
Abstract
Posttraumatic stress disorder (PTSD) is associated with a wide range of risky behaviors (e.g., substance use and risky sexual behaviors); however, few studies have examined mechanisms that may underlie risky behaviors in this population. The present study utilized a prospective experimental design to examine the effects of emotion dysregulation and impulsivity on risky behaviors across time. Thirty women with sexual assault–related PTSD were randomly assigned to receive emotion modulation (EM), impulsivity reduction (IR), or healthy living (HL; comparison condition) skills trainings. Participants completed measures of emotion dysregulation, impulsivity, and risky behaviors pre-manipulation and 1-month post-manipulation. Participants in the EM and IR conditions reported a significant reduction in risky behaviors from pre- to post-manipulation relative to the HL condition. Changes in emotion dysregulation from pre- to post-manipulation fully accounted for reductions in risky behaviors over time. Results provide preliminary experimental support for the role of emotion dysregulation in risky behaviors.
Posttraumatic stress disorder (PTSD) is characterized by symptoms of intrusion (e.g., intrusive thoughts/memories and nightmares), avoidance (e.g., avoidance of trauma-related cues), alterations in cognition and mood (e.g., self-blame and restricted range of affect), and alterations in arousal and reactivity (e.g., hypervigilance and exaggerated startle response) in response to a traumatic event (American Psychiatric Association [APA], 2013). Notably, risky behaviors (defined as any behavior that puts one at risk for a negative outcome, be it physical, emotional, social, or financial; see Byrnes, Miller, & Schafer, 1999) were added as one criterion for PTSD in the fifth revision of the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; APA, 2013). Indeed, a burgeoning literature highlights the robust relationship between PTSD and risky behaviors. For example, individuals with PTSD have been found to be at heightened risk for alcohol and drug use (Epstein, Saunders, Kilpatrick, & Resnick, 1998; Shipherd, Stafford, & Tanner, 2005), antisocial and/or aggressive behavior (Booth-Kewley, Larson, Highfill-McRoy, Garland, & Gaskin, 2010; Monson, Fredman, & Dekel, 2010), binge eating and purging (Holzer, Uppala, Wonderlich, Crosby, & Simonich, 2008), deliberate self-harm (Gratz & Tull, 2012), and risky sexual behavior (Weiss, Tull, Borne, & Gratz, 2013), as well as negative outcomes associated with these behaviors, including revictimization (Messman-Moore, Ward, & Brown, 2009) and HIV (Hoff, Beam-Goulet, & Rosenheck, 1997). Notably, however, few studies have examined mechanisms that may underlie engagement in risky behaviors among individuals with PTSD. Two mechanisms worth investigating in this regard are emotion dysregulation and impulsivity.
As defined here, emotion dysregulation is a multi-faceted construct involving maladaptive ways of responding to emotions (regardless of their intensity or reactivity), including (a) a lack of awareness, understanding, and acceptance of emotions; (b) the inability to control behaviors when experiencing emotional distress; (c) lack of access to situationally appropriate strategies for modulating the duration and/or intensity of emotional responses to meet individual goals and situational demands; and (d) an unwillingness to experience emotional distress as part of pursuing meaningful activities in life (Gratz & Roemer, 2004; Gratz & Tull, 2010a). Research indicates that levels of emotion dysregulation are heightened among both clinical (Weiss, Tull, Anestis, & Gratz, 2013; Weiss, Tull, Viana, Anestis, & Gratz, 2012) and non-clinical (Tull, Barrett, McMillan, & Roemer, 2007; Weiss, Tull, Davis, Dehon, Fulton, & Gratz, 2012) populations with PTSD. The heightened negative affect that accompanies a PTSD diagnosis (Kashdan, Uswatte, Steger, & Julian, 2006) may make it more difficult for individuals with PTSD to modulate the intensity and/or duration of their emotions (Mennin, Heimberg, Turk, & Fresco, 2005). As such, individuals with PTSD may come to rely on emotionally avoidant regulation strategies (e.g., risky behaviors) that function to immediately reduce or distract attention away from aversive emotions (Heatherton & Baumeister, 1991). However, whereas risky behaviors may be effective in reducing distress in the short term, they are likely to exacerbate distress in the long term. For example, reliance on risky behaviors to escape emotional distress may reduce experiences in which the adaptive modulation of emotions is reinforced (Fischer, Smith, Spillane, & Cyders, 2005) and interfere with emotional processing (Foa & Kozak, 1986), thereby exacerbating levels of emotion dysregulation and PTSD. The negative consequences associated with risky behaviors may also contribute to the experience of more negative emotions (e.g., guilt, shame) that further drive emotionally avoidant regulation strategies. Moreover, because risky behaviors may ultimately result in a return and/or exacerbation of distress, individuals with PTSD may perceive themselves as having less access to effective emotion-regulation strategies.
Consistent with this literature, preliminary evidence provides support for a relationship between emotion dysregulation and risky behaviors, above and beyond other relevant risk factors for these behaviors (Gratz & Tull, 2010b; Tull, Weiss, Adams, & Gratz, 2012; Whiteside et al., 2007). Furthermore, among one cross-sectional study, emotion dysregulation has been found to account for the relation between PTSD and risky behaviors (Weiss, Tull, Viana, et al., 2012). Nonetheless, despite evidence for a relation between risky behaviors and emotion dysregulation, no studies to date have prospectively examined the unique contribution of emotion dysregulation to risky behavior among individuals with PTSD, above and beyond other relevant factors.
Impulsivity is one such factor that has been found to be heightened within PTSD populations (Joseph, Dalgleish, Thrasher, & Yule, 1997; Kotler, Iancu, Efroni, & Amir, 2001) and linked to risky behaviors (Eysenck & Eysenck, 1985; Whiteside & Lynam, 2001). As defined here, impulsivity refers to the tendency to act without forethought, predisposing individuals toward rash, unplanned actions without first considering the negative consequences or long-term effects of those actions (i.e., lack of premeditation; Eysenck & Eysenck, 1985; Whiteside & Lynam, 2001). Past research suggests that the greater physiological arousal found among individuals with PTSD (Gerardi, Keane, Cahoon, & Klauminzer, 1994) may contribute to their heightened levels of impulsivity (Joseph et al., 1997; Kotler et al., 2001). Indeed, the relation between arousal and impulsivity is well-documented (Barratt & Patton, 1983; Eysenck & Eysenck, 1985), and PTSD symptoms reflecting heightened arousal (e.g., irritability and sleep disturbance) are positively associated with impulsivity (Medeiros, Carvalho, Silva, Prado, & Prado, 2005; Stanford, Greve, & Dickens, 1995). Notably, impulsivity has also been found to be positively associated with involvement in a wide range of risky behaviors (Jones, Miller, & Lynam, 2011; Lynam, Miller, Miller, Bornovalova, & Lejuez, 2011; Simons, Maisto, & Wray, 2010; Stautz & Cooper, 2013; Verdejo-García, Bechara, Recknor, & Pérez-García, 2007).
However, recent cross-sectional studies highlight the relative importance of emotion dysregulation (vs. impulsivity) to PTSD and risky behaviors. For example, emotion dysregulation has been found to account for unique variance in PTSD above and beyond impulsivity and co-occurring substance use, mood, and anxiety disorders (Weiss, Tull, Anestis, & Gratz, 2013). Likewise, constructs that theoretically and empirically overlap with emotion dysregulation (e.g., urgency) have been found to evidence stronger associations with risky behaviors than impulsivity as defined here (Cyders & Smith, 2007, 2008). These findings suggest that involvement in risky behaviors among individuals with PTSD may be more strongly related to difficulties controlling behaviors in the context of emotional distress than a failure to reflect on the consequences of behaviors in general. Given these aforementioned findings, concurrent examination of the relative and unique contributions of emotion dysregulation and impulsivity to risky behaviors among individuals with PTSD is warranted.
The current prospective experimental study sought to examine the effects of emotion dysregulation and impulsivity on risky behaviors across time. Levels of emotion dysregulation and impulsivity were manipulated through instruction in specific skills (i.e., emotion modulation [EM] or impulsivity reduction [IR] modules, with a healthy living [HL] skills training module serving as a comparison condition). These relations were examined among a sample of women with sexual assault–related PTSD, given evidence of higher rates of PTSD (e.g., Kessler, Sonnega, Bromet, & Hughes, 1995), involvement in risky behaviors (e.g., Molnar, Buka, & Kessler, 2001), and levels of emotion dysregulation (e.g., Gratz, Bornovolova, Delany-Brumsey, Nick, & Lejuez, 2007) within this population (compared with individuals with exposure to other traumatic events).
We hypothesized that participants assigned to the EM condition would exhibit a significant reduction across a 1-month period in emotion dysregulation, whereas those assigned to the IR condition would report a significant decrease in impulsivity. In addition, given increasing evidence highlighting the emotion-regulating function of risky behaviors (Tull et al., 2012; Weiss, Tull, Viana, et al., 2012), we hypothesized that participants assigned to the EM condition would report the largest reductions in risky behavior over the 1-month period relative to all other conditions. Finally, we expected that changes in emotion dysregulation (but not impulsivity) would fully account for reductions in risky behaviors 1-month post-manipulation.
Method
Participants
The sample was composed of 30 African American women from an urban historically Black university in the southern United States who met criteria for sexual assault–related PTSD. Participants ranged in age from 18 to 28 years (M = 21.5 ± 2.89). Two thirds of the participants (67%) reported an annual family income less than US$30,000 and were not employed. The majority of participants were full-time students (87%) and single (70%). Twenty-three participants (77%) identified their sexual orientation to be heterosexual.
Experimental Manipulations
Skills presented during the EM and IR experimental manipulations were adapted from an empirically supported acceptance-based emotion-regulation group therapy (ERGT) for self-harm and other self-destructive behaviors among women with borderline personality pathology (Gratz & Gunderson, 2006; Gratz & Tull, 2011; Gratz, Tull, & Levy, 2013). ERGT has been shown to significantly reduce deliberate self-harm and other risky behaviors among women with borderline personality pathology (Gratz & Tull, 2011). EM and IR conditions covered material presented in single ERGT sessions and were adapted by author NHW (in collaboration with authors KLG and MTT) for use within this sample (i.e., the focus of the sessions was on strategies for modulating emotions and reducing impulsive behavior more broadly vs. focusing on deliberate self-harm in particular). Single ERGT modules targeted distinct factors (see Gratz & Gunderson, 2006) and did not overlap (see Table 1). The EM condition was comprised of strategies to modulate the intensity and/or duration of emotional arousal in a flexible, situationally appropriate manner, including distraction (i.e., noticing intense and/or aversive emotions and then temporarily directing attention toward something other than the distressing emotion) and emotional approach (e.g., getting in touch with emotions, allowing oneself to experience emotions, and paying attention to the information being provided by emotions). The IR condition taught skills for decreasing rash action and impulsive behavior, including distraction/delay (i.e., directing attention away from urges to engage in impulsive behavior as a means of allowing the urge to pass), behavioral substitution (i.e., replacing impulsive behaviors with healthier behaviors that serve a similar function), pros and cons (i.e., attending to the long-term consequences of impulsive behavior), and consequence modification (i.e., changing the contingencies of impulsive behavior by rewarding attempts to resist urges for impulsive behavior and eliminating rewards associated with engagement in impulsive behavior). Thus, the skills in the EM condition targeted the modulation of emotional responses (i.e., skills for effectively responding to intense emotions), whereas the skills in the IR condition focused on the control of impulsive behaviors (i.e., strategies for reducing urges to engage in impulsive behaviors). Notably, skills presented in the EM and IR conditions closely map on to our definitions of emotion regulation and impulsivity, respectively, such that EM skills targeted the flexible use strategies to modulate emotional responses to meet individual goals and situational demands, whereas IR skills aimed to increase awareness of the negative consequences and long-term effects of rash, unplanned actions.
Content of the One-Hour Emotion Modulation, Impulsivity Reduction, and Healthy Living Manipulations.

Consistent with recommendations (Christensen, 2004; Kazdin, 1998), a comparison condition was developed to control for the effects of self-awareness and monitoring on risky behaviors. The HL condition was comprised of strategies that target physical well-being (i.e., skills for improving diet and exercise; see Table 1). To reduce experimenter bias, detailed experimental manipulation scripts were developed for all three experimental conditions. Furthermore, author NHW was trained to adherence by authors KLG and MTT and served as the experimenter for all experimental sessions. All manipulations were provided to participants in an individual format. Weekly meetings throughout the study ensured experimenters did not deviate from the EM, IR, and HL manipulation protocols. A manipulation check was included to ensure validity of the experimental protocols (see results).
Measures
Screening measures
Potentially traumatic events (PTEs)
The Life Events Checklist (LEC; Gray, Litz, Hsu, & Lombardo, 2004) is a 17-item self-report measure designed to screen for direct or indirect exposure to PTEs in a respondent’s lifetime. The LEC has demonstrated convergent validity with measures assessing PTE exposure and psychopathology known to relate to traumatic exposure (Gray et al., 2004).
Unwanted sexual experiences
Sexual Assault Items (Belknap, Fisher, & Cullen, 1999) were administered to screen for the presence of unwanted sexual experiences. Participants were asked to provide yes/no answers for 10 items assessing a wide range of unwanted sexual experiences. Participants were eligible for inclusion in the present study if they endorsed one of the five items assessing rape (i.e., forced vaginal, oral, or anal sex, or forced penetration of the vagina or anus with digits or foreign objects) or sexual assault other than rape (i.e., unwanted touching, grabbing, fondling, or rubbing).
PTSD symptom severity
The PTSD Checklist-Civilian Version (PCL-C; Weathers, Litz, Herman, Huska, & Keane, 1993) is a 17-item, self-report measure of the severity of PTSD symptoms experienced in response to a PTE. In completing the PCL-C, participants were instructed to refer to the PTE they identified as most traumatic on the LEC or sexual assault supplementary items. Using a 5-point Likert-type scale (1 = not at all, 5 = extremely), participants rate the extent to which each symptom has bothered them in the past month. The PCL-C demonstrates excellent internal consistency and test–retest reliability in college students (Ruggiero, Del Ben, Scotti, & Rabalais, 2003). According to Blanchard, Jones-Alexander, Buckley, and Forneris (1996), a score of 44 or above on the PCL-C is indicative of a PTSD diagnosis (for evidence supporting the use of this cutoff score in college students, see Ruggiero et al., 2003). Internal consistency in the current sample was excellent (α = .97).
Diagnostic interview
Sexual assault–related PTSD
The Clinician-Administered PTSD Scale (CAPS; Blake, Weathers, Nagy, & Kaloupek, 1995) was used to assess for current sexual assault–related PTSD. This structured diagnostic interview assesses Criterion A traumatic exposure (i.e., sexual assault) and the frequency and intensity of the 17 Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; APA, 1994) PTSD symptoms. Frequency items are rated from 0 (never or none/not at all) to 4 (daily or almost every day or more than 80%). Intensity items are rated from 0 (none) to 4 (extreme). The CAPS has adequate interrater reliability (.92-.99), internal consistency (.73-.85), and convergent validity with the Structured Clinical Interview for DSM-IV Axis I Disorders (SCID-IV) and other established measures of PTSD (Weathers, Keane, & Davidson, 2001). For the purposes of the present study, and consistent with past research (see Blanchard, Hickling, Taylor, & Forneris, 1995), we utilized the Item Severity ≥ 4 (ISEV4) rule, which requires that at least 1 re-experiencing, 3 avoidance/emotional numbing, and 2 hyperarousal symptoms have a severity rating (frequency + intensity) of ≥ 4 to establish current PTSD. Participants were asked to refer to the experience of sexual assault that they endorsed as being most distressing when completing the CAPS. Internal consistency in the current sample was excellent (α = .94).
Primary outcome measures
Self-report and behavioral measures were administered before the experimental manipulation and 1-month post-manipulation.
Emotion dysregulation
The Difficulties in Emotion-Regulation Scale (DERS; Gratz & Roemer, 2004) is a 36-item self-report measure that assesses individuals’ typical levels of emotion dysregulation across six domains: non-acceptance of negative emotions, difficulties engaging in goal-directed behaviors when distressed, difficulties controlling impulsive behaviors when distressed, limited access to emotion-regulation strategies perceived as effective, lack of emotional awareness, and lack of emotional clarity. The DERS has been found to demonstrate good test–retest reliability (ρ I = .88, p < .01) and adequate construct and predictive validity (Gratz & Roemer, 2004; Gratz & Tull, 2010a), and to be significantly associated with objective measures of emotion regulation (see Gratz & Tull, 2010a). Items were recoded so that higher scores indicate greater emotion dysregulation, and a sum was calculated. Internal consistency in this sample was good for the overall scale (α = .96).
Impulsivity
The Urgency, Premeditation, Perseverance, Sensation Seeking, and Positive Urgency Impulsive Behavior Scale (UPPS-P; Cyders, Smith, Spillane, Fischer, Annus, & Peterson, 2007; Whiteside, Lynam, Miller, & Reynolds, 2005) is a 59-item self-report measure that assesses five dimensions of impulsivity. Participants rate the extent to which each item applies to them on a 4-point Likert-type scale (1 = rarely/never true, 4 = almost always/always true). The lack of premeditation scale was utilized in the present study. This scale demonstrates the greatest conceptual overlap with trait-level impulsivity as traditionally defined (Eysenck & Eysenck, 1985; Whiteside & Lynam, 2001). The validity of this scale has been established in relation to other personality traits (e.g., low conscientiousness) and risky behaviors (e.g., suicide and deliberate self-harm; Lynam et al., 2011; Whiteside & Lynam, 2001; Whiteside et al., 2005). Internal consistency in this sample was adequate (α = .81).
Subjective measure of past-week risky behaviors
The Impulsive Behavior Scale (IBS; Rossotto, Yager, & Rorty, 1998) is a 25-item, self-report questionnaire that assesses past-week engagement in risky behaviors (e.g., binge-drinking, unprotected sexual intercourse, impulsive spending, deliberate self-harm). Participants report the frequency of each behavior during the past week. Items are summed to create a measure of overall frequency of past-week risky behaviors. The IBS has been found to have adequate reliability and validity (Bender, Gordon, Bresin, & Joiner, 2010; Peñas-Lledó & Waller, 2001).
Behavioral measure of risk-taking propensity
The Balloon Analogue Risk Task (BART; Lejuez et al., 2002) is a behavioral measure of risk-taking propensity that requires participants to inflate a balloon model presented on a computer screen. Participants accrue money for each pump of the balloon in a temporary bank; however, the odds of the balloon “popping” increase with each pump of the balloon. When a balloon explodes, all money in the temporary bank is lost and the next uninflated balloon is displayed. At any point during each balloon trial, the participant can stop pumping the balloon and transfer the money from the temporary bank to the permanent bank. In the current study, 30 balloons (i.e., trials) were presented. Extant literature provides support for the validity of the BART. Specifically, the BART has been shown to be positively correlated with measures of related constructs (e.g., sensation seeking, impulsivity), as well as actual involvement in risky behaviors (e.g., substance use and risky sexual behavior; Lejuez et al., 2002). Consistent with scoring guidelines (Lejuez et al., 2002), the average number of pumps excluding balloons that exploded was calculated, with higher scores representing greater risk-taking propensity.
Skill use
Participants rated the frequency with which they thought about and used skills taught in their respective conditions 1-month post-manipulation on a 5-point Likert-type scale (0 = never, 4 = everyday). The following items were included: “How often did you think about the skills you had been taught in the previous month?” and “How often did you use the skills you had been taught in the previous month?” Ratings on this measure were included to ensure equivalence across experimental conditions in the potency of the manipulations.
Finally, all participants completed a demographics form assessing age, education, employment, sexual orientation, relationship status, and past-year family income.
Procedure
All study procedures were approved by the university’s Institutional Review Board. Screening for inclusion in this study took place in undergraduate psychology courses at Jackson State University. African American women (n = 88) aged 18 or older who provided written informed consent completed a brief questionnaire packet (see Measures). African American women met screening criteria if they (a) reported a history of sexual assault (70.1% of the screening sample) and (b) scored ≥44 on the PCL-C (Weathers et al., 1993; 64.5% of women reporting sexual assault). Participants meeting the screening criteria (n = 40) were invited to participate in the initial assessment. Of the 40 women who met screening criteria, 4 could not be reached and 1 withdrew interest. Thus, a total of 35 participants were scheduled for the initial assessment.
During the initial assessment (which lasted approximately 3 hr), participants were interviewed to assess for current sexual assault–related PTSD, and completed self-report and behavioral measures of emotion dysregulation, impulsivity, and risky behaviors (see Measures). Diagnostic interviews were completed by the first author (NHW), who was trained to reliability by a licensed clinical psychologist (MTT). All interviews were reviewed by MTT, with diagnoses confirmed in consensus meetings.
Participants who met diagnostic criteria for current PTSD (n = 32) were matched on pre-manipulation levels of emotion dysregulation, impulsivity, and past-week frequency of impulsive behavior and randomized to the EM (n = 10), IR (n = 11), or HL (n = 11) experimental conditions. All experimental manipulations (across EM, IR, and HL conditions) were scheduled within 14 days of the initial assessment (MEM = 8.50, SDEM = 0.81; MIR = 8.80, SDIR = 0.89; MHL = 9.50, SDHL = 0.87), provided by the first author (NHW), and lasted approximately 60 min (MEM = 63.40, SDEM = 6.31; MIR = 65.20, SDIR = 2.86; MHL = 61.00, SDHL = 7.36). Following provision of the experimental manipulation, participants were scheduled to complete the post-manipulation assessment 1-month later and provided with instructions for using the instructed skills outside of the laboratory (which included daily monitoring of both the strategies they used and the antecedents and consequences of skillful behaviors [EM and IR conditions] or exercise and food intake [HL condition]).
Follow-up assessments, which lasted approximately 1 hr, were conducted 1-month post-manipulation (mean days = 29.97 ± 3.42). During this assessment, participants completed the same self-report and behavioral measures they completed pre-manipulation (with the exception of the structured diagnostic interviews). Two participants did not complete the follow-up assessment (resulting in a final sample of 30 participants; 10 per condition). Participants were compensated financially (US$25) for their participation in each session.
Results
Preliminary Analyses
Data were first examined for outliers by investigating the presence of data points more than 3 times the interquartile range below the first quartile or above the third quartile for each of the primary measures (Tukey, 1977). No outliers were detected. Next, chi-square analyses and analyses of variance (ANOVA) were conducted on demographic factors, trauma-related variables, and pre-manipulation scores on the primary variables (i.e., DERS, UPPS-P, IBS, and BART) to determine equivalence across experimental conditions. Results indicated no significant between-group differences (see Table 2). To ensure equivalence across experimental conditions in the potency of the manipulations, chi-square analyses were conducted to examine between-group (EM vs. IR vs. HL) differences on items assessing whether participants had thought about and/or used skills from pre- to post-manipulation. No significant between-group differences were detected (χ2s < 5.39, ps > .05).
Analyses of Variance and Chi-Square Analyses Examining Between-Group (EM vs. IR vs. HL) Differences in Demographic Variables, Trauma-Related Characteristics, and Baseline Levels of Emotion Dysregulation, Impulsivity, and Risky Behaviors.
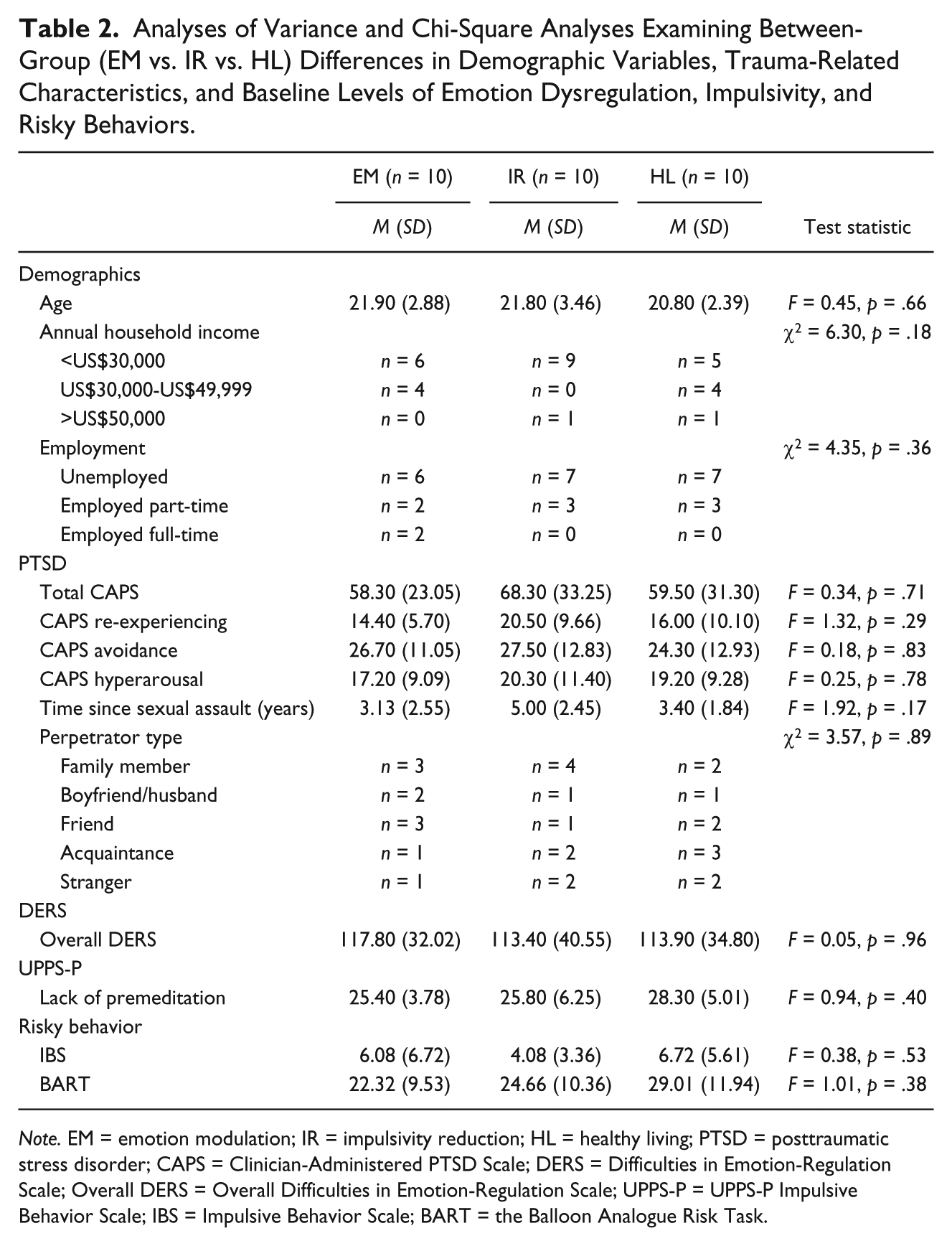
Note. EM = emotion modulation; IR = impulsivity reduction; HL = healthy living; PTSD = posttraumatic stress disorder; CAPS = Clinician-Administered PTSD Scale; DERS = Difficulties in Emotion-Regulation Scale; Overall DERS = Overall Difficulties in Emotion-Regulation Scale; UPPS-P = UPPS-P Impulsive Behavior Scale; IBS = Impulsive Behavior Scale; BART = the Balloon Analogue Risk Task.
Manipulation Check
To examine the validity of the experimental manipulations, a series of 3 (condition: EM vs. IR vs. HL) × 2 (time: pre-manipulation vs. 1-month post-manipulation) repeated measures analyses of variance were conducted to examine between-group differences in changes in emotion dysregulation and impulsivity over time (Table 3). Providing support for the experimental manipulations, results revealed a significant Time × Condition interaction for emotion dysregulation. Post hoc paired-sample t tests revealed that participants in the EM condition evidenced the greatest reduction in overall emotion dysregulation compared with both other conditions. Furthermore, although the time by condition interaction was not significant for impulsivity, findings did reveal a significant main effect of time on impulsivity, with larger effects detected in the IR condition (Cohen’s d = 1.62) compared with the EM or HL conditions (Cohen’s d = 0.97 and 0.82, respectively).
Repeated Measures Analyses of Variance and Post-Hoc Paired-Samples t Tests Examining Between-Group (EM vs. IR vs. HL) Differences in Emotion Dysregulation, Impulsivity, and Risky Behaviors at Pre- and Post-Manipulation.
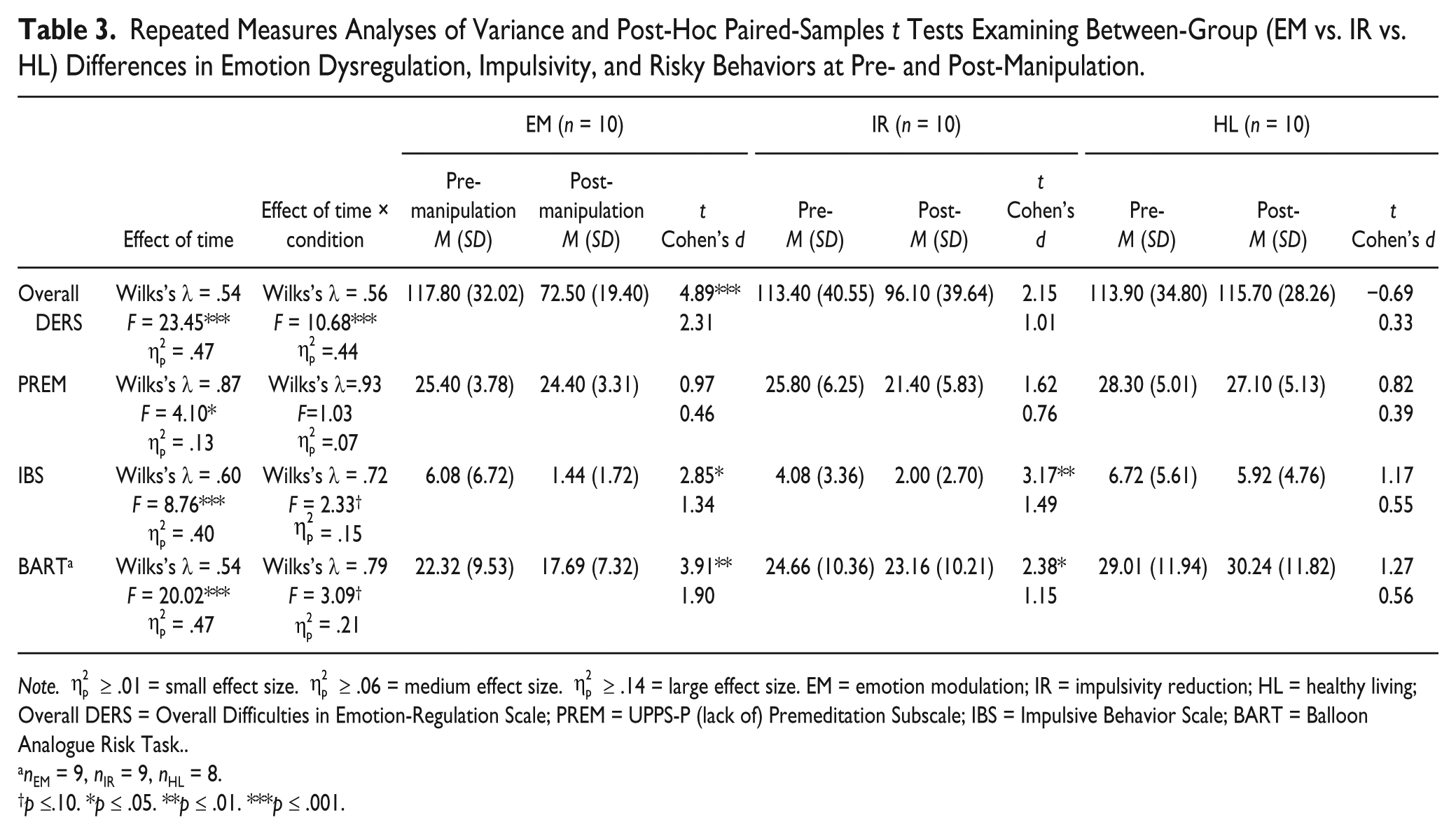
Note.
nEM = 9, nIR = 9, nHL = 8.
p ≤.10. *p ≤ .05. **p ≤ .01. ***p ≤ .001.
Primary Analyses
Two 3 (condition: EM vs. IR vs. HL) × 2 (time: pre- vs. post-manipulation) repeated measures ANOVAs were conducted to examine the effects of the EM and IR manipulations on changes in both past-week engagement in risky behaviors (i.e., IBS) and risk-taking propensity (i.e., BART) over time (Table 3). Of note, given our relatively small sample size, we did not apply an alpha correction to our analyses (for further discussion of problems associated with utilizing an alpha adjustment when conducting comparisons within a small sample, see Tutzauer, 2003). Results revealed a significant main effect of time on both past-week engagement in risky behaviors and risk-taking propensity (observed power > 0.97). Post hoc paired-sample t tests revealed that participants in the EM and IR conditions (but not the HL condition) evidenced significant decreases over time in both risky behaviors and risk-taking propensity. The Time × Condition interactions were not significant for either outcome; however, results of post hoc power analyses suggested inadequate power to detect interaction effects in these analyses (observed power was 0.57 and 0.54 for the IBS and BART, respectively).
Finally, we examined whether changes in emotion dysregulation and/or impulsivity accounted for the observed reductions in risky behaviors over time. First, residualized gain scores (Tucker, Damarin, & Messick, 1966) reflecting changes over time from pre- to post-manipulation were calculated for measures of emotion dysregulation, impulsivity, and risky behaviors. The residualized gain score for the measure of past-week engagement in risky behaviors was significantly associated with the residualized gain scores for emotion dysregulation (r = .55, p < .01), but not impulsivity (r = .01, p > .05). The residualized gain score for the behavioral measure of risk-taking propensity was not significantly associated with the residualized gain scores for emotion dysregulation or impulsivity (rs < 0.31, ps > .05). Therefore, subsequent analyses focused on the role of emotion dysregulation in past-week engagement in risky behaviors.
Following procedures outlined by Preacher and Hayes (2004), analyses were conducted to examine whether the residualized gain score for emotion dysregulation mediated the relation between experimental condition (the IV) and the residualized gain score for past-week engagement in risky behaviors (the DV). The bootstrap method was used for estimating the standard errors of parameter estimates and the bias-corrected confidence intervals of the indirect effects (see MacKinnon, Lockwood, Hoffman, West, & Sheets, 2002; Preacher & Hayes, 2004). The bias-corrected confidence interval is based on a non-parametric re-sampling procedure that has been recommended when estimating confidence intervals of the mediated effect due to the adjustment it applies over a large number of bootstrapped samples (Efron, 1987). The mediated effect is significant if the 95% confidence interval does not contain zero (Preacher & Hayes, 2004). In this study, 5,000 bootstrap samples were used to derive estimates of the indirect effect. Of note, the bias-corrected bootstrapping method is recommended for underpowered samples (Hayes & Scharkow, 2013), and has been shown to be an effective analytic strategy for assessing mediation in smaller samples when effect sizes are medium to large (see Fritz & MacKinnon, 2007). Analyses revealed that changes in overall emotion dysregulation fully accounted for the association between experimental condition and changes in past-week engagement in risky behavior (see Table 4).
Summary of Mediation Analysis (5000 Bootstrap Samples) Examining the Role of the Residualized Gain Score for Emotion Dysregulation in the Relation Between Experimental Condition (IV) and the Residualized Gain Score for Past-Week Engagement in Risky Behaviors (DV).
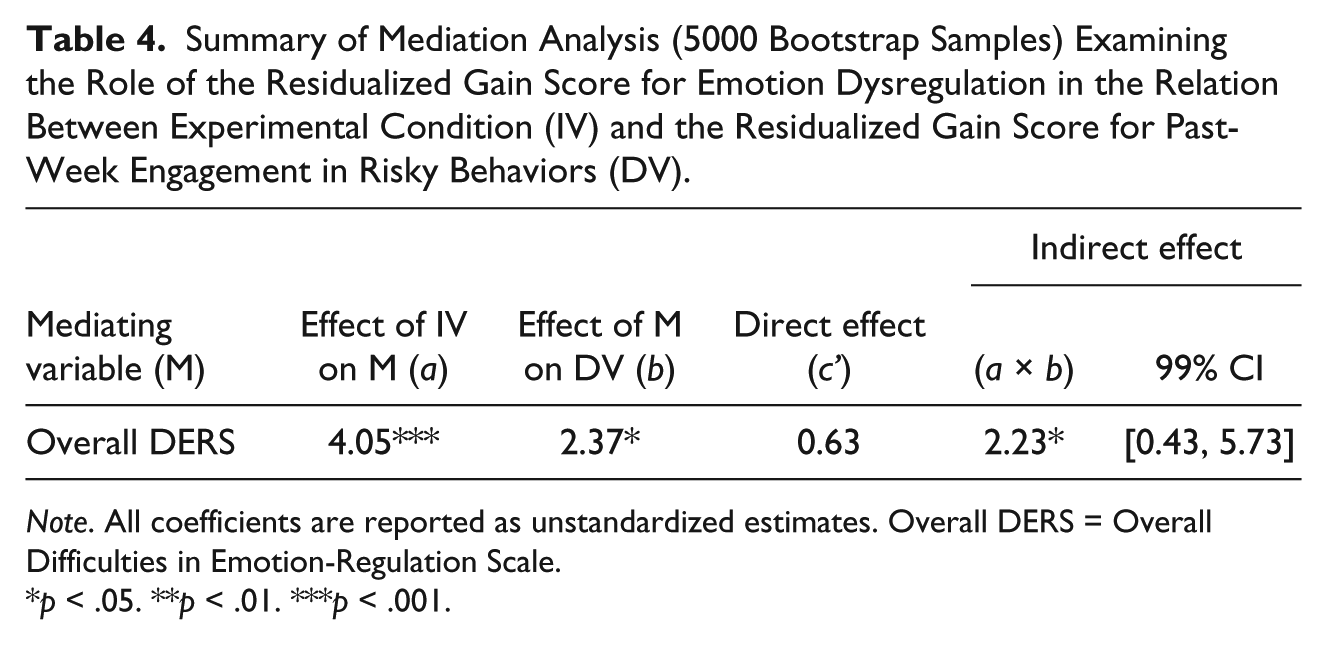
Note. All coefficients are reported as unstandardized estimates. Overall DERS = Overall Difficulties in Emotion-Regulation Scale.
p < .05. **p < .01. ***p < .001.
Discussion
The goal of the current investigation was to examine the effects of changes in emotion dysregulation and impulsivity on risky behaviors among women with sexual assault–related PTSD. To our knowledge, this is the first prospective investigation to examine the mediating roles of emotion dysregulation and impulsivity in engagement in risky behaviors among women with PTSD. Consistent with cross-sectional studies of PTSD populations (Weiss, Tull, Viana, et al., 2012), results of this study provide support for the underlying role of emotion dysregulation in risky behaviors among women with sexual assault–related PTSD. Specifically, changes in emotion dysregulation were found to fully account for changes in risky behaviors over time among the women in our sample. Consistent with emerging theoretical and empirical literature highlighting the emotion-regulating function of risky behaviors (Gratz & Tull, 2010a; Safer, Telch, & Chen, 2009; Weiss, Tull, Viana, et al., 2012), these findings suggest that emotion dysregulation (conceptualized here as involving maladaptive ways of responding to emotions, including difficulties controlling behaviors in the context of intense emotional states, deficits in the functional use of emotions as information, and non-accepting responses) may be relevant to our understanding of risky behaviors among women with sexual assault–related PTSD.
The results of this study highlight the potential utility of targeting emotion dysregulation in treatments aimed at reducing risky behavior in this population. Specifically, results of the present study suggest that teaching women with sexual assault–related PTSD skills for regulating their emotions, such as distress tolerance skills to facilitate behavioral control in the context of emotional distress (Dialectical Behavior Therapy; Linehan, 1993), mindfulness skills to promote emotional clarity and acceptance (Acceptance-based Behavioral Therapy for generalized anxiety disorder; Roemer, Orsillo, & Salters-Pedneault, 2008), and approach and distraction (vs. emotionally avoidant) strategies to modulate the intensity and/or duration of emotions (ERGT; Gratz & Gunderson, 2006; Gratz & Tull, 2011; Gratz et al., 2013), may result in a reduction in risky behaviors. Indeed, PTSD treatments targeting emotion dysregulation (e.g., Dialectical Behavior Therapy Prolonged Exposure [Harned, Korslund, Foa, & Linehan, 2012] and Skills Training in Affect and Interpersonal Regulation/Prolonged Exposure [Cloitre, Koenen, Cohen, & Han, 2002]) have been shown to reduce risky behaviors. Future research is needed to examine their effectiveness in reducing risky behaviors compared with other PTSD treatments and across more diverse populations with PTSD (e.g., with regard to gender, race/ethnicity, diagnosis, and trauma type).
Importantly, results of the current study also highlight the potential utility of brief intervention efforts targeting a reduction in risky behaviors among women with sexual assault–related PTSD. A growing number of studies have examined the impact of brief interventions for reducing risky behaviors. For example, preliminary findings of Baer, Peterson, and Wells (2004) and Monti et al. (1999) highlight the utility of brief (i.e., 35-40 min [Monti et al., 1999] and 2 hr [Baer et al., 2004]) motivational interviewing interventions in reducing substance use and alcohol-related risk, respectively. Notably, however, a dearth of literature has examined brief interventions targeting risky behaviors among individuals with PTSD in particular. As such, future research would benefit from exploring the efficacy of brief prevention and intervention efforts for reducing risky behaviors in this population.
Although the results of the present study add to the growing body of literature on the mechanisms underlying risky behaviors among individuals with PTSD, several limitations must be considered. First and foremost, given the preliminary nature of this study, the sample size was small, limiting both our statistical power and the statistical conclusion validity and generalizability of our findings. Most notably, the present study lacked adequate statistical power for analyses of some of the interaction effects, suggesting that non-significant findings should be interpreted with caution. Furthermore, although we sought to minimize experimenter bias by utilizing standard scripts for all experimental manipulations, it is possible that experimenter bias may have influenced the delivery of the information in the scripts. Replication of these findings in larger samples of individuals with PTSD is needed. In addition, although a growing body of theoretical and empirical literature suggests that emotion dysregulation may underlie risky behaviors (Tull et al., 2012; Weiss, Tull, Viana, et al., 2012), it is also possible that this association is bidirectional, with regular involvement in risky behaviors leading to or exacerbating emotion dysregulation. Larger-scale prospective investigations may improve our understanding of the interrelations of risky behaviors and emotion dysregulation over time. Likewise, studies utilizing experience sampling methods may provide further evidence of the emotion-regulating function of risky behaviors.
An additional limitation is the exclusive reliance on self-report measures of emotion dysregulation and impulsivity, responses to which may be influenced by an individual’s willingness and/or ability to report accurately on emotional and behavioral responses. Future studies would benefit from the multimodal measurement of emotion dysregulation and impulsivity. Similarly, participants’ willingness or ability to report accurately on their engagement in risky behaviors may have been limited given the potential stigma associated with many of these behaviors. Nonetheless, there is evidence that self-report measures may provide more valid reports of risky behaviors than other assessment methods (e.g., interviews; Fenton, Johnson, McManus, & Erens, 2001; Johnson et al., 2000), and the self-report and behavioral measures of risky behavior in this study were significantly positively correlated.
Furthermore, although examination of the mechanisms underlying risky behaviors among African American women with PTSD is a strength of this study, it is unclear whether these findings are generalizable to individuals with PTSD in general or unique to African American women in particular. There is some evidence to suggest greater PTSD symptoms (Davidson, Price, McCauley, & Ruggiero, 2013), greater emotion dysregulation (Gross & John, 2003), and higher rates of some forms of risky behaviors (e.g., risky sexual behavior and deliberate self-harm; Dariotis, Sifakis, Pleck, Astone, & Sonenstein, 2011; Gratz et al., 2012; Pflieger, Cook, Niccolai, & Connell, 2013) among African American versus White women. Importantly, however, although research to date has not directly explored the moderating role of race/ethnicity in the mediation model proposed here, there is no evidence to suggest that the strength and direction of the relations among PTSD, emotion dysregulation, and risky behaviors vary as a function of race/ethnicity (Tull et al., 2007; Weiss, Tull, Anestis, & Gratz, 2013; Weiss, Tull, Viana, et al., 2012). Indeed, extant research highlights the underlying role of emotion dysregulation in risky behaviors across mixed-gender/race samples with exposure to a variety of traumatic events (e.g., Weiss, Tull, Viana, et al., 2012). Together, this research suggests that findings of the present study may generalize to other populations with PTSD. Nonetheless, findings require replication within more diverse groups of individuals with PTSD, including clinical samples with PTSD resulting from other forms of traumatic exposure and larger, mixed-gender and ethnically diverse samples.
Future investigations would also benefit from examining the extent to which the observed associations between risky behaviors and both emotion dysregulation and impulsivity are accounted for by trauma-related variables not assessed in the current study. One variable that may be particularly important to examine in this regard is cumulative trauma, given evidence of a strong association between emotion dysregulation and revictimization (e.g., Messman-Moore, Walsh, & DiLillo, 2010; Messman-Moore, Ward, & Zerubavel, 2013). In addition, the present study did not examine PTSD symptoms prospectively; thus, research examining the interrelations among PTSD symptoms, emotion dysregulation, and risky behaviors across time is needed. In particular, given evidence of elevated rates of sexual assault among African American (vs. White) college women (Abbey, Ross, McDuffie, & McAuslan, 1996; Koss, Gidycz, & Wisniewski, 1987), future research would benefit from further examination of the interplay of emotion dysregulation, PTSD, and risky behaviors following sexual assault among African American women in particular.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research described here was supported, in part, by a grant from the National Institutes of Health (T32DA019426).