
Abstract
School communities face challenges in responding effectively to the rising incidence of student self-harm. Evidence-informed guidelines may provide a platform for schools to provide better responses and improve the outcomes of students who engage in self-harm.
This paper critically reviews policies published in English targeted for schools or education settings on effective early identification and intervention for children and adolescent self-harm. A grey literature search was conducted using Start Page web search engine with a documentary analysis approach applied to review polices that met criteria.
The review identified 16 policies that aim to help school and education staff to identify and respond to student self-harm. The key themes include identification and risk assessment, intervention, roles and responsibilities, as well as addressing issues surrounding evidence-based psychological education and intervention.
An evidence-informed policy that addresses multiple aspects of responding to and reducing student self-harm may be a vital foundation of a school’s response to this growing public health issue. This paper outlines key points that will help inform the development of evidence-informed guidelines for schools to respond to student self-harm and presents an exemplar policy framework for use by schools.
Self-harm, defined as deliberately harming oneself physically, often without the intent to die (Martin et al., 2016), includes a range of behaviours, with cutting, burning, scratching, hitting and overdosing on medication among the most common (De Leo & Heller, 2004; Martin et al., 2010). Self-harm is considered a major public health issue, and has previously been referred to as the ‘new epidemic’ (Heath et al., 2006). This imperative is further emphasised by the inclusion of non-suicidal self-injury (NSSI) disorder as a condition for further study in the most recent Diagnostic and Statistical Manual for Mental Disorders (DSM-5) (American Psychiatric Association, 2013; De Riggi et al., 2017).
Research indicates that the global lifetime prevalence rate for self-harm in adolescents is between 16 to 18%, highlighting the significance of this issue (Muehlenkamp et al., 2012). However, rates of help-seeking for self-harm behaviour are low for this age group and between 33% and 50% of adolescents who self-harm do not seek help for these behaviours (Rowe et al., 2014). Further, students who do seek help are more likely to go to their peers, compared with family members and teachers, for support (Berger et al., 2015a; Rowe et al., 2014), and furthermore, there is a decline in help-seeking from family members as young people age (Rickwood et al., 2005). Some identified reasons for the discrepancy between adolescent prevalence rates and help-seeking behaviour include lack of knowledge of where to access help, concerns regarding confidentiality, fear of stigma, judgement or negative appraisal, and having experienced negative or inconsistent responses when seeking help previously (Rowe et al., 2014).
The majority of adolescents spend a large portion of time at school, making school central to their lives and therefore schools hold a unique position in terms of educating, identifying, responding to, and providing support for student self-harm (De Riggi et al., 2017; Rickwood et al., 2007). Further, given that school staff are often the first to identify student self-harm and schools often have unique access to mental health services including psychologists on-site (Hasking et al., 2016; Rickwood et al., 2007), schools are well positioned to address some of the barriers to help-seeking.
According to one study by Berger et al. (2015b), nearly 70% of education staff report having encountered at least one student who engaged in self-harm. However, these teachers also reported that they have minimal psychological education regarding self-harm and were ill-equipped to respond appropriately to adolescents presenting for help. Another study of teachers’ knowledge and attitudes towards self-harm (Heath et al., 2006) found 78% of teachers underestimated the prevalence of self-harm and only 20% felt knowledgeable about self-harm. The results also indicated a mixture of attitudes towards self-harm, with 48% of teachers finding self-harm ‘horrifying’ and 12% reporting that self-harm was ‘often manipulative’. However, qualitative analysis of these teachers’ responses also revealed a strong desire for further knowledge and training, with an overwhelming amount of teachers responding that they felt ill-equipped and unprepared to manage self-harm within the school context.
As a result of the lack of resources and training surrounding self-harm, Robinson et al. (2008) designed, delivered and evaluated a training course to school staff in Melbourne, Australia. The longitudinal study found that at baseline staff demonstrated high confidence, skill and knowledge, and a relatively positive attitude towards students who self-harm (Robinson et al., 2008). Post-training evaluation found that there was significant improvement in confidence, skill and knowledge of school staff towards self-harm, and that these improvements were sustained at a six-month follow-up. In 2018, the current authors collaboratively developed accredited training for teachers, and found that providing teachers with additional training on complex mental health issues and associated behaviours, such as self-harm, was well received (Townsend et al., 2018). Our results indicated improvements in class teachers’ knowledge and attitudes towards self-harm and complex mental health issues. The intervention also improved the capacity of schools to plan and implement strategies to reduce the impact of mental health problems on the young person and their peers.
These studies suggest that providing psychological education to school staff supports the improvement of skills and confidence in identifying and responding to self-harm among adolescents. However, research identifies the need for evidence-informed policies to guide responses to student self-harm (Berger et al., 2013; De Riggi et al., 2017). Implementation of evidence-informed policies may be a platform for schools to provide more appropriate responses and improve the outcomes of students who self-harm (Robinson et al., 2016). The provision of appropriate resources to support students may also help to alleviate teachers’ fear and anxiety around self-harm (Best, 2006), allowing the best response to student help-seeking.
Recognising the need to provide schools with education and policies, several evidence-informed guidelines and reports have been developed to inform school policies. Recommendations include developing whole-school approaches, detailing correct and consistent protocol for disclosure and risk assessment, addressing concerns about confidentiality and stigma, and providing accurate information and support to all students, including peers of those who self-harm (De Riggi et al., 2017; Hasking et al., 2016). Moreover, school policies are recommended to clearly outline roles and responsibilities of staff, educate staff in self-harm and detail correct procedure for contacting parents (Hasking et al., 2016). Research that asked adolescents what they needed from schools to support themselves and peers in relation to self-harm, highlighted that policies should include educational components to support peers of students who self-harm, provide information on how to safely and confidently access help (Berger et al., 2017; Fisher et al., 2017) and provide guidelines on how staff can listen and talk to students, reduce stigma and have clear directives on referral procedures (Berger et al., 2013).
Despite the increasing prevalence of self-harm among adolescents, the desire for psychological education and self-harm policy in school settings by education staff and the development of some evidence-informed guidelines, minimal research has been conducted into current policies. For example, research with teachers in Australian schools has shown that self-harm policy is currently rare (Berger et al., 2015a), which may be limiting teachers’ ability to respond to self-harm. We aim to explore self-harm policies that are currently in use in schools and education settings and identify how these can shape the development and implementation of self-harm policies more widely in schools. Further, we aim to identify common themes in current self-harm policies, recognise areas that may be lacking in current self-harm policies and provide an exemplar policy framework. In doing so, we hope to further recognise the importance of school self-harm policies, and address issues with support and help-seeking behaviours in adolescents in the school context.
Methods
Procedure
The researchers conducted a search of existing publicly available self-harm policies and guidelines during January 2019. A grey literature search was conducted using Start Page. Start Page was chosen as opposed to a more widely used search engine such as Google or Google Scholar as these are restricted by location and search history, potentially limiting the results accessible (Pariser, 2011). Start Page privacy settings means searches are not restricted by location or search history. This search engine takes results directly from Google and therefore has the benefits of using Google for a grey literature search by identifying a large volume of literature not indexed by databases and reduces the required time needed for searching, allowing identification of many publications (Haddaway et al., 2015).
A grey literature search was selected as it was more likely to identify accessible sources that professionals are likely to use (Godin et al., 2015) and they are appropriate to the context of where the policies are implemented (Adams et al., 2016; Benzies et al., 2006) . Grey literature searches do not have the same limits as those imposed on peer-reviewed article databases meaning the searches often yield large and overwhelming results (Benzies et al., 2006). Due to the wealth of information presented on the internet and lack of standard indexing it was important to develop a systematic search strategy to ensure transparency, minimise bias and ensure time and resource demands were manageable (Adams et al., 2016; Godin et al., 2015) and Start Page search engine results were limited to the top 100 results per search term. This is in line with other studies who review 60–80 results per search term (Nove et al., 2017). A combination of the following search terms were used: policy, self harm, self-harm, SH, DSH, guideline, policies, policy, non-suicidal self-injury, non suicidal self injury, NSSI. Sources known to researchers and scanning of reference lists of policies identified through the electronic search was also used. Inclusion criteria included localised policies applicable to education settings and/or schools. Exclusion criteria included policies not published in English; being designed for a population or work setting not specific to education, for example specific protocol for emergency departments or forensic settings; being an adapted version of an existing policy; being designed for a general population not specific to education; being unable to access a document, despite contacting author or organisation; a document being outdated or replaced; being designed for psychological education rather than policy; and documents that provide policy recommendations or templates. The search strategy of identifying, screening, and inclusion was adapted from that used in a grey literature review on guidelines for school-based breakfast programs in Canada (Godin et al., 2015). The study flow is presented in Figure 1.

Study flow diagram.
Results
The search identified a total of 74 policies. After removing duplicates and applying the exclusion criteria, 16 policies remained. Of this total, 12 policies were tailored to individual schools, and four were targeted more broadly to staff responding to self-harm in an education setting. While our search was not limited by location, policies identified were found to only come from four countries (Australia, United Kingdom, United States of America, and Ireland). Table 1 summarises the policies.
Education setting and school self-harm policies and guidelines.
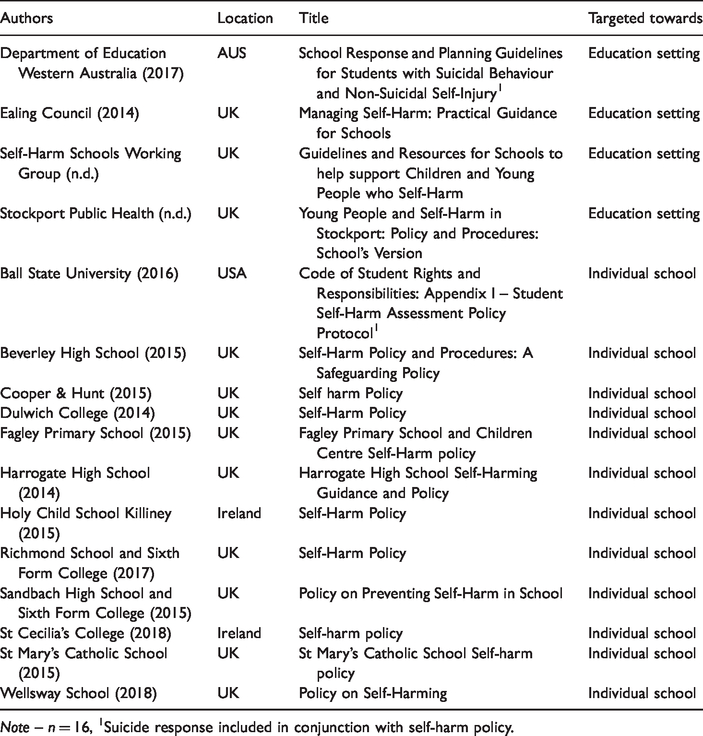
Note – n = 16, 1Suicide response included in conjunction with self-harm policy.
Data analysis
In line with previous research (e.g. Paul & Hill, 2013) the researchers conducted a documentary analysis of the policies. Documentary analysis allows researchers to understand policies at a macro level which are currently implemented in the real-world. It involves an iterative process combining both content and thematic analysis to categorise and identify patterns within documents (Bowen, 2009).
Content analysis
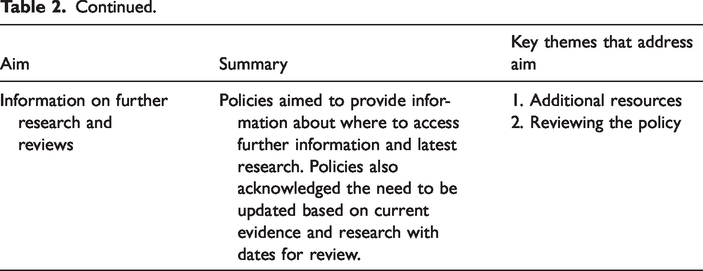
The first stage of data analysis was a content analysis which involved organising information found from documentary searches into categories. Policies were first categorised by author, location, title, and the target audience of the policy (see Table 1). Content analysis was then conducted on each policy to determine quality and extract essential information. Good policies had clearly set out aims or purposes that were thoroughly addressed throughout the policy. Table 2 provides an overview of the key aims addressed in policies and the key themes that addressed these aims. This table draws together an analysis of all the policies presented in Table 1 and offers a framework of what elements an exemplar self-harm policy for young people would include.
Aims outlined within policies and how they are addressed.
Policy aims
Thematic analysis
In the second phase of the documentary analysis, we analysed the themes within the policies. One researcher (AG) completed this by using an inductive process to identify themes. A second rater (EM) also undertook thematic analysis of the policies. Following discussion with the research team, themes of exemplar policies are presented in Table 2.
Self-harm terms and definitions
The majority of policies (n = 15) used the term ‘self-harm’, broadly defined as any behaviour carried out by a person where the intention is to cause bodily harm, irrespective of their motivation. This term encompasses a wide range of behaviours and allows for the possibility that a young person may or may not have suicidal intent. The nature and meaning of self-harm varies greatly from child to child and the reason or trigger for each action may differ on each occasion. Essentially though, self harm is any behaviour where a person intentionally sets out to harm themselves. – Wellsway School (2018, p. 2)
Most policies also discussed the link between self-harm and suicide with two policies integrating both self-harm and suicidal behaviours in the same document (see Table 1), arguing that suicide and self-harm can co-occur and it can often be difficult without in-depth assessment to determine. The policies reviewed varied in their approach to the link between self-harm and suicide. While some policies argued the two terms were separate (n = 7), other studies did not provide clear distinctions between suicide and self-harm (n = 8) or appeared to use the terms self-harm and suicide interchangeably (n = 1). Policies that emphasised differences between the behaviours argued that self-harm and suicide are representative of different motives and it should not be assumed that someone who is self-harming also has suicidal intent. However, there was an acknowledgement that self-harm does increase the risk of future suicide. People often think that self-harm is closely linked to suicide, however the vast majority of people who self-harm are not trying to kill themselves. It’s their way of coping with difficult feelings and circumstances, and people who self-harm say their behaviour is about trying to stay alive and coping, rather than killing themselves. – Ealing Council (2014, p. 5)
Key principles contained in policies
All policies (n = 16) made some reference to key principles underlying their self-harm policies. This was largely grounded in increasing protective factors in a young person’s life. This includes safeguarding individuals from experiencing self-harm behaviour, increasing their resilience, while balancing their autonomy. Policies pointed to the need to establish a safe and caring environment founded on trust between staff and the young person, with appropriate access to support and themes of hope and recovery. Policies also pointed to the importance of reducing stigma towards self-harm behaviours and responding in an empathic, non-judgemental manner: Keep an open mind about the behaviour and don’t refer to it as “attention seeking” – Stockport Public Health (n.d., p. 21) This policy has been put in place to ensure that we have a consistent approach from staff who deal with students who self-harm. It is designed so that those students seeking help will feel secure in knowing how we can deal with them – Wellsway School (2018, p. 2)
Psychological education for school staff
A substantial focus in the majority of policies (n = 13) was placed on providing psychological education for adults working with young people who self-harm. This included: the prevalence of self-harm and self-harm trends, types of self-harm, understanding the functions of self-harm, risk-factors, warning signs, myths about self-harm, self-harm and mental illness, and the cyclic nature of self-harm. The policies emphasised the need for their target audience to be aware of any assumptions or judgements they may have about self-harm, and to focus on being informed with accurate information, with many of the policies including increasing understanding and awareness as one of their aims.
Information on ‘at risk’ groups were also provided in 50% of policies. ‘At risk’ groups included adolescent females, young people in rural environments, the LGBTQIA+ community, and young people with trauma history. Additionally, information on students in residential settings, culturally and linguistically diverse students, primary aged children and/or students over 18 years old was provided in many of the policies. However, despite information provided about ‘at risk’ groups, the policies emphasised the message that self-harming behaviour is not limited to any group: Anyone from any walk of life or any age can self-harm, including very young children. Self-harm affects people from all family backgrounds, religions, cultures and demographic groups. – Ealing Council (2014, p. 7)
Education of young people
Policies (n = 8) recognised the need to educate young people about self-harm as a prevention strategy. Policies provided details on methods of educating young people as well as factsheets and resources to use. The education approach differed among policies, with some policies recommending specific units tailored towards self-harm while others advocated for self-harm education being integrated into general mental health programs: Programs that aim to improve general mental health and wellbeing at the individual and organisational level, promote health seeking behaviour and reduce stigma associated with all mental health issues are useful in addressing the issue – Government of Western Australia (2017, p. 13)
Identification and risk assessment
Understanding how to identify an individual at risk was covered thoroughly in psychological education-related sections of self-harm policies (n = 10). Risk assessment was assessed at different levels, with each level designating appropriate action to follow. Generally this followed from low, moderate, to high risk. There were some differences among policies as to whether a risk assessment should be conducted by a staff member, such as a teacher, or by a mental health professional. The general consensus was that an informal risk assessment could be conducted by the person immediately responding to the situation to inform their response (i.e. refer the student to a school counsellor or call emergency services), while a thorough risk assessment should be conducted by a mental health professional. Some policies (n = 4) provided sample risk assessment templates in their appendices, aiming to streamline and provide consistent assessment procedures.
Interventions implemented
Intervention refers to the processes involved in supporting someone who engages in self-harm behaviours, with all policies (n = 16) providing details on intervention procedures. The initial response following the identification and assessment of risk predominantly focused on the immediate safety of the individual and any risk of harm to others. Policies differentiated between interventions for suspected self-harm versus interventions for current self-harm within the school environment. Intervention for suspected self-harm involved compassionate conversation with the young person, while more life-threatening risk involved contacting emergency services. It was also noted that intervention may involve finding ways to engage in the behaviour safely and promoting alternate coping strategies, with some policies including recommendations and templates for risk management or action plans to complete with the young person. Policies also noted the importance of adults recording the incident. This was particularly evident in individual school policies which outlined formal reporting procedures and the key staff members to be informed. Other policies took a less formal approach, advocating telling senior staff about the behaviour.
Once the young person’s safety has been established, effective communication was recognised as a fundamental factor of intervention with a young person who engages in self-harm behaviour. Policies reported that all communication should be centred on empathy and understanding the function of self-harming rather than focusing on the injury. A number of policies noted the importance of a positive experience of help-seeking. Policies recommended acknowledging, but putting aside, any assumptions or judgements about self-harm, as this may impact on the way school staff intervene with a person engaging in the behaviour. Other key values demonstrated as vital to effective communication involved: the importance of staying calm; active listening; expressing concern; giving support and reassurance; and having courage and compassion in asking about their self-harm. Most individual school policies also included sections on additional considerations for students engaging in self-harming behaviour. Some examples included the option for long-sleeved school uniforms and time out cards from class during times of distress.
Roles and responsibilities of school staff
Clear roles and responsibilities among staff was highlighted in all policies (n = 16) as key to the effective management of self-harm. Policies emphasised that roles and responsibilities of each staff member need to be clearly allocated and known amongst all staff.
Majority of policies (n = 14) included appointing a key person or team to deal with self-harm matters. Teams and roles differed between policies and included a designated safeguarding officer (Stockport Public Health, n.d.), nominated staff member (Government of Western Australia, 2017), designated key staff members (Ealing Council, 2014), designated senior person for child protection (Harrogate High School, 2014), pastoral care team (Holy Child School Killiney, 2015), wellbeing manager (Beverley High School, 2015) and child protection officers (Dulwich College, 2014). Responsibilities of these staff members generally included safeguarding, ongoing communication and monitoring, receiving up-to-date training, and referrals. This designated approach allows for a more streamlined and effective way of supporting the person self-harming and reduces burden among staff.
Within staff roles and responsibilities, the importance of maintaining a whole-school or team approach was also emphasised. Although some staff would have more specialised roles in managing self-harm, having open communication about staff roles and responsibilities and displaying a consistent approach to managing self-harm was recognised in the policies as vital: It is useful for all school staff to have an awareness and understanding of the mental health issues facing young people and the processes in place in the school and system to manage and care for a student – Government of Western Australia (2017, p. 4) Pupils who self-harm need support from school staff but with the appropriate help they must learn to take responsibility for their own self-harm. – Beverley High School (2015, p. 9)
Confidentiality and consent
Issues surrounding confidentiality of personal information, was referred to in 13 of the policies. This included young people having the right to confidentiality but also being informed if any breaches to confidentiality may be required, such as imminent risk of harm or needing to contact parents or carers. Policies also considered situations where a decision may be made to break confidentiality without the young person’s consent. Advice included making a judgement on the imminent risk and the age of the young person.
The importance of a careful but upfront conversation about confidentiality with young people was also noted by policies. This is particularly important given that students may avoid disclosure of self-harm and mental health issues for fear that emergency services or their parents/carers will become involved. Most policies encouraged staff to be open, honest and clear regarding the limits of confidentiality in order to foster openness and trust but to also reassure the student that these measures are in place to ensure that their safety is a priority. Students should be aware of any disclosure and involved in the process: The best prevention for self-harm is to have people available to talk to so it is important that schools build a culture of openness. Children and young people may not like or want their information to be shared with others in order to help them, however they may be more reassured if you explain exactly who you are going to speak with, the reasons for doing this and when, and give the child or young person an opportunity to accompany you. – Self-Harm Schools Working Group (n.d., p. 22)
Connecting with families and other services
A key theme in the policies was the importance of connecting with families and other services (n = 15). The policies outlined the value of a collaborative approach and effective communication between services. However, this was recognised as a challenge for schools, particularly knowing when it is appropriate to contact parents/carers. Across the policies, the importance of contacting parents/carers was highlighted as part of normal procedure. It was specifically noted that parents/carers should be contacted in high risk situations, suicidality, or if emergency services have been contacted, even if the young person’s consent has not been obtained. Conversely, if the risk is low, staff should first talk to the student and encourage them to discuss the issue with their parent. During this conversation staff would seek an understanding of whether it is safe to engage with the parent/carer and how best to do this. Many policies (n = 6) also included fact sheets or information that would be useful to provide to families, as well as details on families’ responsibility. Responsibilities included keeping the young person’s school informed, following school self-harm policies, offering support for the young person and taking care of their own wellbeing.
Policies also emphasised that for the young person to get the most effective support and to maintain staff wellbeing, external services should play a role in support: You are not the only person who can support them, it is important that they understand the other people and services which may be able to help them. Part of our responsibility is to signpost young people to other sources of support and information. – Sandbach high school (2015, p. 3)
Follow-up and further support
Information on how to follow-up with a young person and further support their mental health emerged as a key theme across policies. A number of policies (n = 14) had specific referral procedures in place with designated staff members responsible for following up with the student. One of the policies indicated the helpfulness of developing a collaborative action plan: It is important that students feel that their concerns are being taken seriously and that they have an element of control over the process. A jointly negotiated action plan is a useful way of providing this. – Wellsway School (2018, p. 9)
Self-care
A number of policies (n = 9) recognised that responding to self-harm may place staff and other individuals at risk of experiencing their own psychological distress. Therefore, it was emphasised that staff need to look after themselves by engaging in regular self-care. While not generally a central focus of the policies, it served as a reminder to staff. Policies provided strategies on monitoring personal distress and made recommendations to other organisations and websites to find self-care strategies.
Additional resources
Most documents (n = 10) contained additional resources to accompany their policy. These resources varied with examples including a checklist of steps for schools to follow when responding to self-harm incidents, sample letter to parents/carers, incident form, factsheets, useful contacts and online support. Resources also included useful tips for staff such as lists of ‘dos and don’ts’ and conversation prompts (i.e.: Stockport Public Health, n.d.). Some policies also recommended either their own or third-party training for staff, highlighting the importance of upskilling staff members’ response to self-harm.
Reviewing the policy
Over half the policies (n = 9) mentioned the importance of reviewing the policy every one to two years to ensure that it is in line with current research and guidelines, recognising the importance of evidence-informed guidelines. Without such review, the policy may become outdated.
Exemplar policy framework
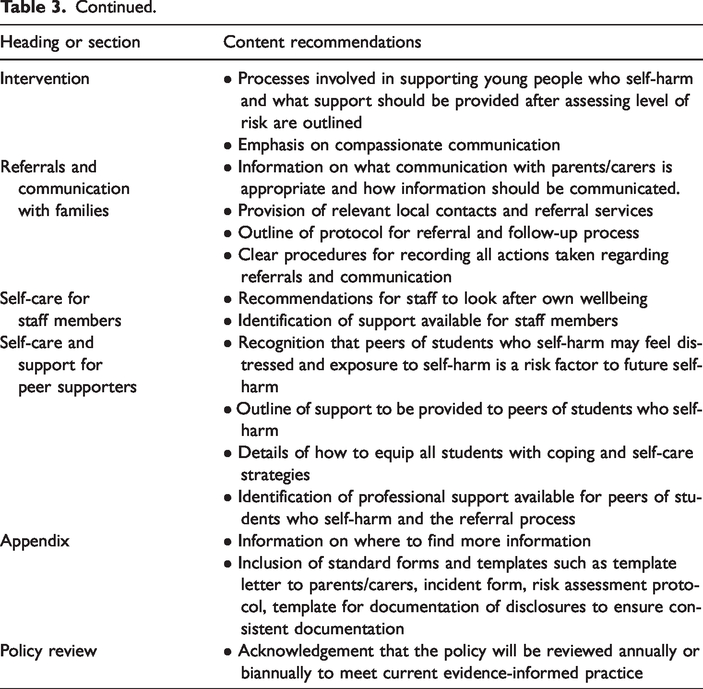
In the final phase of the documentary analysis, we identified an exemplar policy framework for self-harm in young people in schools. This framework was developed through assessing the common themes revealed in the thematic analysis and identifying what was most advantageous for schools to include in their self-harm policy based on current evidence and recommendations (Berger et al., 2015a; De Riggi et al., 2017; Hasking et al., 2016). Table 3 presents our recommendations for an exemplar policy for schools to identify, support and respond to self-harm in young people. Included in this framework are essential headings and content that comprehensive policies should include.
An exemplar policy framework for self-harm in young people in schools.
Discussion
The present study critically reviewed policies for self-harm in schools to understand the key themes of policies that inform the development and implementation of responses to student self-harm. We present here an exemplar policy framework for use by schools that is based on the current evidence and our review of published policy documents in English for self-harm in education settings. The review identified 16 policies that aim to help school and education staff identify and respond to self-harm in young people.
While the review indicated that a number of self-harm policies exist, there is still a need for policies targeted for the needs of education contexts, particularly outside of the United Kingdom. We specifically chose a search engine that did not limit results to location, however the policies reviewed were found to be from only four countries. While we were limited in that only policies in English could be reviewed which may have excluded policies from countries where English is not the primary language, this paper highlights there is still an evident need for school self-harm policies internationally. This demonstrates a gap between the evidence and implementation in practice, which may contribute to education staff feeling under-equipped and distressed when responding to self-harm behaviour (Heath et al., 2006).
Despite diversity among policies, the documentary analysis revealed that good policies contained key aims or purposes that were addressed by major themes for responding effectively to incidents of self-harm. Aims that informed good policies included increasing understanding, as well as providing consistency and support for risk assessment and intervention. Inclusion of psychological education for students, procedures for confidentiality, and outlining clear roles and responsibilities appear to be fundamental to the policies focused on responding to self-harm. In line with the literature, the themes indicate the need for well-informed education staff and resources that would facilitate an effective and comprehensive response to incidents of self-harm (Robinson et al., 2013). Themes regarding improving knowledge and confidence among staff also indicate the value of systemic and comprehensive guidelines. Thus, the themes outlined here should be thoughtfully considered when developing a policy for education staff responding to student self-harm.
Despite the documentary analysis providing a number of common key themes, there are some areas recommended in evidence-informed guidelines that we found to be lacking in school self-harm policies. Given self-harm is a common symptom in several mental health disorders that may emerge during adolescence, such as borderline personality disorder (BPD) and major depressive disorder (MDD) (American Psychiatric Association, 2013), it may be that policies should address or make reference to mental illness in adolescents, if only briefly. Indeed, Boylan et al. (2019) recommend that all clinical practice guidelines for self-harm in adolescence should provide some information on comorbidity with BPD and found in a review of guidelines that this was lacking. Similarly, our review of policies did not find comorbid disorders such as BPD to be a common theme and this may be an area for further research and development.
Moreover, research indicates that adolescents are most likely to seek help from peers and as a result, peers report feelings of distress or anxiety (Fisher et al., 2017). Research also indicates that exposure to self-harm or having peers engaging in self-harming behaviour acts as a risk factor for future self-harming behaviour (Hasking et al., 2013). Therefore, it is recommended that school self-harm policies address this through educating students with reliable information on self-harm, providing coping strategies to all students, encouraging peers to speak to a staff member, and providing support for peers of students who self-harm (Fisher et al., 2017; Hasking et al., 2013). Further, investigation of an education program on self-harm demonstrated that teaching students how to seek help and coping skills positively impacted their knowledge of self-harm and encouraged help-seeking behaviour (Muehlenkamp et al., 2010). While some of these recommendations were presented within the themes in our documentary analysis, it was not explicit and as a result we recommend that future school self-harm policies provide information for peers, which will support prevention and intervention. The exemplar policy framework we presented was developed through both assessing the key themes in our documentary analysis and referring to evidence-informed guidelines, therefore we have aimed to address both comorbidity and peer support in our framework. Future research should continue to explore these areas.
The strength of the present study is its ability to inform the development of comprehensive evidence-informed policies for responding to self-harm in schools. The present study can be used as framework for informing future self-harm policies for young people in the school setting. However, the analysis is limited by the number of policies reviewed and may be subject to bias. Resource constraints meant that only one search engine was used and while Start Page was chosen to identify a large volume of publications not restricted by location, some policies may have been missed. Due to access to resources, only policies in English could be reviewed which may have also biased results. Further, at times, the policies reviewed offered diverse interpretations of one issue, for example, the appropriate term to use for ‘self-harm’ and the link to suicide. These limitations may reflect the reality of the literature on self-harm and the complexity of understanding and responding to these behaviours, as well as the challenges in conducting grey literature reviews (Benzies et al., 2006). Furthermore, the extent that these policies are informed by evidence is unknown and the self-harm literature continues to develop.
While we provide here a summary of the main themes in current school policies on self-harm, as well as an exemplar policy framework, it was beyond the scope of the current study to provide detailed recommendations on best practice to address each of the content recommendations. Professionals seeking to develop school self-harm policies should use the examples and recommendations presented here, as well as referring to other evidence-informed guidelines which outline how to develop and implement policies within schools. These include a position paper for guiding responses to self-harm (Hasking et al., 2016) and research-informed guidelines and recommendations for school mental health professionals and staff (Berger et al., 2014a, 2014b; Bubrick et al., 2010; De Riggi et al., 2017). Further, future research should evaluate the effectiveness of implementing self-harm policies in schools to further understand how these policies can address help-seeking and support students and staff.
A number of self-harm policies exist, with some being evaluated for their efficacy in practice (e.g. Berger et al., 2015a). However, there is still an imperative to develop evidence-informed policies for responding to self-harm in schools (Berger et al., 2015a; Robinson et al., 2016). These policies should also account for the perspectives and needs of education staff, particularly teachers, and would require regular revision (Berger et al., 2015a). The current study can be used to inform the development of aforementioned school policies to adequately respond to adolescent help-seeking for self-harm behaviour.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: Project Air Strategy for Personality Disorders acknowledges funding from NSW Ministry of Health and NSW Department of Education.
Author biographies
![]() ).
).