
Abstract
Undergraduates in 3 introductory psychology courses participated in teaching interventions designed to reduce mental illness stigma. Expanding on previous research, the researchers tested the effects of education, video, and contact interventions. Results of the pretest and posttest scores on a social distance measure revealed a statistically significant reduction in social distancing for the contact intervention. The researchers emphasize the use of stigma-reducing pedagogies in teaching psychopathology to undergraduates.
Past research on mental illness 1 stigma reveals that it is widespread in the United States (see Corrigan & Penn, 1999, for a review) and is one of the largest barriers to mental health treatment (U.S. Surgeon General, 1999). Other research shows that prejudice against those with mental illness may affect their ability to obtain housing and employment, which ultimately reduce resources for mental health services (Corrigan & Penn, 1999; Hinshaw & Cicchetti, 2000). Furthermore, sociological data of public perceptions of mental illness in the past 50 years show that many negative attitudes persist (Pescosolido et al., 2008).
Despite ample research on the causes and consequences of mental illness stigma, few researchers have explored classroom pedagogies to reduce it, especially in U.S. undergraduates (Chan, Mak, & Law, 2009; Chung, Chen, & Liu, 2001; Graham, 1968; Morrison, Cocozza, & Vanderwyst, 1978; Morrison & Teta, 1980). However, a recent study shows that teaching psychopathology to introductory psychology classes using a traditional approach, emphasizing symptoms and causes of disorders, had no effect at reducing mental illness stigma, but humanizing it using first-person narratives did (Mann & Himelein, 2008).
Considering that the American Psychological Association (2007) indicated several student-learning outcomes related to increasing students’ sensitivity for diverse groups (Goal 8), psychology programs ought to explore stigma-reducing pedagogies as part of their curricula. The fact that many psychology majors pursue careers in settings (e.g., education, healthcare, business) where they will work directly with diverse groups also highlights the importance of specifically addressing mental illness stigma. Moreover, many institutions require nonmajors to take introductory psychology. Therefore, not addressing mental illness stigma wastes an opportunity to educate large numbers of students who may have little exposure to this serious public health issue and who may either personally and professionally confront this issue.
In this study, we build on research showing that humanizing mental illness reduces college students’ stigmatizing attitudes (Mann & Himelein, 2008). However, instead of exposing students to first-person narratives, we specifically test education, video, and contact interventions. Although laboratory research has shown that video and contact yield similar results in reducing mental health stigma (Reinke, Corrigan, Leonhard, Lundin, & Kubiak, 2004), we aimed to test whether we could replicate this finding in a college classroom. Specifically, three groups of introductory psychology classes received an education, video, or contact intervention. We predicted that the video and contact interventions would be significantly more effective at reducing stigmatizing attitudes than education alone.
Method
Participants
A total of 69 students (41 female, 28 male) in three introductory psychology classes from a small, Catholic, liberal arts university in the northeast United States participated. Students were 19 years of age on average (SD = 2.95). The three classes were similar in terms of demographics. The majority reported freshman status (78%). Although we did not ask participants to report religious affiliation, approximately 38% of the student population is reportedly Catholic, 34% other Christian, and the remaining report a variety of religious backgrounds or no affiliation. We chose specific classes based on convenience and randomly assigned them to the interventions. Participation was completely voluntary, and we coded responses to protect anonymity. All students chose to participate. Data were discarded if a student was absent for either pretest or posttest.
Materials
Participants in all classes completed identical pretest and posttest questionnaires. The questionnaires included demographic items, two vignettes describing Bill, diagnosed with bipolar disorder, and John, diagnosed with paranoid schizophrenia, taken from Mann and Himelein (2004, 2008). After each vignette, six social distance items derived from a 19-item social distance measure developed by Chung et al. (2001) measured participants’ comfort with Bill and John in social situations such as having them as a roommate or collaborating on a project (Mann & Himelein, 2004, 2008). Scores ranged on a Likert-type scale from 1 (very uncomfortable) to 5 (very comfortable). The pretest and posttest reliability for both social distance measures was consistent with the reliability reported by Mann and Himelein (2004, 2008); Cronbach’s α = .83. Although researchers have raised questions concerning the internal validity of social distance measures (Link, Yang, Phelan, & Collins, 2004), they are common, quick to administer, and for our purposes took little time away from instruction.
All groups had identical textbooks and curricula and differed only in this method of instruction. Griggs’s (2009) textbook primarily focuses on diagnoses, symptoms, and causes of mental illness.
Procedure
Two weeks prior to introducing the psychopathology chapter, we obtained informed consent and students completed the pretest measure at the end of a class period.
For the 2-week period during which instruction covered psychopathology, all groups received similar content and instruction based on the prepackaged slides offered by the textbook publisher. Each group received 6 hr of total instruction for the chapter and 1 hr and 45 min of that time on the topic of mental illness stigma. For all groups, the intervention occurred after they had approximately 1 hr of class introducing them to the general criteria used to establish psychopathology, the background and purposes of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV; American Psychiatric Association, 1994), and the advantages and disadvantages of diagnostic labels. Instructors dedicated the last 15 min of the first class on psychopathology and the entire following class to the interventions. After the interventions, students continued to learn about symptoms and diagnosis of various disorders and types of treatments. All instructors administered a 20-item multiple-choice psychopathology chapter quiz a week after they completed instruction of the topic. Approximately 2 weeks after the psychopathology unit, all groups completed the posttest measure.
Education
The education group engaged in a 15-min, small-group activity that required them to generate cultural stereotypes and myths about individuals with mental illness. In the next class, 90 min in length, the lecture and discussion dealt with the stereotypes and misconceptions associated with mental illness. The information challenged the causes, timeline, consequences, controllability, and common representations of mental illness often viewed in the media using an evidence-based approach.
Video
The video group also engaged in a 15-min, small-group activity. However, the groups generated questions they would ask a person with a mental illness. The instructor told students to not self-censor but consider what they would be interested in knowing about the person’s experience with mental illness. Students then completed an out-of-class assignment in which they had to view three public service announcements produced by a nonprofit organization whose mission is to reduce stigma surrounding mental illness. The website (http://www.bringchange2mind.org) features firsthand accounts about mental illness. Afterward students completed a short 1- to 1.5-page reflection paper addressing the following two questions: “How can we as a society reduce the stigma associated with mental illness? Do you think the website is effective? Support your answer.” To control exposure time, instructors told the students that the total assignment should take them 1.5 hours.
Contact
The contact group engaged in the same 15-min, small-group activity as did the video group. Two days later, in the following class period (90 min), students met three members from the local community diagnosed with a mental illness (diagnoses included schizophrenia, major depression, and attention deficit-hyperactivity disorder). The members were all middle-aged men affiliated with a local mental health advocacy group. Each spent approximately 5 min (15 min total) providing background information about their lives (e.g., age of diagnosis, how they manage their illness, occupation and family information). The instructor then told students to sit with their groups from the previous class activity. The community members circulated to the groups for 15 min each so that every group had an opportunity to meet and ask questions to each member. We devised this procedure to engage the students and provide a more personal contact experience than a panel discussion.
Results
A one-way ANOVA reveals no significant difference for age, race, and gender on the pretest measure across the three groups. To test for an association, we computed correlations on participants’ pretest and posttest total social distance scores for the two vignettes. The correlations were significant, r(69) = .58, p < .01, and r(69) = .77, p < .01, respectively. Therefore, we combined the vignette scores to form a total mean social distance score (theoretical range 2 was 1–5). Table 1 shows the mean social distance scores for the groups at pretest and posttest.
Means and Standard Deviations of Social Distance Scores
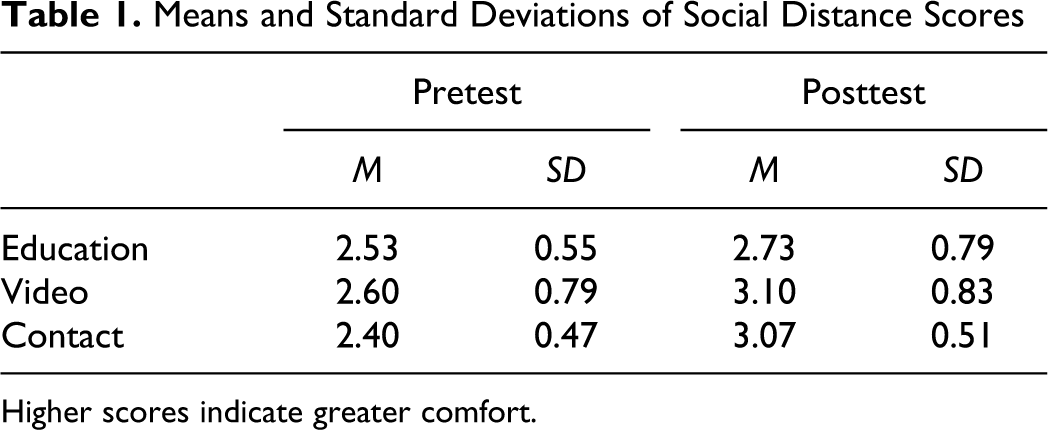
Higher scores indicate greater comfort.
An ANCOVA performed on the total mean social distance scores, with the total mean pretest social distance scores as a covariate, yielded a significant condition effect at posttest, F(2, 68) = 3.92, p = .03, partial η2 = 0.11. Follow-up Bonferroni-adjusted pairwise comparisons reveal that the contact group reported greater comfort with a person with a mental illness compared to the education group (p = .03, d = 0.50). We found no significant differences when comparing the video and education group or the contact and video group (p > .05).
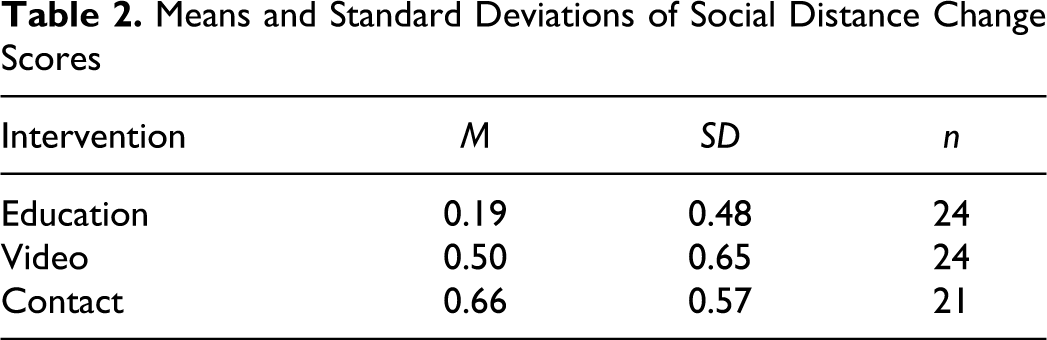
We also computed change scores by subtracting the pretest social distance scores from the posttest social distance scores. Results of a one-way ANOVA reveal a significant effect, F(2, 68) = 4.03, p = .02 (see Table 2 for mean change scores). Follow-up Bonferroni-adjusted pairwise comparisons show the contact group had a statistically significant reduction in social distance (p = .02, d = 0.78) compared with the education group. We found no significant differences when comparing the video and education group or the contact and video group (p > .05).
Means and Standard Deviations of Social Distance Change Scores
Finally, we assessed students’ knowledge of mental illness by obtaining scores on the psychopathology chapter quizzes. Analyses revealed no significant differences in performance across the three groups.
Discussion
This study compared the effectiveness of three interventions in reducing introductory psychology students’ stigmatizing attitudes of individuals with mental illness. Results partially support our hypothesis, indicating students became significantly more comfortable with individuals with mental illness after a contact intervention. Although the pattern of means shows that the video group reported greater comfort with individuals with mental illness at posttest, the amount of change is not significant.
Limitations and Future Directions
Despite showing the benefits of a contact intervention in the classroom, we address several limitations and possibilities for future research. First, the posttest social distance scores for the contact group revealed relatively more comfort, but participants were still not highly comfortable. Similar research by Chan et al. (2009), with ninth graders in Hong Kong, also found only moderate levels of comfort after a combined education-video intervention, and the effects lessened after 1 month. Moreover, Chan et al. found a 15-min video intervention to be effective only after 30 min of a demythologizing lecture, not when the lecture came afterward. In our study, the video was not effective, but perhaps pairing it with a similar demythologizing lecture would have led to greater attitude change. Another limitation that might have lessened the effectiveness of the video intervention was our inability to precisely control students’ exposure time. Time and level of engagement would have more closely matched the other groups if students watched the video during class. We recommend that instructors, especially those without the time or ability to facilitate contact, still consider video as a viable method but to include prior education before exposure. To avoid possible demand effects, future research should also consider embedding the social distance measures within other attitude measures and have others administer the surveys.
In conclusion, multiple findings suggest educating students using traditional approaches, including lecture and discussion, does little to reduce mental illness stigma. Our research provides a practical classroom intervention for reducing mental illness stigma. Similarly, other research has found that interpersonal contact with the mentally ill through undergraduate internships also reduces stigma (Kolodziej & Johnson, 1996). Our intervention was designed to increase perspective taking and provide counter-stereotypic examples of individuals with mental illness. Future theoretical research should tease apart what aspects of contact lead to attitude change and if it coincides with actual behavior change (Couture & Penn, 2003). Finally, we strongly recommend that undergraduate psychology programs currently using traditional approaches to teaching psychopathology consider contact and other evidence-based instructional methods.
Footnotes
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was partially supported by a Faculty Excellence Grant awarded by Alvernia University.