
Abstract
This study sought to understand the pervasiveness and impact of physical, psychological, and sexual violence on the social adjustment of Grade 8 and 9 school children in the state of Tripura, India. The study participants, 160 boys and 160 girls, were randomly selected from classes in eight English and Bengali medium schools in Agartala city, Tripura. Data were collected using a self-administered Semi-structured Questionnaire for Children/Students and a Social Adjustment Inventory which were custom-made for the study based on measures in the extant research adapted for the Indian context. Findings revealed that students experienced physical (21.9%), psychological (20.9%), and sexual (18.1%) violence at home, and 29.7% of the children had witnessed family violence. Boys were more often victims of physical and psychological violence while girls were more often victims of sexual violence. The social adjustment scores of school children who experienced violence, regardless of the nature of the violence, was significantly lower when compared with scores of those who had not experienced violence (p < 0.001). Social adjustment was poorer for girls than boys (p < 0.001). The study speaks in favour of early detection and intervention for all child maltreatment subtypes and for children exposed to interparental violence, and highlights the crucial role of schools and school psychology in addressing the problem.
Keywords
Physical, psychological, and sexual violence against children are worldwide problems generating serious short- and long-term effects on children’s health, development, and learning, and severe consequences for the well-being of families, communities, and nations (Pinheiro, 2006; World Health Organisation [WHO], 2002). The extent of violence against children is difficult to measure because much occurs in the privacy of family homes and is never reported or investigated (UNICEF, 2009). Compounding this difficulty is the fact that in some nations data collection mechanisms do not exist (Pinheiro, 2006; UNICEF, 2009). At its worst, violence against children can result in child mortality. For example a decade ago, WHO (2002) estimated that annually worldwide 57,000 child deaths of children under 15 years of age were attributable to homicide at the hands of their parents. UNICEF (2003) estimates that in high-income countries, between 0.1 and 2.4 child deaths per 100,000 children are attributable specifically to child maltreatment and rates are estimated to be two to three times higher in low- and middle-income countries. Data from 37 low-income countries collected as part of the UNICEF (2009) Multiple Indicator Cluster Surveys which assist countries to monitor their progress towards the Millennium Development Goals (UNICEF, 2005), revealed that approximately 86% of children aged 2- to 14-years-old experienced both physical punishment and psychological aggression in the month preceding data collection. A global meta-analytic review of population-based studies of childhood sexual abuse has estimated cumulative prevalence rates for sexual abuse prior to age 18 as 18.0% for girls and 7.6% for boys (Stoltenborgh, Ijzendoorn, Euser, & Bakermans-Kranenburg, 2011).
A recent discussion article on child protection and child welfare in the Asia-Pacific region (Pouwels, Swales, Mccoy, & Peddle, 2010) summarized primary studies reporting the pervasiveness of physical, psychological, and sexual violence in the preceding 12 months for children in China (10%, 13%, and 2% respectively), Malaysia (19.0%, 20.4%, and 22.2% respectively), and Vietnam (47.5%, 39.5%, and 19.7% respectively). A study of childhood maltreatment in seven low- and middle-income countries (Dunne et al., 2009) revealed rates of physical, psychological, and sexual violence ever experienced during childhood for children in India were 33.1%, 46.8%, and 20.2% respectively. The results of these studies suggest that children in different countries experience different types of victimization at different rates. Even within countries there may be regional differences. These data are an important source of information for policy makers, children’s rights advocates, and professionals who work with children, including school psychologists. Differential patterns evident in the data highlight the considerable heterogeneity of risk and protective factors for children in different contexts. Hence, rates of physical, psychological, and sexual victimization must be considered in relation to multiple factors in the complex social ecology of children’s lives (Cicchetti & Lynch, 1993; Theron & Donald, 2012; Toland & Carrigan, 2011).
The purpose of this article is to draw attention to the impact of physical, psychological, and sexual violence on the social adjustment of school children in India: It is an effort to address the paucity of literature and research on child victimization in Indian societies (Deb, 2006). Indeed, very little empirical research has been conducted with adolescents in low and middle income countries on the association between children’s adjustment and physical, psychological, and sexual violence. This is important for school psychologists, internationally, who have the potential to play an important role in the detection of child physical, psychological, and sexual victimization, the provision of interventions to assist students to address the consequences of maltreatment, and to advocate for and with their counterparts in school systems and professional associations for better service-provision worldwide (Cook, Jimerson, & Begeny, 2010; Jimerson, Stewart, Skokut, Caredenas, & Malone, 2009). School psychologists, therefore, must be alert to the prevalence of different types of victimization within their school communities as child protection and preventive work are fundamental areas of work for all school psychologists (Woods, Bond, Tyldesley, Farrell, & Humphrey, 2011). Furthermore, with increasing globalization, school psychologists find themselves working interculturally, with a diverse array of students from different backgrounds requiring their focus on social adjustment and inclusion.
In this study we use the term social adjustment to mean children’s struggle to get along or survive in their social and physical environment (Lazarus, 1976). It is a functional term encapsulating both a state of being and signifying a process of change in response to circumstances (Miller, Yahne, & Rhodes, 1990). Research suggests that the consequences of violence against children depend on factors including the type of maltreatment, its severity and frequency, the age of the child, the child’s gender, and the presence or absence of risk and protective factors which increase or decrease child and family resilience (Macdonald, 2001; Peirson, Laurindeau, & Chamberland, 2001).
In the ensuing sections we also define and operationalize each of the violence subtypes as they are used in this study. This is important because, as Segal (1992) and others have pointed out (see Chen & Astor, 2009, and Rees & Seaton, 2011 in this journal, for example), most empirical knowledge about violence against children has been generated in the West and it is crucial that researchers assess this phenomenon within the constructs of their own socio-cultural contexts.
Physical violence and adjustment problems
Physical violence towards children is defined by the WHO (2002) as acts of commission by a caregiver that cause actual physical harm or have the potential for harm. The harm may or may not have been intended. Such acts can arise from the use of excessive discipline or corporal punishment. In this study, it specifically includes pushing, grabbing, kicking, hitting, choking, locking, burning, and punishing the child in painful ways. A large population-based self-report study of parents conducted in Chile, Egypt, India, and the Philippines, also known as the WorldSAFE study, revealed that mothers in India reported the highest rates of severe physical punishment including hitting children with objects (36%), kicking (10%), and choking (2%) at least once in the six months preceding data collection (Sadowski, Hunter, Bangdiwala, & Munoz, 2004).
The consequences of physical abuse and its relationship to adjustment have been documented in a number of studies. These studies have shown that physically abused school-aged children show greater overall adjustment difficulties, poorer social competence, lower cognitive capacity, and poorer overall school performance than their nonabused counterparts (see for example Kolko, 2002; Macdonald, 2001). For example, physically abused children may show aggressive and violent behaviours towards their peers (Beeghly & Cicchetti, 1994; Chen & Astor, 2009), have fewer positive interactions, and become disruptive and antisocial (Howes & Eldredge, 1985). They are over-represented in delinquent populations (Scudder, Blount, Heide, & Silverman, 1993) and juvenile offenders (Steele, 1976). Physically abused children are 2.5 times more likely to have repeated a year of school (Kurtz, Gaudin, Howing, & Wodarski, 1993). They complete fewer total years of school than other school students (Perez & Widom, 1994). Those in foster care are disproportionally represented in special education classes, grade retentions, and disciplinary actions resulting in suspensions and exclusions (Scherr, 2007). Research has also documented a concerning range of subsequent mental health conditions in adolescence and adulthood. For example, Silverman, Reinherz, and Giaconia’s (1996) longitudinal study found physically abused individuals experienced significantly more instances of depression, post-traumatic stress disorder, and anti-social behavior. Associations have also been found between a history of physical abuse and later health risk behaviours including heavy drinking, drug and inhalant use and abuse, smoking, HIV-risk behaviours, and use of dangerous weapons (Bensley, Van Eenwyk, & Simmons, 2000; Hussey, Chang, & Kotch, 2006; Malete, 2007). Retrospective studies of adults have shown that males are more likely than females to have experienced physical abuse as a child. Although negative consequences are evident for both genders, physical abuse seems more detrimental for girls (Thompson, Kingree, & Desai, 2004; Widom & White, 1997).
Psychological violence and adjustment problems
Psychological or emotional violence towards children is defined as non-physical forms of hostile treatment that have a detrimental effect on the child’s health and development (Gilbert et al., 2009; Pinheiro, 2006; WHO, 2002). In this study it includes verbally harassing, disparaging, criticizing, threatening, and ridiculing. These acts are intentional and convey to a child that he/she is worthless (Gilbert et al., 2009). Psychological violence may be the most prevalent form of child maltreatment, but it is also the most hidden, under-reported, and least studied of all the maltreatment subtypes (Barnett, Miller-Perrin, & Perrin, 2005). In a recent study of street children in Jaipur, India, Mathur, Rathore, and Mathur (2009) found high levels of what they defined as verbal and psychological abuse with boys being abused more than girls, and children who reported higher levels of psychological abuse also experiencing other forms of maltreatment.
Psychological or emotional abuse impacts children’s functioning in several ways. For example, research has shown that emotional abuse in early childhood increases the risk of aggression and social withdrawal in middle childhood and poor socioemotional competence in early adolescence (Shaffer, Yates, & Egeland, 2009). Clinical and research findings have revealed that psychologically or emotionally abused school-aged children can present with behaviours such as anger, noncompliance, high levels of negativity, poor impulse control, and lower social competence, as well as academic underachievement (see for example Erickson, Egeland, & Pianta, 1989; Yates, 2007). In particular, paternal psychological abuse has been associated with anxiety, depression, interpersonal sensitivity, and dissociation (Briere & Runtz, 1988). In retrospective research, psychological or emotional abuse has been associated with increased levels of psychopathology into adulthood including anxiety, depression, lowered self-esteem (Mullen, Martin, Anderson, Romans, & Herbison, 1996; Ney, Fung, & Wickett, 1994), interpersonal relationship problems (Berzenski & Yates, 2010), borderline personality traits (Allen, 2008), and eating disorders (Hund & Espelage, 2006; Mazzeo & Espelage, 2002). A history of psychological or emotional abuse has also been associated with an increased likelihood of dropping out of college (Duncan, 2000). Further, psychological or emotional abuse is thought to amplify the effects of other co-occurring maltreatment subtypes (Briere & Runtz, 1990).
Sexual violence and adjustment problems
Sexual violence towards children is defined as a crime involving a child in sexual activity with an adult or older person (generally five or more years older). It may involve contact or noncontact sexual acts. Contact acts include unwanted touching, masturbation, oral-genital contact, digital penetration, and vaginal and anal rape. Noncontact acts include voyeurism, exposure, making sexual comments, and showing children pornography (Gilbert et al., 2009; Putnam, 2003; WHO, 2002). In this study, sexual violence specifically includes touching of private body parts, fondling, penetration, and rape. In a recent study of high school students in Goa, India, Patel and Andrew (2001) found that one-third of the children surveyed had experienced some form of sexual abuse, and these individuals had significantly poorer academic performance, poorer mental and physical health, greater substance abuse, poorer parental relationships and higher rates of consensual sexual behaviours than their non-abused counterparts. Further, in a study conducted in Kolkata, India, Deb and Mukherjee (2009) found that 69.2% of sexually abused girls suffered from moderate or severe depression compared with 27.5% of non-sexually abused girls. The study also found that 20.8% and 60.1% of sexually abused girls had poor levels of social and emotional adjustment respectively, compared with 4.17% and 32.5% of non-sexually abused girls.
Child sexual abuse is the most researched of all the maltreatment subtypes. In addition to the physical consequences such as sexually transmitted infections, bedwetting, and soiling (Kendall-Tackett, Williams, & Finkelhor, 1993), children who have been sexually abused report higher rates of emotional and behavioural problems than their non-abused peers. In particular they may display inappropriate sexual behaviour (see for example Berliner & Elliot, 2002; Herrera & Carey, 1993; Putnam, 2003). In middle childhood, sexually abused children have problems with social withdrawal, isolation and dissociation (see for example, Macdonald, 2001). Sexually abused adolescents are at greater risk for deliberate self harm and attempted suicide (Kendall-Tackett et al., 1993). In the long-term, there are consequences for adult adjustment including risky sexual behaviours and sexual revictimization (Andrews, Corry, Slade, Issakids, & Swanston, 2004; Polusny & Follette, 1995; Van Roode, Dickson, Herbison, & Paul, 2009), and substance abuse (Kendall-Tackett, 2002). Research has identified debilitating mental health sequelae including higher risk for major depression (Briere & Runtz, 1993), suicidal behaviours, anxiety and phobias, post-traumatic stress disorder, dissociation, and problematic cognitions (see for example Berliner & Elliot, 2002). Studies have also uncovered association with health problems in adults including cardiac disease (Goodwin & Stein, 2004).
Multiple violence types
School-aged children can be exposed to more than one type of maltreatment occasionally or on a continuous basis (Finkelhor, Ormrod, & Turner, 2007). This has been termed multi-type maltreatment (Higgins & McCabe, 2001). Studies have disclosed that witnessing interparental violence and child maltreatment co-occur in the same families (Appel & Holden, 1998; Casanueva, Martin, & Runyan, 2009; Edleson, 1999). For example, Straus and Smith (1990) reported that child maltreatment is 18 times more likely to occur in homes where interparental violence exists. It is clearly established that experiencing dual violence not only has an immediate negative effect on children, but also a long-term detrimental impact on adult adjustment (Feerick & Haugaard, 1999; Grych, Jouriles, Swank, McDonald, & Norwood, 2000; O’Keefe, 1996; Shen, 2009a, 2009b). A study of married men conducted in the northern Indian state of Uttar Pradesh in the 1990s found high levels of domestic violence in the range of 18% to 45% across the different regions studied. Such violence included men shouting and yelling, slapping, pushing, punching, and kicking their wives. Only 1% to 2% of wives had sought medical treatment for their injuries (Martin, Tsui, Maitra, & Marinshaw, 1999).
There remains a paucity of empirical data on the pervasiveness and associated features of specific forms of violence against children in particular parts of India. The present study attempts to address this knowledge gap. The study is modest in that it attempts to determine the association between social adjustment and the experience of physical, psychological, and sexual violence. This is an essential precursor to more complex studies which may be able to isolate and consider multiple variables simultaneously. The following two hypotheses have been formulated for testing: (1) social adjustment of children who experienced physical, psychological, or sexual violence will differ significantly from social adjustment of children who did not experience physical, psychological, or sexual violence; (2) Social adjustment of boys and girls who experienced physical, psychological, and sexual violence will differ significantly.
Method
Site
The study was conducted in eight secondary schools in Agartala, Tripura, India. The state of Tripura is located in the far North-Eastern part of India to the west of Bangladesh. It is the third smallest state comprising approximately 3 million people, most identifying as Hindu. The literacy rate in Tripura (73.6%) is slightly higher than that for India overall (63.0%). Rates are higher for males (81.0%) than for females (64.9%) and higher in urban (89.2%) than rural areas (69.7%) (Census Commissioner, 2001). Workforce participation rates are 51% for males and 21% for females, and average monthly incomes in Tripura (Rs 1,600) (Government of Tripura, 2007) are below the Indian average (Rs 3,000) (Expressindia, 2009). In schools, the medium of instruction is predominantly Bengali or English and, to a lesser extent, Kokborok and the Tripuri tribal languages. Schools in Tripura are administered by the state government or private agencies including religious and philanthropic organizations. Approximately one-fifth (21.4%) of children drop out of school before completing the primary stage of education (which is up to Class 5 of elementary school). In Tripura, the middle stage of education (i.e. middle school) spans Classes 6 to 8, and the secondary stage (i.e. high school) caters for children in Classes 9 and 10. There has been substantial improvement in school attendance rates in Tripura between 1991 and 2001. The proportion of children aged 6- to 14-years-old not attending school has been reduced by half in the past decade from 43.4% in 1991 to 23.0% in 2001 (Government of Tripura, 2007).
Sample
Children (n = 320) aged 14- to 19-years-old were randomly selected from eight English and Bengali medium schools in the city of Agartala, Tripura. An equal number of boys (n = 160) and girls (n = 160) from Class VIII and Class IX participated in the study.
Instruments
Two self-report study tools were custom-made for the study: A Semi-structured Questionnaire for Children/Students (Deb & Modak, 2007) and a Social Adjustment Inventory (Deb & Mukherjee, 2009). These were developed from reviews of the extant literature and from adaptation of existing measures. The first tool, the Semi-structured Questionnaire for Children/Students (Deb & Modak, 2007) is similar to what has since become known as the ISPCAN Child Abuse Screening Tool Children’s Version (ICAST-C) (Zolotor et al., 2009) to which the first author of this article was a contributor in the development and testing phases. The ICAST-C has been field tested in five middle and low income countries finding moderate to high internal consistency for item sub-scales and low rates of missing data (Zolotor et al., 2009). This screening tool is, in turn, based on elements of the Parent-Child Conflict Tactics Scale (Straus, Hanby, Finkelhor, Moore, & Runyan, 1998) and the Juvenile Victimisation Questionnaire (Finkelhor, Hamby, Ormrod, & Turner, 2005) both of which have been widely used in research worldwide. The Semi-structured Questionnaire has three sections. Section 1 covers background information about the respondent’s family and current circumstances including age, number of siblings, family type, academic performance, parents’ education and occupation, monthly family income, living environment, perceptions about the family environment, parenting style/approach, and parents’ drug and alcohol use. Section 2 consists of 15 items asking for information about the nature of violence experienced by the child (physical, psychological, and sexual), the frequency of violence, and the profile of the perpetrators of that violence. Section 3 comprised five items collecting data about reporting of violence to authorities such as law enforcement officials or local non-government organizations (NGOs) and the reasons for reporting or not reporting the incident to them.
The second study tool was the Social Adjustment Inventory. This instrument was originally based upon the Bell’s Adjustment Inventory (Bell, 1939, 1962) which has a long tradition of adaptation in psychological research in India. Bell’s original Adjustment Inventory measured a person’s degree of adjustment in four realms of life: health, social, emotional, and occupational. It has been widely used in therapeutic practice as it assists clinicians to identify relevant areas of adjustment and maladjustment. Several adaptations of this inventory can be found in the Indian literature (see for example Hussain, 1970; Jain, 1972; Mohan & Hussain, 1987; Pal, 1995; Singh, 1974. In this study, the Pal (1995) version of the Social Adjustment Inventory (1995) was used after local adaptation to the Bengali language (Deb & Mukherjee, 2009). It was employed as a means of determining the degree of social adjustment held by each child. The advantage of using this instrument lies in its wide use as it provides profiles of social adjustment in children with a range of comparative childhood issues, for example, chronic illness or disability. In this version, there were 60 items each with response categories of ‘yes’ or ‘no’. Example items included: ‘I don’t have any problem in mixing with people’; ‘It has become my habit to take an active part in social functions’; and ‘In my view, it is better to work in a group rather than individually’. Scoring was straightforward as recommended by Bell with ‘yes’ responses allocated a score of 2 and ‘no’ responses allocated a score of 1; generating a maximum score of 120 and a minimum score of 60. Low scores indicated poorer social adjustment while higher scores indicated better social adjustment. The socio-cultural admissibility of the test was ascertained by translating the items from English into the local Bengali language. This was undertaken independently by three experienced researchers. The Bengali version of the test was then back-translated into English to ensure stability of the test items (Mukherjee, 2006).
Procedure
To collect data in schools, permission was sought and obtained from the school authorities and then a tentative time schedule was developed for data collection. Data were collected from the children during school time. They gave informed, voluntary consent and all information provided by them was collected anonymously. The ethical issues which were of particular concern in this study included the need to ensure participants were fully informed about the nature of the study and measures taken to preserve their privacy, the voluntary nature of participation, and the importance of their consent for the data collection process. Additionally, in research with potential to cause distress, it was important to implement subtle actions for monitoring participant distress during the research process and for ensuring ongoing support for children who may need it (Cashmore, 2006; Simmel, Flanzer, & Webb, 2006).
Data analysis
The data collected from the school children were subjected to a thorough in-house review, before data were entered for analysis. Apart from descriptive statistics such as measures of central tendency and dispersions, t-tests were used for verification of hypotheses. Confidence Intervals for group comparisons were calculated at 95% and significance levels were set at 0.01 and 0.001. Calculations were performed using SPSS for Windows 17.0 (SPSS Inc., 2008).
Results
The sample comprised 320 children: 50% boys and 50% girls with 50% each from Classes 8 and Class 9. Their ages fell into three groupings: 14- to 15-years-old (92.5%), 16- to 17-years-old (5.9%) and 18-years-old and older (1.6%). Approximately 27.8% of respondents were the only child of their parents, 53.8% had one sibling, 12.8% had two siblings, and 5.6% had larger families with three or more siblings. Regarding the family type, slightly more children were growing up in single/nuclear families (53.8%) than joint/extended families (46.2%).
Participants’ background information (n = 320)
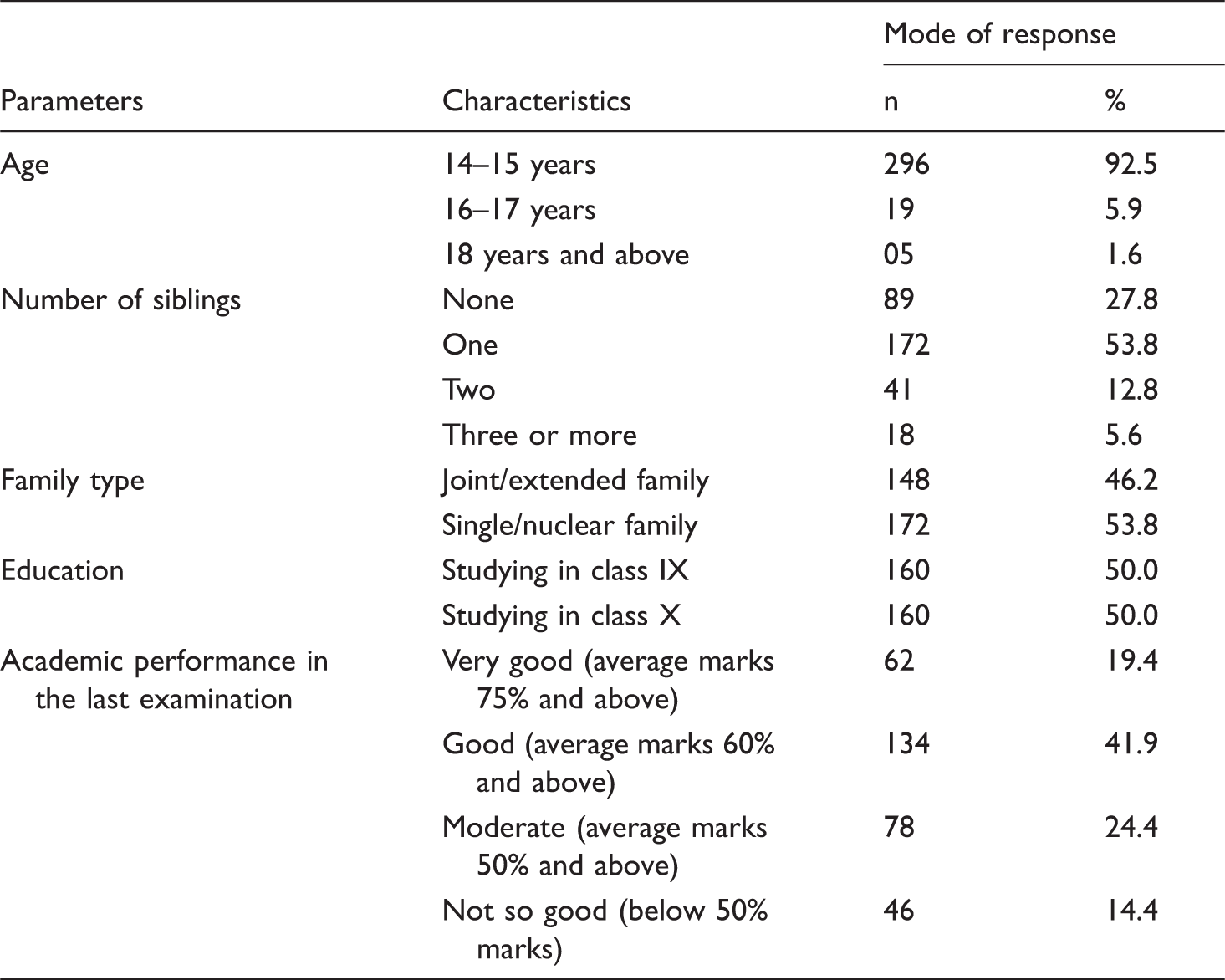
The majority of the families lived in urban (51.1%) and semi-urban areas (21.1%). With regards to parents’ education, 50.0% of the fathers and 35.3% of the mothers were university graduates and 37.5% of the fathers and 27.9% of the mothers had post-graduate qualifications. Data indicate that 70.0% of the children’s fathers and 40.6% of the mothers were in the paid workforce. Of these parents, the most common type of occupation was in business with 25.3% of fathers and 10.3% of mothers engaged in business-related work. The remainder of parents were engaged in casual work and more than one-quarter of the mothers (28.8%) were stay-at-home mothers described as housewives in this study. The total monthly family income was spread with a small proportion of children (5.0%) reporting their parents’ incomes as more than Rs 20,001/per month. The majority of the families (69.0%) had incomes in the range Rs 10,000/to 20,000/per month and a smaller proportion (26.0%) reporting incomes of below Rs 10,000/per month.
Since family violence has a direct or indirect relationship with child abuse and neglect, the present study probed the issue with the children to understand the pervasiveness of the situation in Agartala, Tripura. About 29.7% of the children reported that they witnessed violence in the family mostly between their parents. In this regard, boys witnessed more violence (35.0%) as compared to girls (24.4%). About 8.4% of the children, irrespective of gender, witnessed violence regularly, defined as once or twice per week, while 34.7% witnessed the same occasionally, that is, once per month or once every six months. So far as manifestation of the violence is concerned, children mostly reported parents shouting or yelling at each other, followed by beating, kicking, or other forms of physical assault.
Nature of violence experienced by children
Nature of violence experienced by children
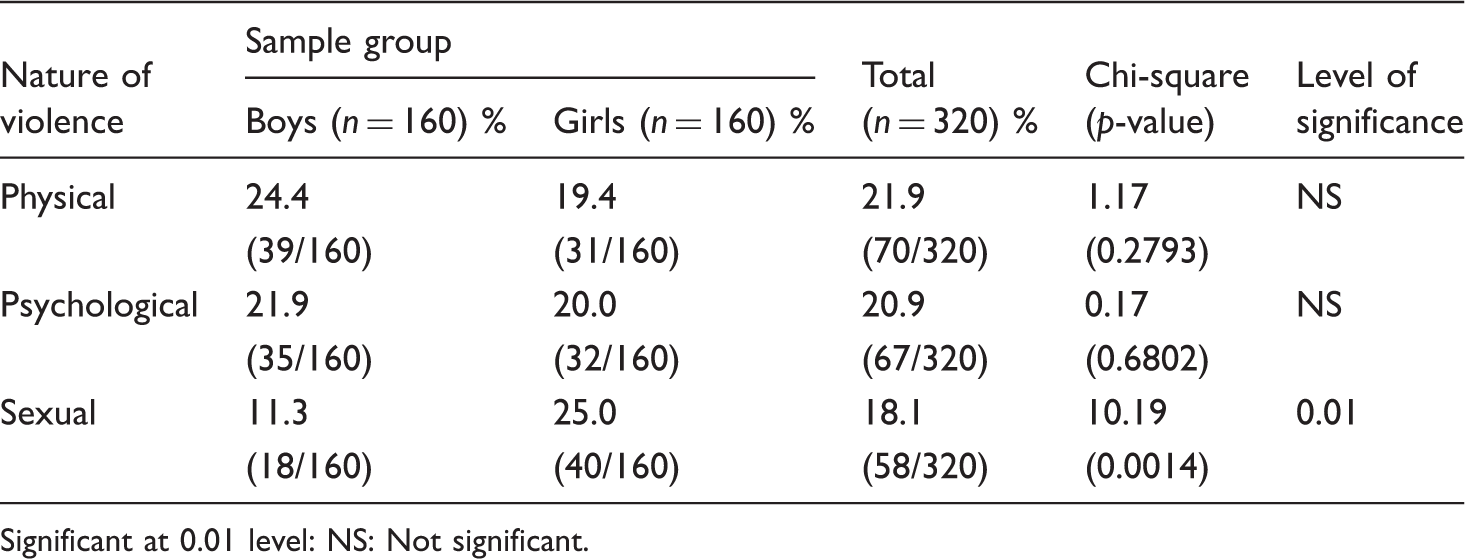
Significant at 0.01 level: NS: Not significant.
Social adjustment
Comparison of the social adjustment scores of physically, psychologically, and sexually abused, and non-abused children

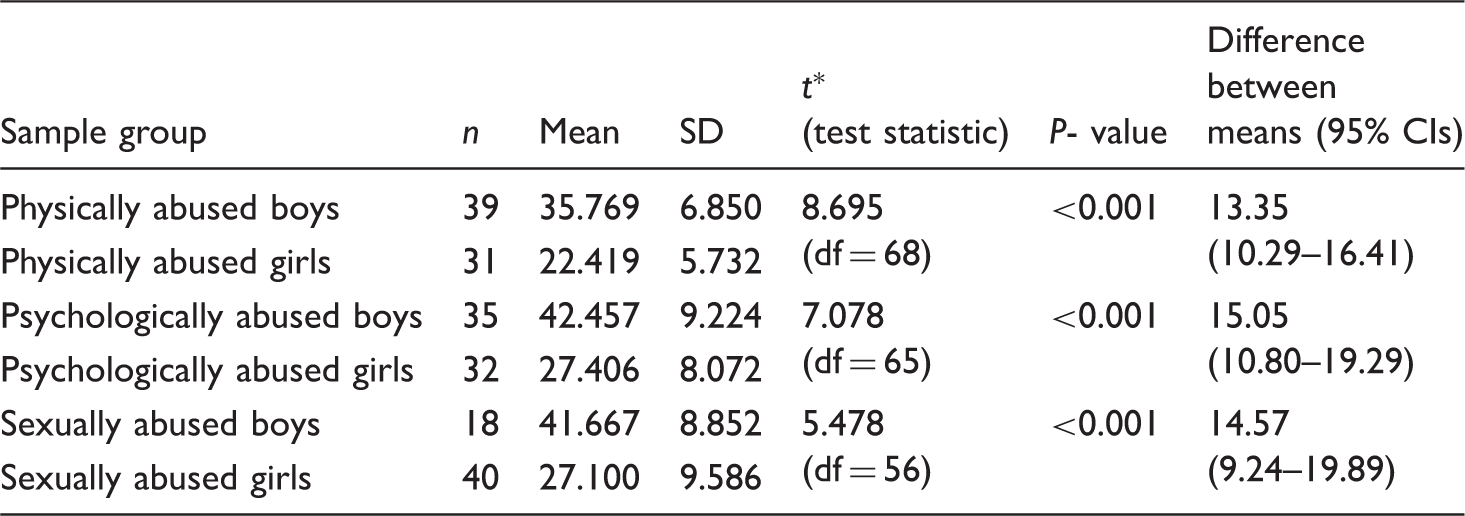
Comparison of the social adjustment scores of physically, psychologically, and sexually abused boys and girls
Discussion
Before discussing the specific findings regarding physical, psychological, and sexual violence against children, it is important to be mindful of the social and cultural context within which it occurs. Tripura is a state with a diverse population attributable to the historical difficulties it has faced with successive waves of immigration and influxes of refugees, mainly from Bangladesh, at the time of partition (1947), during the Bangladesh war of independence (1971), and more recently because of the economic situation in that country. Tripura is not a particularly urbanized state with a lower proportion (17%) of the population living in urban centres compared with India’s national average (28%) (Government of Tripura, 2007). Many of the rural inhabitants are tribal people with ancestry in countries such as Tibet, Myanmar and Mongolia. Hence, in some ways, this state faces unique challenges.
This sample of children from schools, however, was from an urban area. Children were attending school beyond the elementary stage. They had parents who were more highly educated than the general population in India and had higher proportions of parents in the paid workforce with higher than average household incomes. Even so, a substantial proportion (29.7%) of the children in this study reported witnessing interparental violence involving their parents shouting, yelling, beating and kicking each other. Boys witnessed more violence (35.0%) than girls (24.4%). Available research confirms that this problem is not confined to India alone. For example, in a multi-country study conducted by Zolotor et al. (2009) found rates of exposure to violence at home in the past 12 months, reported by children (operationalized as adults shouting, hitting, kicking, slapping, or using weapons against each other) was 67% in Russia, 57% in Columbia, 49% in India, and 30% in Iceland. These comparisons are significant because the methodologies used to measure violence exposure in previous studies, and the present study, are similar. The findings support emerging theories suggesting that interparental violence is more likely in impoverished households and poorer countries, and where adults have little or no formal education (UNICEF, 2009).
The findings of the present study are congruent with the findings of Martin et al. (1999) who studied domestic violence in Northern India. Their study found that 30% of the men in their 6,000-strong sample had witnessed family violence as children. Moreover, men who had experienced family violence were more likely as adults to perpetrate physical and sexual assaults against their wives and to believe it was their right to do so. Furthermore, 54% of Indian women aged 15- to 49-years-old considered a husband to be justified in hitting or beating his wife in certain circumstances (UNICEF, 2011). This is cause for concern for the future families of children in our sample as it appears that that family violence levels have remained fairly stable over two generations.
For the children who have experienced family violence, research indicates that they will be at risk for a wide range of both internalizing and externalizing behaviour problems which may vary by developmental stage (Hughes, 1988; Moore & Pepler, 2006). Research also indicates that there is a risk of a wide range of adjustment problems for children exposed to family violence. However, the research is not unequivocal: some children exposed to family violence show extreme adjustment difficulties, while others score well within the normal range (Hughes & Luke, 1998). Much depends on the constellation of risk and protective factors surrounding the child, their family, and community. Protective factors would include sensitive and authoritative parenting, decent educational opportunities, good physical health, and psychological autonomy (Patel, Flisher, Nikapota, & Malhotra, 2008).
The pervasiveness of physical (21.9%), psychological (20.9%), and sexual violence (18.1%) experienced by the children, both reflect and contradict previous research. Almost one-fifth of the sample reported physical violence which seems comparable, or even lower, than findings from similar studies conducted in other countries. For example, in the United Kingdom, May-Chahal and Cawson (2005) studied over 2,800 young adults with 16% reporting some type of childhood violence and 7% reporting severe physical abuse at the hands of their parents. In the USA, Hussey, Chang, and Kotch (2006) found 28.4% of their 10,828 respondents had been slapped, hit or kicked by a parent or adult caregiver. Gilbert and colleagues’ (2009) review of the burden and consequences of violence against children in high-income countries reported on studies conducted in European countries which found rates of physical abuse of 12% in Macedonia and 29% in Moldava, and higher rates in rural than urban areas. In Segal’s (1995) study of discipline practices of professional middle class Indian parents, 42% of parents used harsh discipline including kicking, biting, punching, striking with an implement, or beating. Sadowski, Hunter, Bangdiwala, and Munoz (2004) found 36% of Indian mothers used the same. The data in the current study tend to show a decline from these figures and a slightly lower preponderance of physical abuse than that previously reported. Findings from the current study, however, indicating that boys experienced more physical violence than girls (24.4% versus 19.4%) were not supported by data from the WorldSAFE study of child discipline practices in India which found boys and girls were harshly disciplined rather equally (Hunter, Jain, Sadowski, & Sanhueza, 2000).
With respect to psychological violence, one-fifth (20.9%) of the sample reported exposure to psychological violence at home. This seems higher than some studies conducted in other countries. For example, May-Chahal and Cawson (2005) reported that 6% of young adults in the UK reported severe psychological abuse. In contrast, however, 22% of 14- to 17-year-olds in the USA reported recollections of emotional abuse during childhood (Finkelhor, Turner, Ormrod, & Hamby, 2009), a figure comparable to that found in the current study. Psychological or emotional abuse is the most common and intense form of violence reported by Indian street children (Mathur, Rathore, & Mathur, 2009). Regarding the impact of psychological violence against children, Shaffer et al. (2009) observed that both emotional neglect and emotional abuse were associated with increased aggression and social withdrawal in middle childhood, and lower ratings of socioemotional competence in early adolescence. Other studies have shown that children’s exposure to verbal aggression was the strongest predictor of adjustment difficulties (Moore & Pepler, 2006).
Findings that one-quarter of the girls experienced sexual abuse (25.0%) and that girls also experienced more sexual violence than boys (25.0% versus 11.3%) were not unexpected: These findings are comparable with studies throughout the world. For example, in a meta-analysis of 39 child sexual abuse prevalence studies in 21 countries, Pereda, Guilera, Forns, and Gomez-Benito (2009) reported rates of 10% to 20% for girls and approximately 10% for boys. However, the highest prevalence rates were found in South Africa with over 50% for both girls and boys. In an Indian sample of runaway, boys at an observation home in Delhi 38.1% reported exposure to sexual abuse (Pagare, Meena, Jiloha, & Singh, 2005). Importantly, Varia, Abidin, and Dass (1996) revealed that sexually abused children consistently had more psychological and social adjustment problems than their non-abused counterparts. Roberts, O’Connor, Dunn, Golding, and The ALSPAC Study Team (2004) investigated the links between child sexual abuse occurring before 13 years of age, and later mental health, family organization, parenting behaviors, and adjustment in offspring. The findings indicated that child sexual abuse had long-term repercussions for adult mental health, parenting relationships and child adjustment in the succeeding generation.
Social adjustment is an important functional dimension of human life that is indicative of mental health. It is essential to well-being and to an individual’s ability to ‘perceive, comprehend and interpret our surroundings, to adapt to them or change them if necessary, and to communicate with each other and have successful social interactions’ (Lehtinen, Ozamiz, Underwood, & Weiss, 2005, p. 46). In this study, children who experienced physical, psychological, or sexual violence were found to have significantly poorer social adjustment when compared with non-abused children. These results are not surprising and are corroborated by numerous existing studies indicating negative outcomes for children experiencing maltreatment (for succinct reviews of this research see Asnes & Leventhal, 2009; Gilbert et al, 2009). The present study found that female children faced more social adjustment challenges than male children. This can be understood in terms of the structural inequalities in Indian society including gender inequality (Deb, 2006). Girls have less access to supports which are known to moderate the effects of family violence such as self determination, freedom of movement, and help seeking (Margolin & Gordis, 2000; Patel et al., 2008). As Kliewer, Lepore, Oskin, and Johnson (1998) note, opportunities to talk about violence exposure to supportive others is associated with less intrusive thinking and fewer internalizing symptoms. Despite the scope of domestic change brought about by globalization, underlying patriarchal structures persist in Indian societies (Da Costa, 2008; Kingdon, 2007). Culture may still determine the norms, values and beliefs surrounding the use of violence, and the way children understand and label their own experiences (Margolin & Gordis, 2000). More work is needed in this area to fully comprehend the ways in which culture affects violence towards children. Although we are cognizant of new perspectives urging for a paradigm shift in understanding child well-being with a focus on positive rather than negative indicators for children, activity rather than passivity, and survival rather than victimization (see for example Saith & Wazir, 2010; Theron & Donald, 2012), we also argue that illuminating the scope of the problem in previously unstudied areas is an important first step towards addressing the issue.
Limitations
This study has some limitations which must be considered. First, the sample comprised school children only from urban areas, limiting the diversity of the sample by ethnic background, socioeconomic and educational status. Thus, the findings may not be generalized to broader community samples. Second, the prevalence of physical, psychological and sexual violence, and rates of exposure to family violence were based on children’s self-reports. Although privacy, confidentiality, and anonymity was assured, it may be that some children did not reveal the true extent of the violence they experienced because of feelings of embarrassment, shame or guilt or, moreover, because of their emotional attachment to their parents and their desires for loyalty (Deb, 2006). In an article from a landmark longitudinal study, Fergusson and colleagues (2000) note substantial unreliability in the reporting of child maltreatment owing to individuals’ forgetting or blocking out memories of traumatic events, avoidance of recalling or describing their abusive experiences, and the influence of an individual’s level of adjustment at the time of completing a survey. These authors conclude that the main shortcoming of self-reports is the propensity to result in false negative reports (i.e. people who have experienced victimization reporting that they had not). Future studies may consider corroborating student self-report measures of adjustment with teacher reports. Teacher reports may be extended to also identify the specific educational effects of exposure to different types of violence. This information may assist schools to better address victimized students’ specific psychological needs.
Conclusion and implications
Overall, about one-fifth of the children experienced psychological, physical, and sexual violence in this sample of school children from Tripura, India. This is the first study to document pervasiveness of different violence subtypes against children in this small north-eastern Indian state. The study found that boys were more often victims of physical and psychological violence while girls were more often victims of sexual violence. The social adjustment scores of school children who experienced violence, regardless of the nature of the violence, was significantly lower when compared with scores of those who had not experienced violence. Social adjustment was poorer for girls than boys.
For school psychology worldwide, the findings of this study recapitulate the need for early detection and intervention for all maltreatment subtypes and for children exposed to interparental violence. However, for awareness about the prevalence of adolescents’ physical, psychological, and sexual violence to be useful to schools, it must be embedded in broader understandings about the key features of the complex and dynamic social ecologies in which children live (Cicchetti & Lynch, 1993; Toland & Carrigan, 2011). Victimization does not occur in a social and/or political vacuum. Demonstrating links between the presence of victimization and children’s social adjustment problems is the first step in articulating the problem. Future research, however, must undertake more complex analyses to understand the process by which adjustment problems arise in some children and not others living in similar contexts and, moreover, to identify culturally-meaningful resiliency-enhancement strategies (Theron & Donald, 2012). This takes on particular salience in developing countries where children’s vulnerability is compounded by influences in the wider macro-system such as community poverty, poor literacy, unemployment, and deeply-rooted cultural beliefs and practices (Deb, 2006).
The study’s findings have implications for schools generally. Within schools, teachers can be guided to take their role as ‘sentinels’ for children very seriously (Sedlak, 1993). Teachers, as well as school psychologists, have the potential to play a key role in identifying children who have experienced victimization, providing support in the classroom on a day-to-day basis, modelling and building trusting relationships, ensuring children’s safety and security at school, and referring them to appropriate treatment programs where necessary (Phasha, 2008; Watts, 1997). To champion this role, teachers will do better with the support of school psychologists; their involvement is crucial to creating deeper understandings about physical, psychological, and sexual violence and its consequences for children’s adjustment. Within an eco-systemic view there is hope: A sense that children’s school experiences and relationships have the potential to generate protective effects enabling vulnerable children to thrive in the face of adversity (Theron & Donald, 2012).
The availability of school psychologists within schools in India, however, is likely to present some serious challenges. A study conducted approximately 15 years ago found that counselling services were available in only 9% of schools in India (Bhatnagar, 1997), and a more recent study of school psychology provision in 83 member states of the United Nations found the number of school psychologists in India was unknown (Jimerson et al., 2009). It is estimated that in the world’s most child-populous countries (China, India, and Indonesia), at least 379 million children have no access to school psychology services (Jimerson et al., 2009; Ying, Wu, & Lin, 2012). In India, psychologists, including counselling psychologists, tend to work in clinics and provide support to schools and services for children rather than being located within school environments where they can deliver key services such as individual assessments, specific interventions for individuals and groups, training for other school staff, and promoting mental health and wellness overall. Hence, the profession of school psychology in India is in its relative infancy despite advocacy for the same at least two decades (see for example Paliwal, 1984; Arulmani, 2007). To this end, the Indian School Psychology Association (InSPA) is setting an aspirational goal of appointing at least one trained school psychologist in each school (InSPA, 2010). To meet this goal will require enormous professional effort and political will. Should it be achieved, school psychologists in India will be well on the way to creating supportive contexts with capacity to build resilience for and with children in the face of adversity.
Footnotes
Acknowledgements
Sibnath Deb acknowledges the work of Dr Subhasis Modak in data collection for this study. Sincere gratitude is extended to the school authorities for giving permission for data collection, and to the students who volunteered to be part of the study; they merit special appreciation. The collaboration between India and Australia to facilitate dissemination of these research findings was made possible by an Endeavour Executive Award awarded to Sibnath Deb when he was a Visiting Research Fellow in the Faculty of Health, Queensland University of Technology. To support the completion of this research Dr Walsh was supported by a Queensland University of Technology Vice-Chancellor’s Research Fellowship (2010–2012).