
Abstract
The current study examines the mediating roles of self-efficacy and sleep disturbance and the moderating role of gender in the association between the duration of youth/parent communication on depression and anxiety during the COVID-19 isolation period in China. We used the self-designed demographic variable questionnaire, General Self-Efficacy Scale, the Pittsburgh Sleep Quality Index, the Self-Rating Depression Scale, and the Self-Rating Anxiety Scale with 1,772 youths aged 15–24 from 26 provinces in China during the COVID-19 lockdown. We performed demographic variable analysis, correlation analysis, mediation analysis, and moderated analysis. The duration of daily communication with parents was significantly positively correlated with self-efficacy and significantly negatively correlated with sleep disturbance, depression, and anxiety. The chain mediation analysis revealed that the duration of communication with parents directly affected depression and anxiety. Self-efficacy, sleep disturbance, and self-efficacy sleep disturbance had significant mediating and chain-mediating effects on the duration of communication with parents, depression, and anxiety. The interactions between sleep disturbance and gender (B = 0.35, 95% CI 0.06 to 0.64, p = .02 < .05) were significant. The duration of parent/youth communication directly affected depression and anxiety and indirectly affected depression and anxiety via the chain-mediating effect of self-efficacy and sleep disturbance. Gender moderates the relationships between sleep disturbance and depression.
Introduction
The global outbreak of COVID-19 began in 2020. At the time of this report, the virus was mutating, affecting public health security and imposing psychological burdens on the public (Chen et al., 2022; Ryerson, 2022; Santomauro et al., 2021; Thompson et al., 2022; Xiang et al., 2020). Studies showed that depressive and anxiety disorders increased by 28% and 26% (respectively) worldwide in 2020, with significant increases (especially among youth) in countries severely affected by COVID-19 (Santomauro et al., 2021). A literature search in Chinese databases revealed that the rates of depression and anxiety among Chinese youth increased during the pandemic (Dian-Jiang et al., 2021; Wanlong & Shihao, 2021; Xiaolin et al., 2020; Zheng Chen et al., 2020).
Depression is a mood disorder characterized by significant and persistent low mood, decreased activity, delayed thinking, and cognitive dysfunction. Simple depression is relatively rare and is commonly comorbid with anxiety (Zi-qiang et al., 2011). Anxiety is a complex emotional state generated when an individual anticipates the occurrence of an adverse consequence or vague threat; it is interwoven with feelings of tension and fear (Kircanski et al., 2017). Comorbid anxiety and depression are characterized by severe symptoms, functional impairments, profound courses, high rates of suicide, and poor outcomes (Miyuan et al., 2020). Most studies have focused on depression or anxiety alone (Kircanski et al., 2017; Pandi-Perumal et al., 2020), and there are few studies on comorbid anxiety and depression; in particular, there are few studies on comorbid depression and anxiety among youth during the pandemic. Thus, the protective factors for depression and anxiety for youth, especially in COVID-19 isolation, should be identified to help improve their mental health.
Family support is a protective factor for youth (Guerra et al., 2018; Wills et al., 1992). Studies have shown that support from family is one of the most important predictors of depression (Nasser & Overholser, 2005). Strong family support was associated with fewer experiences of depression and anxiety (Guerra et al., 2018). A study also suggested that a higher degree of perceived social support (e.g., family support) correlates with lower general anxiety among students and a lower impact on the COVID-19 pandemic (Wu et al., 2021).
The family is an individual's closest social support system and can provide care, companionship, and other emotional communication and spiritual support; the family is also the most accessible source of help for youth isolated at home (Jacob et al., 2019; Jiuju et al., 2022). Studies have shown that adequate parent–child communication time is essential for family support (Diggs et al., 2017; Vaterlaus et al., 2019). In addition, studies have found that there is a chain mediating the relationship between parent–child communication and sleep quality and depressive symptoms (Dong et al., 2022).
Self-efficacy (defined according to Bandura's self-efficacy theory as a sense of control over one's environment and behavior) is also a protective predictor of psychological distress (Bandura et al., 1997). Studies have shown that self-efficacy affects depression and anxiety (Cui-mei et al., 2022; Song et al., 2019). Furthermore, students who reported more substantial availability of family support reported stronger self-efficacy (Torres & Solberg, 2001).
Several studies have also suggested that good sleep quality is associated with depression and anxiety (Dao-Yang et al., 2016; Tsuno et al., 2005; Zhou et al., 2020; ZHU et al., 2021). Studies demonstrated that sleep quality (as a mediating variable) affects depression and anxiety, and self-efficacy affects sleep quality (Diaz-Piedra et al., 2014; Hwanjin et al., 2018; Zhu et al., 2020). Moreover, a study has shown that depression and anxiety are parallel mediating relationships between sleep disturbance and subjective cognitive decline, suggesting that sleep is closely related to depression and anxiety (Xu et al., 2021). Besides, similar literature has found that social support affects sleep quality. This suggests that interpersonal communication can affect sleep quality (Pan et al., 2022).
Studies have shown that parent-child communication has a differential effect on males and females, for example, Ohannessian's (2013) research found that open adolescent-parent communication specifically acts as a protective factor for girls but not for boys. Moreover, One study found that gender has a moderating relationship with self-efficacy (Chung et al., 2017). Furthermore, previous studies have shown that there are significant differences in sleep quality between different genders (Duan et al., 2022; Islam et al., 2021; Joao et al., 2018). Besides, the difference in gender has an influence on the degree of depression and the effect of the intervention (Cahuas et al., 2020; Sun et al., 2017). In addition, the degree of anxiety and the effect of intervention are different in different genders (Kjellenberg et al., 2022).
Although the duration of youth/parent communication, self-efficacy, and sleep quality have been identified as independent predictors of depression and anxiety in various populations, to the best of our knowledge, the associations of these five variables among youth during the COVID-19 lockdown have not been fully explored. Moreover, examining whether gender plays a role in the associations among the duration of youth/parent communication, self-efficacy, and sleep quality may be worthwhile (Diggs et al., 2017). Therefore, the current study explored the following: (1) The associations among duration of youth/parent communication, self-efficacy, sleep quality, and psychological distress (depression and anxiety) based on a serial multiple mediation model and (2) the moderating role of gender.
We hypothesize that (Figures 1 and 2): (1) Duration of parent/youth communication is negatively associated with depression and anxiety and positively associated with self-efficacy, and negatively associated with sleep disturbance, (2) Self-efficacy and sleep quality significantly mediate the association between the duration of youth/parent communication and depression and the duration of youth/parent communication and anxiety, and (3)Gender moderates the associations among youth/parent communication duration, self-efficacy, sleep disturbance, and depression and anxiety.
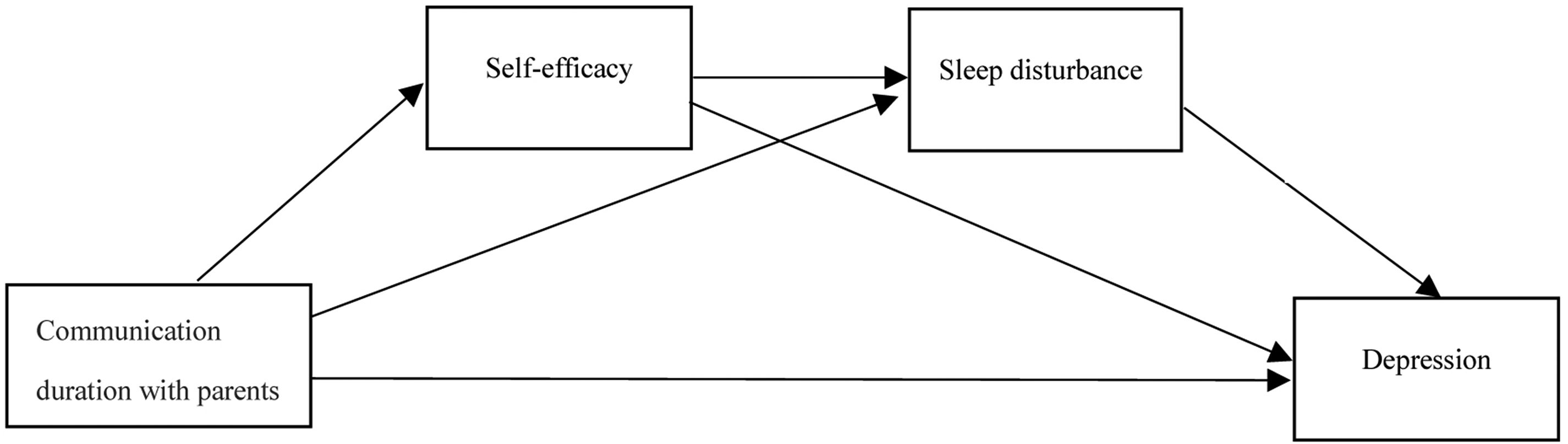
The conceptual model of self-efficacy and sleep disturbance between the communication duration with parents and depression.
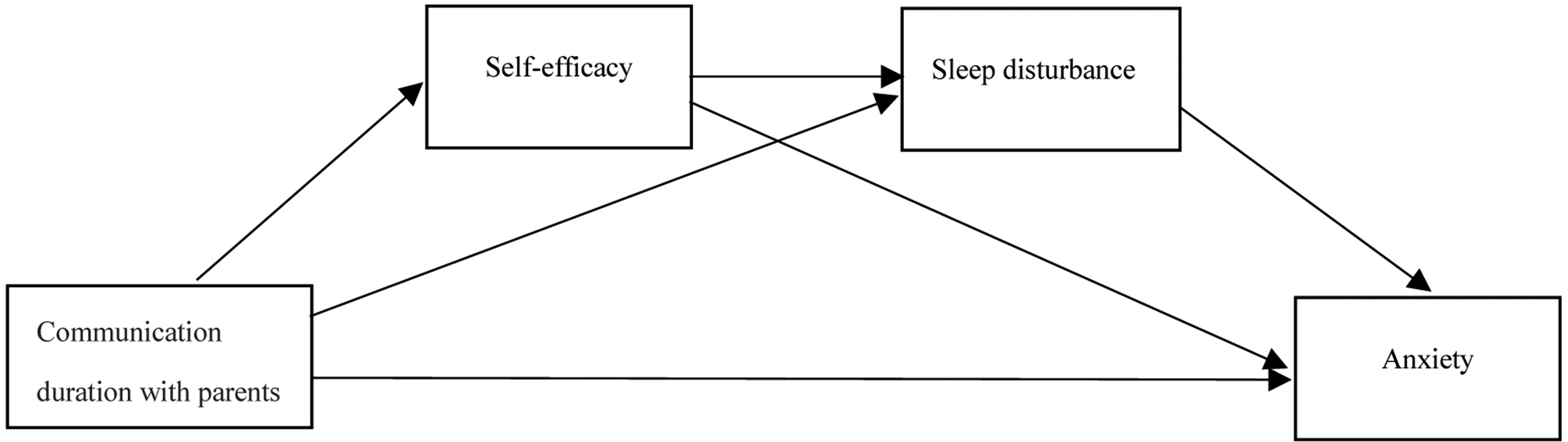
The conceptual model of self-efficacy and sleep disturbance between the communication duration with parents and anxiety.
Methods
Measures
A self-designed questionnaire concerning demographic variables and four related scales were used for the research. The subjects used mobile phones to scan two-dimensional codes and fill in the electronic questionnaire.
The self-designed demographic variable questionnaire
This instrument gathered personal information, including gender, age, educational background, residence, living place, and daily contact time with parents during the nearly one month of home quarantine during the pandemic.
Self-efficacy
The original version of the General Self-Efficacy Scale was developed by Jerusalem and Schwarzer in 1981, initially as a 20-item version and later as a simplified version of 10 items. It has been used in numerous research projects, where it typically yielded internal consistencies between α = 0.75 and 0.90. The scale is not only parsimonious and reliable, but also it has also proved valid in terms of convergent and discriminant validity. The General Self-Efficacy Scale measures individual self-efficacy with ten items on a 4-point Likert scale. The statistical index is the total score; higher scores correlate with higher self-efficacy(Schwarzer & Born, 1997; Schwarzer et al., 1999). The Chinese version of the General Self-Efficacy Scale was first used in Hong Kong in 1995 and has demonstrated good reliability and validity, with an internal consistency coefficient of 0.87, retest reliability of 0.83 within 10 days, and split reliability of 0.90 (Zhang & Schwarzer, 1995). The scale showed good internal consistency in this study (Cronbach's α = 0.90).
Sleep disturbance
The Pittsburgh Sleep Quality Index is a self-rating sleep quality scale developed by Buysse et al. in 1989. Because of its simplicity, high reliability and validity, and high correlation with polysomnography test results, it has become a common scale in research and psychiatric clinical evaluation. The Pittsburgh Sleep Quality Index measures the degree of sleep disturbance; higher total scores correlate with lower sleep quality. Seven factors are on the scale, including subjective sleep quality, sleep time, sleep efficiency, sleep disorders, hypnotic drugs, and daytime dysfunction. The measurement index is the sum of the seven factors. This scale was introduced in China by Liu Xianchen et al. and tested for reliability and validity. For the construct validity test, Liu used PSQI, SDS, and SAS to measure 560 college students. The correlation analysis showed that the correlation coefficients between PSQI and SDS and SAS were 0.43 and 0.42, respectively, showing a significant positive correlation. For the internal consistency reliability test, Liu tested Cronbach's coefficient of PSQI's 7 factor, which was 0.84. The correlation coefficients between each component and the total score of PSQI ranged from 0.63 (daytime function) to 0.81 (subjective sleep quality), with an average of 0.72, showing a high correlation. For the retest reliability test, 30 college students were evaluated again by PSQI two weeks later, and the correlation coefficient between the total scores of the two PSQI scores was 0.81 (Buysse et al., 1989; Liu Xian Chen et al., 1996). Today, PSQI is still proven to be a reliable and effective method for assessing and screening sleep disorders in the Chinese population (Chen et al., 2017). The internal consistency reliability of the scale was good among the seven factors in this study (Cronbach's α = 0.72).
Depression
The Self-Rating Depression Scale was developed by Professor Zung of Duke University in 1965. Because of its simple method and good quality, it has been widely used abroad. It was introduced in China by Wang Zhengyu and is widely used in the field of clinical psychology. The scale uses a 4-point Likert scale that measures an individual's level of depression with 20 items (10 positive and 10 negative scores). Positive items were scored on original 1, 2, 3, and 4 points, while negative items were scored on original 4, 3, 2, and 1 points. Add the scores of each item to get the original total score, and the measurement index is the standard total score. The standard total score is calculated according to the formula (standard total score = original total score × 1.25, rounded to whole number). A higher standard total score correlates with more severe depression (Quan-Quan & Li, 2012; Zung, 1965). The scale showed good internal consistency in this study (Cronbach's α = 0.70).
Anxiety
The Self-Rating Anxiety Scale was proposed by Professor Zung in 1971. From the form of scale construction to the specific evaluation method, it is very similar to the self-rating depression scale. It was introduced in China by Wang Zhengyu and is widely used in the field of clinical psychology. The scale uses a 4-point Likert scale that measures an individual's level of anxiety with 20 items (15 positive and 5 negative scores). Positive items were scored on original 1, 2, 3, and 4 points, while negative items were scored on original 4, 3, 2, and 1 points. The scores of each item are summed to get the original total score, and the measurement index is the standard total score. The standard total score is calculated according to the formula (standard total score = original total score × 1.25, rounded to the whole number). Higher standard total scores correlate with more severe anxiety (Zhengyu & Yufen, 1984; Zung, 1971). The scale showed good internal consistency in this study (Cronbach's α = 0.79).
Procedures and quality control
The questionnaires were anonymous. The instructions explained the survey's purpose in detail, and informed consent was obtained. The permissions allowed one internet protocol address to be submitted only once to prevent repeat submissions. Two questions with specified answers were inserted into the questions as lie-detection questions to screen out the subjects who did not answer seriously. If the two lie detection items were not answered correctly, the subject was classified as invalid and excluded (DeSimone & Harms, 2018; Huang et al., 2012). The total test time was about 5 minutes. The subjects could only submit the test after answering all the questions, and no modifications were allowed after submission.
Sampling and participants
In May 2020, during the Covid-19 lockdown, questionnaires were distributed to the campus network groups of four universities and three middle schools in Guangdong, Sichuan, and Shaanxi provinces by simple random sampling using the Questionnaire Star application, a popular online questionnaire application in mainland China. A total of 2231 questionnaires were received, of which 1943 were valid (questionnaires with complete answers to all questions and correct answers to two lie detection questions were listed as valid questionnaires), with an effective rate of 87.09%. All subjects were stay-at-home youth living in 102 cities in 26 provinces (including four municipalities directly under the Central Government and one special administrative region) in China. According to the definition of youth by the United Nations, subjects with an age range of 15–24 years old were included (Youth, 2022), and those below 15 years old and above 24 years old were not included in the statistics. Finally, 1772 samples were retained, with an average age of 18.18 ± 2.09, ranging from 15 to 24 years old.
Data analysis
The preliminary data were sorted using Excel and were analyzed using SPSS24.0 statistical software. First, descriptive statistics were used to analyze the demographic characteristics. Second, Pearson's correlation analysis was performed to estimate the associations among communication duration with parents, self-efficacy, sleep disturbance, depression, and anxiety. Third, Model 6 of the PROCESS macro program compiled by Hayes was used to analyze the mediation effect. Communication duration with parents, depression, and anxiety were identified as the independent (X), dependent (Y1), and (Y2) variables, respectively. The mediators were self-efficacy (M1) and sleep disturbance (M2). The total, direct and indirect effects were estimated, and the 95% confidence interval (CI) was calculated with 5000 bootstrapping resamples. Fourth, PROCESS Model 1 was used to conduct moderating analysis, including living place and the highest level of education as covariates, to explore the moderating effect of gender on communication duration with parents, self-efficacy, sleep disturbance, depression, and anxiety.
Ethical considerations
Ethical approval (LLSC2022001) was obtained from the Academic Committee of Guangzhou College of Technology and Business ethics committee. All data files are securely stored in a secure location on an encrypted computer at the college.
Harman single-factor test
The Harman single-factor test was used to diagnose common method deviation. The unrotated principal component factor analysis results revealed 14 factors with eigenvalues greater than one, among which the variation explained by the first factor was 20.14%, less than the critical value of 40%. This finding suggests no evident common method deviation in the questionnaires.
Results
We compared self-efficacy, sleep quality, depression, and anxiety among different youth groups in subgroups such as gender, living place, the highest level of education, and communication duration with parents. The analysis of demographic variables is shown in Table 1.
Analysis of demographic variables.
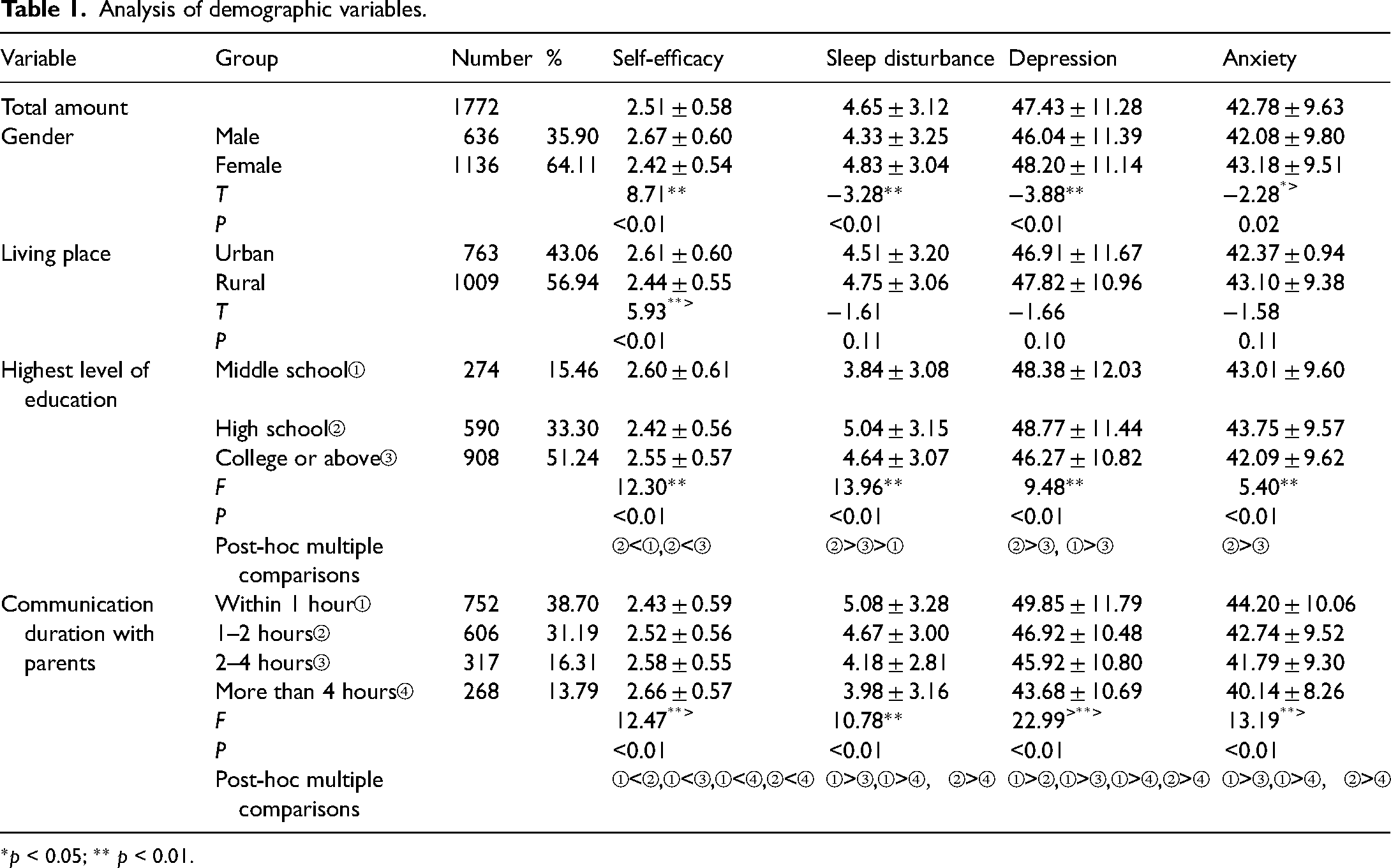
*p < 0.05; ** p < 0.01.
Pearson product–moment correlation analysis showed that youths’ daily communication time with their parents was significantly correlated with self-efficacy, sleep disturbance, depression, and anxiety (Table 2). Specifically, the daily communication time with their parents was significantly positively correlated with self-efficacy, while the daily communication time with their parents was significantly negatively correlated with sleep disturbance, depression, and anxiety. In addition, self-efficacy was negatively correlated with sleep disturbance, depression, and anxiety. Moreover, sleep disturbance has a significant positive relationship with depression and anxiety.
Correlation analysis.
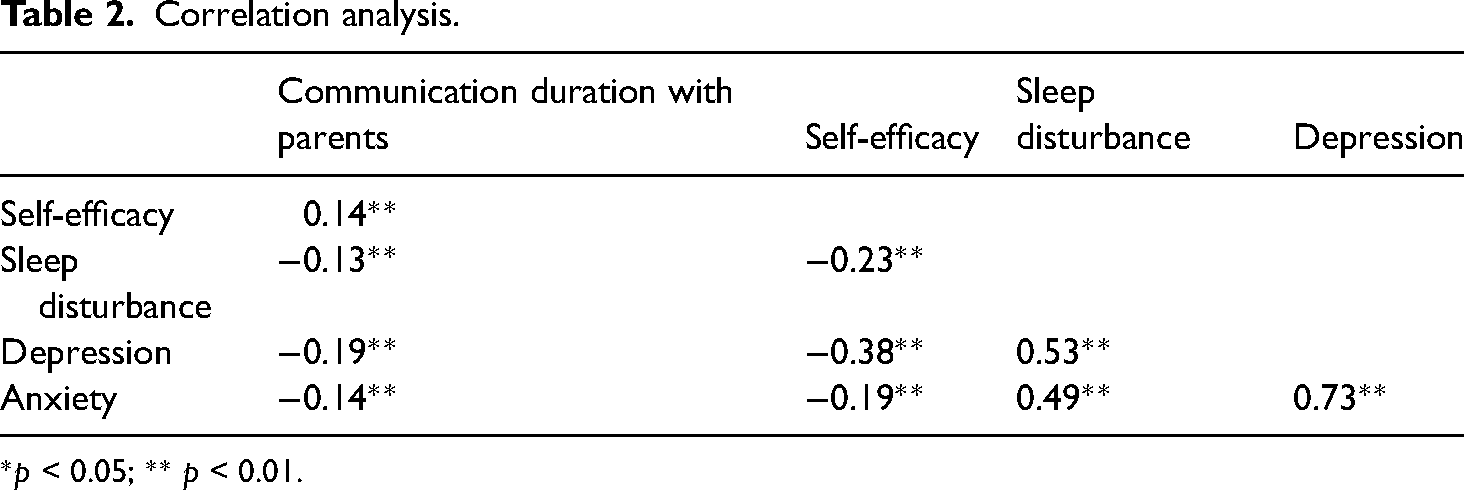
*p < 0.05; ** p < 0.01.
Chain-mediated model analysis
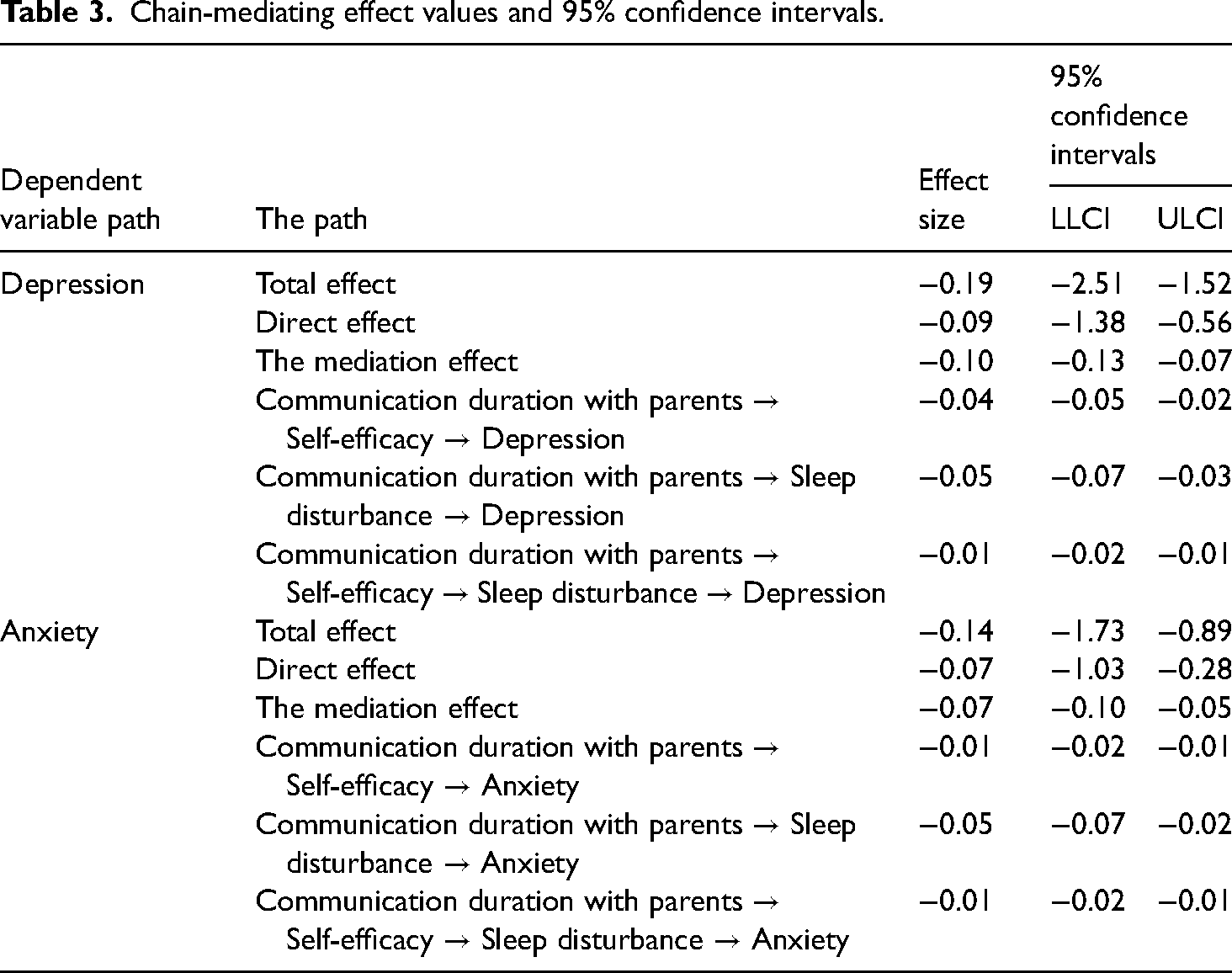
Model 6 of the PROCESS macro program in the SPSS plug-in was used. We set daily communication duration with parents as the independent variable, self-efficacy and sleep disturbance as intermediary variables, and depression and anxiety as dependent variables. The bootstrap method (5000 samples) was used to estimate the chain mediation model of “daily communication duration with parents—self-efficacy—sleep disturbance—depression” and “daily communication duration with parents—self-efficacy—sleep disturbance—anxiety.” The results are shown in Table 3 and Figures 3 and 4. Completely standardized path coefficients marked with an asterisk identify 95% bootstrap confidence intervals which do not include zero and significant levels (p < .01). In the chain-mediated test with depression as the dependent variable, the communication duration with parents directly predicted depression (B = −0.19, 95%CI: −2.51 to −1.52). The independent mediating effect of self-efficacy and sleep disturbance and the chain-mediated effect of self-efficacy and sleep disturbance were significant (B = −0.04, 95%CI: −0.05 to −0.02; B = −0.05, 95%CI: −0.07 to −0.03; B = −0.01, 95%CI: −0.02 to −0.01; respectively). Model statistics for the direct model: R2 = 0.04, F (1, N = 1770) = 64.21, p < .01. For the mediated model: R2 = 0.36, F (3, N = 1768) = 326.58, p < .01. The total indirect effect accounted for 51.87% of the total effect, the indirect effect of self-efficacy intermediary effect accounted for 19.79% of the total effect, the mediating effect of the sleep disturbance was 24.60%, and the chain-mediating effect of the total score of self-efficacy and sleep disturbance was 6.42%. The communication duration with parents directly predicted anxiety in the chain-mediated test, with anxiety as the dependent variable (B = −0.14, 95%CI: −1.73 to −0.89). The independent mediating effect of self-efficacy and sleep disturbance and the chain-mediated effect of self-efficacy and sleep disturbance were significant (B = −0.01, 95%CI: −0.02 to −0.01; B = −0.05, 95%CI: −0.07 to −0.02; B = −0.01, 95%CI: −0.02 to −0.01; respectively). Model statistics for the direct model: R2 = 0.02, F (1, N = 1770) = 36.81, p < .01. For the mediated model: R2 = 0.25, F(3, N = 1768) = 197.57, p < .01. The total indirect effect accounted for 50.35% of the total effect. The indirect effect of the self-efficacy intermediary effect accounted for 7.69% of the total effect, the mediating effect of the sleep disturbance was 32.87%, and the chain-mediating effect of self-efficacy and sleep disturbance was 9.79%.

The chain mediation model of self-efficacy and sleep disturbance between the communication duration with parents and depression.
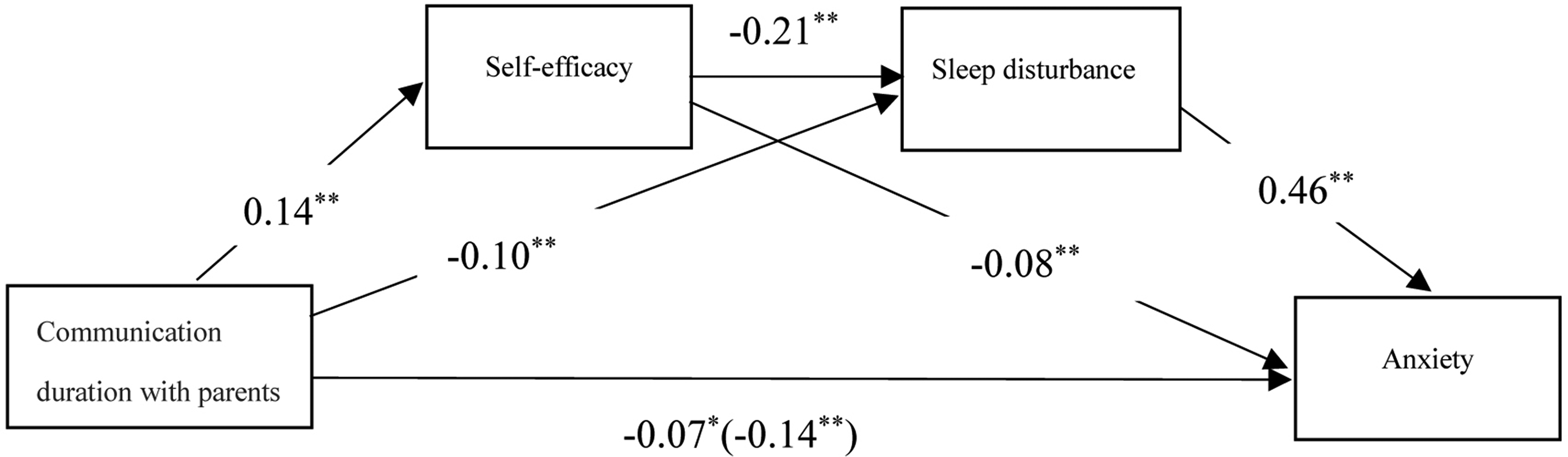
The chain mediation model of self-efficacy and sleep disturbance between the communication duration with parents and anxiety.
Chain-mediating effect values and 95% confidence intervals.
The moderation model
The results of the moderation analysis after controlling for the effect of living place and the highest level of education are depicted in Figure 5. In Model 3 (communication duration with parents → depression), the interaction of communication duration with parents and gender was insignificant (B = − 0.39, 95% CI: −1.40 to 0.63, p = .46), indicating that gender did not moderate the relationship between communication duration with parents and depression. Similarly, in Models 4, 5, 6, 8, 9, 10, and 11, the moderating effect of gender was not significant (B = 0.22, 95% CI: −0.66 to 1.10, p = .63; B = −1.77, 95% CI: −3.53 to −0.02, p = .05; B = −1.42, 95% CI: −3.01 to 0.17, p = .08; B = −0.07, 95% CI: −0.33 to 0.19, p = .60; B = −0.17, 95% CI: −0.68 to 0.35, p = .52; B = −0.06, 95%CI: −0.34 to 0.23, p = .69; B = −0.02, 95% CI: −0.08 to 0.03, p = .35; respectively). In Model 7 (sleep disturbance → depression), as shown in Figure 6, gender moderated the association between sleep disturbance and depression (B = 0.35, 95% CI: 0.06 to 0.64, p = .02 < .05; βmale = 1.69, t = 14.62, p < .01; βfemale = 2.04, t = 22.11, p < .01).

Analysis of moderating effects.
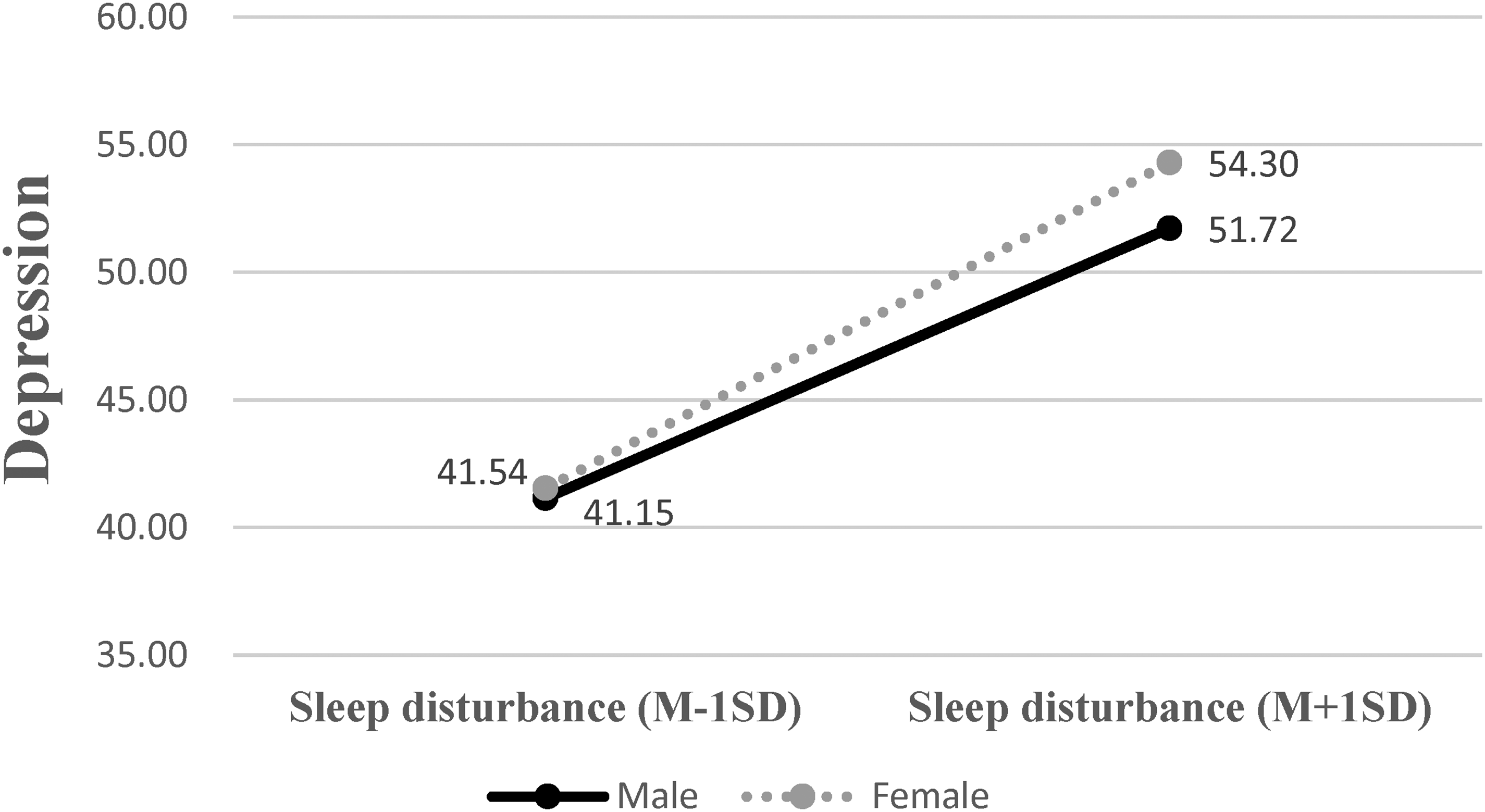
The interaction between sleep disturbance and gender depression.
Discussion
The results confirm the original hypothesis that a significant negative correlation exists between youth's daily communication time with parents and depression and anxiety, and self-efficacy and sleep quality play a chain-mediating role during COVID-19 isolation.
First, in the analysis of demographic variables, the self-efficacy scores of female youth were significantly lower than that of male youth. In contrast, the sleep disturbance of female youth was higher than that of males, suggesting that female sleep quality was significantly lower than that of males. In addition, the scores of depression and anxiety of female youth were significantly higher than that of male youth. These findings suggest that the mental health of female youth was affected considerably during the home-staying period of the epidemic, which is consistent with international studies (Santomauro et al., 2021; Simba & Ngcobo, 2020; Vuelvas-Olmos et al., 2022; Wenham et al., 2020). Studies have shown that females are more likely to be left with more caregiver and household responsibilities due to school closures or family illness (Santomauro et al., 2021). Female issues did not suddenly appear during this COVID-19 pandemic but have been or will be compounded by it. These issues have a direct and indirect influence on several aspects of female health, including putting them at a greater risk of COVID-19 infection, and worsening already existing diseases (Simba & Ngcobo, 2020). The self-efficacy of urban youth was higher than that of rural youth, suggesting that rural youth were more likely to feel powerless during the home-staying period. With the education level of youth as a sub-group, compared with middle school and college students, the high school students had lower self-efficacy and higher sleep disturbance, depression, and anxiety. The results suggest that high school students during the quarantine period were the most affected among adolescents; this phenomenon might be related to the pressure they face regarding the college entrance examination. According to the subgroup comparison of parent/youth daily communication time during the COVID-19 epidemic isolation, youth who communicated with their parents for less than 1 hour a day had significantly lower self-efficacy and significantly higher sleep disturbance, depression, and anxiety levels. These findings suggest that youth who communicate well with their parents have better mental health.
Second, correlation analysis found that daily youth/parent communication duration was associated with self-efficacy, sleep disturbance, depression, and anxiety. Consistent with other literature, family factors are associated with depression and anxiety (Guerra et al., 2018; Nasser & Overholser, 2005; Wang et al., 2020). Time spent communicating with parents daily correlated with self-efficacy and inversely correlated with sleep disturbance, depression, and anxiety.
Third, the chain mediation model analyzed the internal mechanisms of how the duration of daily youth/parent communication alleviated depression and anxiety. The duration of daily communication with parents indirectly affected depression and anxiety via the chain-mediating effect of self-efficacy → sleep disturbance. These findings suggest that the duration of daily communication with parents, self-efficacy, and sleep quality critically affected depression and anxiety levels among youth during the epidemic stay-at-home period. Similar to other literature (Duan et al., 2022; Levens et al., 2016; Olatunji et al., 2020; Torres & Solberg, 2001; Tsuno et al., 2005), self-efficacy and sleep disturbance are important mediating variables between family factors and negative emotions(Dong et al., 2022).
Fourth, gender moderated the associations among duration of daily youth/parent communication, self-efficacy, sleep disturbance, depression, and anxiety, which is consistent with existing literature (Diggs et al., 2017). Specifically, gender moderated only the associations between sleep disturbance and depression. This indicates that the pathway of the duration of daily youth/parent communication → self-efficacy → depression was different for male youth compared with their female counterparts, which is consistent with previous research (Monteiro et al., 2015; Wang et al., 2022; ZHU et al., 2021) and contributes to the gender difference in the model.
In summary, China implemented strict prevention and control measures in the early stages of the COVID-19 outbreak. The public stayed at home, controlling the spread of the epidemic and protecting public health (Chen et al., 2021; Wang, 2022). On the other hand, isolation measures hindered communication and interaction, resulting in alienation and loneliness (Ganesan et al., 2021; Lu et al., 2022). According to Erikson's psycho-social development theory, 14–18-year-olds are adolescents who experience conflict between self-identity and role disorder; 18–25-year-olds are young adults who experience conflict between intimacy and loneliness (Munley, 1975). In these stages, young people are in unstable states while shaping their personalities; they experience stress when facing significant emergencies such as the epidemic, which trigger potent psychological and behavioral responses. This study provides a potential direction to alleviate psychological distress for youth during COVID-19 isolation and in major health events in the future.
Implications for practice
This study confirms that when youth are isolated at home because of an epidemic, communicating with their parents is associated with improved self-efficacy and sleep quality and reduced levels of depression and anxiety. Youth who communicated with their parents for less than an hour a day reported significantly lower self-efficacy, significantly higher sleep disturbance, and substantially higher depression and anxiety than those who communicated more often. This finding suggests that schools encourage youth to maintain friendly communication with their parents during epidemics. Communication should last at least one hour a day, especially during the COVID-19 epidemic. For example, parents and children share their knowledge and feelings about the COVID-19 epidemic and express their views and suggestions on quarantine policies. Of course, it can be extended beyond the pandemic. For instance, parents and children can also communicate their daily life experiences, emotional feelings of the day, and opinions on current affairs and policies. These methods to promote parent-child communication can effectively create a warm and supportive family environment to help youth cope with anxiety and depression during family isolation.
Limitations and future directions
There are some limitations to this study. First, the youth from the four universities and three middle schools included in this study may not be representative of the general youth population; thus, these findings should be further validated with a larger sample comprising participants from diverse cultural backgrounds. Second, due to the cross-sectional nature of this study, causal relationships could not be established, and a longitudinal study should be conducted to replicate these findings. Third, this study only assessed the quantity of communication, but not the quality or type (e.g., positive or negative) of communication. Thus, future directions would like to further study the influence of the quality of communication between youth and parents on depression and anxiety. Fourthly, several potential confounding variables such as family environment, family income, family structure, parenting style, and family rituals (CHENG Zao-huo et al., 2016; Krauss et al., 2020; Wu Mingzheng et al., 2021), were not considered in the moderated mediation model due to the heavy scale burden; this may have impacted the association estimation. However, these factors should be analyzed in future research.
Conclusion
The mental health level of female youth and high school students was relatively low among youth who stayed at home during the epidemic. Youth who communicate with their parents for less than one hour have significantly lower self-efficacy, a substantially higher sleep index, and substantially more depression and anxiety. During the social isolation period, the duration of parent/youth communication directly affected depression and anxiety and indirectly affected depression and anxiety via the chain-mediating effect of self-efficacy and sleep disturbance. Gender moderates the relationships between sleep disturbance and depression.
Footnotes
Acknowledgments
We would like to express our sincere gratitude to the teachers who helped distribute questionnaires and collect data for this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and publication of this article. The study is supported by the 2020 Annual Research Project of the 13th Five-Year Plan of Education Science of Guangdong Province, Grant No. 2020GXJK054.