
Abstract
The authors examined heterogeneity in posttraumatic stress disorder (PTSD) symptom presentation among veterans (n = 335) participating in the clinical interview subsample of the National Vietnam Veterans Readjustment Study. Latent class analysis was used to identify clinically homogeneous subgroups of Vietnam War combat veterans. Consistent with previous research, three classes emerged from the analysis, namely, veterans with no disturbance (61.4% of the cohort), intermediate disturbance (25.6%), and pervasive disturbance (12.5%). The authors also examined physical injury, war-zone stressor exposure, peritraumatic dissociation, and general dissociation as predictors of class membership. The findings are discussed in the context of recent conceptual frameworks that posit a range of posttraumatic outcomes and highlight the sizable segment of military veterans who suffer from intermediate (subclinical) PTSD symptoms.
Keywords
Until recently, posttraumatic mental health outcomes were conceptualized as binary phenomena. Individuals either developed a psychological disorder, such as posttraumatic stress disorder (PTSD), or were considered resilient in the face of the trauma. This simplistic assumption failed to acknowledge that people can be suffering and functionally impaired short of having a diagnosable condition and that, over time, outcomes are likely to be dynamic trajectories (e.g., some people may shift from minimal impact to clinically significant states, and so forth). Recent theory has emphasized heterogeneity in posttrauma outcomes, arguing that survivors may manifest numerous outcomes that differ in terms of symptom severity, presentation, and longitudinal course (e.g., Bonanno, 2004; Layne, Warren, Watson, & Shalev, 2007).
One analytical tool for examining heterogeneity in posttrauma outcomes is latent class analysis (LCA). LCA is a statistical technique that identifies homogeneous, qualitatively distinct subgroups of individuals, such as individuals with similar symptom presentations. Three LCAs of PTSD have been conducted to date. In the first, Breslau, Reboussin, Anthony, and Storr (2005) examined latent classes of PTSD symptoms in two trauma-exposed community samples. They found evidence for three distinct classes of individuals in both samples: those with no, intermediate, and pervasive symptom disturbance. The derived classes differed by severity and symptom configuration, with individuals with pervasive symptoms endorsing more symptoms of emotional numbing. Second, Ayer et al. (2011) examined latent classes of PTSD symptoms across two time points in a nationally representative community sample of adolescents and also found three discrete classes differing in terms of symptom severity (no, intermediate, and pervasive disturbance). As with Breslau et al. (2005), they found evidence for distinct symptom patterns that characterized the pervasive disturbance class (comprising a combination of symptoms from the different clusters). Third, Naifeh, Richardson, Del Ben, and Elhai (2010) examined latent classes of PTSD in a sample of Canadian veterans (mainly peacekeepers) receiving psychotherapy. They found a two-class solution consisting of intermediate and pervasive symptoms; the pervasively disturbed class endorsed more emotional numbing and dysphoria symptoms. Taken together, these studies suggest that, across trauma-exposed populations, homogeneous groups of individuals can be identified that are distinguishable by the extent and nature of their symptoms.
The nature of latent classes of PTSD symptoms in combat veterans remains unclear. The only study to investigate this to date, that of Naifeh et al. (2010), employed a sample composed predominantly of peacekeepers. The generalizability of their findings is also limited by the treatment-seeking nature of their sample, meaning that their findings are confined to individuals experiencing clinically significant distress, a relatively small subcomponent of the adjustment spectrum (a no disturbance class was likely not found for that reason). Determining the full range of responses to combat is important because service personnel and veterans with nontrivial but nondiagnosable PTSD may be uniquely at risk for chronic problems (see Nash, Steenkamp, Conoscenti, & Litz, 2011) and need to be identified to receive preventative interventions (e.g., in theater).
This study had two aims. First, we examined heterogeneity in PTSD symptom presentation in combat-related PTSD by conducting a LCA on a subsample of veterans participating in the National Vietnam Veterans Readjustment Study (NVVRS). The NVVRS was a congressionally mandated epidemiological study designed to assess the postwar adjustment of Vietnam veterans (Kulka et al., 1990).
Second, we aimed to extend earlier findings on LCA in PTSD by examining predictors of latent class membership. Specifically, we investigated the association of demographic variables, trauma exposure (physical injury and war-zone stressor exposure), and dissociation (peritraumatic dissociation and general dissociative experiences) with latent class membership. Exposure to deployment trauma is well established to be strongly related to psychological outcomes in veterans (e.g., King, King, Foy, Keane, & Fairbank, 1999). Peritraumatic dissociation and trait dissociation have been shown to be robust predictors of PTSD across trauma samples (Ozer, Best, Lipsey, & Weiss, 2003; van der Velden & Wittmann, 2008). In the NVVRS sample specifically, peritraumatic dissociation has been strongly associated with severity of PTSD symptoms, degree of stress exposure, and general dissociative tendencies, and predicts PTSD caseness over and above the contribution of war-zone stressor exposure and general dissociative tendencies (Marmar et al., 1994; Tichenor, Marmar, Weiss, Metzler, & Ronfeldt, 1996; see also Bremner et al., 1992). However, dissociation has not yet been examined as a predictor of latent classes of posttrauma outcomes, and the relationship between dissociation and quantitative and qualitative symptom variation in PTSD symptoms is unclear.
Based on the previous studies of LCA in civilian PTSD, we hypothesized that a three-class solution involving different degrees of symptom severity (no, intermediate, and pervasive disturbance) would best fit the data, and that the pervasive disturbance class would be characterized by greater emotional numbing. We also hypothesized that exposure to war-zone stress, sustaining physical injury, and endorsing higher levels of peritraumatic and general dissociation would predict membership in the pervasive disturbance class.
Method
Data Source
Participants were 335 theater veterans participating in the clinical examination component (CEC) of the NVVRS. The NVVRS, conducted between 1986 and 1988, employed a national probability sample to compare three groups: Vietnam theater veterans (i.e., veterans who served on active duty in Vietnam, Cambodia, or Laos), era veterans (i.e., veterans who were on active duty at the time of the Vietnam War but who did not serve in the Vietnam theater), and nonveteran civilians (i.e., those eligible to serve in Vietnam but who did not enter the military; see Kulka et al., 1990). A stratified subsample of individuals subsequently participated in the CEC, which involved more thorough structured diagnostic assessments administered by doctoral-level trauma experts (compared with trained lay interviewers in the main study); the aim of this subsample was to obtain valid estimates of PTSD prevalence. CEC participants lived within commutable distance of 28 designated metropolitan areas. The current analyses focused on theater veterans who participated in the CEC.
Measures
PTSD symptoms were evaluated with the PTSD module of the Structured Clinical Interview for the Diagnostic and Statistical Manual of Mental Disorders (3rd ed., rev.; DSM-III-R; American Psychiatric Association, 1987; Spitzer, Williams, Gibbon, & First, 1989), which followed DSM-III-R PTSD symptom criteria. Clinicians coded participants’ responses as absent, subthreshold, threshold, or as having inadequate information. Lifetime and current PTSD were assessed; only current PTSD was employed in the present analyses and was defined as PTSD being present for at least 1 month at any time during the past 6 months. An independent reliability check of current PTSD diagnoses yielded a kappa statistic of .87 (Weiss et al., 1992).
War-zone stressor exposure was a composite variable created by NVVRS investigators; scores were dichotomized into either low/moderate exposure or high exposure, based on an algorithm of relevant variables (see Schlenger et al., 1992). Example items include receiving enemy small arms fire, being involved in the killing or injuring of civilians, lacking food and supplies, and feeling a sense of purposelessness. Using this scale, Schlenger et al. (1992) found that current PTSD rates were 4 times higher in male veterans with high combat exposure than those with low/moderate combat exposure.
Dissociative tendencies as an individual difference characteristic was assessed using the Dissociative Experiences Scale (DES; Bernstein & Putnam, 1986), a 28-item self-report measure assessing absorption, amnesic experiences, depersonalization, and derealization. Participants rated the percentage of time (i.e., 0%-100%) that they experienced each symptom. DES is widely used in studies assessing dissociation in PTSD and has been demonstrated to have excellent reliability and validity (Bernstein & Putnam, 1986). Previous NVVRS studies conducting principal component analyses of this measure have found a one-factor solution, supporting the use of a total score on the measure to represent general trait dissociative tendencies (Marmar et al., 1994; Tichenor et al., 1996).
Peritraumatic dissociation was assessed with the Peritraumatic Dissociative Experiences Questionnaire, Rater Version (PDEQ; Marmar, Weiss, & Metzler, 1997), an eight-item interviewer-based questionnaire asking about experiences of dissociation (depersonalization, derealization, amnesia, altered time perception, and out-of-body experience) at the time of the most threatening war trauma, subjectively determined by the veteran. An earlier study of the NVVRS found the PDEQ to be internally consistent, with a Cronbach’s alpha of .80 (Marmar et al., 1994).
The number of serious postmilitary readjustment problems was a composite variable created by NVVRS investigators. Example items include having problems holding a job, problems with excessive drinking, problems having enough money to live on, and problems with the law. Participants rated each problem as either serious or minor; only serious problems were included in this variable.
Data Analysis
LCA was used to model PTSD symptoms profiles. Specifically, LCA uses binary indicators to identify patterns of responses and assigns individuals to classes on the basis of these patterns. In this analysis, latent classes were identified on the basis of 17 dichotomous indicators of PTSD symptoms. Individuals with similar symptom profiles were placed in the same class. LCA was undertaken in Mplus version 6.0 (Muthén & Muthén, 2006), and full maximum likelihood estimation was used to adjust for missing data on latent class indicator variables. Of a total of 440 participants in the CEC, 344 were theater veterans. Of these, 8 participants had missing data on all 17 symptoms and were excluded from the analyses. Sampling weights were used to adjust for oversampling by NVVRS researchers and to allow for the projection of results to the larger population of Vietnam veterans. One participant was excluded from analyses as the participant had no sampling weight available. LCA was used to identify the minimum number of classes that can account for associations between symptoms. The most parsimonious (one-class) model was initially fitted, followed by successive models with increasing numbers of classes to determine the number of latent classes that best fit the data. We assessed comparative model fit using the Sample-Size-Adjusted Bayesian Information Criterion, the Akaike’s Information Criterion, and entropy (an index of classification quality).
To assess predictors of class membership, we conducted multinomial logistic regression analyses using posterior probabilities of latent class membership derived from the optimal latent class model. Predictors included in the initial model were age, sex, race, educational status, war-zone exposure, injury, peritraumatic dissociation, dissociative experiences, use of mental health services, and number of readjustment problems. Only significant predictors were retained in the final model.
Results
Demographic characteristics of the sample are reported in Table 1. Three quarters of the sample were male (75.2%), and the mean age was 23 years; most had either a high school diploma (22%) or some college education (46%).
Demographic Information

Note: PDEQ = Peritraumatic Dissociative Experiences Questionnaire; DES = Dissociative Experiences Scale; PTSD = posttraumatic stress disorder.
LCA
The goodness-of-fit indices for the one- to four-class models are presented in Table 2. Based on fit indices and interpretability of class solutions, a three-class solution, representing no, intermediate, and pervasive PTSD symptoms, was judged to be the optimal solution (see Figure 1). Although it can be argued that a four-class solution had superior fit to a three-class solution, the fourth class identified consisted of only 14 individuals (4.4%) and was composed of a symptom pattern that was not consistent with theory and past research. Final-class counts based on estimated posterior probabilities were 42 (12.5%) for Class 1 (pervasive disturbance), 86 (25.6%) for Class 2 (intermediate disturbance), and 206 (61.4%) for Class 3 (no disturbance). Conditional probabilities of symptoms for the three-class solution are reported in Table 3. These represent percentages of members of each class that exhibit each symptom. In the pervasive disturbance class, 87.6% of participants met DSM-III-R criteria for PTSD, compared with 34.2% in the intermediate disturbance class and 3.0% in the no disturbance class. The mean number of PTSD symptoms reported was 11.01 (standard error [SE] = 0.49) in the pervasive disturbance class, 4.33 (SE = 0.27) in the intermediate disturbance class, and 0.44 (SE = 0.09) in the no disturbance class.
Goodness-of-Fit Statistics for One- to Four-Class Solutions

Note: BIC = Bayesian Information Criterion; AIC = Akaike’s Information Criterion.
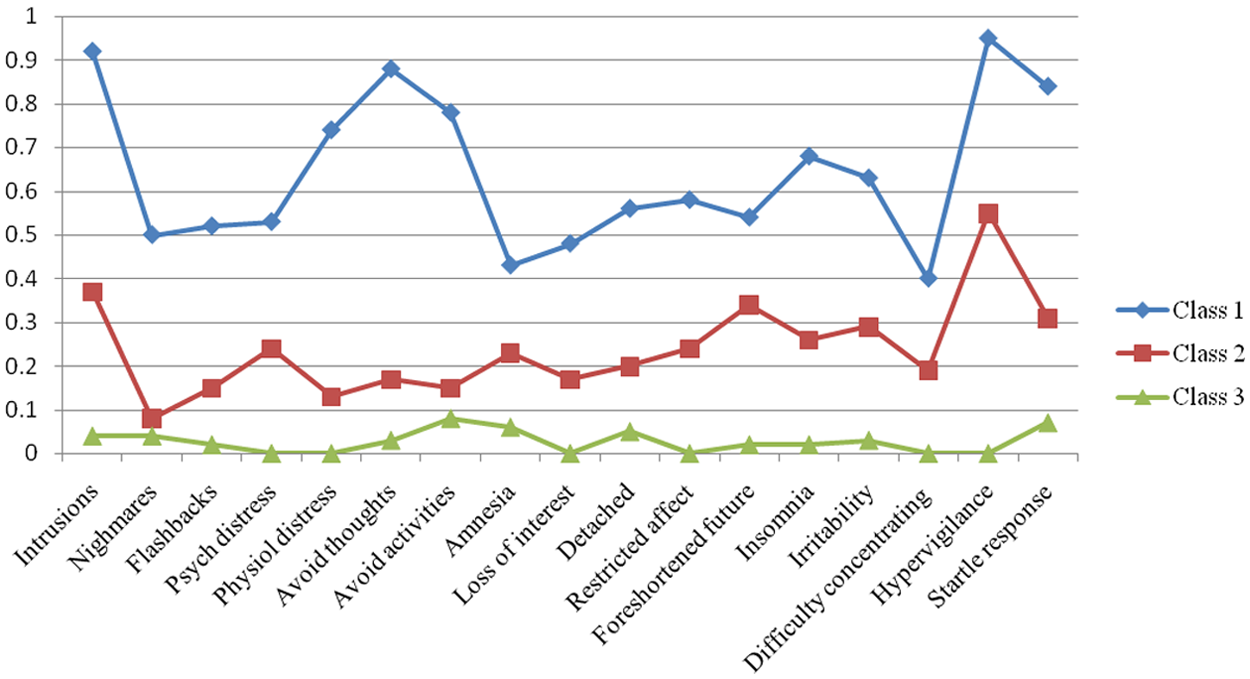
Estimated prevalence of posttraumatic stress disorder symptoms for each of the three latent classes
Conditional Probabilities of Class Membership for PTSD Symptoms for Three-Class Solution
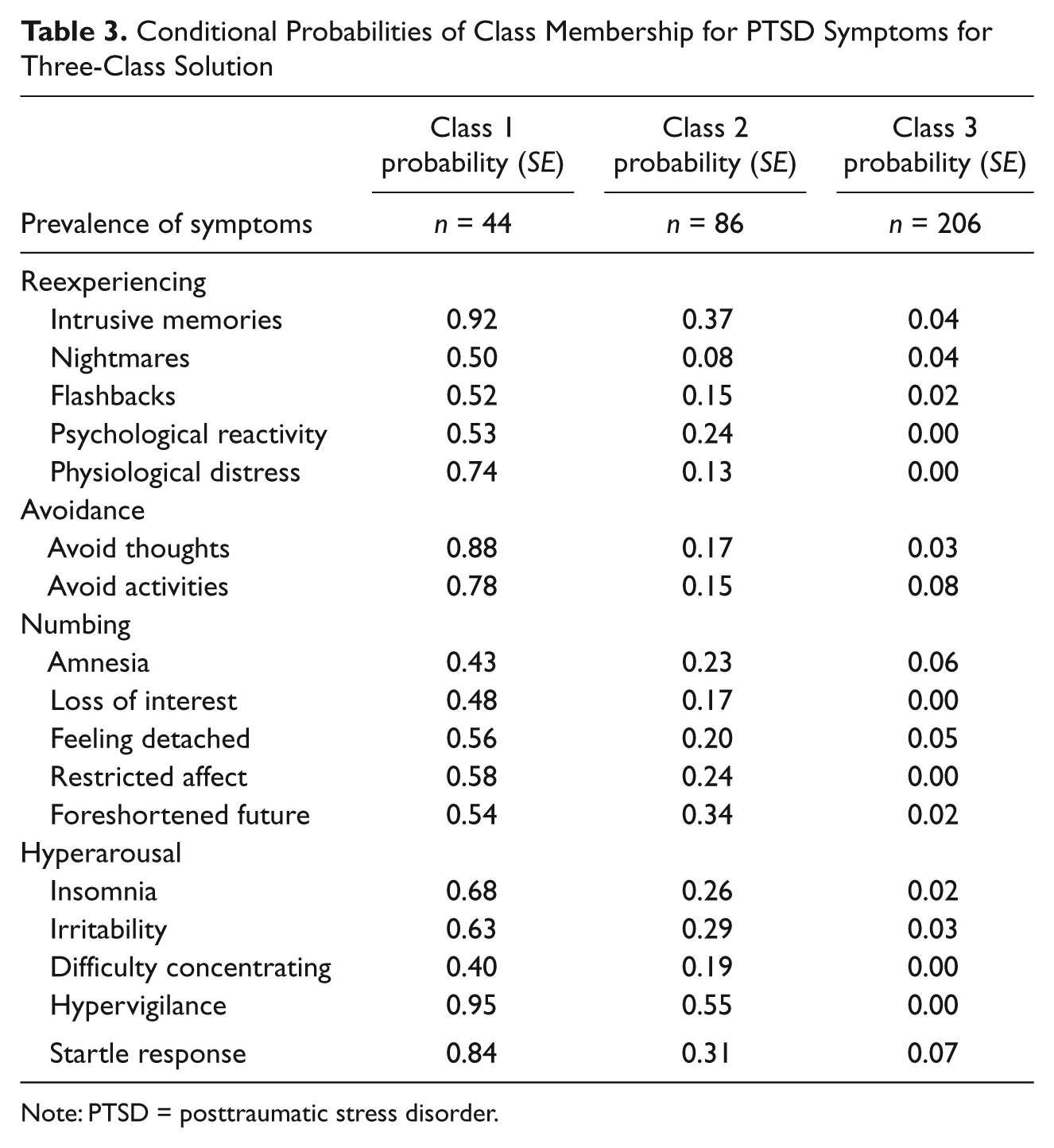
Note: PTSD = posttraumatic stress disorder.
Multinomial Logistic Regression
A multinomial logistic regression was conducted to examine predictors of class membership. Predictors in the initial model included sex, age, educational status, physical injury, number of serious postmilitary readjustment difficulties, war-zone stressor exposure, peritraumatic dissociation, and general dissociative experiences. Only significant predictor variables are reported here. Compared with those in the no disturbance class, individuals in the pervasive disturbance class had higher war-zone exposure (OR = 21.54, p < .001) and higher levels of readjustment difficulties (OR = 2.90, p < .01). Participants in the pervasive disturbance class also reported significantly higher levels of peritraumatic dissociation (OR = 15.85, p < .01) and general dissociative experiences (OR = 1.38, p < .001) than those in the no disturbance class. Compared with those in the no disturbance class, individuals in the intermediate disturbance class had significantly higher levels of peritraumatic dissociation (OR = 0.65, p < .001) and general dissociative experiences (OR = 1.27, p < .001). They had also been exposed to greater war-zone stressors (OR = 3.28, p < .05) and had more readjustment difficulties (OR = 2.08, p < .01). Compared with those in the intermediate disturbance class, individuals in the pervasive disturbance class had significantly higher war-zone stressor exposure (OR = 6.57, p < .01), higher levels of general dissociative experiences (OR = 1.09, p < .01), and more readjustment difficulties (OR = 2.49, p < .05).
Discussion
We examined latent classes of PTSD among Vietnam theater veterans to examine possible heterogeneity in postcombat outcomes. Three latent classes emerged from the data: a no, intermediate, and pervasive disturbance class. This three-class solution is consistent with earlier LCA studies of PTSD conducted in non-treatment-seeking civilian samples (Ayer et al., 2011; Breslau et al., 2005). Together, these studies underscore the dimensionality of the PTSD construct (e.g., King, Leskin, King, & Weathers, 1998; Ruscio, Ruscio, & Keane, 2002) and offer preliminary support for conceptual models positing a spectrum of responses to deployment stress and trauma (e.g., Nash et al., 2011).
Despite all participants serving in the Vietnam theater, the majority (61%) reported few PTSD symptoms. Indeed, other studies of veterans from past and current eras likewise show that, despite the stressors of war, the majority of veterans appear to fare well following war and report no to few psychological difficulties (e.g., Hoge et al., 2004; Larson, Highfill-McRoy, & Booth-Kewley, 2008; Toomey et al., 2007). Only 12% of the CEC fell into the pervasive disturbance class, a class that had a strong relationship with DSM-III-R PTSD diagnosis (approximately three quarters of the individuals in this class met criteria for PTSD). This is consistent with initial findings from the entire NVVRS sample, which indicated rates of current PTSD of 15.2% and lifetime PTSD rates of 30.9% (Kulka et al., 1990), although a subsequent reanalysis of the data following controversy over the accuracy of the initial results yielded rates of current PTSD of 9.1% and lifetime PTSD of 18.7% (Dohrenwend et al., 2006).
A particularly important finding when considering heterogeneity in posttrauma outcomes is that a quarter of the sample fell in the intermediate disturbance class. By comparison, Breslau et al. (2005) and Ayer et al. (2011) found that approximately one third of their participants fell in this class. Veterans in the intermediate disturbance class reported fewer PTSD symptoms than those in the pervasive disturbance class; approximately two thirds did not meet full diagnostic criteria for DSM-III-R PTSD but reported symptoms deemed by expert interviewers to be clinically significant. There is likely overlap in this class with subclinical PTSD (also called partial, subthreshold, or preclinical PTSD, that is, meeting some but not all criteria for a PTSD diagnosis), although it is not fully analogous to subclinical PTSD, as roughly one third of cases in this class did indeed meet full PTSD criteria. In a previous analysis of the NVVRS, Weiss et al. (1992) found current subclinical PTSD rates of 11.1% in males and 7.8% in females. Grubaugh et al. (2005) found that military veterans who experienced combat were approximately three times more likely to develop subclinical PTSD, compared with no PTSD.
These findings indicate that a sizable segment of military personnel will suffer from intermediate levels of exposure-related disturbance. However, compared with resilient outcomes and diagnosable PTSD, subclinical PTSD has received little empirical attention. The limited evidence available suggests that subclinical PTSD can result in levels of impairment and distress comparable with that of full PTSD (e.g., Marshall et al., 2001; Stein, Walker, Hazen, & Forde, 1997; Zlotnick, Franklin, & Zimmerman, 2002). For example, subclinical PTSD is associated with a host of negative physical health outcomes (e.g., Pietrzak, Goldstein, Malley, Johnson, & Southwick, 2009; Schnurr et al., 2000), as well as negative work outcomes, such as employee absenteeism and dysfunctional days at work, and these are similar in intensity to those of individuals with full PTSD (Shelby, Golden-Kreutz, & Andersen, 2008; Zlotnick et al., 2002). Subclinical PTSD cases have also been shown to have high rates of suicidal risk and ideation (Grubaugh et al., 2005; Marshall et al., 2001), and subclinical PTSD is a significant predictor of delayed onset PTSD (Carty, O’Donnell, & Creamer, 2006; Harvey & Bryant, 1999; Smid, Mooren, van der Mast, Gersons, & Kieber, 2009).
Dichotomous conceptualizations of PTSD may thus fail to recognize significant distress, dysfunction, and morbidity in the sizable portion of veterans with intermediate or subclinical levels of PTSD. Expanding dichotomous views to recognize individuals with intermediate PTSD reactions holds implications for the rates of perceived “resilience” in veterans and service members. That is, rates of resilience will be much higher when using binary PTSD/no PTSD conceptualizations, given that anyone not meeting diagnostic criteria for PTSD is presumed to be resilient (rather than possibly struggling with subclinical levels of distress). Taking into account subclinical levels of PTSD will thus provide a more accurate estimation of the need for psychological services among veterans and active duty personnel, and holds important policy implications for prevention and treatment programs. Moreover, with the development of the DSM-V underway, our findings highlight the disconnect between diagnostic thresholds for PTSD that are based on a medical model and that bisect survivors into either healthy or disordered, and the growing empirical evidence that PTSD reactions lie on a continuum of severity. To ensure that all suffering trauma survivors receive needed services, it may be helpful to allow for greater flexibility surrounding diagnostic cutoffs and to encourage greater emphasis on degree of functional impairment rather than symptom algorithms.
Although our findings suggest that classes of individuals were primarily distinguishable by the severity of their symptoms, some qualitative differences were also evident between the classes. We found that avoidance and hypervigilance were most pronounced in the pervasive disturbance class. This is in contrast to findings by Breslau et al. (2005) and Naifeh et al. (2010) who found emotional numbing to best distinguish the pervasive disturbance class. The importance of avoidance in the onset and maintenance of PTSD has been well documented (e.g., Dunmore, Clark, & Ehlers, 1999; Ullman, Townsend, Filipas, & Starzynski, 2007); theoretically, avoidant coping may preclude necessary cognitive and emotional processing of the trauma, maintaining symptoms over time. The prominence of hypervigilance among the pervasive class may be related to the nature of our sample. All veterans included in this analysis had served in theater; while in theater, hyperarousal is an adaptive response, facilitating scanning the environment for danger. Hypervigilance that persists in situations of safety, particularly many years following the combat situation as in the current sample, may be a salient indicator of severe posttraumatic stress reactions and failure to down regulate anxiety responses. Moreover, the intermediate and pervasive disturbance classes endorsed nightmares, in contrast to the no disturbance group, suggesting that nightmares may be a key indicator of a pathological posttrauma process.
We also examined predictors of latent class assignment, namely, age, sex, educational status, war-zone stressor exposure, being injured, peritraumatic dissociation, and general dissociation. Such analyses are important because as the military increasingly aims to develop indicated and selective PTSD prevention strategies for troops (e.g., Casey, 2011), risk and protective algorithms are needed to identify those service members unlikely to recover naturally on their own. Those in the pervasive disturbance class reported greater war-zone stressor exposure, lower education, and more peritraumatic and general dissociation. Our findings are consistent with numerous studies that have indicated a dose–response relationship between war-zone stressor exposure and the development of PTSD, including in the NVVRS (e.g., Schnurr, Lunney, & Sengupta, 2004). For instance, among male Vietnam theater veterans, 35.8% with high combat stress exposure develop PTSD, compared with only 8.5% of those with low combat stress exposure (Schlenger et al., 1992). Our results also support previous findings that lower educational level is a risk factor for PTSD in Vietnam veterans (Kulka et al., 1990).
In terms of peritraumatic and general dissociation, it may be that veterans who did not experience dissociation were more able to emotionally and cognitively process their traumas (possibly because trauma memories were less fragmented and disorganized), and thus saw a decrease in symptoms over time (e.g., Ehlers & Clark, 2000). Of note, veterans in the intermediate disturbance class reported more peritraumatic and trait dissociation than those in the no disturbance class, suggesting that dissociation may be a predictor of clinical and subclinical PTSD.
A limitation of this study is that it is cross-sectional in nature, precluding examination of latent classes of individuals within a longitudinal framework; examination of longitudinal trajectories of postdeployment outcomes is an important next step in the field. For example, latent transition analysis, which examines transitions in latent class membership over time (e.g., transitioning from the intermediate disturbance class to the pervasive disturbance class), could shed light on the dynamic course of symptoms over time. In particular, future research is needed to determine whether subclinical PTSD symptoms are predictive of later full PTSD in military populations and to identify factors that influence its progression. Although numerous studies have examined risk factors for full PTSD among military personnel (see Maguen, Suvak, & Litz, 2006), there is very little research examining risk factors for subclinical PTSD. The data are also retrospective, which may have affected memory of predictor variables such as peritraumatic dissociation and extent of war-zone stressor exposure. It is also unclear to what extent these findings are generalizable to service members and veterans taking part in more recent wars, such as those in Iraq and Afghanistan. Last, PTSD symptoms in our sample were assessed based on DSM-III-R criteria, which did not require that symptoms produce functional impairment, as is the case with DSM-IV (American Psychiatric Association, 1994); our estimated rates of PTSD diagnoses may thus not generalize to diagnoses based on current criteria. We assessed the number of serious readjustment problems in our sample as a proxy for functional impairment, and found more readjustment problems in intermediate and pervasive disturbance classes.
In sum, this study adds to a growing body of research supporting a recent theoretical shift that underscores the heterogeneity of outcomes following trauma and loss. In contrast to frameworks that tacitly assume outcomes dichotomized into either PTSD or resilience, our findings suggest that combat-exposed veterans fall into three groups following deployment. These classes differ in PTSD severity and symptom presentation, with those with the most pervasive disturbance being characterized by avoidance and hypervigilance in particular. Our findings likewise indicate that membership in these outcome groups can be predicted, and that lower educational level, greater war-zone stressor exposure, and more peritraumatic dissociation and general dissociation are factors that may help in the identification of risk in combat veterans. As a new generation of veterans emerges from the wars in Iraq and Afghanistan, a broader view of deployment trauma and its sequelae is needed that takes into account the full range of postdeployment outcomes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.