
Abstract
The prevalence of domestic violence is concerning due to its debilitating impact on the psychological, social and academic functioning of children. This study explored the experiences, strengths and challenges of school mental health staff in relation to students exposed to domestic violence. Interviews with 10 school wellbeing staff working in Victoria, Australia, showed that these staff felt confronted and distressed, and were unsure of their role in managing the complexities associated with students’ exposure to domestic violence. Staff reported the need for educators, students and parents to be educated on domestic violence, and for improved school structures and policies that encourage staff consultation and self-care following students’ disclosures of domestic violence. The results of this study are discussed within the context of trauma-informed practice and multi-tiered mental health promotion in schools.
Globally, millions of children are exposed to traumatic experiences, such as exposure to family violence, physical or sexual abuse, and disasters (Devaney, 2008). Experiences of trauma in childhood can impact the psychological and physiological health of children in multiple ways, leading to adverse outcomes such as depression, anxiety and developmental issues (Perfect et al., 2016). Experiences of trauma in childhood may also result in a child’s impaired concentration at school, anxiety and withdrawal from school, learning difficulties and school absenteeism (Alisic, 2012). As such, mental health staff in schools have been identified as fundamental in providing psychological support to students exposed to trauma and in implementing wellbeing programs for these students (Berger, 2019). Therefore, it is imperative that school mental health staff receive adequate training and resources in the area of students’ exposure to trauma, including students’ experiences of domestic violence. However, limited research has explored how students’ domestic violence (DV) exposure is managed in schools, and specifically, how this issue is managed by mental health and wellbeing staff in schools.
The term DV will be used throughout this article to refer to acts of violence between current or previous intimate partners, and the experience or witnessing of these events by children (Devaney, 2008; Ellis et al., 2019). DV encompasses a broad range of violent events that occur within the home, and several terms are used to describe DV, including family violence and intimate partner violence. DV denotes any violence, abuse or threatening behaviour between individuals who are currently, or have previously been intimately involved, or between family members (Devaney, 2008). DV can include sexual, physical, financial, verbal, emotional or psychological abuse, and often victims of DV are exposed to two or more of these types of violent and controlling experiences (Buckley et al., 2007; Curtis et al., 2019; Devaney, 2008). Moreover, DV is a global issue, with the recent COVID-19 pandemic increasing rates of DV across the world (Campbell, 2020). For example, in the United States of America, Boserup et al. (2020) reported a 10 to 27% increase in instances of DV during state lockdown periods associated with COVID-19.
In Australia, from 2015 to 2016, 355,935 notifications were made to child protection services regarding children being at risk of abuse and/or neglect in their home (Australian Institute of Family Studies, 2019). Research regarding DV has also found that 50% of DV perpetrators also abuse the children in their care (Faller, 2003). In addition, it has been reported that 65% of women in Australia who have experienced DV had children in their care at the time of the abuse, and that these children had either seen or heard the violence as it was occurring (Australian Bureau of Statistics, 2017). Similar to the effects of trauma on child development, research on the impact of DV on children has found that DV is associated with greater risk of childhood mental illness (Sonego et al., 2018), problems engaging socially with peers (Vikse Nicholson et al., 2018), lowered academic achievement (Kiesel et al., 2016), and greater lifetime risk of DV exposure (Cohen et al., 2018). Enlow et al. (2012) found that young children who had witnessed DV had lower intelligence scores when compared to children who had not experienced DV. They also found that these children’s cognitive development was impaired due to the extreme stress and their impaired brain functioning following DV.
Research has also found a strong link between childhood exposure to DV and child physical or sexual abuse, with children often experiencing physical or sexual abuse by the DV perpetrating parent or parental figure (Buckley et al., 2007). As outlined by Faller (2003), children can be involved in DV in a number of ways: “These include actually witnessing domestic abuse, hearing but not seeing the violence, being forced to watch the abuse, being caught in the cross fire of violence between parents and thereby injured, being held hostage by the batterer, being used as a weapon in an attack, and being manipulated by the assailant” (p. 378). However, children and families often conceal DV and school staff may only be able to identify behavioural issues, aggression and social difficulties associated with a student’s exposure to DV (Byrne & Taylor, 2007; Devaney, 2008; Elliffe & Holt, 2019; Meltzer et al., 2009).
To understand the perspectives of children regarding DV, Buckley and colleagues (2007) conducted interviews with children to understand their experiences of DV. Children explained that their home situation led to academic difficulties at school, friction with their teachers and disengagement from school. Students also stated that greater knowledge among teachers on the impacts of DV for children would help to improve these students’ experiences at school (Buckley et al., 2007). This research highlighted the importance of school staff being aware of DV and knowledgeable about the potential impacts of DV exposure on students’ learning, behaviour and social-emotional functioning. Importantly, the findings are also consistent with the wider trauma and trauma-informed literature which has suggested that school staff should be made more aware of the prevalence, nature and impact of trauma on children (Substance Abuse and Mental Health Services Administration (SAMHSA, 2014). Alisic et al. (2012), for example, found that teachers required more trauma-informed approaches and greater trauma-based training for them to be able to adequately support students exposed to trauma. The teachers in this study also acknowledged the essential role of school mental health staff in supporting both students exposed to DV and their teachers (Alisic et al., 2012). However, research has found school mental health and wellbeing staff have little training concerning how trauma can affect students and how to assist these students in achieving greater educational outcomes (Ko et al., 2008; Powers et al., 2014).
In Australia, school mental health and wellbeing staff can include school psychologists, counsellors, welfare coordinators, speech therapists, occupational therapists, social workers and other student wellbeing staff. Australian schools have access to these different types of mental health staff, who may have varying perspectives regarding students’ exposure to DV and their role in response to these students. For example, initiatives such as the National School Chaplaincy Program (Australian Government. Department of Education, Skills and Employment, 2020) and the Mental Health Practitioners in Secondary Schools program (State Government of Victoria, Australia, 2020) have been implemented in Australia to ensure that schools can appoint a wellbeing staff member of their choosing (e.g., school chaplain and/or school psychologist) to support the social and emotional wellbeing of students and families. However, generally school chaplains, psychologists and social workers in Australia work across several schools, and there has been recent debate about the varying levels of training and services provided by these professionals in schools (Martin et al., 2020).
Currently, there is a gap in the current research concerning school mental health and wellbeing staff and their interactions with students who have experienced DV, including an understanding of their role and responsibilities, and their level of training and confidence in response to students exposed to DV. For example, mental health workers who provide treatment to students experiencing trauma have reported experiences of secondary trauma based on their work with these students. This is evidenced by symptoms among mental health staff of anxiety, avoidance of reminders about a student’s traumatic experiences, irritable behaviour, and intrusive negative thoughts about a student’s traumatic experiences (Bride, 2007). Although there is a lack of literature in the area of school mental health and wellbeing staff and students’ DV exposure, the existing research has found that school mental health staff require more training and support to respond to student issues of mental illness and trauma exposure (Berger & Samuel, 2020; Powers et al., 2014).
In addition, teachers and other school staff are obliged by state and territory laws in Australia to report any instances of suspicions of child abuse to the relevant child protection agency (Faller, 2003). Mandatory reporting laws in Victoria, Australia, affect registered psychologists, teachers, school principals, registered medical practitioners and police force members (i.e., anyone who is in contact with children through their work; State Government of Victoria, 2019). The laws state that people belonging to these groups must disclose to the Department of Health and Human Services (DHHS) if they have any belief that a child or young person requires protection, resulting from physical or sexual abuse, and when the child’s parents are unable or unwilling to safeguard their child (State Government of Victoria, 2019). The introduction of these laws has impacted practices in schools, with research in Western Australia documenting an increase in reporting of child abuse following the introduction of mandatory reporting laws (Mathews et al., 2016).
In addition to mandatory reporting, trauma-informed approaches have been designed to respond to the needs of students exposed to trauma. The SAMHSA (2014) created six principles for trauma-informed care. These include: 1) promoting students’ psychological and physical safety at school; 2) promoting trustworthiness and transparency between educators and students; 3) ensuring peer support for students; 4) ensuring collaboration and mutuality between educators and students; 5) empowerment, voice and choice provided to students regarding their learning and other goals; and 6) cultural, historical and gender issues which might impact the trauma response of students and trauma responding of school staff (SAMHSA, 2014). These principles guide teachers and school staff to understand the impact of trauma on students, encourages them to respond to these children using less punitive approaches, and promotes school culture and policy changes that limit repeated re-traumatisation of traumatised students (SAMHSA, 2014). Trauma-informed approaches in schools can be extremely beneficial for staff and students (Berger, 2019); however, implementing trauma-informed practice in schools can be challenging due to limited staff training, the lacking evidence-base of programs, inadequate school budgets and resources, and competing priorities within schooling systems (Berger, 2019; Powers et al., 2014).
The aim of this study was to look at the experiences of mental health and wellbeing staff in primary and secondary schools in relation to students who are exposed to DV. Consistent with earlier research (e.g., Berger, 2019), outcomes of this study were expected to result in recommendations for targeted training and/or school policy regarding student DV exposure for school mental health staff and wellbeing teams. Also consistent with prior research, the current study followed a similar qualitative methodology and used a similar interview schedule to earlier research with teachers and their experiences with traumatised students (e.g., Alisic, 2012; Davies & Berger, 2019). The current study investigated two research questions through qualitative semi-structured interviews with school mental health and wellbeing staff. The questions were:
What are the experiences of mental health and wellbeing staff in relation to students who are exposed to DV? What role do mental health and wellbeing staff play in response to students who are exposed to DV?
Method
Participants
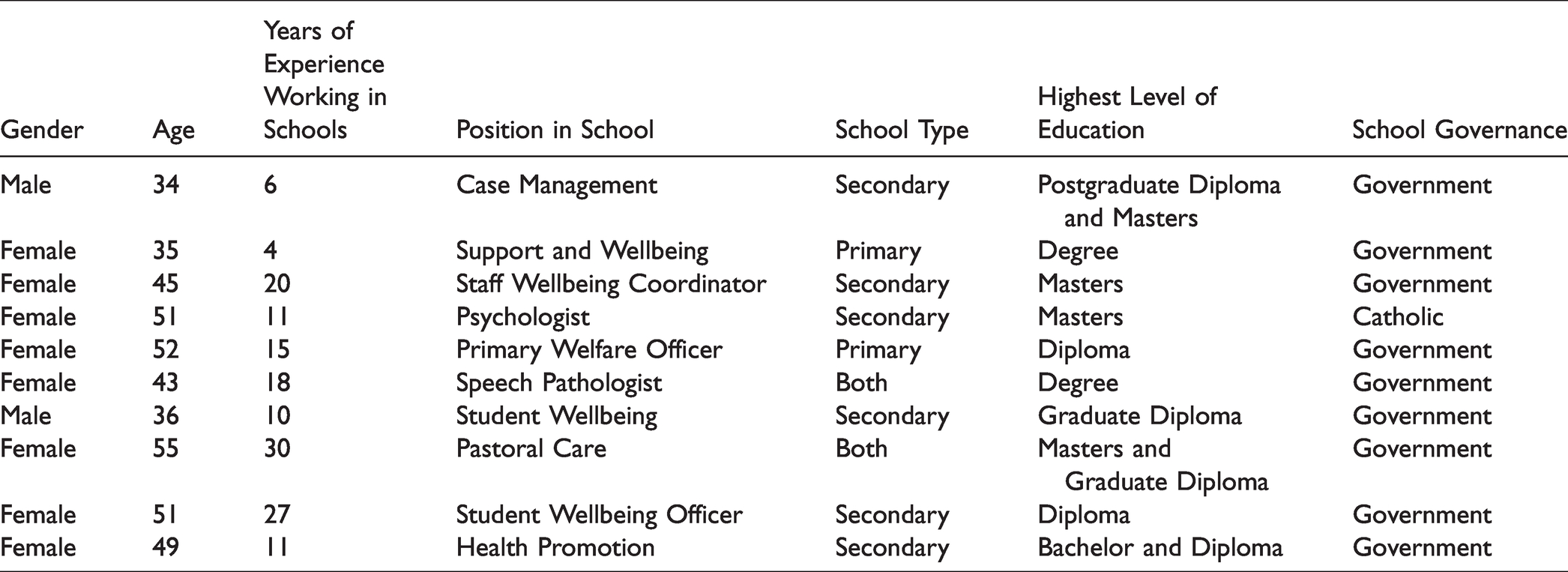
Ten school mental health and wellbeing staff (who classified themselves as wellbeing staff, school psychologists, case management workers, speech pathologists, pastoral care and health promotion workers in schools) were included in the current study (refer to Table 1). Two staff were sampled from primary schools (for children aged between 5 and 12 years), six from secondary schools (for children aged 12 to 18 years), and two combined primary and secondary schools. Participants ranged from government (i.e., publicly funded, non-denominational schools; n = 9) and Catholic (publicly and privately funded Catholic religion schools; n = 1) schools. Both males (n = 2) and females (n = 8) participated in the study, with participants ranging between the ages of 34 to 55 years (M = 45.1, SD = 7.37). Participants had an average of 15.2 (range = 4–30 years; SD = 8.13) years of experience in primary and secondary schools.
Participant demographic details.
Materials
The study consisted of conducting semi-structured interviews to qualitatively uncover the experiences of school mental health and wellbeing staff in relation to student exposure to DV. DV was defined for participants as any experiences of students in which they may have heard, seen, become directly involved in, such as attempting to intervene, or experienced the aftermath of physical or sexual violence between their parents or caregivers. Semi-structured interviews were conducted with school mental health staff using an interview schedule. This schedule consisted of questions regarding the experiences of school mental health and wellbeing staff in relation to students exposed to DV, the state of current support and training provided to school mental health and wellbeing staff, and the future support and training needs of these staff regarding this issue. Examples of questions regarding student’s exposure to DV included “Tell me about your experience with regard to students and DV?” Questions about the school context and school staff roles in relation to DV included “Could you describe any barriers you perceive to dealing with students and DV?” and “How do you talk about the topic of students and DV with colleagues, if at all?” Questions regarding current support and training included “Tell me about any training that you have undertaken in the area of DV?” Future support and training needs included items such as “Tell me about the extent to which you would like to have more information than you have now about students and DV?” Probing questions were then asked under these broader questions, such as “Can you provide an example?” and “Can you tell me more?” with probing questions dependent on the responses of participants. These probing questions explored these areas and the comments of participants in more details. The researchers have several years of experience conducting interviews in schools regarding the experiences and training and support needs of staff concerning student trauma and vulnerable children and families.
Procedure
Monash University Human Research Ethics Committee, Department of Education and Training, and Catholic Education Office approval was obtained for this study. School principals from all schools in Victoria, Australia, were then contacted and asked to give consent for the study to be presented to their school mental health and wellbeing staff. An information sheet was provided to school mental health and wellbeing staff by the principal of the school and interested staff then contacted the researchers to participate. A sample of 10 school wellbeing staff consented to participate in the study. Interviews with school mental health personnel occurred over the telephone by a researcher with several years of experience in qualitative interviewing and lasted between 40 to 60 minutes. Interviews were audio taped with a digital recorder, transcribed verbatim by a professional transcription company and subject to member checking. The process of member checking involved participants being emailed a copy of their interview transcript and given a two-week period to clarify any details or to correct details within the transcript. No participant involved in the current study accepted the invitation to revise their transcript. Following the completion of the member checking procedure, the data were thematically analysed by the authors.
Design
A qualitative research design using a constructivist epistemological approach was used to guide the current study. A constructivist epistemology perspective was adopted to construct an understanding of school mental health professionals’ experiences and perspectives in response to students exposed to DV (Savin-Baden & Howell Major, 2013). Adopting a constructivist epistemology stance and using semi-structured interviews also provides researchers with information about a topic that has been understudied in the past, compared to structured interviews or other quantitative design methods. This is because a constructivist design and semi-structured interviews encourage participants to share experiences which may be unanticipated by the researchers, while also allowing for the researchers to direct the interview in line with predetermined research questions. Based on the lack of prior research in this area, a semi-structured qualitative approach was deemed to be appropriate for this study in order to understand the experiences of school mental health staff in relation to students exposed to DV. Through qualitative data collection and analysis, researchers can understand school mental health and wellbeing staff experiences, challenges and capacity when responding to students exposed to DV, and this information can be used to inform interventions and staff training programs for DV in schools.
Analysis
This analysis approach used Braun and Clarke’s (2006) method for thematic analysis, which is a well-established and data driven method of analysing qualitative data (Howitt & Cramer, 2008). This method follows a six-phase process that involves finding, evaluating and creating patterns and themes within the data (Braun & Clarke, 2006). Both of the authors independently analysed the interviews and collaborated on the themes in accordance with phases one and phase two of Braun and Clarke’s (2006) approach. Specifically, phase one involved both of the authors independently familiarising themselves with the data through reading and re-reading the transcripts, leading to phase two where initial themes were generated independently by the authors. The authors used mind maps to generate the themes and work through a process of identifying related themes and subthemes. Phases three, four, five and six used a collaborative approach between the two authors whereby the authors met to discuss and collaborate on the final set of themes and subthemes. This shared process involved searching and reviewing the themes, defining and naming the identified themes, and finally, writing up the results of the analysis (Braun & Clarke, 2006). Cross-checking of the data, whereby 20% (n = 2) of the transcripts were analysed by a researcher independent of the study using Braun and Clarke’s (2006) approach, showed that the final themes and subthemes created by the authors captured all the themes within the data. This cross-checking procedure and independent analysis by the researchers were used to minimise researcher bias and improve reflexivity in the data analysis.
Results
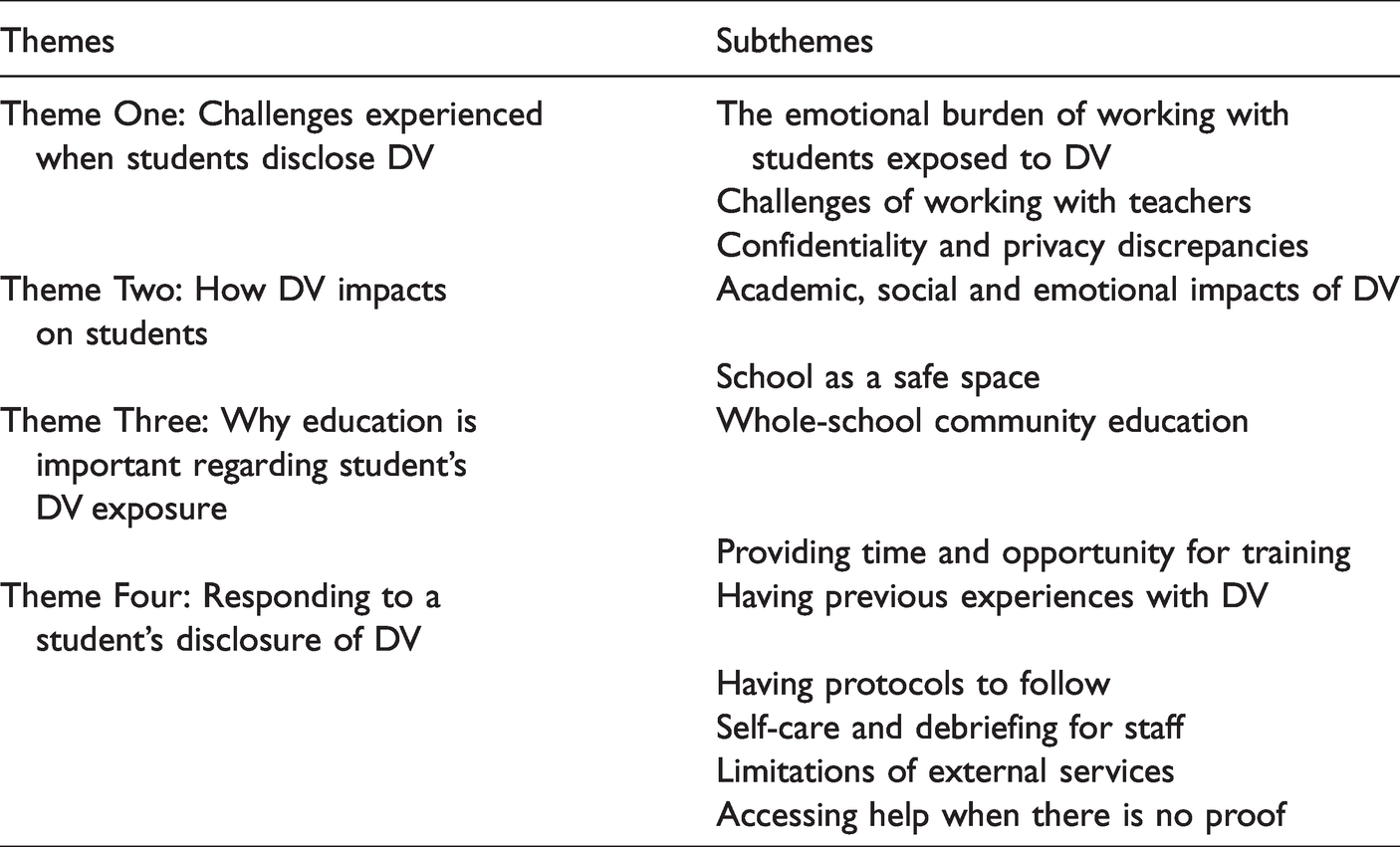
Five major themes surfaced from the analysis and are listed below (with subthemes organised within these main themes; see Table 2). Quotes have been provided to illustrate the subthemes contained within each main theme. Identifying markers are used following each quote that describe the position of the participant who supplied the quote and their years of experience working in that role.
Themes and subthemes identified in the analysis.
Theme one: Challenges experienced when students disclose DV
The emotional burden of working with students exposed to DV
Participants indicated that following a disclosure of DV they often have to assist with all aspects of the student’s life. Participants noted that students often have extremely volatile home environments, that children can become aggressive themselves, and that following a disclosure of DV, they find it extremely difficult to send the student home. Participants indicated feelings of powerlessness and being burdened by the responsibility and limitations of their role in response to student DV exposure. Staff were reluctant to contact parents following a disclosure if they were aware that the parent was the perpetrator of the DV, however also explained that open and honest communication with parents is important. Participants felt the need to support the parents of children exposed to DV. However, they noted that on some occasions parents can feel embarrassed by their situation and do not accept the help offered by staff. Participants indicated that parents had often been victims of DV themselves as children. Okay, so typically or usually they [child] have a pretty unstable home life to begin with and so the DV usually means that they’re quite anxious and fearful … they can be quite aggressive themselves. (Student Wellbeing Officer, 10 years) Some [parents] are really forthcoming and are grateful for the help and their main concern is making sure their children are okay. And the other half can be very hesitant. (Support and Wellbeing Worker, 4 years)
Challenges of working with teachers
Participants expressed concern regarding students’ disclosures of DV to teachers. They found that logistically teachers are unable to leave the classroom to assist students following their disclosure of DV. Participants revealed concerns regarding the multiple roles and responsibilities of teachers and the lack of expertise of these staff. They indicated also that often wellbeing staff in schools come from a teaching background and they are not adequately equipped to manage and support students exposed to DV. Student wellbeing need [sic] to be professionalized… most of them are not equipped to deal with this situation. They often have a teaching load and a developing role on the side … they don’t have the, the training and the expertise like a social worker, youth worker would have or a psychotherapist. (Student Wellbeing Coordinator, 20 years) If we put another single thing onto teachers, the system will break. The government need [sic] to actually start putting some money into things … rather than putting it on teachers and expecting them to carry more load. (Health Promotion Worker, 11 years)
Confidentiality and privacy discrepancies
Participants had differing opinions on whether all staff should be informed if a student has been/is currently being exposed to DV, or whether it should be kept confidential amongst specific staff members. Some participants stated the benefits of all staff being aware of the student’s DV background when working with the child. These benefits included being able to contextualise the student’s behaviour based on their exposure to DV rather than seeing the child as having behavioural problems. Other participants stated that it is imperative that confidentiality for the student and family be maintained. Participants also noted that it is important for students to have a clear understanding of the limits of confidentiality when they make a disclosure of DV, and under what circumstances confidentiality would be broken and information about the DV would be disclosed to authorities, such as child protection or to the police. But as a school, we are very open to keep our – all teaching staff informed of what’s going on because it’s really important that if you’re – if the child’s teacher knows, that then everybody externally [within the school but external to the school counselling setting] knows so that we know when things are melting down that it’s not just a behavioural. (Support and Wellbeing Worker, 4 years) A whole lot of stuff has gone on about it but no one else knows like there’s been court cases and stuff like that and she is new to the school so it’s a bit awkward in a sense that you can’t say anything… we just say look there’s stuff going on that is more important than dealing with not doing your assignment. (Pastoral Care Worker, 30 years)
Theme two: How DV impacts on students
Academic, social and emotional impacts of DV
Staff explained that some students exposed to DV are hypervigilant or hyperactive, whilst others seem to be more passive and withdrawn. Participants reported that this variation can make it difficult for staff to notice signs of DV exposure in students. Participants found that students often were not able to cope academically following exposure to DV. Staff also reported the negative impacts that exposure to DV has on students’ friendships and their emotional wellbeing. This often presented as a lack of motivation and difficulties in maintaining friendships. Sometimes kids that are being abused have no signs of affect and sometimes they can be really angry, sometimes they can be quite introverted, sometimes they can be quite really super pleasant and like totally the A+ student… because they work on those things so hard to cover up that kind of abuse. (Student Wellbeing, 10 years) I’ve seen kids be very apathetic towards doing anything in life because they are being abused emotionally, sexually and those kind of things… it can really make them fearful of creating relationships with adults and even peers and things like that because they don’t want to put themselves in those situations again. (Student Wellbeing, 10 years)
School as a safe space
Participants reported that students considered school to be a safe place in which they could escape their home lives to be in a more supportive environment. Participants also noted that if students were still experiencing DV, that they could be triggered throughout their school day. In that sense that [school] becomes their safe place and that becomes their normality so they tend to, some of them, if they have got the ability, they shut down what’s going on at home and their school becomes their safe place and their community activity, their soccer, their football. (Pastoral Care Worker, 30 years) But kids with posttraumatic stress disorder. We see kids going into – they might be grabbed on the shoulder by another child and they’ll turn around and just lose it…. they seem to be trigged constantly by bad memories. (Welfare Officer, 15 years)
Theme three: Why education is important regarding students’ DV exposure
Whole-school community education
Participants acknowledged a need for all staff to be more aware of students’ exposure to DV. Participants stated how important it is for all school staff to be trained in trauma-informed practices and to be aware of what DV encompasses and how it can manifest in children. Participants acknowledged a need for students to also be educated in DV so that they can be made aware of what DV encompasses. Participants felt that parents and families also need to be better educated on how DV affects children. They indicated that school can be a place that helps parents to break the cycle of DV through education. But there are staff that don’t have an understanding. And that’s – it’s not that they don’t have an understanding because they don’t want to, it’s because they’ve never been taught. So, you can’t put anything into practice if you haven’t been - if you haven’t learnt. (Support and Wellbeing Worker, 4 years) Just really educating the kids on what’s not normal. Because for a lot of kids that suffer from some sort of violence or anything, some of them think that’s what everybody else lives. (Support and Wellbeing Worker, 4 years)
Providing time and opportunity for training
Staff believe further training on trauma-informed practices and the impact of students’ exposure to DV is needed. Time and funding were major factors as to why participants believe that school staff are not well trained in DV, and why only certain staff are selected from schools to attend training. Participants expressed that their workload is already full so they find it difficult to attend training, despite reporting the importance of training. Teaching staff and everybody in schools generally are underpaid, overworked and do not have the time to sit down to focus on a [training] document of any variety … they are expected to do wellbeing within the classroom which they are not trained for or are trained to the minimum degree. (Pastoral Care Worker, 30 years) [Schools] don’t prioritize the right people or enough people to go [to training] because if they take teaching staff out, they’ve got to do CRT [casual relief teaching] cover, that costs money, they’re not going to do that because they don’t have the money for it. Sometimes they don’t send the right people to it or sometimes the right people don’t put their hand for it and say, I want to go to. (Student Wellbeing Officer, 27 years)
Theme four: Responding to a student’s disclosure of DV
Having previous experiences with DV
Staff who had experience with students exposed to DV felt confident and equipped to deal with a disclosure when it was presented to them. Participants reported that trauma-informed training helped increase their knowledge of student exposure to DV. This allowed them to identify and understand the differences between behavioural issues and trauma in students. Staff reported that understanding these experiences, and sometimes their own personal experiences with DV, have helped them to understand the importance of self-care. The most helpful thing about my response is that because I’ve done it so many times I'm able to have enough knowledge to give to that person or that child around what’s going to happen and what’s scary and what’s not and that kind of stuff and usually preparation for what’s going to happen is usually the most anxiety reducing thing for a person in that situation. (Student Wellbeing, 10 years) I just looked at their faces and thought you are not functioning – and I suppose that’s where experience comes in whereas a younger person who hasn’t had a lot of experience in domestic violence type stuff, they might dismiss it as oh they’re tired. (Pastoral Care Worker, 30 years)
Having protocols to follow
Participants expressed conflicting attitudes towards having strict protocols to follow. Most participants preferred being able to follow a set of rules, such as the mandatory reporting procedure, as well as school specific protocols. They felt that protocols protected them. However, some staff noted certain grey areas in school policy that hindered their responses, such as children begging them not to tell anyone for fear of the situation becoming worse at home. Grey area might be I'm getting abused at home, but if you tell anyone about it I know I'm going to get abused more. Or if you tell my parent or they find out then I'm in more danger than I was beforehand, so then the protocols become grey. (Student Wellbeing Officer, 10 years) I’m a mandated reporter. It’s absolutely clear – and sometimes I think that protects or also is very supportive to me because as distressing as that might be in some situations, I’m required to. (Student Wellbeing Officer, 27 years)
Self-care and debriefing for staff
Staff-to-staff debriefing and external support were reported as extremely important in the process of training and self-care. Staff reported that their experiences with students exposed to DV have helped them to understand the importance of self-care. However, some participants felt reluctant to access external psychological help and stated that wider cultural change within school settings is needed to reduce stigma related to help-seeking and increase staff access to supervision and consultation, either from their colleagues or from external mental health professionals. They think their principal will see it as a weakness [accessing help] so they’re not going to put me into a higher position if I’m the one that needed EAP [Employee Assistance Program] so it’s all around that stigma… rather than recognize, yay, this person actually is looking after themselves. (Student Wellbeing Officer, 27 years) The whole culture in education is stuffed … . I don’t think the system works particularly well. Another school was like don’t you dare ring anyone else – we will deal [with it] in school and they don’t have the skills to do it. … and hiring their own internal school resources that aren’t qualified to do what they are doing. (Pastoral Care Worker, 30 years)
Limitations of external services
Staff considered external resources to be flawed. Participants felt external resources would try to pass cases of student neglect or abuse off to each other and not take ownership of cases. As a result, staff felt limited in what they could offer to support children exposed to DV. For example, participants reported difficulty when working with child protection services, as they believe them to be understaffed, under-resourced and overworked. They found an inconsistency in the amount of support the child and family would receive, either enough support or support that was grossly inadequate for the child and family. The complaint often is that services say, “Oh we are not equipped to deal with that case because it’s too complex.” And then it’s like a hunt, hunting of any other services or individual counsellors or psychologists who is able to take a referral. (Staff Wellbeing Coordinator, 20 years) Especially DHHS [Department of Health and Human Services] being overworked and … depending on what case manager a child gets to whether they get proper support … there’s not a consistency around how well children are supported from outside agencies. (Speech Pathologist, 18 years)
Accessing help when there is no proof
DV encompasses many different types of abuse, including physical, sexual, verbal and emotional. Participants believed external organizations found it difficult to make cases against verbal and emotional abuse as there is little or no proof, thus this is a barrier to gaining assistance. However, participants could note times when they felt that external organizations helped. They found that these organisations had improved in terms of their training and standards in response to students exposed to DV. If you are reporting on – and I’ve had this discussion with DHHS – if you are reporting on basically mental abuse or emotional abuse technically it’s not reportable – it’s not recognized because there is no proof. (Pastoral Care Worker, 30 years) Often it’s not a physical abuse that’s happening, it’s, verbal and emotional which is more difficult to address … if we’re looking at trying to get child protection intervention or similar … it’s harder to make a case. (Case Management Worker, 6 years) I’ve just recently done a couple of reports and I’ve been very impressed with, well much more impressed with Child Protection staff, who’ve come out to interview the kids … I’ve been impressed with all of them actually. So I think they’ve gotten a lot more training. (Psychologist, 11 years)
Discussion
This study aimed to fill a current gap in the literature about the experiences of mental health and wellbeing staff in schools in relation to children exposed to DV. Specifically, the study explored the experiences of school mental health and wellbeing staff in Australia and their perception of the school response in relation to student DV exposure. Staff showed an understanding that schools can be triggering for students who have experienced DV and the impact that this can have on students’ academic performance. Participants also expressed understanding of the importance of whole-school training and debriefing for staff, the importance of their ability to form relationships with students and parents exposed to DV, and the necessity of self-care when responding to these students and families. Challenges for staff included their lack of education in this area, their difficulty identifying the signs of DV and in managing the social, emotional, behavioural and academic impacts of DV for students, problems understanding confidentiality and appropriate disclosure of a student’s experience of DV, and problems accessing external assistance and services for children and families exposed to DV. The issue of confidentiality requires clear policies and guidelines for school staff regarding their ethical responsibility to report students’ experiences of DV. While mandatory reporting legislation of child abuse and neglect exists for school staff, there are ethical considerations for school mental health staff around disclosure of information and breaching of student and parent confidentiality. Prior research has shown the benefits of consultation and debriefing between school staff regarding a student’s home circumstances to improve students’ classroom learning and wellbeing. For example, teachers have reported that they and their students benefit when they know when a student has visited with their DV perpetrating parent, or when a student has had a disrupted day or night before attending school (Berger et al., 2020).
It can be challenging for school wellbeing staff to understand their role in situations of students’ exposure to DV. This included difficulty managing the impact of DV on the students’ social and academic functioning, as well as the complexities of working with parents when they are known perpetrators or victims of DV. Added to the role of school mental health and wellbeing staff to support students and families is their role to support and provide training to teachers. Although maintaining student, staff and parent wellbeing, as well as responding to referrals from teaching staff, is clearly within the role of school mental health workers, this study found that some school mental health staff can become overburdened by and may not have the appropriate training to undertake this role. The current results also suggested that wider structural change and policies are required to support staff around issues of mandatory reporting of child abuse and neglect, maintaining confidentiality of students and families, and approaches to make schools ‘a safe place’ for students by removing triggers which cause student re-traumatisation. Staff also made recommendations that mirrored trauma-informed practice around supporting students exposed to DV. These recommendations included recognising that the child’s behaviour is a result of their trauma, giving students time and space if they arrived to school with their ‘bucket already full’, and acknowledging that school can be re-traumatising for students who have experienced DV (SAMHSA, 2014). Individual learning plans (ILPs) are one method used in Australian schools to enhance home-school communication and use of trauma-based strategies by school staff. ILPs are typically developed collaboratively by parents, caregivers, classroom teachers and school wellbeing staff and can include approaches such as how to help students during transition times at school and/or development of individually tailored learning goals for students exposed to trauma (Victorian Department of Education and Training, 2020). Unfortunately, no known research has evaluated the effectiveness of ILPs and the perceptions of school staff around use of ILPs for students exposed to trauma, including DV.
Adding to the role and responsibilities of school mental health staff, participants reported that students and parents need to be better educated on the issue of DV and its effects for students. Participants believed that educating students would allow them to understand and identify DV, while for parents, training would increase their understanding of the effects of DV on a child’s social, psychological and academic functioning. Providing education for staff, students and parents aligns with the trauma-informed approach of the Healthy Environments and Response to Trauma in Schools (HEARTS) model (Dorado et al., 2016) and more recent research by Berger (2019). The HEARTS model encompasses a whole-school, multi-level approach that incorporates educating and supporting parents alongside educating and supporting teachers, other school staff and students (Dorado et al., 2016). Evaluation of the HEARTS model has found that this approach can foster greater school support and resilience amongst students impacted by trauma (Dorado et al., 2016). Participants in the current study supported a whole-school approach to professional learning, including training and support for students and parents, and training, consultation and supervision for teachers and school mental health staff. While multi-tiered support is important within schools, participants felt external resources, such as child protection and mental health services, were barriers to supporting DV exposed students. The importance of engaging with external services has been emphasised in trauma-informed models (see the review by Berger, 2019); however, the collaborative process between schools and external professionals, and models to improve this process, have not been extensively evaluated in relation to DV. Similarly, consultation approaches between teachers and school mental health workers in relation to student DV exposure have not been widely discussed in the literature. Models of consultation and communication between school staff, without breaching student and family confidentiality, need to be developed and tested in schools. Although more research is needed, recent evidence suggests that trauma-informed training for staff can improve their capacity to notice and support students exposed to trauma and students with other social, emotional and behavioural concerns (Berger, 2019; Diggins, 2020; Thomas et al., 2019).
Limitations and recommendations for future research
Whilst the current study yielded important findings for mental health and wellbeing staff in relation to children exposed to DV, several limitations need to be considered. Firstly, this study relied on staff identification of their position as a mental health worker in schools. As such, their role and experience in schools varied, with some participants moving into a school wellbeing role after studying, whilst others indicated that they once were teachers. Participants also noted that they had different levels of training regarding childhood trauma, which was dependent on their previous experience. The qualitative nature of this study meant that it was not possible to quantify the amount and level of trauma and/or DV training undertaken by staff. The diversity of the sample and broad nature of the questions is both a strength and limitation of the study, and it would be beneficial for future research to examine a more specific staff population and their experiences responding to DV in schools. Future research using more targeted samples will inform more specialist training for different members of school staff. Furthermore, this research was qualitative and conducted in schools in Australia. Therefore, it is unclear as to whether these results would be consistent within a wider population and research replicating this project design in other contexts would be warranted. What is clear from this research is that the findings both reflect what is known about the challenges (and continued challenges) of schools in response to DV, but also provide greater depth regarding the educational experience of students who experience DV, the continued trauma that can be inadvertently inflicted upon these students while attending school, and the necessity for school policies and training to support these students and their teachers. Finally, the definition which we used to define DV for this study (i.e., “experiences where students may have heard, seen, become directly involved in, such as attempting to intervene, or experienced the aftermath of physical or sexual violence between their parents or caregivers”) was narrow in order to focus on one aspect of DV - violence which occurs between parents or caregivers - however future research should use this methodology to explore the experiences of school mental health staff with students exposed to DV between siblings.
Conclusion
Mental health and wellbeing staff reported varied experiences with students, parents and external services in relation to students and their exposure to DV. Changes in training, policy and school structure were indicated as necessary to ensure that mental health and wellbeing staff are able to access training and support, and able to assist and support students exposed to DV. Ensuring that trauma-informed approaches and whole-school staff training are consistently delivered in schools will go some way to ensuring that students and school staff are supported in their roles specific to DV exposure.
Human ethics
Monash University Human Research Ethics Approval was obtained for this study.
Footnotes
Acknowledgements
The authors would like to acknowledge the work of Dylan George who conducted the interviews with participants.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.