
Abstract
☑ Earn CEs Online
by answering questions on this article.
For more information, visit:
http://my.aerbvi.org/AER-Store/Publications/BKctl/ViewDetails/SKU/AER
Vision impairment and blindness are significant causes of disability and contribute to high health care expenditures in the United States (Frick & Singman, 2019; McLaughlin et al., 2017). National Academies of Science, 2016). Approximately 15 to 20% of vision impairment cases and 5 to 10% of blindness cases are caused by eye injuries (Swain & McGwin, 2020). Although traumatic eye injuries can have a far-reaching impact on an individual and society, traumatic eye injury has not been a focus of research in nonmilitary populations.
Research has demonstrated associations between progressive vision loss and disability, including decreased mobility and subsequent injury, as well as impaired mental and cognitive functioning (Bittner et al., 2010; Cimarolli et al., 2016; Ekici et al., 2015; Mangione et al. 1998; Nelson et al. 1999; Rovner et al., 2002; Lisboa et al., 2013; National Academies of Science, 2016; Richman et al., 2010; Vu et al., 2005). Few studies, however, have examined the effect of acute traumatic vision loss on quality of life and functioning in nonmilitary populations. This study fills this knowledge gap by examining individuals’ experiences after acute traumatic vision loss and their recommendations for services that would be useful after hospital discharge. The goal is to identify the needs of individuals as they transition home from the hospital to inform the development of services and other resources that could improve their care experience and long-term outcomes.
Methods
We used a qualitative approach to conduct semi-structured interviews with individuals who had experienced acute traumatic vision loss. All English-speaking patients who were aged 18 years and older and were treated in either the emergency department (ED) or inpatient unit at a specialty eye hospital for a traumatic eye injury leading to acute vision loss in the previous 2 years were eligible for participation. Traumatic eye injury was defined as injury to the eye from a foreign body or object or unknown internal process resulting in acute vision loss. All patients received the same level of care at the specialty eye hospital including: (1) assessment of vital signs and visual acuity; (2) external face and eye exam and slit lamp examination of both eyes; (3) measurement of intraocular pressure, both eyes; (4) full dilated exam (unless contraindicated), both eyes; (5) ocular ultrasound if no clear view of fundus (unless contraindicated); and (6) computerized tomography (CT) scan of face and head. We used a two-year range in time since injury to elicit a broad range of perspectives from participants. A hospital utilization coordinator identified a convenience sample of potentially eligible patients from medical records. We also queried the hospital’s electronic medical record system to identify patients treated for a globe rupture. We contacted all potential participants by telephone to assess their interest in participating in the study. Enrollment continued until thematic saturation was reached.
Data Collection
We developed a semi-structured interview guide, with questions about participants’ experiences post-discharge and the impact of the eye injury on functioning and quality of life (see Box 1). We refined the guide after administration to four participants to improve clarity and to ensure that the questions were broad enough to capture participants’ unique experiences. Interviews were conducted by telephone by three researchers between May and December 2019. Verbal consent was obtained prior to each interview, and participants were compensated $25 for participation. Interviews ranged in duration from 13 to 51 minutes. Participants also completed a demographic survey and the National Eye Institute Visual Functioning Questionnaire–25 (VFQ-25; Mangione et al., 1998). Audio recordings were sent to a transcription agency. Participant-identifying information was removed from the transcription files and transcripts were stored on a password-protected computer. Study approval was obtained from the university’s institutional review board.
1. Please tell me about your vision loss. a. What was the cause of your vision changes? b. How did your life change after experiencing vision loss?
2. Talk about what happened when you were discharged from the hospital after your visual loss. a. How did you feel? b. What needs or worries do you remember having at that time of discharge? c. What materials or resources were you given? d. What other help would you like to have received? (materials, education, etc.)
3. What were the most surprising or unexpected things that happened when you came home? a. What tasks became more difficult to complete? b. What become inconvenient to do? c. What activities were less enjoyable after vision loss? 4. How did social interactions change after your vision loss? a. After the vision loss, did you notice any changes in the relationships you had? b. Did you notice changes when interacting with strangers? 5. How has your quality of life been affected since your vision loss? a. Economic burden, Feeling physically unhealthy, Feeling mentally unhealthy, Activity limitation b. Some studies have shown that people with vision loss experience greater levels of dissatisfaction in life. Does that feel accurate for you? We are aware that a sudden loss of vision can be challenging in many ways, both physically and mentally. We also know there are different ways people cope with such an unexpected change in their life and we’d like to hear more from you about what that part of the experience was like. 6. How have you coped with your loss of vision? a. What helped you cope with your vision loss? b. What kind of support would have been helpful? c. Did your vision loss change anything about the way you deal with stressful situations? d. Did you develop any specific coping mechanisms to deal with the vision loss? 7. What things do you wish your doctors or health care providers had offered you? 8. What types of emotional support did you find most helpful? a. What other types of support did you want or need? 9. When thinking about the future, what fears or worries do you have? (Optional, if time) We’ve talked about many of the challenges and needs people have when they experience vision loss. What do you think are the most important resources or services we could recommend to people who have just experienced acute vision loss? 10. Is there anything we haven’t talked about that you think we should know about?Box 1. Interview Guide.
G
D
I
C
Data Analysis
A member of the research team reviewed transcripts for accuracy. Discrepancies with the audio recording were corrected and transcripts were imported into NVivo 12
qualitative research data-analysis software (QSR International, 2018). We used an iterative axial coding process in which the development of codes began after the first set of transcripts was received. The research team read the first three transcripts and developed individual lists of preliminary codes to capture important concepts that emerged from the data. To ensure the coding scheme was grounded in the data and consistent in meaning, codes were systematically developed and defined until consensus was reached and a final codebook was established. All transcripts were coded using the consensus categories. Inter-rater reliability was periodically confirmed using kappa coefficient and percentage agreement. Demographic data and responses to the VFQ-25 (Mangione et al., 1998) were summarized using descriptive statistics.
Results
Participant demographics (N = 26).

aResponses do not equal 26 because participants marked all that apply.
Causes of acute vision loss, self-reported visual acuity, and prior experience with an eye injury or problem.
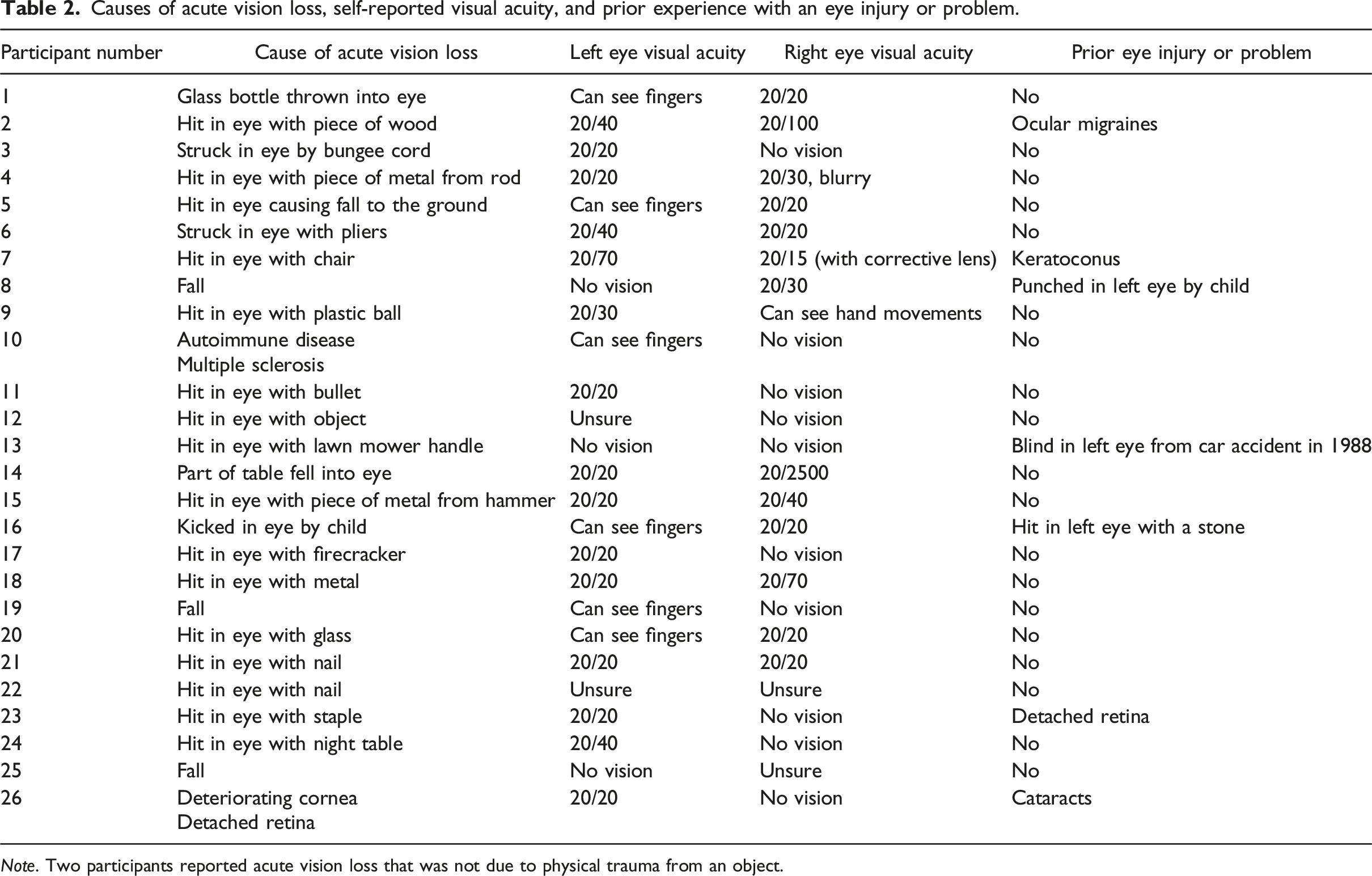
Note. Two participants reported acute vision loss that was not due to physical trauma from an object.
Visual functioning questionnaire-25 (N = 26).
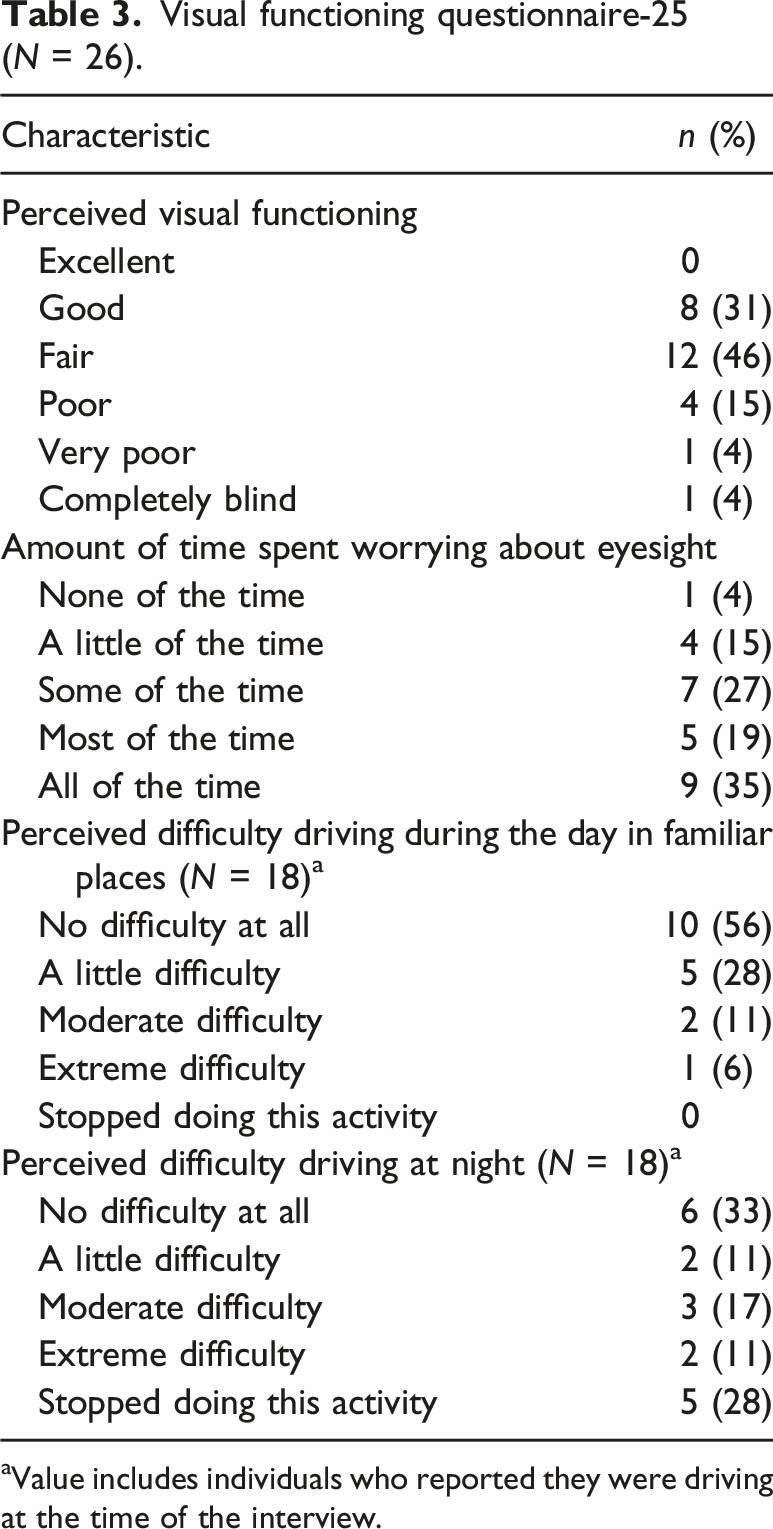
aValue includes individuals who reported they were driving at the time of the interview.
Informational Needs
Regarding the transition home from the hospital, several participants wanted more information from providers about what to expect over time. A few participants mentioned not being prepared for the severity of pain experienced. Participant two stated, “I did not expect the pain to be as bad as it was, and I have a pretty high threshold.” Some participants expressed frustration that providers did not answer their specific questions. Participant 17 stated, It was very wishy-washy. Oh, I don’t know. It could happen or that might work—it was never a good solid answer. And I’m one of those people, I completely understand no two cases are the same. But, there should still be a ballpark of stuff, like oh, we’ve had patients in the past that have done this.
Similarly, participant 3 noted, It seemed like everybody was tiptoeing around the fact that it’s a possibility I might lose my eye. They just kept saying well, we’ll see what happens. We’re going to try—we do a lot of things here and we save a lot of people’s eyesight and it may or may not be back to 100 percent , but we’re going to do the best we can.
Finally, participant 20 identified the need for providers to use lay terms, At some points with the doctors, I was like, what’s going on? And then sometimes, they would say stuff and it was clearly above my head. If they could dumb it down and explain it a little bit more as to what’s going to happen (that would be great).
Some participants were dismayed with the lack of material information provided. Many identified a desire to understand more about the eye injury and the corrective procedures undertaken. Participant 17 noted, So I really wasn’t given much (information). After I left the hospital, my ocularist suggested a book that I read which was recommended to me for depth perception. There were no pamphlets given out—honestly, the lack of information in general that is given out was pathetic.
Other participants wanted reading material about vision loss, anatomy of the eye, pain management, medication education and eye drop administration, and protection of the eye.
In addition to identifying the need for more information, patients discussed different ways they would like to receive guidance once at home. Participant 14 suggested having a coach, You know how people have a coach to tell them how to eat healthy? People can have a coach that can tell them this is what’s happening, this is what you’re going do for the first day and this is what you’re going to experience the first day, if you don’t do this.
Another participant found it helpful to receive texts and follow-up telephone calls from his physician.
Functional Needs
Participants noted significant struggles with daily functioning after their eye injuries. Participant 17 shared challenges related to weight restrictions in lifting: I had a limited weight restriction—you don’t have many abilities when you’re first discharged— when you get back to normal everyday life that is the issue, trying to go back to work and do the job you once did or get back in your car and try to drive.
Activities that were previously second nature became more challenging for many participants. Participant 14 lamented, Life changed a lot. I couldn’t write or read. I couldn’t go on the—you know how the Internet is always now second nature for everybody. I couldn’t read texts or emails. I had to enlarge everything. Even with enlarging, I couldn’t read through the glow—it’s painful.
Other participants discussed the effect of changes in depth perception on their daily activities. As participant 11 lamented, Putting the toothpaste on the toothbrush, I would miss the toothbrush every (time). Things that I would never even have thought about before ever being an issue (were a problem). Cooking. I’d try to crack an egg and put it in a cup, and I’d miss the whole cup.
Similarly, participant 23 shared, It was a lot harder to get around—you don’t really realize how much you really need both eyes to go through day to day activities. So even trying to pour a glass of water was more difficult because I couldn’t see out of the one side so I always had to have everything on one side so I could see it.
Difficulties with driving were highlighted as an significant challenge. Participant 26 described apprehension about driving for the first time after the injury, Driving, for instance, I didn’t wanna drive at all. Today was the first day and I was out. I did a trial run (driving). It was a straight drive. I was very careful. I would not have anybody else in the car with me at this point. I’m behind the wheel and I’m supposed to feel safe myself. But, as long as I’m around places that I’m familiar with, I think I’ll be okay until I know what’s gonna happen with my vision.
Others identified activities that became more difficult including grocery shopping, going to the bank, using the computer, cutting the grass, riding a bicycle, and reading.
Participants consistently identified the importance of having a person to assist with eye care (e.g., placing eye drops) and other activities of daily living (e.g., showering). Some participants found it difficult to depend on people for their basic needs, while others accepted dependency as part of recovery. Participant 19 stated, I needed to find somebody to do my grocery shopping for me, because I do it online. But somebody has to come here and put it through (the computer) for me. My bills—I have to have somebody pay those. They’re just things that I would have ordinarily done that I have to have somebody do for me now.
Participant 22 noted, “I was not able to go back to work for a couple weeks, I had to hire a driver. I wasn’t really allowed to do anything.”
Multiple participants talked about how their inability to work led to significant emotional and financial stress. As participant 5 lamented, I don’t wanna say I always have an answer, but for the first time I really didn’t have any answers to give. I didn’t know where—like I said, where any money was gonna come from. I didn’t even know when I would be able to work again.
Participant 26 explained that they felt stressed:
Stressed, not knowing what’s gonna happen. I have no control over this. And I try to read up on it—it’s just so confusing. And I can only read so much, because I get tired, and then the screen puts me in a whirl spin of, oh my God, I’m supposed to go back to work, I still can’t see. I work with computers and I can’t even look at my screen on the phone.
Although the majority of participants identified significant changes in their lives, a few noted that their lives did not change drastically, which seems to be related to the extent of vision loss. Participant 10 said, I can’t really say that I’ve had major changes though. At this point, I haven’t. I couldn’t imagine if I lost more of the vision. But what I can see of, I still—I’m still trying to function as a normal person.
Although a few participants mentioned that it would be helpful to receive assistance with transportation to appointments and finding a job, the majority focused on a desire to receive occupational and physical therapy. Participant 11 noted, I wasn’t told I had to do any physical therapy or anything like that post-leaving the hospital…(M)aybe telling people or giving people resources to places to go to help with the depth perception and those things that I was having a lot of trouble with at first. That would totally be very helpful after the first week of being back at home.
Participant 12 emphasized the need for physical therapy in the absence of having a support person available to help: Physical therapy for people who lose their vision in a sense of—I know it’s hard adjusting to not be able to see this way or look that way—having to turn your head all the time. And took me working on stuff like peripheral vision and how far can I see that way—my wife helping me and stuff like that. But, everybody doesn’t have that person there to help them.
Psychosocial Needs
Participants uniformly expressed concerns, fears, and uncertainty about the future, which caused emotional distress. Participant 11 emphasized stress related to not knowing if he was going to lose his eye: After the surgery they were like, if you get some really, really bad pain, that means your eye’s just dying off back at the nerve and we’re going to have to take it out.... So that was kind of nerve-wracking to go home and not really know what to expect.
Participant 2 brought up the concern of the effect of her vision loss on her ability to have children, So this fear only just came up the other day, which is eventually when I want to start having kids, is it going to be a risk having a child, like with the pressure and everything else, like am I going to have to schedule a C-section? My concern is just around the eyesight in the future.
Social and emotional support were important during recovery. Some participants were unable to fathom not having a support system to assist with their transition. Participant 17 said, “I can’t imagine losing vision and having nobody around and having to do it myself. That would’ve been terrible.” Participant 27 expressed the importance of understanding and compassion in the context of acute vision loss, I don't mean this as a derogatory remark, but I got the opinion that the doctors knew what they were doing and they handled it very, very well and I got the very best care I could've possibly had, but the emotional part seemed to be a little lacking.
Although uncertainty related to prognosis and function was worrisome to almost all of the participants, a subset of participants experienced significant mental health distress as a result of their injuries. Participants described severe depression, anger, and isolation. They used phrases such as “I was very afraid,” “I felt helpless,” and “It was a real dark time.” Participant 17 said, “(It) feels like I’m having a heart attack every day of my life” to describe their emotional states. Some participants disclosed how their mental health impacted their daily life. Participant 5 said, I (had) a sense of disappointment because I felt as though I let my family down. I couldn’t provide for them. I was down on myself a lot. I shut myself off pretty much from everybody. I didn’t wanna talk about it.
Likewise, participant 12 said, “I didn’t want to be bothered. I just wanted to stay in the room. Because I felt like little stuff that I love to do, I couldn’t even do.”
Some participants noted that they would have wanted access to professional mental health services that were not offered. Participant 24 shared the difficulty he experienced trying to obtain such support, Psychological support is not the easiest thing to obtain. My family doctor told me to get cognitive behavioral therapy. But, to try and get a doctor to do that on Medicare is almost impossible. We made 20 calls from the list and we had three callbacks just to tell us that they don’t accept my insurance.
Other participants echoed the need for mental health services stating, including participant 27, who said, “It would have been nice to have someone to talk to about this instead of figuring it out on my own.” Participant seven noted that he was able to cope with vision loss, but said, “I think a lot of people would have a difficult time with that. So counseling might be a good thing.”
In addition to interest in professional mental health services, participants discussed a desire for peer support and support groups. Discussing peer support, participant four suggested, I guess just talking to other people that have had [vision loss would have helped]. I know a couple of friends that have had detached retinas or an infection of the eye, and I would just ask them, how long is it going to take? And they said it always took months to go away. It's nice to know from somebody else that it got better for them.
Another participant offered to share his telephone number with people who experience vision loss. Similarly, some participants thought it would be helpful to have support staff members to talk with over the telephone or someone to remind them about an upcoming appointment or to follow up if an appointment was missed.
Several participants suggested having support groups for people who have experienced vision loss. Participant 2 stated, One of the things that might be helpful is finding a group of people who also have had eye injuries, just to share their experiences and what they expected—to hear from people who have had severe injuries and where they’re at—because unless you have it happen to you, you don’t know what to expect afterwards.
Participant 9 echoed a similar sentiment about having a support group: “to be able to be around other people that are going through something similar to what you’re going through. They can relate to it more than somebody else that’s never been through it.”
Discussion
To our knowledge, this is the first study to explore the needs of individuals who experienced acute traumatic vision loss and to identify their suggestions for addressing those needs. Findings suggest that individuals with an acute traumatic eye injury have considerable unmet informational, functional, and psychosocial needs. Individuals who experienced acute eye injury had numerous informational needs including wanting to know about the eye injury and corrective procedures and expectations for the course of recovery, and needing to hear this information in understandable lay terms. These findings about the need for use of lay language are consistent with research that has identified the use of medical jargon as a hindrance to patient-provider communication across health care settings (Thomas et al., 2014; Ross et al., 2017).
Regarding the perceived lack of sufficient information at discharge, these findings are supported by a literature review that found that patients discharged from EDs perceived that they received inadequate information from providers (Roh & Park, 2016). In addition, the specific types of information patients discussed needing parallel those that have been identified as important for a high-quality ED discharge: discharge diagnosis, prognosis, treatment plan, and expected course of illness (Body et al., 2015; Hoek et al., 2020; Johns Hopkins University, 2014). Providers can play an integral role in addressing patients’ informational needs through skillful communication avoiding medical jargon and setting expectations for recovery. Further, providers could engage in discussions during discharge as well as subsequent outpatient visits about the impact of vision impairment on quality of life (Sleath et al., 2017).
The functional needs of persons who experienced acute injury are similar to those of persons with glaucoma and other diseases that cause progressive vision loss including difficulty with daily activities and self-care (Mangione et al. 1998; Nelson et al., 1999). Both unilateral and bilateral vision impairment have been associated with difficulties with activities of daily living and increased dependence on others (Stevelink et al., 2015; Vu et al., 2005). Participants in this study offered suggestions for addressing their functional needs including assistance with transportation to appointments, physical therapy, and occupational therapy.
Low vision rehabilitation has been found to have potential to improve the quality of life and adaptation to vision impairment (Frick & Singman, 2019; McLaughlin et al., 2017; National Academies of Science, 2016). A study by Stevelink et al. (2015) found that the majority of former military personnel used low vision devices including a white cane and a dog guide. Additionally, findings from a study of older adults with age-related vision changes suggest that vision rehabilitation services fostered the use of new coping skills and improved adaptation to vision impairment (Brennan & Cardinali, 2000). Unfortunately, services such as low vision rehabilitation were not routinely offered to the study participants.
Finally, our sample with acute eye injuries experienced fear and uncertainty about the future, which caused significant emotional distress. The high levels of mental distress experienced by participants in this study are consistent with research on individuals with disorders that result in progressive vision loss (Bittner et al., 2010; Brown et al., 2000; Cimarolli et al., 2016; Mangione et al. 1998; National Academies of Science, 2016; Rovner et al., 2002). Similarly, Stevelink et al. (2015) found that former military personal who sustained vision loss also experienced mental health distress including depression and social withdrawal. Participants in this study suggested that a recovery coach, peer support, support groups, and mental health services would be beneficial for addressing their psychosocial needs. Despite the participants’ interest in these services, they were not offered routinely.
Our findings point to a significant gap in the services that are available to meet the needs of individuals with acute traumatic eye injuries. This work has far-reaching implications for providers since it supports the need for the development and delivery of integrated interventions that include emphasis on addressing psychosocial and functional aspects of recovery. Findings should be considered in light of the study limitations. Our sample was limited to individuals treated in a single specialty eye hospital in a large city. In addition, our response rate was low, with only 20% of individuals contacted agreeing to participate, which limits generalizability of findings. Further, recall bias likely prevented some participants from remembering education they received and materials that were provided at discharge. Finally, the inherent biases of researchers may have influenced analysis. To minimize bias, a researcher not involved in data collection or coding reviewed the data interpretations. Despite these limitations, our work is novel in exploring patients’ needs after acute traumatic eye injuries and providing potential interventions that can improve patient outcomes. Future research is needed to test the effect of an integrated-care model that includes routine offering of psychosocial and functional services for patients with acute vision loss to determine the effect on outcomes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.