
Abstract
Migrant care workers (MCWs) are increasingly relied upon in contemporary care economies, yet they often labour under restrictive immigration regimes and precarious employment conditions. This article explores how non-EU MCWs employed under the Health and Care Worker visa scheme in the UK cope with these constraints in their everyday work. Drawing on qualitative interviews with 20 West African MCWs and informed by practice theory, the study conceptualises coping as an enacted social practice rather than an individualised response to stress. The analysis identifies three interrelated forms of coping: collective and relational practices, hybridised caregiving practices and tactical acts of micro-resistance. These practices, we argue, illuminate how MCWs navigate legal dependency, workplace surveillance and devalued care labour while exercising limited but meaningful forms of agency. The article extends practice theory to migrant labour and coping literature, with implications for practice further highlighted.
Introduction
A growing demand for care services, driven by the dual pressures of population ageing and chronic understaffing, has intensified reliance on migrant care workers (MCWs) in many developed countries (Liao et al., 2024). In the UK, this dependence has become especially pronounced in the wake of Brexit, which reduced the availability of European Union (EU) labour, prompting the government to introduce the Health and Care Worker (HCW) visa scheme to fill widening labour gaps (Gov.UK, 2021). While the scheme increased the presence of non-EU workers in frontline care roles, it has also drawn criticism for producing new vulnerabilities including heightened exposure to legal precarity and exploitation (Goel and Penman, 2015; The Guardian, 2022a). Accounts of long working hours, racialised and gendered labour hierarchies, inadequate organisational support, and the psychological toll of intimate, embodied care work have emerged (Amrith, 2023; Boese et al., 2013; Omeri and Atkins, 2002; Wu et al., 2022). These challenges raise an important question to which we ask: How do recently arrived non-EU MCWs in the UK enact coping in their everyday work?
In exploring the coping of MCWs in the UK, we turn to practice theory as a lens to understand the ways through which coping is enacted. Coping has fundamentally been conceptualised within psychological paradigms as a cognitive and behavioural strategy to manage stress (Duhachek, 2005; Kashdan et al., 2006; Lazarus and Folkman, 1984, 1991). Within this tradition, individual traits, personality factors or discrete emotional responses are foregrounded. Yet, there are also suggestions that coping is not only about reducing negative emotions to manage stress but also includes cultivating positive states (Folkman and Moskowitz, 2000) which open doors to seeing coping in broader, more socially embedded ways (Bruce and Banister, 2019). In the case of migrant labour where structural inequalities shape the terrain of adaptation (Anderson, 2010; Berry, 1997; Boese et al., 2013), it is important to contextualise the material, social and institutional conditions in which coping unfolds as well as cast light on the relational, embodied and situated nature of how it is enacted.
Recent scholarship has begun to point to the social embeddedness of coping, highlighting the role of peer support, informal networks and collective strategies in enabling migrant workers to survive particularly precarious conditions (Eyong, 2017; Liao et al., 2024; McFadden et al., 2021; Sarpong et al., 2022). We build on these views to argue that coping must be understood not merely as a psychological or individual process, but as a socially organised and materially mediated practice. That is, coping unfolds through the patterned, collective practices that workers draw on in response to constraint. Thus, in adopting practice theory (Reckwitz, 2002; Schatzki, 1996, 2001), we reframe coping as a form of socially choreographed action: bundles of ‘doings and sayings’ shaped by competences, meanings, materialities and norms (Shove et al., 2012). This perspective enables us to view coping not merely as response to stress, but as a performative and situated mode of agency that reflects how MCWs engage with the constraints of their everyday work environments.
We develop our contribution based on lived experiences as narrated by 20 migrant care workers of West African origin. Placing this discrete group of care workers as a unit of research within a larger non-EU migrant health workers research study, we give voice to a growing but diverse group of migrants with different identities but sharing similar socioeconomic experiences, colonial histories and religious syncretism (Eyong, 2017; Sarpong et al., 2022, 2024), with potential to influence their patterns of situated migration narratives, work actions and practices, as well as shape the tactics they may employ to survive (De Certeau, 1984) in the ‘new’ workplace. By extending practice theory (e.g. Pais Zozimo et al., 2023; Schatzki, 1996; Shove et al., 2012) to the migrant labour and coping literature, our study makes three contributions. First, we reconceptualise coping in migrant care work as bundled social practices and materially situated performances, not merely individual psychological management. Second, we emphasise agency in coping, showing how MCWs not only endure challenges but actively rework and, at times, quietly resist the structural constraints embedded in care work. Third, we offer insights for practice. In so doing, we respond to calls for more grounded, relational and embodied understandings of how migrant workers ‘get in’ and ‘get on’ in the labour markets of host societies (Anderson, 2010; Rolfe et al., 2019). Our approach also challenges reductive portrayals of MCWs as passive victims, instead showing how they improvise, negotiate and assert forms of agency through everyday practices. In theorising coping as materially embedded, socially organised and temporally unfolding, we offer a more nuanced account of migrant labour agency.
Coping among migrant workers: From individual adaptation to collective practice
The concept of coping has historically been associated with individual psychological adjustment to stress. Rooted in psychoanalytic and stress-response traditions, early theorists such as Freud (1926) conceptualised coping through defence mechanisms, while Lazarus and Folkman (1984) later defined it as cognitive and behavioural efforts to manage situations appraised as overwhelming. This dominant framing positioned coping as an individualised, cognitive response to stressors, thus arising from an individual’s appraisal of a situation as threatening and the efforts mobilised in response (Eib and Bernhard-Oettel, 2024). These are often further organised into binary categories such as problem-focused versus emotion-focused or approach versus avoidance (Duhachek, 2005; Kashdan et al., 2006). Nevertheless, while such frameworks have their utility, they often tend to decontextualise coping from the structural and material conditions in which it occurs.
Recognising such limitations, recent scholarship has expanded the concept to encompass socially and institutionally embedded responses, including the mobilisation of social support and communal resources (Akpan-Idiok et al., 2020; Gillen et al., 2022; McFadden et al., 2021). This perspective is particularly salient for understanding coping among migrant workers, whose experiences of work are shaped by immigration regimes, marginalised labour markets and multi-sited vulnerabilities (Goel and Penman, 2015; Wu et al., 2022). Within this migrant labour scholarship, a growing body of work has examined how migrant workers cope under structurally adverse conditions (e.g. Ahmed, 2010; Ho et al., 2022; Liao et al., 2024; Zainal and Barlas, 2022). Early contributions, notably the acculturative stress literature (Berry, 1997), highlight how migrant worker adaptation is influenced by factors such as country of origin and pre-migration socioeconomic position (Liem et al., 2020). However, research on low-waged migrant workers increasingly demonstrates that coping cannot be understood without reference to precarious legal status, exploitative employment relations and racialised hierarchies that shape everyday working lives (Wu et al., 2022; Zou et al., 2023).
Taken together, these studies suggest that coping among migrant workers is fundamentally shaped by legal precarity and labour market segmentation, which generate persistent uncertainty and constraint (Goel and Penman, 2015; Wu et al., 2022). At the same time, coping frequently assumes collective and relational forms, enacted through co-ethnic networks, religious communities and other informal social infrastructures that compensate for the absence or failure of formal support mechanisms (Eyong, 2017; Sarpong et al., 2022). Beyond endurance, coping also operates as a form of constrained agency, encompassing adaptive reworking and subtle practices of resistance (Katz, 2004; Krings et al., 2011; Overgaard and Høgedahl, 2024).
This body of work marks a significant shift in how coping is theorised within migrant labour studies. Rather than treating coping as a static, individual-level response to stress, these accounts situate it within broader regimes of structural constraint, workplace power relations and everyday agency. For example, Krings et al. (2011) demonstrate how immigration and labour market regulations pattern migrant workers’ responses to insecurity by restricting access to rights, mobility and collective representation, often channelling coping into informal and individualised strategies. Similarly, Overgaard and Høgedahl (2024) show how employer practices actively fragment migrant collectivism, suppressing worker voice and redirecting coping into dispersed and covert forms. Extending these insights, Miles et al. (2024) illustrate how UK-based migrant care workers did not simply endure post-COVID precarity but actively reworked and resisted the conditions shaping their labour through everyday practices that blurred the boundaries between survival, adaptation and dissent. Although such studies are not always framed explicitly as coping research, they implicitly conceptualise coping as an enacted, relational and material practice through which migrant workers navigate hostile labour regimes. Coping, therefore, emerges not merely as a mechanism of endurance, but as a dynamic site of struggle, adaptation and limited autonomy (Miles et al., 2024).
Building on these insights, this study adopts a practice theory perspective grounded in Schatzki’s (2001) conceptualisation of social practices as ‘temporally unfolding and spatially dispersed nexuses of doings and sayings’. From this standpoint, coping among migrant care workers (MCWs) is understood not as an internalised response to stress, but as something enacted through social relations, material engagements and spatial arrangements. This perspective foregrounds the mundane, everyday tactics (De Certeau, 1984) through which migrant workers navigate structurally constrained work environments, allowing coping to be examined as a relational and materially situated accomplishment rather than solely an outcome of institutional forces. Such an approach is particularly well suited to the study of migrant labour, as many migrant workers are excluded from formal mechanisms of representation and collective voice, yet continue to enact coping through adaptive, resistant and solidaristic practices. For example, Hau and Borello (2024) demonstrate how MCWs sustain weak and fragmented forms of collectivism through digital communication and informal exchanges, even within highly individualised and dispersed work settings. These practices blur the boundary between individual and collective action, revealing how solidarity is enacted in partial and contingent ways.
By drawing on the recent turn to practice in social theory, this study contributes to migrant labour scholarship by conceptualising coping as a context-sensitive, materially mediated and socially embedded practice. This framing provides a more nuanced account of how migrant workers navigate the environments in which they labour and the limited yet meaningful forms of agency they enact under conditions of precarity (Umeh et al., 2023).
A practice theory perspective on coping among MCWs
Practice theory has emerged as a valuable lens to examining the relational and processual nature of social life (Reckwitz, 2002; Schatzki, 1996; Shove, 2007). Rather than focusing solely on individual behaviours or macro social structures, practice theory conceives the social world as constituted by practices (Schatzki, 1996, 2001), offering a framework that situates actions within broader fields of meaning, competence and material engagement (Shove et al., 2012). As Barnes (2005) emphasises, practice is not reducible to individual conduct but rather comprises shared, routinised and relational behaviours, produced through the reciprocal shaping of agency and structure (Giddens, 1984). In an empirical articulation of what constitutes practices, Schatzki (1996) conceptualised practices as the temporally unfolding and spatially dispersed nexus of doings and sayings that permeates the unfolding of everyday social life. This is organised by three interlacing elements of practical understanding (competence), teleoaffectivity (goals, emotions) and normativity (rules and expectations). Shove et al. (2012) further disaggregated practices into three core components of materials, competences and meanings which provide the scaffolding through which practices are formed, reproduced and transformed.
Individuals enact these elements through performances that are socially recognised and sustained within communities of practice (Giustini, 2023). In the context of migrant care work, materials, both transitive and epistemic (Knorr-Cetina, 2001), may include work visas, qualifications and certificates, regulatory frameworks and care infrastructures. Meanings encompass the symbolic, emotional and social significances attached to participation in work, while competence refers to what Shove et al. (2012) describe as the multiple forms of understanding and knowledgeability: that is, the know-how and insight required to excel in the performance of the practice. These may include embodied competences, intelligibility, skills, expertise and even routine caring tasks. In this framing, practices are neither static nor institutionally fixed. Rather, they unfold through intersubjective performances that are at once responsive and productive, and inflected by actors’ values, motivations and material constraints (Sarpong et al., 2022; Shove, 2007).
This performative dimension is particularly salient in migrant care work where coping behaviours are often invisible yet remain central to how work is experienced and endured. Migrant workers’ coping emerges through practices that are materially embedded, emotionally charged and normatively governed, residing not only in what individuals do but also in how they make sense of what they do under structured conditions. Situating practices therefore within the context of migrants’ coping pushes scholars to consider coping as a process of making life liveable under constraint, rather than escaping or resolving it. It foregrounds agency not as resistance alone, but as a capacity to sustain, adjust and subtly reshape conditions through everyday acts. This aligns with the concept of ‘quiet encroachment’ (Bayat, 2010) and ‘infra-political acts’ (Scott, 1990), which have been used to describe how marginalised populations navigate structures of domination through routine practices that fall under the radar of formal politics. This line of thinking likewise aligns with scholarship that challenges the individualising tendencies in dominant migration and labour discourses. For instance, Anderson (2010) critiques the ‘migrant as victim’ trope, arguing instead for an approach attentive to how migrant subjectivities and actions are shaped by, but not reducible to, structural conditions. Similarly, Waite and Lewis (2017), through the concept of ‘embodied precarity’, highlight how insecurity is lived and managed through the body and in relation to others, opening space to understand coping as relational, teleoaffective and situated.
Our practice theory perspective on coping thus offers a grounded and sociologically informed lens for understanding how MCWs circumnavigate everyday structural pressures. Rather than framing coping as a conscious, mental response to stress, a practice approach situates coping within routine, socially patterned and materially mediated practices (Schatzki, 2001; Nicolini, 2012). It emphasises what people do, and how they do it, in specific contexts, drawing attention to the ways in which coping is enacted, reproduced and negotiated through habitual performances embedded in work and life. In sum, a practice approach allows for a more nuanced understanding of coping as it occurs in situ within the intersections of migration, care work and precarity. It shifts focus from what migrants think about stress, to what they do in response to it, and how such practices are shaped by the institutions, infrastructures and histories in which they are embedded. As this article explores, these everyday practices are neither wholly adaptive nor wholly resistant but are complex forms of social navigation that sustain migrant care workers.
Method
Research context
More than 11 million people, constituting 18% of the UK population, are aged 65 and over, and are either currently in care or will require health and social care support in the next decade (Office for National Statistics [ONS], 2025). In response to growing demand, estimates indicate that an additional 480,000 roles in the care sector will be needed by 2035 (Kilkey, 2024). However, these workforce requirements emerge against a backdrop of persistent staffing shortages (House of Commons, 2023), further exacerbated by a decline in the availability of EU migrant care workers post Brexit (Migration Advisory Committee, 2022). To mitigate these shortages, the UK government introduced the Health and Care Worker (HCW) visa scheme in June 2021. Designed to attract overseas labour, the policy effectively binds migrant workers to a UK Home Office approved employer, for whom they must undertake a specified eligible care role with said employer, and can only switch jobs where another approved employer is willing to sponsor the visa holder for a similar role. Additionally, visa holders and their dependants, if any, are not eligible to claim any public funds or state benefits, and must ensure to work only in the approved sponsored role. Notwithstanding these caveats, the HCW scheme saw considerable uptake, particularly among non-EU migrants.
While initially welcomed, the sustained influx of MCWs provoked concern with reports of widespread exploitation, including incidences of rogue employers taking advantage of workers’ dependent immigration statuses (The Guardian, 2022b). Further research also points to skill mismatches and the psychological strains of embodied care work among visa holders (Turnpenny and Hussein, 2022). These vulnerabilities intersect with broader structures of racialisation, gendering and class, which often frame migrant care workers as disposable labour and further position them to be disproportionately overworked, underpaid and tightly regulated by punitive immigration and managerial controls (Amrith, 2023; Nasol and Francisco-Menchavez, 2021; Ogawa, 2024; Turnpenny and Hussein, 2022). Acknowledging the sector’s exposure to poor working conditions, including risks of modern slavery, the Government has since signalled the termination of the HCW visa route for overseas carers (UK Parliament, 2025). Given the above, there is a need to explore the lived realities of those who perform this labour, and whose experiences offer a crucial lens through which to examine broader questions of coping in precarious work. In this sense, the study of MCWs offers important insights into how coping is enacted in UK care work.
Participants
A flurry of reports highlighting the challenges of the UK care workers visa scheme (e.g. Holland, 2023; The Guardian, 2022a), and the paucity of research exploring the lives of migrant care workers in the UK (Ho and Chiang, 2015; Turnpenny and Hussein, 2022), triggered our interest to conduct our study. Our methodological choices were guided by our research question: How do recently arrived non-EU migrant care workers (MCWs) in the UK enact coping in their everyday work? To address these questions, we adopted a qualitative design grounded in practice theory, which views coping not as a static trait or psychological disposition but as an unfolding nexus of doings, sayings and material engagements (Schatzki, 2001; Shove et al., 2012). We thus adopted an abductive approach to qualitative enquiry, informed by discursive and interpretive theorisation processes (Rinehart, 2020), and focusing on health and social care migrant workers from West Africa with residency granted under the HCW visa programme. We conducted our study in and around the city of Leicester, in the East Midlands area of England.
We devised a robust theoretical sampling strategy (Glaser and Strauss, 2017) to select our research participants based on their capacity to illuminate the phenomenon under study, which is coping as a practice. Given our focus on how coping unfolds within the constraints of an often precarious migrant labour, we purposively selected non-EU MCWs employed under the UK’s Health and Care Worker visa scheme, a group that embodies the structural vulnerabilities central to our enquiry. This approach enabled us to engage participants whose lived experiences offered the most conceptual insight into how agency is enacted, negotiated and constrained through everyday practices of coping. Similarly, our focus specifically on West African MCWs stems from the fact that this group remains underrepresented in the literature (Eyong, 2017; Sarpong et al., 2022; Sarpong et al., 2024), yet are heavily involved in the UK care economy, particularly in the aftermath of Brexit which saw many European nationals leave (Sarpong et al., 2022). Thus, for our sampling criteria, participants first needed to be MCWs having arrived in the UK through the HCW visa programme. Second, they needed to be non-EU nationals. Third, they had to be in active employment as care workers for at least six months. We relied on a health care agency providing work to migrant care workers and snowballed into networks of care communities in Leicester to reach over 50 of this ‘hidden’ migrant population (Robson, 2011). From this initial sample, 20 MCWs meeting our sampling criteria agreed to participate in our study.
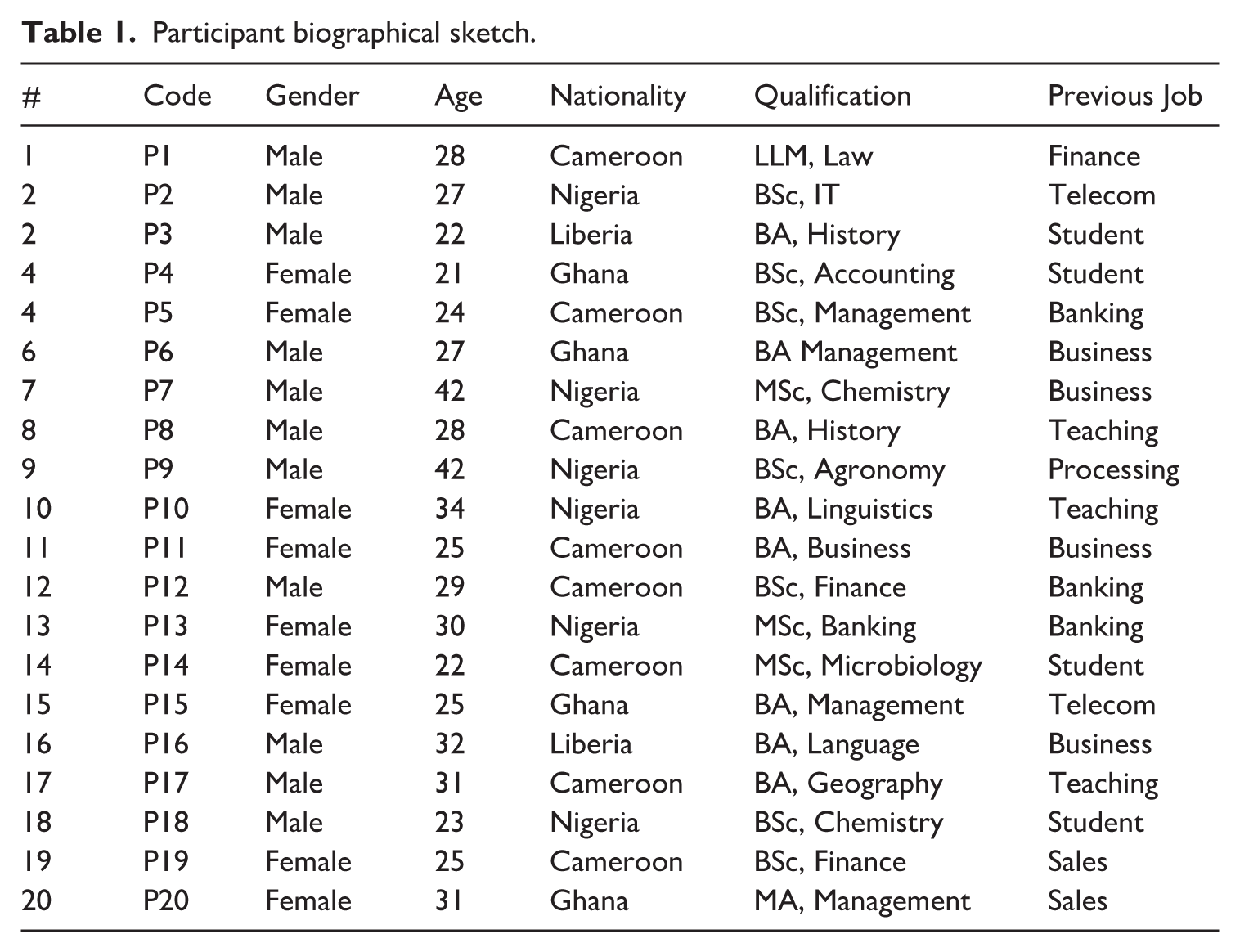
Data were collected over a period of 12 months, starting from December 2022 to November 2023 and deployed semi-structured interviews (Braun et al., 2017; Gray et al., 2020). Each interview lasted approximately 90 minutes, and all were digitally recorded and instantaneously transcribed using Microsoft Teams. Prior to data collection, each prospective participant received a detailed information sheet describing the study aims, the procedures for anonymising and securely storing data, their rights to partake or withdraw from the study, issues on protecting anonymity, and the ways in which interview material would be used for research purposes. Signed consent forms were also obtained from each participant prior to the interview. All interviews were conducted by the same researcher to ensure consistency in rapport-building, interviewing style and probing. The interview guide remained unchanged throughout, although later interviews benefitted from the researcher’s deepened familiarity with participants’ contexts, in line with iterative qualitative research (Miles and Huberman, 1994). No follow-up interviews were conducted. However, participants were invited to clarify initial statements during transcription checking. The interview guide (Appendix A) was theoretically informed by practice theory with questions exploring materiality (tools, artefacts, technologies used to cope), spatial affordances (how workplace environment enabled or constrained coping practices) and tactics used in coping. This structure reflects Schatzki’s (1996) and Shove et al.’s (2012) components of practice including materials, competences, meanings and De Certeau’s (1984) theorisation of everyday tactics. Particular attention was thus paid to the material and spatial conditions of work including the tools participants mobilise, the ways care home environments afford or restrict agency, and the tactics workers deploy to cope with their everyday work. Interviews opened with a narrative prompt (‘Describe a typical day at work’), to elicit a temporal map of daily activities. Subsequent probing questions explored specific scenarios (e.g. ‘What do you do when work gets emotionally difficult?’ ‘Have you found ways of coping with difficult clients or long shifts?’ ‘What helps you carry on?’), enabling a deeper examination of situated coping tactics and the embodied experience of care labour. This design provided a consistent structure while allowing participants to foreground the practices most salient to their lived realities. We applied a coding protocol identifying participants using participant number as P1 to P20, to preserve anonymity. Our participants originated from the West African countries of Cameroon, Ghana, Nigeria, Liberia and Sierra Leone. All participants reported having studied at university level with degrees in various fields, as presented in Table 1.
Participant biographical sketch.
Data analysis
Data analysis followed three main steps, in a non-linear manner. Mostly, it involved constant reflective actions of forward and backwards reviewing and rechecking of processes. First, open coding was conducted using an inductive approach consistent with the exploratory nature of the study (Glaser and Strauss, 2017). At this stage, we coded for concrete actions, interactions and material engagements through which MCWs enacted coping in their everyday work. Particular attention was paid to participants’ accounts of coordinated coping practices and meaning-making processes across different phases of their migration and work trajectories. Frequently recurring phrases drawn directly from participants’ narratives such as ‘connecting with people from my community’, ‘I took the advice of a colleague’, ‘my study helps me to get some time away from care work’, ‘I got a second job’ and ‘I cannot wait to leave’ were treated as analytically meaningful power phrases (Pratt, 2009) that captured how coping was enacted in practice (Boje, 2018). In line with practice-theoretical sensibilities, this initial coding focused on mapping doings and sayings, as well as participants’ identities, work environments and expressions of coping (Glaser, 1996).
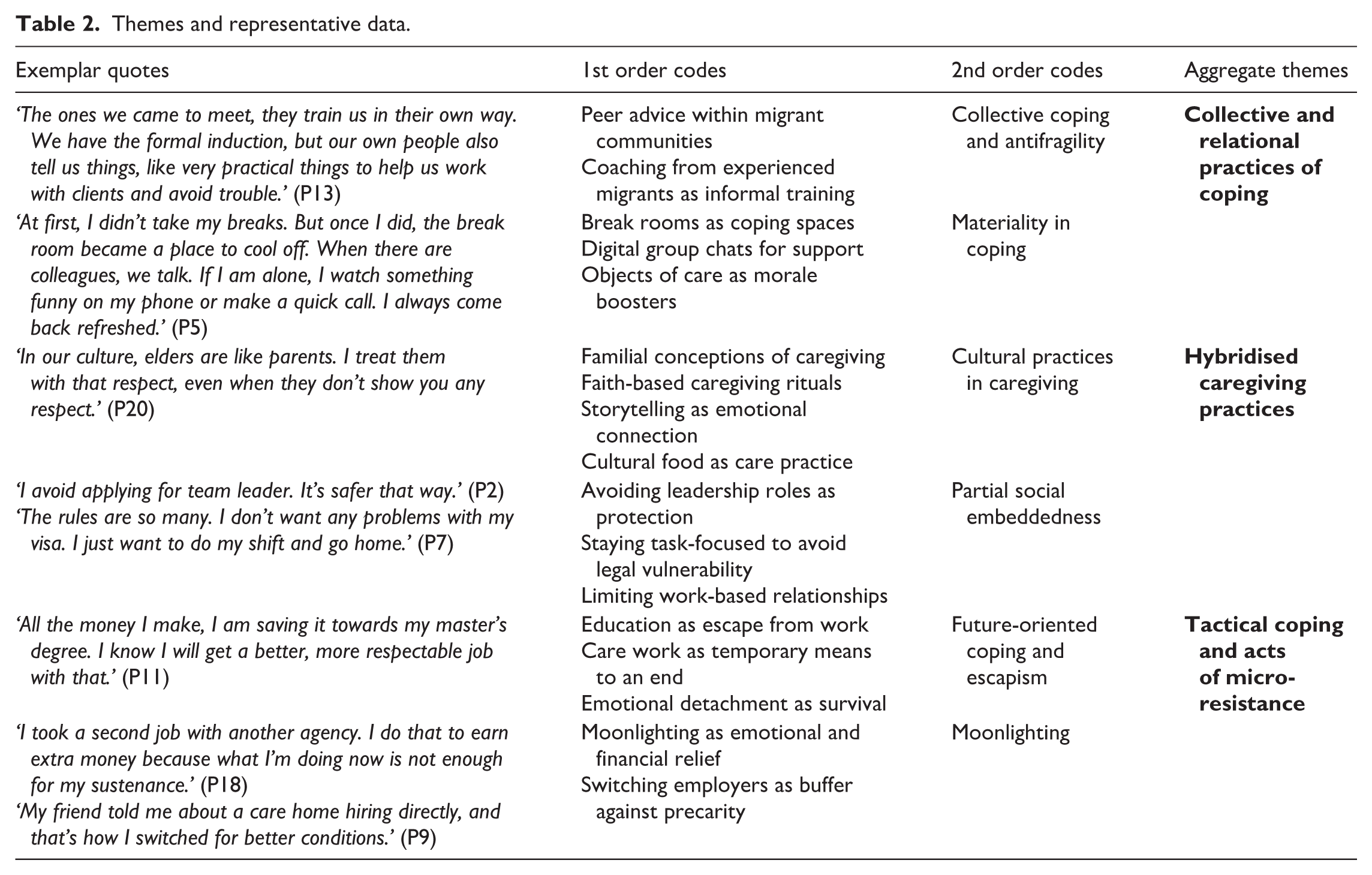
Second, axial coding was used to refine first-order codes into more abstract second-order categories (Miles and Huberman, 1994; Pratt, 2023). Through constant comparison (Corbin and Strauss, 2008), we clustered analytically similar codes to identify patterned forms of coping-as-practice, including relational, material and tactical modes of coping. Engagement with the extant literature on coping and migrant labour at this stage supported theoretical sensitivity, enabling us to situate participants’ practices within broader scholarly debates while remaining grounded in the empirical data. Finally, theoretical integration involved linking narrative codes and second-order categories into aggregate themes that captured how coping is enacted as a relational, materially mediated and social practice. Thus, stage resulted in three interrelated aggregate themes: (1) collective and relational practices of coping, (2) hybridised caregiving practices and (3) tactical coping and acts of micro-resistance. Together, these themes explain how coping among MCWs is accomplished through patterned practices embedded in everyday care work.
To enhance the credibility and rigour of our analysis, we conducted two peer-debriefing sessions with two qualitative researchers who possess substantial expertise in research on migrant and ethnic minority work, but who were not involved in the present study. These researchers functioned as ‘disinterested peers’ (Klein and Amis, 2021; Torbor et al., 2024), providing an independent and critical assessment of our analytical framework. Their role as methodological outsiders enabled them to interrogate our interpretive processes, challenge emerging categories and identify potential analytical blind spots. These peer-debriefing engagements also facilitated reflexive dialogue around our interpretations and sense-making processes, thereby strengthening analytic transparency and robustness (Gioia et al., 2012). They further prompted closer scrutiny of the alignment between empirical evidence and our theoretical and conceptual claims, contributing to the abductive refinement of our analysis (Timmermans and Tavory, 2012). We then refined the outcomes, re-evaluated the relevance of our theorisation and presented our findings to a select corpus of our interviewees for confirmation and authentication. Table 2 is a summary of the emerging dimensions and themes highlighting the practices of coping and representative data. Next, we present the fine details of our research findings.
Themes and representative data.
Findings
We interpret the coping of MCWs through the lens of practice theory (Schatzki, 1996; Shove et al., 2012), which emphasises how social practices are constituted through the interaction of meanings, competences and materialities. The three core themes we develop – Collective and relational practices of coping, Hybridised caregiving practices and Tactical coping and acts of micro-resistance – represent distinct but interrelated enactments of coping that emerge through this nexus of doings and sayings. They demonstrate how MCWs’ coping is contextually performed, materially supported and socially situated. Each of these aggregate themes is further discussed, using data codes and quotes to support explanations (Pratt, 2009).
Collective and relational practices of coping
Collective coping and antifragility
In examining how coping is enacted in care work by migrant care workers, the findings emphasised the socio-material dimensions that emerge through interactions and collaboration among workers, clients and managers. MCWs rely on shared practices, predominantly informal support networks, collective problem-solving and emotional exchanges to navigate workplace challenges. The creation of informal migrant worker groups to share advice on handling difficult patients or leaning on each other during emotionally taxing situations created a sense of collective resilience. Analysis showed considerable individual antifragility among MCWs emerging from such collective resilience. Narratives revealed emotional sharing within migrant groups as fostering collective coping, which becomes crucial for managing stressors and failures at work. By open exchange of feelings, thoughts, and experiences related to their work and personal lives, MCWs are able to not only cope with workplace challenges but also thrive and grow stronger under pressure. One participant’s experience, echoing the sentiments of others, is highlighted below: Connecting with people from my home community here has made me feel more, to an extent, that sense of loneliness – greatly reduced. I found people from my country and most of them also work in care. They shared their experiences with me, and it really helped me to manage my own work. Even before I started with my training, I knew a lot about the basic routines involved in care work and how to manage the daily challenges. (P4)
Coping is deeply embodied and involves managing physical and emotional labour (Hochschild, 2019). MCWs therefore rely on bodily routines, emotional detachment or empathetic engagement to manage challenges. Participants revealed that not only were ingroup communities of migrants relevant to physical coping, but that individuals rely on such informal support – even if they came from people in other workplaces – to cope emotionally as well as physically. Some interviewees told of instances where they were advised by more experienced migrant colleagues in their communities to consciously regulate their tone, gestures or physical presence to maintain professionalism and emotional composure under stress: I was advised by someone in my community who has done this [job] for years, to just present a happy and confident personality even when clients disrespect me. On taking that advice, I find it makes a difficult situation look normal. It has helped me to avoid a lot of trouble since I came. (P13)
Another pointed out: There’s a WhatsApp group that I was encouraged to join. They give tips on how to manage at work. For instance, how to deal with racial abuse and the rest. If something like that happens, there’s someone I can call or text for advice. They also explain some of the situations to us and tell us to process it as ignorance and just get on with the job if it’s not too serious. There’s a lot of things that group has taught me which I wouldn’t have known on my own. (P15)
Similar accounts highlighted the role of peer-led support networks, such as WhatsApp groups to prepare MCWs for the emotional demands of their roles. The group functioned not only as a space for the exchange of practical strategies such as responding to racial abuse, but also as a mechanism for normalising and reframing emotionally charged encounters. By encouraging members to interpret certain behaviours as ‘ignorance’ rather than intentional hostility, the group promoted cognitive reframing for managing the strain of emotional labour. This prior socialisation into the emotional realities of care work appears to have cushioned workers against some of the psychological shocks of the job. Exposure to shared narratives, anticipatory advice and accessible peer mentorship cultivated an anticipatory emotional preparedness. In this way, the group acted as an informal site of workplace learning, transmitting tacit knowledge about the other side of care work that might otherwise remain unspoken in formal training.
Materiality in coping
The material effects at work also enabled coping practices among MCWs. Objects, spaces and physical resources emerged as vital components in MCWs’ ability to cope. Participants described using shared spaces, and even mundane items as anchors for coping and connection. One participant stressed how their decision to use shared spaces brought about a sense of relief: I was quite adamant to take breaks because I didn’t want to come across as lazy. But once I took the advice of a colleague and started using the break room, I realised I always returned to my duties in a better state. I meet other staff there, some migrant workers like me and we just sit down and have a cup of tea or talk about the day. It’s something that keeps us all going. (P17)
Break rooms, as mentioned by this participant, become more than a physical location but relational hubs where emotional support and camaraderie are cultivated. Many participants agreed that these spaces provided them with opportunities to connect, share experiences and engage in collective problem-solving on a daily basis. In this regard, such material spaces become enablers for collective practices that ease stress and foster emotional bonds. In a likewise manner, small, intentional acts from managers and clients were seen as reinforcing a sense of being part of the caring community. A participant noted how such expressions helped them to cope by feeling appreciated: A client once left a note saying – thank you, you’re doing great – . . . My supervisor always tells me to not forget to take my breaks. For me, it shows that someone appreciates what I am doing. It makes a big difference because even when you are down, you remember that your efforts are appreciated, and you get on. (P19)
The practice of leaving notes or reminders to take breaks then becomes a conduit through which MCWs cope, as these visible gestures become imbued with symbolic value, operating as tangible affirmations of worth and care. In this way, the material artefacts of work life become active mediators in the coping process MCWs experience and endure in their roles. In these shared spaces, material tokens become part of a collective coping repertoire. They mark the workplace as a site where support is not only spoken but made visible. For MCWs, this material and spatial embedding of care reinforces bonds with others, creating a quiet but powerful infrastructure of mutual resilience. It is through such everyday exchanges that the demands of care work become more bearable, and the community of workers more tightly knit.
Hybridised caregiving practices
Cultural practices in caregiving
Our analysis revealed MCWs as incorporating elements of their cultural heritage into coping practices, blending these with organisational norms to create hybrid strategies. This cultural hybridity manifested in approaches to caregiving, emotional regulation or communication. Many interviewees alluded to using culturally specific caregiving rituals, drawing on familial notions of caregiving, in addition to what they had been ‘trained’ to do. For instance, a participant explained how they viewed care work from a humanity perspective and drew on their experience of looking after parents and grandparents in their home countries as rationale to get involved: For me, I will say it goes back home, because growing up with my grandparents, I used to look after my granddad, my grandma, and especially when he had an accident and was using the wheelchair, I used to help with giving him a shower. On the actual job of caring, it was not strange for me because we in Africa, you are brought up to care for your aged relatives. For the work, I consider factors like, what if this person was a family person? How will I look after them? Even though promoting independence is a big thing here, I also always offer help in any way I can without compromising on the person’s independence. (P20)
Another agreed with the above, saying: Care is about being human and helping and thinking with empathy, knowing that you could be in his/her position. I once looked after a client who shared [a] similar background as me. She was very happy that I could communicate with her in her native language. She found so much comfort in that, as her English was not very good. (P17)
Thus, for many participants, caregiving is not merely a task dictated by organisational policies or professional training, but a deeply ingrained value shaped by their cultural upbringing. This perspective often led them to adopt a more personalised and empathetic approach, which sometimes diverged from the standardised norms they were taught during training. Participants highlighted how cultural values like respect for elders, communal responsibility and emotional attuneness influenced their interactions with clients. They blended these values with organisational expectations, creating a hybrid model that both fulfilled professional standards and resonated with their cultural identities. This dual approach not only enhanced the quality of care but also allowed MCWs to remain connected to their cultural roots while navigating the professional demands of the care sector.
Partial social embeddedness
Partial social embeddedness was identified as a common coping strategy by MCWs. By partial social embeddedness, we mean the engagement with certain presumed beneficial practices by MCWs while preserving distinct cultural and personal practices. In our interviews, participants narrated instances where they took steps to form bonds with colleagues and supervisors, gaining access to vital support networks that help them manage the demands of their roles, but signalled an unwillingness to take greater responsibility or leading roles such as team leader or supervisor at their places of work now and in the future. According to participants, as their right to live and work in the UK was dependent on the continuous sponsorship of their employer, they believed a way of coping was to distance themselves from higher roles, and instead focus on accomplishing the very basic function of providing care service and support roles. As stated by one participant: All I want to do is just be here and do my job. Afterall the company has helped me to get my visa. If I take up a leadership role, it will not help me. It might get me into trouble, so I am not keen to take up any role. (P2)
For this participant and many others, inadequate knowledge about the complex legalities involved in care work was a key precursor to their coping playing out as not fully embedding themselves in their workplace. In sum, they ‘just want to do [their] work and go home without any problems’ (P12). This relative deficit in their situated social capital in a new country makes greater embeddedness less appealing. Behind partial embeddedness was caution against the risk of MCWs exposing themselves to litigation or blame if they embedded themselves fully in their care work, thus having to take responsibility should any aspect of their work go wrong.
The laws are rather many and they are always changing – health and safety, safeguarding, confidentiality, human rights, language restriction and so on. If I become team leader and something happens, I might lose my right to work. (P2)
Despite the very acute shortage in healthcare workers, as already elucidated, data analysis revealed that MCWs work in a tense, challenging and power asymmetric context. Their livelihood, visa status,and right to remain in the UK are contingent on the decisions of managers and owners of sponsoring healthcare organisations. This dynamic significantly limits their bargaining power, often compelling them to adopt a strategy of compliance to traverse the period of employment under their sponsor. Consequently, the interpersonal relationships between MCWs and managers are predominantly functional and restricted to task accomplishment. In this context, alongside the coping strategies previously outlined, the pronounced power asymmetry fosters a principle of unquestioning obedience in their interactions with managers.
Tactical coping and acts of micro-resistance
Future-oriented coping
A significant cluster of coping articulated by participants centred on future-oriented practices which were essentially tactical engagements that allowed them to endure present constraints while investing in alternative futures. These practices involved actors adaptively reshaping their pathways within existing structures rather than directly resisting them (Katz, 2004). In our study, future-oriented coping emerged through self-investment in education, upskilling and aspirational reimagining of life beyond care work. Participants frequently framed care work not as a long-term career but as a transitional phase to something ‘better’. For some, this meant pursuing formal education with the intention of pivoting into new occupational fields. One participant explained: I started a professional program in IT, that is, in basic coding sometime in September. It is difficult because I did not know much about IT. So, I can say, my study kind of helps me to get some time away from care work while preparing for the future. (P18)
For most participants, the decision to retrain was not simply about disliking care work. Rather, it reflected a deliberate, long-term plan to buffer or hedge against employment precarity in migrant care work. Many noted that UK visa policies were ever changing, and that sponsorship renewal was often at the discretion of employers, leaving workers vulnerable to sudden termination and legal insecurity. In this context, retraining in other areas served as both a coping mechanism and a form of futureproofing.
I am taking a degree programme in management online. Hopefully, I can secure another role with better pay when my visa becomes open. Sometimes, the employers will tell you they can’t sponsor you again. I have seen it happen to people, and they become stranded because you have a few months to look for another sponsor or you go home. So, in this case, it is better to have something else that can also help you to get a sponsor if something like that happens to you. (P5)
While some acknowledged that care work in the UK offered comparatively higher wages than their previous jobs in their countries of origin, they also pointed to the lack of recognition and the social devaluation of care work as drivers of their desire to transition out. These experiences produced a dual consciousness where participants expressed gratitude for current employment and income, but dissatisfaction with the social and professional status it conferred. By holding onto care work as a means to a better end, participants demonstrated that coping is not merely about survival but also about self-empowerment and quiet refusal to stay in an environment where they endured daily indignities of their labour. One participant recounted: In some homes, we are refused to use the toilet or even put on the kettle to make a cup of tea when the weather is extremely cold. Imagine working a whole night shift in such a place. What do you do? People undermining us, using racist language, making faces or gestures that suggest that, you know, they treat you with contempt or, disregard you all the way. What do you do? We keep quiet and say nothing because we don’t want trouble. Also, we need the money. But over here people look down on you if you do this type of work, and especially if you’re not from here. I obviously don’t want to do it forever because I don’t feel valued or appreciated. (P4)
Such narratives linked to perceptions of care work as low-skilled and lacking in professional recognition, prompting MCWs to reposition themselves in more socially valued forms of employment, particularly in sectors where their qualifications or upskilled competencies might become more visible and respected. This form of coping, as narrated by participants, reflects a quiet disengagement from structural devaluation, and may constitute a form of micro-resistance enacted through long-term planning, emotional distancing and skill diversification. By simultaneously performing the demands of care work and preparing to exit it, participants demonstrate that migrant workers are not always ‘passive’, ‘powerless’ or ‘integrating agents’ (Newlands, 2022), who forfeit their cultural selves and become fragile (Sarpong et al., 2024). Rather, MCWs remain operational in a system that undervalues them, while also seeking to transcend that system on their own terms.
Moonlighting
In addition to future planning, many MCWs turned to moonlighting, undertaking secondary jobs or informal income-generating activities as a coping mechanism, even in instances where their visas restricted them from engaging in such activities. These practices served both economic and cultural functions, simultaneously relieving the pressures of care work and reasserting identities that were marginalised or invisible within formal employment. A participant explained: During my spare time, I do hair braiding with African women, and I am beginning to know more people. This is good for me because it takes me away from the bustle of care work. It also brings me additional income to help with the bills. (P12)
This practice functioned as a form of cultural reworking, enabling the participant to engage in a familiar, affirming activity that contrasted with the physically and emotionally taxing routines of care labour. Hair braiding is embedded in shared cultural norms and communal participation and provided more than just income by offering a return to a valued self-image, a form of agency that contrasted with the institutional depersonalisation of care work. By performing culturally familiar roles, MCWs found ways to reclaim dignity, autonomy and relational connection, all of which are diminished in their primary employment relationships. Others used moonlighting as a way to enhance their material conditions or secure better employment arrangements. One participant recounted how a second job in a care home opened doors to new opportunities: I got a second job in a care home where I got regular shifts. My main sponsor at the time was an agency so work was not regular. There was an opportunity that came with sponsorship, so I spoke to the manager, applied and they offered me the sponsorship. It meant leaving my old job, but it also meant a permanent job with regular shifts. (P18)
By taking on another job in parallel to their sponsored role, participants were able to convert a precarious, irregular shift pattern into a more stable and predictable work arrangement with less uncertainty around hours and pay. What makes such practices particularly significant is that they often entail risk, especially under the UK’s Health and Care Worker visa scheme, which legally binds MCWs to a single employer, and allows care workers to only undertake 20 extra hours a week with another care provider other than their sponsoring employer. Some participants acknowledged that they took on more additional work despite knowing it contravened the conditions of their visa: I know I am only supposed to work for the sponsor, and 20 hours with another care home, but how do I survive when I don’t even get regular shift with my main employer? The hours they give are not enough. So, I do other jobs quietly. If I don’t, I can’t pay my rent and send money home. (P16)
These accounts underscore the structural vulnerabilities that characterise migrant labour in the care sector. While not framed by participants as overt acts of rebellion, moonlighting nonetheless serves as a subversive practice through which workers reject the full terms of their employment and reassert agency over their time, identity and income as means of coping. By leveraging opportunities outside their primary employment, MCWs could assert control over their careers, circumvent restrictive visa conditions and improve their working conditions in their own way.
Discussion
Care work provides a context in which coping is pervasive, a condition that becomes particularly acute for migrant care workers (MCWs) operating under restrictive immigration regimes and heightened vulnerability to exploitation (Ahmed, 2010; Ho et al., 2022; Liao et al., 2024; Zainal and Barlas, 2022). This study set out to examine how MCWs enact coping under such constraints, with a focus on the situated practices through which they endure, adapt to or at times even resist adverse working conditions. Our findings demonstrate that coping is neither an idiosyncratic psychological response nor a series of ad hoc individual tactics. Rather, coping emerges as a patterned social practice, materially and relationally embedded in the everyday organising of care work. While coping may initially be enacted at the individual level, for instance through cognitive reframing, it is sustained, reinforced and legitimised through collective practices such as informal knowledge exchange, migrant community support networks and the shared use of material resources. Through mutual aid, emotional reciprocity and informal knowledge-sharing, MCWs transform individual struggles into shared concerns, thereby reducing isolation and strengthening collective leverage vis-a-vis employers. Similarly, by blending formal organisational protocols with cultural repertoires drawn from their home countries, MCWs develop context-specific modes of caregiving that enhance both their sense of professional agency and the quality of care provided. Additional practices, such as moonlighting and informal upskilling, function as buffers against employment precarity, enabling workers to regain pockets of control and to covertly navigate unfavourable labour regimes. Importantly, these practices are recursive. As MCWs repeatedly mobilise material objects, relational ties and hybridised caregiving practices, these resources become routinised and collectively recognised as legitimate modes of coping. Coping thus emerges not as an individual attribute, but as a process mediated by and embedded within broader collective practices.
Building on practice theory (e.g. Pais Zozimo et al., 2023; Schatzki, 1996; Shove et al., 2012), this study makes two contributions to the migrant labour and coping literatures. First, we reconceptualise coping in migrant care work as a bundled social practice composed of patterned, collective and materially situated performances, rather than as individual psychological management (Duhachek, 2005; Kashdan et al., 2006). Because practices are constituted through their relations with material arrangements and social orders (Schatzki, 2013), coping becomes socially choreographed, in that it is learned, rehearsed, revised,and sanctioned within migrant collectivities. For instance, MCWs in our study described being coached by more experienced colleagues to manage challenges like racial microaggressions through quiet perseverance, peer support and cognitive reinterpretation of such encounters as ignorance rather than malice. In this sense, coping is neither purely individual nor fully collective, but fundamentally relational. This repertoire of coping thus combines cognitive reframing, material engagement (e.g. mobile and digital communication technologies),and socio-emotional support (Reckwitz, 2002; Schatzki, 2013). As Hau and Borello (2024) show, WhatsApp groups, social media networks and digital remittance platforms not only sustain emotional ties with families abroad but also facilitate the circulation of information about work rights, informal job opportunities and shared grievances. These platforms operate as teleoaffective infrastructures through which solidarity, humour and episodic resistance are enacted, even in the absence of formal unionisation or collective bargaining. At the same time, while such practices function as adaptive responses (Katz, 2004), they may also contribute to the normalisation of the structural conditions that necessitate coping, thereby obscuring the systemic inequalities embedded in visa regimes, labour relations and broader regimes of social reproduction (Wu et al., 2022; Zou et al., 2023).
Second, our findings of coping as a learned, shared and material practice illuminates how MCWs exercise agency within highly constrained and hierarchical work environments (Goel and Penman, 2015; Miles et al., 2024; Wu et al., 2022). By foregrounding the material and spatial dimensions of coping, we demonstrate how care settings, often doubling as both workplace and living space, actively shape which forms of coping are possible, permissible and intelligible. Factors such as sleep arrangements, access to food, surveillance technologies (e.g. CCTV) and spatial boundaries between ‘worker’ and ‘family’ roles profoundly structure everyday experiences of care labour (Anderson, 2000; Kilkey et al., 2018). Coping practices such as strategic compliance and silent withdrawal are not merely routine performances, but survival-oriented enactments shaped by spatial arrangements, material access and power asymmetries. Hybridised caregiving practices of blending formal protocols with cultural repertoires from home emerged as an unanticipated but significant coping mechanism, enabling MCWs to reclaim professional meaning and agency in constrained settings. This suggests the need for practice theory to more fully account for cultural transposition and improvisation in migrant labour contexts. Again, practices such as moonlighting and informal upskilling further emerged as covert forms of micro-resistance. While not overtly oppositional, these practices allowed MCWs to buffer against precarity and regain limited control over their futures. Following Katz’s (2004) framework, such practices operate along a continuum of resilience, reworking and resistance, blurring the boundaries between endurance and dissent. Therefore, by theorising coping as practice, this study contributes to a more temporally and spatially attuned understanding of agency in precarious labour. Coping, in this context, is neither reducible to acquiescence nor fully adversarial, but constitutes a future-oriented repertoire through which MCWs navigate, mitigate and at times subtly reconfigure the structural conditions of their work and lives.
Taken together, our findings suggest that care-providing institutions reliant on migrant workers and committed to the sustained delivery of care services should prioritise the design of supportive environments that enhance workers’ coping capacities. By incorporating materiality into the conceptualisation of coping, that is, emphasising how spaces, objects and social embeddedness co-constitute coping practices, this study offers insights for managers and policymakers by calling for the recognition of coping as a collective and practice-based phenomenon, rather than an individual’s show of resilience. Contrarily, when coping is framed solely as the responsibility of individual workers, it can foster resistance, potentially exacerbating workforce attrition. Organisations must therefore view coping as a potential driver of positive change, rather than simply a mechanism for maintaining status quo. For instance, investing in culturally sensitive training programmes, fostering collaborative team dynamics and optimising material and technological resources can improve migrant worker coping.
Limitation and further research
While our study advances understanding of migrant care workers’ coping, it also has some limitations, which in turn open opportunities for future research. First, while analysis of the stories we heard enabled us to identify MCWs’ coping practices, we conducted our research over a 12-month period. Longitudinal research that tracks the career journeys of migrant care workers over an extended duration is needed to elucidate the full temporal dynamics of their career mobility, so we can fully characterise antecedents, processes and consequences and effectively determine whether they exit or continue as care workers in the future given their present challenges.
Similarly, exploratory analysis inevitably opens itself to subjectivity and suspicion about potential inferences that merit further research. Yet, discursively grounded research based on migrant experience has implications for migrant workers’ success in cross-border deployment. The detailed spoken evidence of actors is equally relevant for policymakers to address the serious problem of care worker shortage in developed economies. Future studies could explore the interlinkages between age groups, country-specific response and tactics approaches between groups. Our sample comprised MCWs of African origin. We want to think that there are many migrant care workers who might engage and address the issues raised in the study in different ways as they do not fall within our sample. Similarly, there may even be cases of failure, where MCWs have either returned to their home countries, failed to meet the migration visa conditions, or had their sponsorships revoked. In such circumstances, how do they cope? These are fruitful cases for further exploration.
Conclusion
Research on coping among migrant care workers has gained traction as migrant labour becomes central to contemporary care economies. Nevertheless, the everyday ways in which MCWs themselves enact coping within care work remain underexplored. Drawing on practice theory, the study attends to this call by reconceptualising coping not as an individual psychological response, but as a relational, materially mediated and socially organised set of practices embedded in the labour process. In doing so, we contribute to migrant labour scholarship by showing how coping emerges through peer networks, shared cultural repertoires and tactical adaptations to restrictive visa regimes and often unfavourable workplace conditions. Our findings demonstrate that these coping practices are shaped by prior socialisation and lived experience, and are continually learned, circulated and normalised within migrant communities. By foregrounding coping as practice, the study further advances practice theory accounts of work by illustrating how agency is enacted under conditions of structural constraint. The coping practices identified constitute forms of endurance, adaptive reworking and, at times, micro-resistance. At the same time, our analysis complicates reductive portrayals of MCWs as either passive victims of exploitation or idealised, endlessly resilient workers. It reveals a central paradox: that is, while these practices enable migrant care workers to sustain themselves within unequal labour arrangements, they may also contribute to the normalisation and reproduction of the very conditions that necessitate coping. Ultimately, our findings suggest that sustaining migrant care labour requires moving beyond individualised notions of resilience towards systemic interventions that address the structural inequalities embedded in migration regimes, employment relations and care provision.
Footnotes
Appendix A: Interview guide
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.