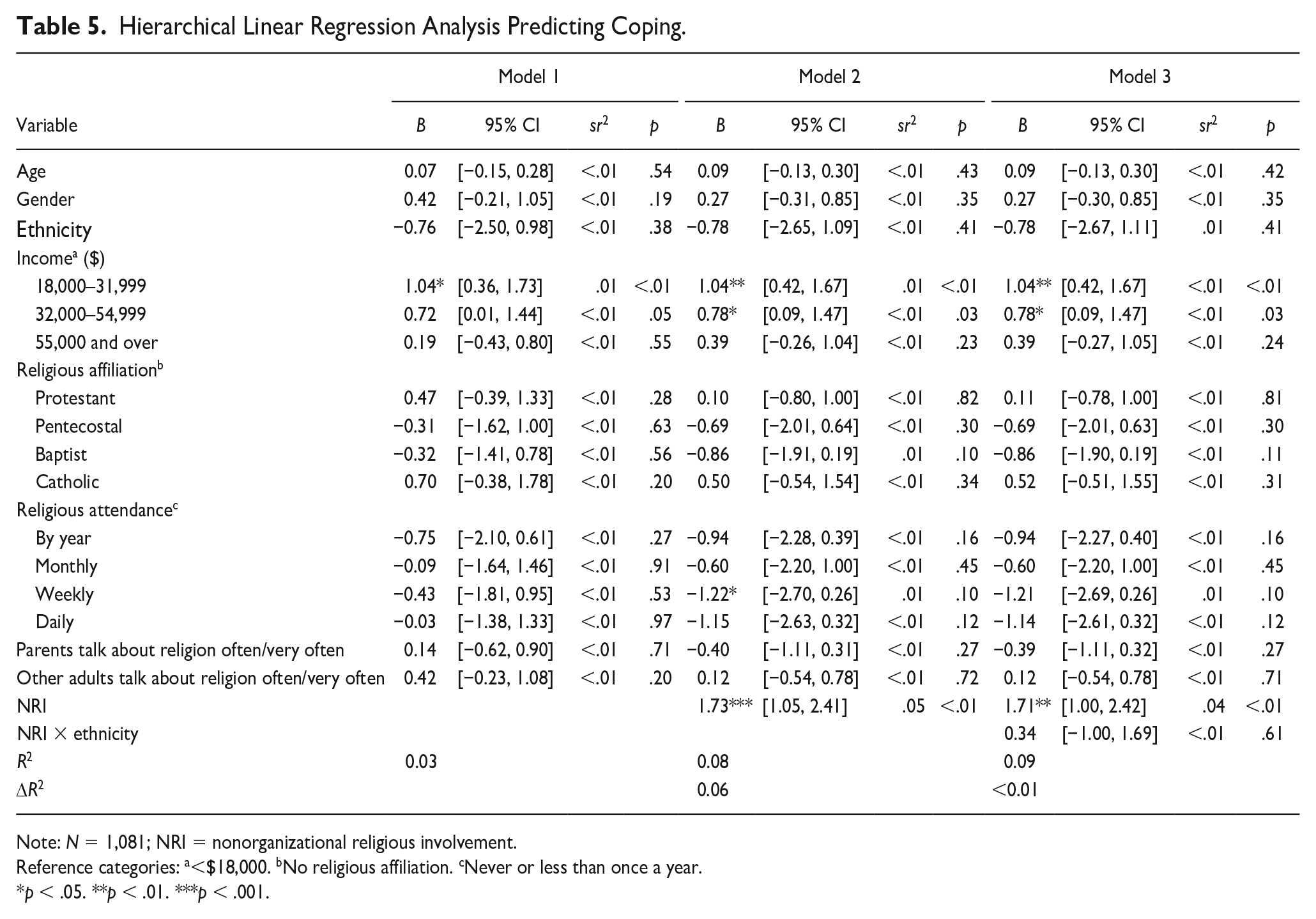
Note: N = 1,081; NRI = nonorganizational religious involvement.
Reference categories: a<$18,000. bNo religious affiliation. cNever or less than once a year.
p < .05. **p < .01. ***p < .001.
Perceived stress
Covariates explained 5.4% of the variance in perceived stress. Adding NRI in Block 2 had a negligible impact on the explained variance, and NRI was not statistically significant (b = .14, 95% CI [−1.2, 1.5], p = .83, ΔR2 < .001).
Depressive symptoms
Covariates alone explained 2.5% of the variance in Block 1 (Table 6). Adding NRI in Block 2 explained less than 1% of the variance. NRI was a statistically significant predictor of depressive symptoms (b = .70, 95% CI [0.11, 1.29], p = .022, ΔR2 = .01).
Hierarchical Linear Regression Analysis Predicting Depression.
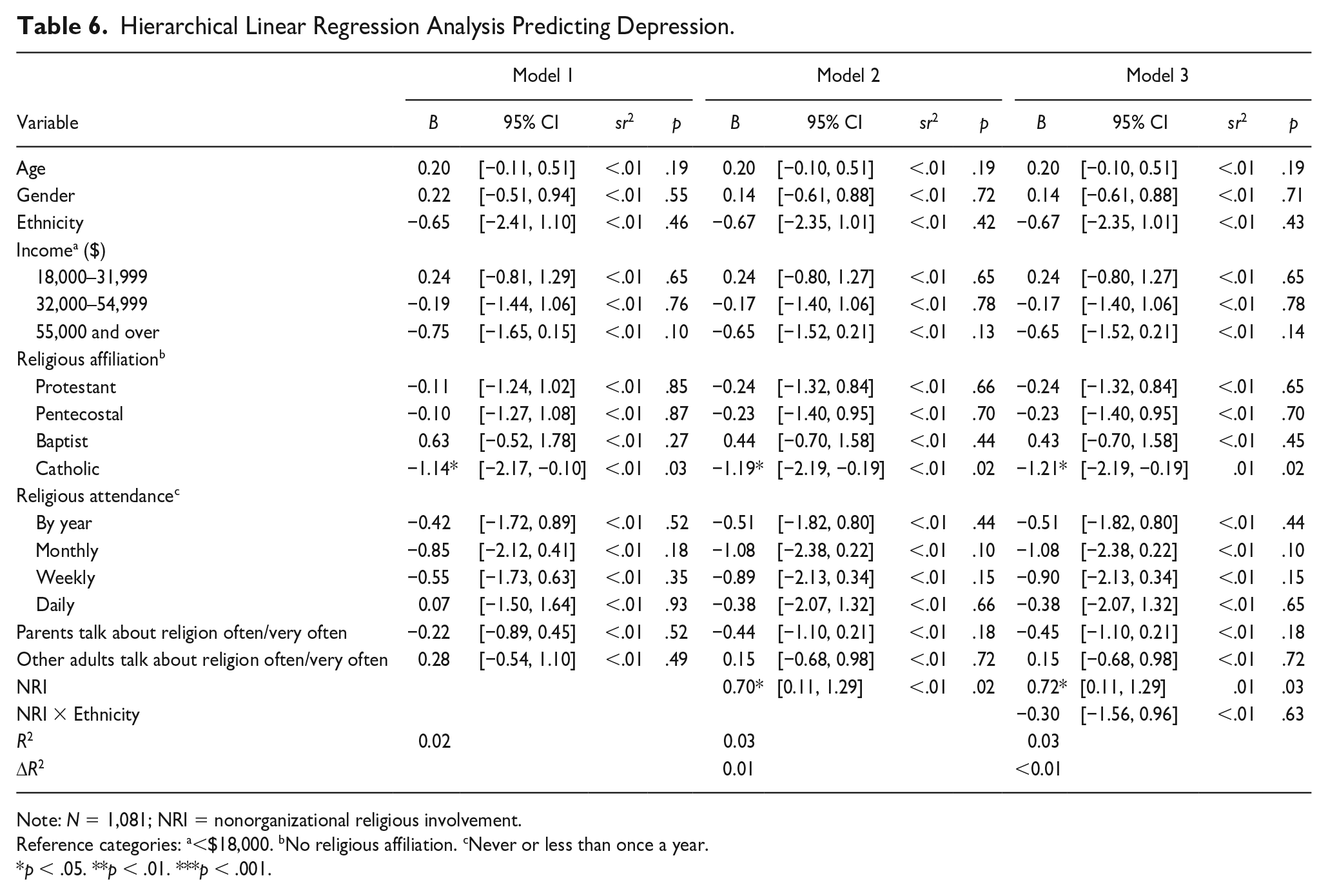
Note: N = 1,081; NRI = nonorganizational religious involvement.
Reference categories: a<$18,000. bNo religious affiliation. cNever or less than once a year.
p < .05. **p < .01. ***p < .001.
FDR Adjustment
Notably, the Benjamini-Hochberg FDR adjustment did not change any of the substantive findings. Coping, life satisfaction, depressive symptoms, and self-esteem were all statistically significant at an FDR of 0.10 (Table 7).
Benjamini-Hochberg FDR Adjustment for Hierarchical Linear Regression Analyses.
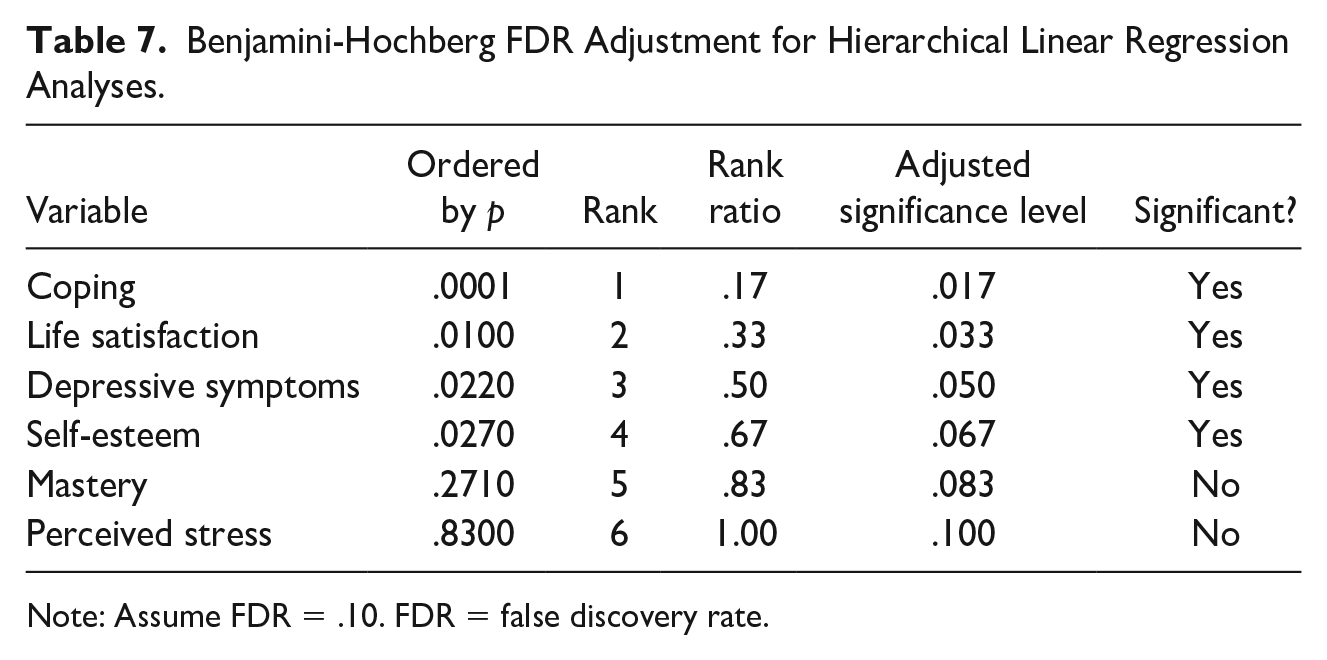
Note: Assume FDR = 0.10. FDR = false discovery rate.
Discussion
To date, studies on Black religiosity have tended to focus mainly on adults and the elderly (e.g., Hays & Lincoln, 2017; Taylor et al., 2011). Few studies have addressed nonorganizational aspects of religiosity for Black youth or how religion, broadly, promotes positive outcomes for Black youth (Gooden & McMahon, 2016; Rose et al., 2014). Faith development theory and psychosocial theory posit a relationship between enhanced cognitive functioning and identity formation among youth, which undergirds the integration of NRI activities and subsequent promotion of youth well-being. Because developmental processes within cultural and historical contexts shape Black adolescents’ perspectives on NRI and its integration in their lives, our study explored the influence of NRI on AA and CB youth’s psychosocial well-being. Our findings provide partial support for our first hypothesis in that NRI, regardless of ethnicity, was associated with four of our six outcomes: life satisfaction, self-esteem, coping, and depressive symptoms. However, the results did not support our second hypothesis regarding moderation by ethnic group.
Youth in our study who reported higher levels of NRI tended to express greater life satisfaction than their less religiously involved counterparts. This finding is consistent with previous studies documenting significant and positive associations between NRI factors and life satisfaction for emerging adults (Desmond et al., 2018), urban youth (Van Dyke et al., 2009), and AA youth (Shannon et al., 2013). This positive association may be partially explained by religious socialization (i.e., religious messages and values), which may undergird NRI. For example, adolescents may internalize these beliefs and messages, emphasizing the importance of forgiveness and praying for those who wrong them. In response to these beliefs, youth may choose to forgive others by talking to God, and perhaps, in turn, they experience comfort and relief. Similarly, adolescents may experience greater life satisfaction as NRI provides concrete ways to integrate internalized beliefs and reframe challenging life events in more positive ways (Holder et al., 2016).
Results suggest a small yet significant positive association between NRI and self-esteem, which is consistent with previous research supporting a positive correlation between prayer and self-esteem (Butler-Barnes et al., 2016), as well as having a relationship with God and better psychological well-being (Butler-Barnes et al., 2018). Our finding also adds to a broader research literature linking greater religiosity to higher self-esteem among adolescents, generally (e.g., Yonker et al., 2012). This finding may be partially explained by identity development processes (Erikson, 1968), a fundamental characteristic of adolescence. As adolescents explore various identities, they may examine, as part of their religious identity, the relevance of religiosity and associated belief systems (Davis & Kiang, 2016; Francis, 2013). Furthermore, some Black youth may be socialized within faith traditions that situate theological principles within the context of the Black American experience (Butler-Barnes et al., 2008; Martin & McAdoo, 2007), which could indirectly bolster self-esteem processes (Butler-Barnes et al., 2008). Increased exposure to images and messages may encourage conformity to an often unrealistic and unattainable ideal self (M. Anderson & Jiang, 2018). Nevertheless, principles promoting authenticity and intrapersonal connection with the divine through NRI activities (e.g., reading sacred texts) may contribute to self-acceptance and positive self-esteem (Schieman et al., 2017).
This study did not find any significant association between NRI and mastery, perhaps due to effects of theological principles. From existing theoretical perspectives, we posit that religious beliefs and practices might provide a sense of empowerment or increased capacity to manage life events (Bryant-Davis et al., 2012). However, some faith traditions consider “surrender to God” as an absence of subsequent action on the individual’s part. If socialized in these settings, youth’s NRI activities may be prioritized over or used in place of concurrent or subsequent action. In turn, this process may result in lower levels of or no significant changes in mastery (e.g., Schieman et al., 2003).
Stressful events, alongside normative adolescent challenges, often test youth’s ability to cope (Joyce et al., 2013). In our study, a small but significant effect was observed such that youth with greater NRI tended to report more active coping. Some religious traditions encourage youth to use NRI as faith-sustaining activities that can also be used to cope. Although we do not conceptualize NRI as a form of active coping, we consider that the adolescents in our study may use NRI to navigate stressful events (Dill, 2017; Molock & Barksdale, 2013). Considering faith development theory, the growth of cognitive functioning can facilitate attitudes, beliefs, rituals, and practices (e.g., NRI activities) that may help youth negotiate and manage different types of stressors (Bryant-Davis et al., 2012). For example, some Black adolescents living in high-risk neighborhoods may explore what it means for them to maintain engagement with God and use that engagement as a coping strategy in the midst of ongoing community adversity (Dill, 2017). Black Christian youth may harness Biblical truths (e.g., “Weeping may endure for a night, but joy comes in the morning”—found in Psalm 30:5, Amplified Bible) as a source of hope and perseverance in adversity. That said, the results did not support the hypothesized link between NRI and perceived stress, which was surprising given the established relationship between coping and stress (Aldwin, 2007; Compas et al., 2017). In our study, NRI may not directly mitigate stress but may do so through coping, a well-being outcome that was significantly related to NRI. Private beliefs and practices of the youth in this sample could be providing the strength and reassurance needed to deal with difficult circumstances, some of which are inherent in adolescent development. Our finding was not consistent with studies that supported the use of NRI activities to mitigate stress (e.g., Patton & McClure, 2009). However, although prayer was unrelated to perceived stress among AAs, it was related to perceived stress among CB youth (Butler-Barnes et al., 2016). More research is needed on NRI and stress among Black youth to better understand how these constructs relate to coping.
Finally, consistent with previous research, we found a small and significant effect of NRI on depressive symptoms. Scholars suggest a significant link between greater NRI and fewer depressive symptoms for some Black youth (Cole-Lewis et al., 2016), varying across ethnic groups (Butler-Barnes et al., 2016). For example, Butler-Barnes et al. (2016) identified prayer as a means of buffering the negative effects of discrimination on depression. Similar studies have indicated the significant influence of prayer on depression (J. W. Anderson & Nunnelley, 2016; Wachholtz & Sambamthoori, 2012). Our finding also supports a larger body of research that delineates the protective influence of broader constructs of religiosity on depressive symptoms among Black youth (Cullins et al., 2019).
Previous studies have documented some differences in the role of prayer for Black youth (e.g., Butler-Barnes et al., 2016); however, there were no significant interactions between NRI and ethnicity for any of our well-being outcomes. Although NRI is prevalent in Black adults, within-group ethnic differences in previous studies have indicated that AAs tend to request prayer for others whereas CBs read religious materials more frequently (e.g., Chatters et al., 2009). The nonsignificant link between NRI and ethnicity for the youth in our study may be due, in part, to the strong influence of peers during adolescence (Brechwald & Prinstein, 2011), such that youth’s religious involvement may mirror that of their peers regardless of ethnic background. Thus, their experiences and use of NRI may be more similar during adolescence. More work is needed to delineate the mechanisms that undergird NRI across different ethnic subgroups of Black youth.
Study Limitations
Although our study extends what is known regarding the role of NRI for Black youth and uses the only existing national probability sample of Black youth, including CB youth, to date, we acknowledge several limitations. Given the use of cross-sectional survey data, causal inferences are limited as well, as the ability to explore the long-term impact of NRI on youth well-being. The data were also self-reported, which increases the possibility of social desirability bias. Additionally, the Caribbean youth constituted 30% of the sample, so exploring within-group differences (e.g., immigrant status, place of birth, acculturation) was not possible. Furthermore, we did not explore denominational differences; thus, we do not know the extent to which our results reflect distinctions in praxis within the Judeo-Christian tradition. Similarly, although the youth in our study predominantly identified as Christian, we do not know how these results may vary for Black youth affiliated with other faith traditions (e.g., Islam). We used a single-item measure of life satisfaction, which may not capture the full conceptualization of the construct. The measures were also administered in the same sequence as outlined in the study questionnaire; thus, there may be an issue of order effects in this study. Finally, our findings may be generalizable to youth in similar demographic groups in the United States but not to other ethnic groups of youth in the United States or beyond.
Future Research and Implications
We provide several recommendations for next steps in research as well as implications for the design and implementation of culturally sensitive individual and faith-based interventions for Black youth. Future research should explore the variance across demographic covariates, such as gender and income, given their potential influence on the relationship between NRI and youth well-being. Next, stakeholders should examine the associations between NRI and well-being across time, as much of what is currently known regarding Black adolescent NRI originates from cross-sectional designs. Longitudinal studies could document the ways in which adolescents engage with God and how their religious faith shifts as they navigate developmental milestones during the transition through and out of adolescence. Future research should also examine the role of religious diversity with regard to NRI and well-being. The majority of studies of Black American religiosity among adults and adolescents reflect experiences with Christian beliefs, traditions, and settings. However, there is a growing need to consider the experiences of Black youth from other religious traditions (i.e., Islam, African religions), those coming from interfaith households, as well as those who choose to engage in religious practices while in areligious, agnostic, or atheist households. More work should assess the role and participation of adolescents within these faith traditions, as well as which aspects of NRI are most salient for Black youth in and across these traditions.
Furthermore, research should attend to the wide range of ethnic identities in the Black diaspora. Black Americans may identify as African American, Afro-Latinx, African, or Caribbean Black, for example (Hope et al., 2020). Finally, other religiosity and spirituality variables may account for the associations between NRI and adolescent well-being. Examples worth considering include religious socialization (the ways in which individual and organizational social factors shape religious beliefs and practice; Sherkat, 2003) and religious and spiritual struggles (how individuals make sense of suffering or strain within their religiosity and spirituality; Exline & Rose, 2014). Religious socialization within immigrant faith contexts may frame religious and immigrant ethnic group membership singularly. In addition, some adolescents may experience religious and spiritual struggles (Exline & Rose, 2014) as they examine and question religious beliefs. This questioning may potentially affect the level and types of NRI with which they engage (e.g., adolescents may express anger or frustration with God and refuse to read sacred texts).
We envision a few ways in which our results may support existing initiatives and priorities of practitioners, religious institutions, and parareligious organizations that serve Black youth and their families. Consistent with faith development theory (Fowler, 1981), one inherent strength of NRI is that it provides opportunities for adolescents to personalize their faith, particularly given that their organizational religious involvement may partially reflect familial or community endorsement and pressure. NRI may encourage and challenge youth to integrate beliefs and practices into their daily decision making and cultivate intrinsic motivation to engage with their faith. Given that the current study suggests that these beliefs and practices may enhance areas of well-being, mental health practitioners could potentially integrate NRI within existing interventions with Black youth as a way to promote better well-being. Although NRI occurs outside religious settings, religious institutions working with Black youth can also empower youth’s NRI. First, many religious institutions have educational tools that they have traditionally used in youth-focused ministries and programs. However, they may consider creating additional space for youth to explore questions and concerns about NRI activities (e.g., praying and hearing from God, reading sacred texts). Furthermore, rather than solely hearing from those designated as community “leaders,” religious institutions may explore inviting speakers closer in age to adolescents to lead workshops and activities that address why NRI is important and different ways to engage. For example, youth in traditions that highly endorse prayer may be able to learn about different methods of prayer—for example, journaling, praying while walking in nature, or incorporating dance.
Another way to support Black youth NRI and psychosocial well-being is to provide mental health resources for adolescents and their families. In many Black families and communities, seeking mental health care is stigmatized, and in some religious institutions, clergy and laypeople alike may counsel individuals to rely on their faith alone to address mental health concerns. While NRI activities are undoubtedly important facets and expressions of faith, clergy and lay leaders may consider that seeking mental health care may be a form of faith in action (e.g., God as a healer via prayer vs. seeing a therapist). This perspective may be shared with congregants across formal and informal gatherings and communications. For example, religious communities often disseminate news, events, and other information during services and other gatherings, in written format through pamphlets and newsletters, or on their websites. These forms of communication and connection could also include information about faith-inclusive or faith-oriented mental health providers. Religious communities could also invite faith-oriented mental health professionals to share how they incorporate NRI into the services they provide. Furthermore, clergy and youth leaders may facilitate conversations with adolescents and their families regarding how NRI, within their particular faith tradition, may support positive psychosocial outcomes.
In sum, the study results have implications for stakeholders (e.g., psychologists, clergy) working with Black youth. Because many Black adolescents participate in religious activities with their families, it is important to create and maintain spaces that equip and empower adolescents and their families, individually and collectively, to understand the dynamic avenues and modalities through which NRI may enhance thriving. Our results offer empirical validation for targeted service delivery and program implementation to support the inclusion of Black youth’s faith within treatment plans and health promotion programs as part of a holistic approach. NRI may function promotively or protectively in the development of individual and community-based interventions that promote psychosocial well-being among Black youth.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The NSAL is supported by the National Institute of Mental Health (U01-MH57716), with supplemental support from the Office of Behavioral and Social Science Research, the National Institute on Drug Abuse at the National Institutes of Health, and the University of Michigan.