
Abstract
For individuals with generalized anxiety disorder, worry becomes associated with numerous aspects of life (e.g., time of day, specific stimuli, environmental cues) and is thus under poor discriminative stimulus control (SC). In addition, excessive worry is associated with anxiety, depressed mood, and sleep difficulties. This investigation sought to provide preliminary evidence for the efficacy of SC procedures in reducing anxiety-, mood-, and sleep-related symptoms. A total of 53 participants with high trait worry were randomly assigned to receive 2 weeks of either SC training (consisting of a 30-min time- and place-restricted worry period each day) or a control condition called focused worry (FW; consisting of instructions to not avoid naturally occurring worry so that worry and anxiety would not paradoxically increase). At post-training, SC was superior to FW in producing reductions on measures of worry, anxiety, negative affect, and insomnia, but not on measures of depression or positive affect. Moreover, SC was superior to FW in producing clinically significant change on measures of worry and anxiety. Results provide preliminary support for the use of SC training techniques in larger treatment packages for individuals who experience high levels of worry.
Generalized anxiety disorder (GAD) is characterized by excessive, uncontrollable worry about various topics. GAD affects a large number of individuals, with 12-month and lifetime prevalence rate estimated at 2.7% and 5.7%, respectively (Kessler et al., 2005). Despite the high prevalence rates of GAD, the field’s success in identifying efficacious treatments has been relatively limited. Specifically, although cognitive-behavioral therapy (CBT) for chronic worriers has been shown to produce large effect sizes at post-therapy and at follow-up compared with no treatment, nonspecific components, component control conditions, and alternative treatments (Borkovec & Ruscio, 2001), this treatment is associated with high end-state functioning in only 50% of treated clients (Borkovec, Newman, Pincus, & Lytle, 2002). Whereas most anxiety disorders are characterized by fear of discrete stimuli (e.g., public situations for an individual with social anxiety disorder), the lack of an identifiable core fear in worry and instead a broad range of poorly defined stimuli and future-oriented potential negative events limits our ability to design efficacious behavioral exposure-based treatments for GAD. It should be noted that cognitive exposure-based treatments such as an imaginal exposure (Craske, Barlow, & O’Leary, 1992) have been shown to be efficacious in larger treatment packages (e.g., intolerance of uncertainty therapy [IUT]; van der Heiden, Muris, & van der Molen, 2012) as well as a stand-alone treatment for GAD (Hoyer et al., 2009). In recent years, several treatment packages for GAD have emerged with promising outcomes (e.g., IUT, Dugas & Ladouceur, 2000; metacognitive therapy [MCT], Wells, 1999); however, these treatment packages contain multiple interventions designed to target areas of functioning that have been identified as maladaptive in the lives of chronic worriers (Behar & Borkovec, 2005). Thus, it is important to examine the efficacy of each intervention that comprises the various treatment packages.
One therapeutic tool designed to target maladaptive behavioral functioning is stimulus control (SC) for worry (Behar & Borkovec, 2005, 2009). For individuals with GAD, excessive worry becomes associated with numerous aspects of daily life (e.g., time of day, environmental cues). As a result, these individuals tend to worry about many different topics, across many different contexts, and are thus described as having poor discriminative SC. Indeed, Lang (1979, 1985) theorized that GAD is characterized by lack of specificity of fear stimuli, which ultimately leads to difficulties in memory network activation (a necessary component of emotional processing; Foa & Kozak, 1986) and thus interferes with successful habituation of fear. SC procedures for the treatment of worry were initially developed by Borkovec, Wilkinson, Folensbee, and Lerman (1983) to help chronic worriers increase specificity of fear stimuli and consequently gain greater control over the incidence of worry. In SC for worry, clients are provided with four general rules: (a) identify worrisome and unpleasant thoughts and learn to distinguish those from other more pleasant thoughts, (b) establish a 30-min “worry period” to occur at the same time and in the same location, (c) delay spontaneous worry to the worry period and instead focus on the present moment, and (d) use the 30-min worry period to worry about concerns and problem solve to reduce or eliminate concerns (Borkovec, Wilkinson, et al., 1983).
Unlike the other components of CBT for GAD (e.g., cognitive therapy, self-control desensitization, relaxation; Borkovec et al., 2002), SC for worry has limited empirical support. Only one study has investigated the efficacy of SC procedures among high worriers (Borkovec, Wilkinson, et al., 1983). In this investigation, undergraduate participants who reported worrying at least 50% of the time were randomly assigned to either a SC training condition or to a no-treatment condition. All participants completed a baseline assessment for 1 week, during which they completed daily ratings of the percentage of time they worried or felt tense each day, the severity of tension they experienced, and the degree to which their worry content for that day related to six topics (see Borkovec, Wilkinson, et al., 1983). Following this baseline assessment, participants in the SC training condition were asked to continue completing these measures each day for the 4-week training period and were given instructions for SC treatment of worry as detailed above (Borkovec, Wilkinson, et al., 1983). Participants in the no-treatment condition were not given any additional instructions and were asked to continue completing daily ratings throughout the treatment period. Results indicated that participants in the SC condition reported greater reductions in daily percentage of worry and tension relative to those in the no-treatment condition.
A major methodological limitation of the Borkovec, Wilkinson, et al.’s (1983) investigation is that it failed to include a credible control condition, introducing numerous rival hypotheses to explain observed differences between the SC and no-treatment conditions (e.g., attention to the problem, expectancy for change, therapeutic relationship, demand characteristics). Thus, the present study sought to improve on Borkovec, Wilkinson, et al.’s investigation by including a second credible training condition to systematically control for all major threats to internal validity and thus provide a more rigorous test of the efficacy of SC procedures for worry. To this end, we compared SC training with a condition in which worry was not subject to discrimination training, but rather was allowed to occur throughout the day without limitations regarding time or place.
In addition to the impact of chronic worry on anxiety and mood (Andrews & Borkovec, 1988), worry is also closely associated with sleep disturbance. Insomnia is highly comorbid with a number of psychological conditions, especially anxiety and depression (Ree & Harvey, 2004). Individuals with insomnia often report the inability to fall asleep as a result of excessive worry while trying to engage in sleep (Harvey, 2002). Furthermore, Mellinger, Balter, and Uhlenhuth (1985) found that among patients with severe sleep disturbance, 42% reported elevated anxiety symptoms and 13% of those patients with sleep disturbance reported symptoms typical of GAD. Interestingly, the inspiration for employing SC training with chronic worriers originated with Bootzin’s (1972) SC treatment for insomnia. This procedure’s presumed applicability to the treatment of GAD was developed based on theoretically similar classical conditioning processes (i.e., like sleep difficulties, worry is likely conditioned to environmental stimuli). Given these similar processes and the frequent experience of worry during sleep attempts in insomnia, SC for worry may also be effective in reducing sleep disturbance.
The present study was a replication and extension of Borkovec, Wilkinson, et al.’s (1983) original investigation of SC training. The goal of this study was to provide preliminary empirical support for the efficacy of SC training for worry by comparing it with a credible control condition. Specifically, we examined the efficacy of SC for worry 1 among high trait worriers on measures of worry, anxiety, and depression. In addition, we sought to evaluate the efficacy of SC training for worry on general emotionality given the strong association between negative affect (NA) and worry (Borkovec, Robinson, Pruzinsky, & DePree, 1983), as well as on insomnia given the association between worry and insomnia (Harvey, 2002). We compared SC training with a credible control training procedure (called focused worry [FW]) to control for common factors and threats to internal validity (Behar & Borkovec, 2003). We hypothesized that compared with the FW condition, SC training would lead to greater ameliorations in subjective reports of worry, anxiety, depression, NA, and insomnia, as well as enhanced positive affect (PA).
Method
Participants
A total of 53 introductory psychology students from a large urban university were included in this investigation. The Penn State Worry Questionnaire (PSWQ; Meyer, Miller, Metzger, & Borkovec, 1990) was initially administered to a group of 800 students as part of a group screening procedure. Individuals scoring at least a 67 on the PSWQ (shown to distinguish GAD individuals from nonanxious individuals; Molina & Borkovec, 1994) were initially invited to participate and were retained in the investigation if their PSWQ score at the baseline assessment session was at least a 53 (one standard deviation above the mean for nonselected samples; Gillis, Haaga, & Ford, 1995). On average, participants’ scores on the PSWQ decreased slightly from the group screening session to the baseline assessment (M = −4.00, SD = 6.44); however, participants still evidenced elevated PSWQ scores at the baseline assessment (M = 67.85, SD = 5.78). One participant was excluded from the investigation because he no longer met this inclusionary criterion at the baseline assessment session. Six additional participants’ data were excluded from analyses because they did not provide enough data (more than 30% missing data, n = 4 [3 in SC and 1 in FW]) or dropped out of the study for personal reasons prior to being randomly assigned to a condition (n = 2).
Remaining participants were predominantly female (82.6%), with a mean age of 19.9 years (SD = 3.8 years). The sample was ethnically diverse and comprised 43.5% Caucasian, 10.9% African American, 19.6% Asian, 13.0% Latino, and 13.0% other participants. Participants included in the analyses did not differ from excluded participants with respect to age, t(50) = −0.98, p = .33; sex, χ2(1) = 0.00, p = .97; ethnicity, χ2(1) = 1.62, p = .20; or race, χ2(7) = 7.33, p = .40. Race, ethnicity, and gender were equivalent across the two experimental conditions; however, age was not equivalent, SC: M = 21.00, SD = 5.00; FW: M = 18.74, SD = 1.45, t(44) = −2.08, p = .04. Two participants in SC condition were outliers with respect to age; when these individuals were excluded from the analyses, results did not differ. Thus, data analyses included these participants, and we entered age as a covariate in all analyses. Participants were randomly assigned (using a computerized random number generator) to either the SC (n = 23) or FW (n = 23) condition. The purpose and hypotheses of the study were masked throughout the experiment. All participants received course credit as compensation for participation in the experiment.
Measures of Symptomatic Functioning
Participants were asked to complete a battery of measures during the pre- and posttraining sessions to assess trait levels of worry, anxiety, depression, PA and NA, and insomnia.
PSWQ
The PSWQ (Meyer et al., 1990) is a 16-item self-report questionnaire that assesses the frequency and intensity of worry. The PSWQ has demonstrated favorable reliability and validity for clinical and nonclinical populations (Brown, Antony, & Barlow, 1992). It has good sensitivity (0.75) and specificity (0.86) in distinguishing GAD samples from nonanxious controls and from other anxiety groups (Behar, Alcaine, Zuellig, & Borkovec, 2003; see also Brown et al., 1992). In this study, the PSWQ had acceptable to good internal consistency (.72 at pre-training and .90 at post-training).
Beck Anxiety Inventory (BAI)
The BAI (Beck, Epstein, Brown, & Steer, 1988) is a 21-item self-report questionnaire that measures severity of anxiety. The BAI has favorable retest reliability (0.75), as well as good convergent (0.51) and discriminant validities (0.15-0.48; Beck, Epstein, et al., 1988). In this study, the BAI had good internal consistency (.84 at pre-training and .86 at post-training).
Beck Depression Inventory (BDI)
The BDI (Beck, Ward, Mendelson, Mock, & Erbaugh, 1961) is a 21-item self-report questionnaire that measures severity of depression in clinical and nonclinical samples. In an undergraduate sample, the BDI had good stability (0.83) and favorable discriminant validity (Beck, Steer, & Garbin, 1988). In this study, the BDI had excellent internal consistency (.90 at pre-training and .93 at post-training).
Positive and Negative Affect Schedule–General (PANAS-General)
The PANAS (Watson, Clark, & Tellegen, 1988) is a 20-item self-report measure that assesses PA and NA. In the present study, we asked participants to indicate how they “generally feel.” The PANAS demonstrates good reliability for PA (0.86-0.90) and NA (0.84-0.87) as well as good external validity (Watson et al., 1988). In this study, the PANAS evidenced good internal consistency for PA (.88 at pre-training and .93 at post-training) and NA (.86 at pre-training and .87 at post-training).
Insomnia Severity Index (ISI)
The ISI (Bastien, Vallieres, & Morin, 2001) is a 7-item self-report questionnaire that assesses sleep problems, impairment of functioning due to inadequate sleep, and perceptions of severity of insomnia. The ISI has good concurrent validity at baseline (0.32-0.55) and following CBT, pharmacotherapy, or combination treatment (0.50-0.91; Bastien et al., 2001). In addition, the ISI has good internal reliability at baseline (0.76) and follow-up (0.78; Bastien et al., 2001). In this study, the ISI had good internal consistency (.82 at pre-training and .87 at post-training).
Procedure
Pre-training
Following participants’ consent to take part in the study, they were asked to complete all pre-training measures (PSWQ, BAI, BDI, PANAS, and ISI). The first author met with each participant individually for one session to explain the training conditions. All instructions were scripted to ensure consistency of information across participants and minimize risk of experimenter bias. Participants were asked to complete the Credibility and Expectancy Questionnaire (CEQ; Borkovec & Nau, 1972) to allow for testing of potential between-groups differences in the degree to which the two types of training were perceived as credible and the degree to which each training elicited expectancy for improvement. This questionnaire contained six items about credibility and four items about expectancy regarding participants’ perceptions and anticipated benefits of the training procedures. Each item utilized a 1 to 9 Likert-type scale with higher numbers indicating greater credibility or expectancy. Participants were asked to complete one CEQ regarding their perceptions of the effects of training on worry (CEQ-Worry), and a separate CEQ regarding their perceptions of the effects of training on insomnia (CEQ-Sleep). Participants were also provided with written materials that reiterated the rationale for the training procedure and all instructions that had been delivered by the first author, and were asked to review these materials periodically to ensure proper implementation of all training procedures. Participants used all training procedures over the course of a 14-day period. 2
Training conditions
Participants in both conditions were first informed that they had been selected to participate in this study based on their high levels of worry in their everyday lives and that as part of the study, they would learn and subsequently engage in procedures specifically designed to help them reduce their worry.
In the SC training condition, the experimenter first provided participants with the rationale for the intervention. Participants were told that when worry occurs throughout the day, it can become associated with many places, times, and situations, such that over time mere exposure to those places, times, and/or situations can come to elicit spontaneous worry. The goal of SC is thus to reduce the frequency of worry by gradually coming to associate worry with more distinct and specific times and locations, so that only those times and locations come to elicit worry and its associated emotional experiences. Participants were given the same four instructions as outlined earlier from Borkovec, Wilkinson, et al. (1983). Specifically, participants were taught to identify their worrisome thoughts and were asked to identify a specific and consistent 30-min worry period and location each day, during which they would focus on these worries. In helping participants to identify a 30-min worry period, the first author ensured that the period was at least 3 hrs prior to participants’ bedtimes so that the worry process would not interfere with their ability to fall asleep, given that worry and anxiety that occur before bedtime can lead to increased subjective reporting of insomnia and daytime fatigue (Chambers & Kim, 1993). Participants were instructed to worry as they normally do during their prescribed worry period, to do so as intensely as possible, and to keep the focus of their attention on the worry process. They were instructed to postpone spontaneous worry during the day to the worry period and instead to focus on the present-moment experience when they noticed themselves worrying outside of their prescribed worry periods. Finally, they were instructed to use the worry period to worry about their concerns and problem solve when appropriate.
In the FW condition, we sought to provide participants with a rationale that would encourage them to engage in worry as they normally do, and to expect that this practice would lead to a reduction in worry and its associated emotions. Compared with nonanxious individuals, individuals with GAD are more susceptible to experiencing paradoxical increases in worry while trying to suppress worrisome thoughts (Becker, Rinck, Roth, & Margraf, 1998). Thus, participants in this condition were told that people often try to avoid the occurrence of worry throughout the day, which paradoxically leads to increased levels of worry and its associated emotional experiences. The goal of the training program was thus to help them not avoid spontaneous worry, but rather to allow it to naturally occur to decrease the frequency and intensity of paradoxical increases in anxious thoughts and emotions. Participants were instructed to worry as they normally do anytime they noticed such thoughts occurring, to make this worry as intense as possible, and to keep the focus of their attention on the worry process. Although participants in this condition did not have a prescribed amount of time during which they were to engage in worrying each day, and thus may have engaged in more worry relative to participants in the SC training condition, it is important to note that chronic worriers report worrying for the majority of the day (60% of the day, as compared with 18% for nonanxious individuals; Craske, Rapee, Jackel, & Barlow, 1989). Thus, we anticipated that a credible intervention would most likely lead to reductions (as opposed to further increases) in overall levels of daily worry. It should be noted that the FW condition contained some elements of existing treatment packages. For example, the instructions to not avoid spontaneous worry are similar to the experiential exercises taught in acceptance and commitment therapy (ACT; Hayes, 2004; Hayes, Luoma, Bond, Masuda, & Lillis, 2006). Similarly, the instruction to focus attention on the process of worry is consistent with mindfulness techniques that have been shown to reduce worry among individuals with GAD (Roemer, Orsillo, & Salters-Pedneault, 2008).
Post-training
At the post-training session, participants were asked to complete the same measures that were given at the pre-training session. On completion, they were given a debriefing statement that informed them about the purpose of the two training conditions.
Results
Preliminary Analyses
Equivalence of symptomatic functioning at pre-training
Preliminary analyses sought to ensure equivalent pre-training levels of symptomatic functioning across the two training conditions. A series of univariate ANOVAs examining between-groups differences on each measure of symptomatic functioning (PSWQ, BAI, BDI, ISI, PA, and NA) indicated that participants across the two experimental conditions did not differ at pre-training on any of these measures (all ps are ns). Thus, random assignment to condition successfully produced equivalent scores on these measures across the two training conditions. Table 1 presents participant functioning on all symptom measures at pre- and post-training.
Means (and SDs) for Each Outcome Measure at Pre- and Post-Training With Effect Sizes
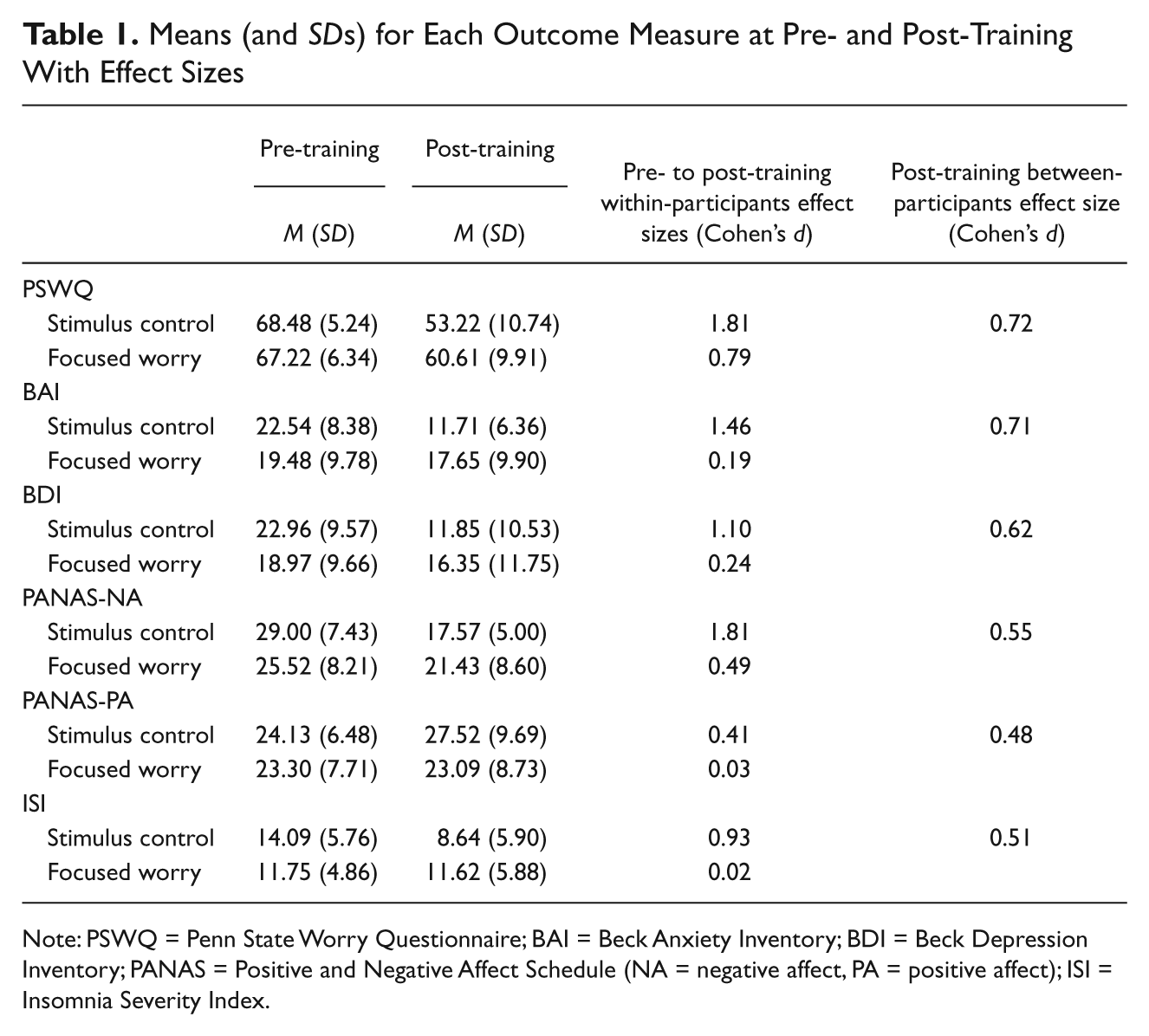
Note: PSWQ = Penn State Worry Questionnaire; BAI = Beck Anxiety Inventory; BDI = Beck Depression Inventory; PANAS = Positive and Negative Affect Schedule (NA = negative affect, PA = positive affect); ISI = Insomnia Severity Index.
Credibility and expectancy
We also sought to ensure that participants in the two conditions perceived their assigned training conditions to be equally credible and that they evidenced equivalent levels of expectancy to change. We conducted two separate sets (for the CEQ-Worry and CEQ-Sleep) of univariate ANOVAs, with Condition as the between-participants variable, for credibility and expectancy ratings. For the CEQ-Worry analyses, results indicated equivalent levels of credibility across the SC (M = 23.83, SD = 5.47) and FW (M = 23.48, SD = 5.98) training conditions, F(1, 43) = 0.05, p = .83,
Training compliance
We sought to ensure that participants in both conditions evidenced adequate and equivalent compliance to their training. Compliance was measured by calculating the number of days (ranging from 0 to 14) that each participant completed 60% or more of their daily questionnaires. 2 Participants evidenced good compliance in SC (M = 13.14, SD = 1.28) and FW (M = 13.43, SD = 1.04) conditions, and compliance did not differ across the two groups, t(42) = 0.84, p = .41. In addition, participants in the SC condition evidenced good compliance to engaging in their worry periods throughout the 14-day training (M = 87.50%, SD = 16.85%). 3
Symptom Measures
A 2 (Condition: SC, FW) × 2 (Time: pre-training, post-training) repeated measures MANCOVA was run on the three primary outcome measures (PSWQ, BAI, and BDI). Given that these three dependent variables were moderately correlated (.37 ≤ rs ≤ .49), we interpreted the Roy–Bargmann stepdown analyses instead of the univariate analyses. 4 Results indicated that there was a multivariate main effect of Time, F(3, 41) = 5.87, p = .002, which was qualified by a multivariate Condition × Time interaction, F(3, 41) = 4.67, p = .007. The results of the Roy–Bargmann stepdown analyses indicated that the Condition × Time interaction was significant for the PSWQ, F(1, 43) = 6.90, p = .012, and for the BAI, F(1, 42) = 5.34, p = .026, but not for the BDI, F(1, 41) = 1.06, p = .310.
Follow-up analyses for the PSWQ and BAI findings involved conducting 2 (Condition) × 2 (Time) mixed model ANCOVAs on each dependent variable, with Condition as a between-participants variable and Time as a repeated measures variable. Both sets of analyses yielded significant results. For the PSWQ analysis, results indicated a main effect of Time, F(1, 42) = 44.05, p = .000,
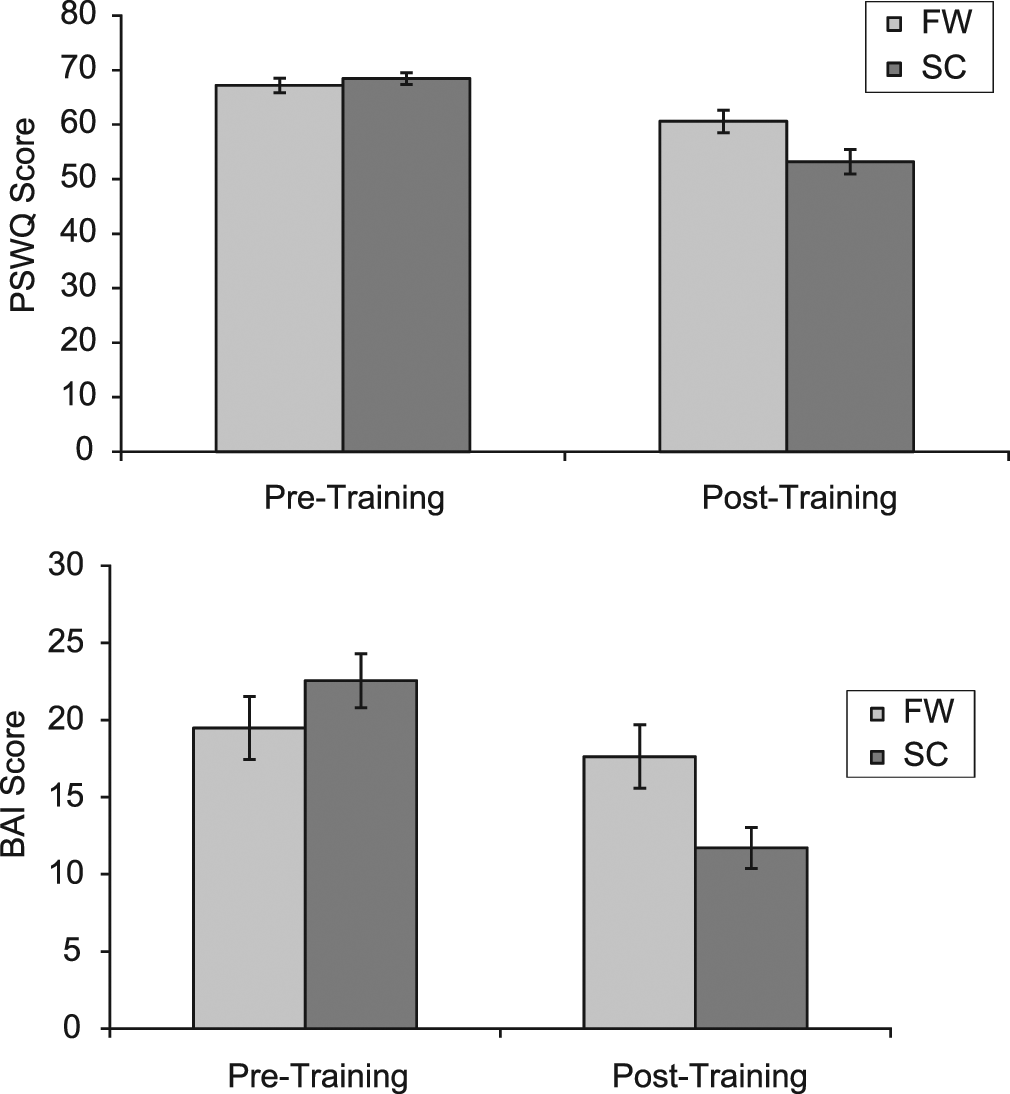
Pre- to post-training changes in PSWQ scores for the FW and SC conditions (top) and pre- to post-training changes in BAI scores for the FW and SC conditions (bottom)
General Affect Measures
To examine the two secondary general affect measures (NA and PA), we conducted two separate 2 (Condition: SC, FW) × 2 (Time: pre-training, post-training) mixed model ANCOVAs. For the NA analysis, results indicated a main effect of Time, F(1, 42) = 45.63, p = .000,
Insomnia
To examine the effect of training on insomnia, we ran a 2 (Condition: SC, FW) × 2 (Time: pre-training, post-training) mixed model ANCOVA on the ISI. Results indicated a main effect of Time, F(1, 42) = 14.23, p = .001,
Clinically Significant Change
Consistent with recommendations by Jacobson and colleagues (Jacobson, Follette, & Ravenstorf, 1984; Jacobson & Truax, 1991), we assessed clinically significant change by calculating the proportion of participants in each group who scored two standard deviations below the pre-training group mean for the PSWQ, BAI, BDI, and ISI (see Table 2). Results indicated that for the PSWQ, 65.2% of participants in SC and 30.4% of participants in FW evidenced clinically significant change; this difference was statistically significant, χ2(1) = 5.58, p = .018. For the BAI, 21.7% of participants in SC and none of the participants in FW evidenced clinically significant change; this difference was also statistically significant, χ2(1) = 5.61, p = .018. For the BDI, 13% of participants in SC and none of the participants in FW evidenced clinically significant change; this difference represented a nonsignificant trend, χ2(1) = 3.21, p = .07. For the ISI, 8.7% of participants in SC and none of the participants in FW evidenced clinically significant change; however, the two groups did not statistically differ, χ2(1) = 2.09, p = .148.
Percentage of Participants Evidencing Clinically Significant Change at Post-Training
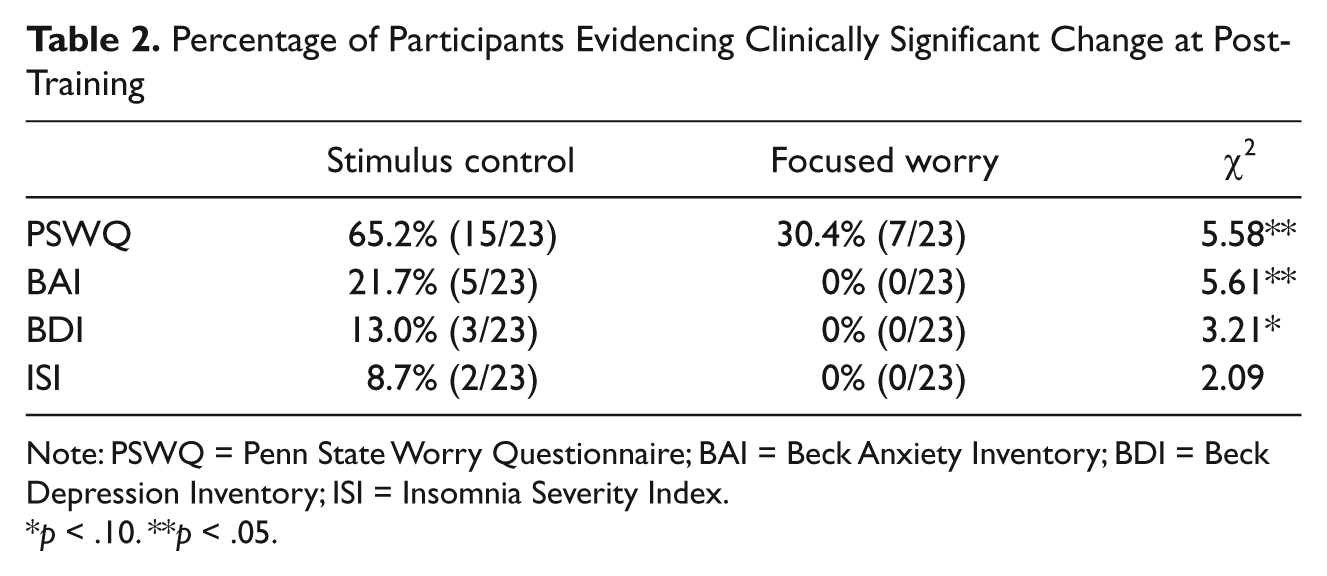
Note: PSWQ = Penn State Worry Questionnaire; BAI = Beck Anxiety Inventory; BDI = Beck Depression Inventory; ISI = Insomnia Severity Index.
p < .10. **p < .05.
Discussion
We examined the efficacy of SC training for individuals with high trait levels of worry. Participants were randomly assigned to receive 2 weeks of either SC training or a credible control training condition (FW) in which they were asked not to engage in avoidance of worrying, which otherwise leads to paradoxical increases in worry activity and its associated emotions. Results indicated that although participants in both training conditions evidenced significant decreases in trait worry and anxiety from pre- to post-training, this decrease was more pronounced among participants who received SC training. Thus, SC was efficacious in reducing worry suggesting that it is a viable treatment option for individuals who experience high levels of worry. Although these results warrant replication in a clinical sample, they provide preliminary support for the utility of incorporating SC procedures for worry into more comprehensive treatment packages for individuals with chronic worry. SC for worry has been cited as a potentially useful behavioral technique (Behar & Borkovec, 2005, 2009; Borkovec, Newman, & Castonguay, 2004). In addition to providing empirical support for this claim, our results further demonstrate that this technique can be obtained after a single treatment session and 2 weeks of practice (in contrast to Borkovec, Wilkinson, et al., 1983, who found beneficial effects after 4 weeks of practice). Thus, SC for worry is a relatively simple treatment to disseminate that helps individuals reduce their levels of worry and anxiety.
One plausible mechanism of change in SC training is increased stimulus specificity. Lang’s (1979, 1985) bioinformational theory states that a strong memory network expands (through rehearsal and new experiences that strengthen the fear) to build a coherent associative network. The more extensive this network, the greater the fear activation (i.e., emotional processing; Foa & Kozak, 1986) elicited on exposure to fear stimuli, and the greater the likelihood that specific, reliable cues will elicit that fear. Lang argues that the anxiety disorders are distributed along a continuum of affective memory defined by the extent to which emotional responses are elicited by specific and stable stimuli. He proposed that at one end of the continuum are specific phobias, wherein a single type of situation reliably activates the memory network and thus leads to an emotional response. At the other end of the continuum is GAD, wherein worry and anxiety are associated with a variety of stimuli and situations; this low specificity of stimuli means that the memory network is not reliably activated. In addition, Otto et al. (2007) found that trait worry predicts heightened fear conditionability, suggesting that individuals who experience high levels of worry in their everyday lives may also become more easily conditioned to external situations that elicit anxiety. Evidence suggests that individuals with GAD do indeed experience worry across multiple contexts (Craske et al., 1989), and this low specificity of stimuli may make successful treatment of worry especially difficult, given that it limits the degree to which emotional processing occurs during exposure (Foa & Kozak, 1986). SC training may reduce symptoms in part by increasing the specificity of situations that will elicit worry. Greater specificity in turn may increase emotional processing of fear cues, so that habituation of fear is more likely to occur.
Contrary to our hypotheses, neither conditions produced significant decreases in symptoms of depression. This is surprising given high rates of comorbidity between depression and GAD (see Mineka, Watson, & Clark, 1998), the strong association between worry and depressive symptoms (Andrews & Borkovec, 1988), and the tendency for symptoms of depression to abate in tandem with reductions in worry (Borkovec, Abel, & Newman, 1995). The lack of improvement in depressive symptoms likely points to the specificity of SC procedures in targeting a unique area of functioning. Unlike other treatments that show general improvements in symptomatic functioning, including reductions in depressive symptoms following treatment for worry (e.g., Borkovec & Costello, 1993; Butler, Fennell, Robson, & Gelder, 1991), SC training is targeted at reducing worry specifically by reducing the number of contexts with which it is associated. Furthermore, investigations finding decreases in comorbid depression following psychotherapy for GAD have incorporated various therapeutic tools (e.g., cognitive restructuring) that are likely to target mechanisms that are implicated transdiagnostically (e.g., maladaptive cognitions, core schemas) and are thus likely to influence symptoms other than worry. In contrast, SC training likely targets a much more circumscribed mechanism (i.e., conditioning of worry) and is thus unlikely to affect symptoms unrelated to that mechanism. Thus, although our results point to the potential specificity of SC training in targeting conditioning-relevant mechanisms and symptoms, its use in isolation may have limited value in achieving reduction of comorbid symptoms of depression. Rather, a more comprehensive cognitive-behavioral intervention is recommended for more generalized symptom reduction. It is important to note, however, that changes in depression symptoms may simply have not been evident at post-training. As the BDI asks participants to retrospectively report their depression ratings over the past 2 weeks (the same duration as the training period), more time might be necessary for the accurate examination of changes in symptoms of depression.
Given the strong association between worry and NA (Borkovec, Robinson, et al., 1983; Zebb & Beck, 1998), we also examined the impact of SC training on this construct. As hypothesized, SC training led to greater decreases in NA compared with FW training, but there was no significant change in PA for either training condition. This is not surprising, given that reduced PA is uniquely implicated in depression (Clark, Watson, & Mineka, 1994) but not in GAD (Brown, Chorpita, & Barlow, 1998), whereas increases in NA are implicated in both conditions (Brown et al., 1998). Furthermore, the SC condition’s lack of impact on PA is consistent with its lack of impact on symptoms of depression.
Given high rates of comorbidity between worry and insomnia (see Harvey, 2002), and given that worry is a common complaint among clients with sleep disturbance (Monti & Monti, 2000), we also hypothesized that SC training would lead to decreases in insomnia symptoms. As expected, there was a larger decrease in insomnia symptoms from pre- to post-training for participants receiving the SC intervention compared with participants receiving the FW intervention. It is noteworthy that the theoretical rationale for SC procedures for worry and insomnia are identical (i.e., to achieve increased specificity of stimuli that will elicit the maladaptive response), and SC procedures for worry were developed directly from Bootzin’s (1972) SC procedures for insomnia (Behar & Borkovec, 2009). In addition, for many chronic worriers, the bedroom is another external context associated with worry, which often leads to difficulty sleeping. Thus, as clients gain greater control over the incidence of their worry, it is likely that the association between worry and their bedroom will become weakened, thereby producing improvements in insomnia symptoms. Moreover, it is possible that instructions regarding worry postponement led participants to delay the worry that often occurs prior to sleep onset, thereby eliminating one process (worry) that interferes with the ability to fall asleep. These results point to the potential utility of including SC for worry in larger treatment packages for insomnia to target comorbid worry symptoms and potentially enhance the efficacy of Bootzin’s SC interventions that specifically target sleep.
In addition to finding that SC training was statistically superior to the FW condition on various measures, we also found that relative to the FW condition, a larger percentage of participants in the SC condition evidenced clinically significant change on measures of trait worry and anxiety. Although the percentage of participants evidencing clinically significant change in symptoms of anxiety (21.7%) and worry (65.2%) was modest to large, the rate of clinically significant change for depression (13%) and insomnia (8.7%) were small. These relatively low rates of clinically significant change in depression and insomnia symptoms provide further support for the specificity of SC for worry in targeting symptoms of worry and anxiety.
This investigation has several limitations that should be improved on in future studies. First, participants were not formally diagnosed with GAD, but rather they were recruited using cutoff scores on a self-report measure of trait worry (i.e., the PSWQ). Although we utilized a cutoff score that ensured that our participants had high levels of trait worry and that the mean of our sample had similar trait worry severity to individuals with diagnosed GAD (Molina & Borkovec, 1994), we cannot state with certainty whether these results would generalize to a population of individuals with formally diagnosed GAD. Future studies should examine the efficacy of SC training among diagnosed individuals. Second, the current investigation did not include follow-up assessments. Although the SC condition demonstrated superiority of worry, anxiety, and sleep-related symptoms at post-training, future studies should include follow-up assessments to examine whether such treatment gains are maintained over the course of time. Third, the present study was unable to control for the overall time spent worrying, thereby introducing the possibility that participants receiving FW training worried for more time per day relative to participants receiving SC training, and thus potentially accounting for greater severity of reported symptoms on measures of functioning.
Fourth, the FW condition contained some elements of existing treatment packages. Specifically, it contained an element consistent with mindfulness techniques. In addition, the instructions of the FW condition were similar in theory to a tenet of ACT, experiential avoidance (Hayes et al., 2006). The FW condition was not intentionally modeled after an ACT framework and did not include other aspects of ACT (i.e., cognitive diffusion, discussing values). As such, we do not suggest that the present study provided an empirical test of ACT or mindfulness techniques. Rather, the inclusion of these elements in the FW condition may have accounted in part for observed reductions in worry and NA among participants in this condition.
Fifth, although our results support the efficacy of SC training for worry, the multiple components comprising this intervention introduce rival hypotheses to explain the beneficial effects of the training procedure. Specifically, participants receiving SC training were instructed to delay worry to a later period, focus on the present moment, and worry actively in a prescribed place and time. It is therefore unclear whether treatment effects were due to the postponement of worry, the employment of mindfulness, or to the controlled incidence (i.e., SC) of worry. Because of the well-documented success of SC in the insomnia literature that does not include a postponement instruction (e.g., Espie, Lindsay, Brooks, Hood, & Turvey, 1989; Lacks, Bertelson, Sugerman, & Kunkel, 1983; Riedel et al., 1998), it is likely that the positive effects of this intervention on worry symptoms can similarly be attributed to the SC procedures themselves. However, a recent investigation (Verkuil, Brosschot, Korrelboom, Reul-Verlaan, & Thayer, 2011) found that participants who engaged in worry postponement for 2 weeks prior to receiving stress management therapy (SMT) evidenced greater decreases in anxiety and somatoform symptoms following SMT when compared with a waitlist control condition. Similarly, mindfulness-based procedures such as focusing on the present moment have been shown to lead to reductions in chronic worry and anxiety (Roemer et al., 2008).
Finally, a rival hypothesis for the relative success of SC condition is that use of the multiple components increased the efficacy of this intervention. Whereas the FW condition contained a single treatment component (focusing on worry), the SC condition contained four components. It is thus possible that the disparate number of treatment components could account for differences between groups. It is especially important that future investigations identify the active components of SC training by utilizing dismantling designs (e.g., SC vs. postponement of worry vs. SC + postponement of worry) to determine the exact components of SC training that are causative of symptom reduction.
Footnotes
Acknowledgements
We would like to acknowledge Shannon Stanfill for her assistance with data collection. We would also like to thank Robin Mermelstein, Stewart Shankman, and Brady Nelson for their comments on an earlier version of this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.