
Abstract
Keywords
☑ Earn CEs Online
by answering questions on this article.
For more information, visit:
http://my.aerbvi.org/AER-Store/Publications/BKctl/ViewDetails/SKU/AER
Cortical or cerebral visual impairment (CVI) is a brain-based visual impairment and the leading cause of bilateral visual impairment in children in high-income countries (Chang & Borchert, 2020; Weinstein et al., 2012). Children with CVI have difficulty processing visual information, which can lead to delays in the child’s learning and development, as well as difficulties in areas of occupation such as self-feeding, playing, dressing, learning, crawling, and exploring the environment (Good et al., 2001; Lueck et al., 2019). Occupational therapists and teachers of students with visual impairments are two groups of professionals who evaluate and intervene with children who have CVI (Philip & Dutton, 2014; Salavati et al., 2017). Therefore, it is essential that these professionals have the necessary training to provide optimal care to maximize independence in school and everyday activities for these children.
Anecdotal reports suggest a lack of formal academic training and continuing education opportunities addressing evaluation and intervention for professionals working with individuals with CVI. There seems to be a disconnect between the amount of education provided and the number of children served by occupational therapists and teachers of students with visual impairments. Children with CVI require specialized interventions that are different from interventions for children with ocular visual disabilities to enhance their visual processing (Khetpal & Donahue, 2007). Therefore, education on how to assess and intervene with children with CVI is imperative and needs to be included in the current curriculum for occupational therapy practitioners and teachers of students with visual impairments. The goals of this study were to (1) explore the education and training received by occupational therapy practitioners and teachers of students with visual impairments specific to CVI and (2) quantify the confidence level of these professional to evaluate, treat and/or teach children with CVI.
Methods and Materials
This study was approved by the Institutional Review Board (IRB) at Cincinnati Children's Hospital Medical Center prior to the questionnaire distribution. An online questionnaire was developed to assess previous training and education obtained on CVI and the confidence levels of occupational therapy professionals, certified occupational therapy assistants and teachers of students with visual impairments working with individuals with CVI. Occupational therapists and certified occupational therapy assistants were combined and were referred to throughout the rest of the manuscript as occupational therapy practitioners. The 41-item electronic survey included open-ended, multiple-choice, and Likert scale questions. The survey took 15–30 minutes to complete. Data collected included topics such as education received regarding CVI, current caseloads, access to medical information, and learning needs regarding CVI.
Participants
Study participants included licensed occupational therapists, certified occupational therapy assistants, and certified teachers of students with visual impairments. There were no exclusion criteria; however, the survey was only available in English.
Recruitment Strategies
Surveys were sent via e-mail to individuals contacted through professional membership organizations and universities’ member lists. Researchers contacted occupational therapy licensure boards in 50 states to obtain e-mail addresses for occupational therapy practitioners. Surveys were sent to occupational therapy practitioners whose e-mail addresses were available at no cost. Additionally, the survey link was posted on professional organization websites, state licensure board websites, professional social media groups, and CVI advocacy and workplace groups.
Data Collection
Participants completed the questionnaire online and data were collected in REDCap, a secure database, between June 2019 and November 2019. A waiver of formal consent was approved by the IRB. Participants were given an information sheet to read prior to filling out the questionnaire. No identifying information was collected. The data was grouped into five categories including types of CVI training received, frequency and types of CVI services provided, access to medical information, importance of access to materials and information regarding children served, and knowledge and confidence in working with children with CVI. The questionnaire was developed by an occupational therapist and reviewed by occupational therapists and an ophthalmologist, optometrist, and a teacher of students with visual impairments to establish consensus on the wording and content of the questions prior to implementation. This study followed the STROBE guideline to ensure high quality of reporting the study procedures (Von Elm et al., 2007).
Statistical Analysis
Descriptive statistics (means and standard deviations) were completed. Data analysis was completed using SPSS. Frequencies, percentages, and means were calculated to describe the characteristics of the survey sample. Qualitative data were analyzed for patterns on the five open-ended questions.
Results
Questionnaires were completed by 205 participants. Questionnaires were completed by 86 occupational therapists (42%), 13 certified occupational therapy assistants (6%), and 106 teachers of students with visual impairments (52%). The mean (range) years of experience was 20.5 (3–49) for occupational therapists, 17 (3–27) for certified occupational therapy assistants, and 14 (1–50) for teachers of students with visual impairments. Questionnaires were collected from practitioners in 43 U.S. states; Washington, D.C.; and Canada. Occupational therapy practitioners and teachers of students with visual impairments reported providing both direct and consultative services to children with CVI. Results indicated that the percentage of occupational therapists, certified occupational therapy assistants, and teachers of students with visual impairments who treated or taught children with CVI using direct services was 67%, 31%, and 81%, respectively and consultative services was 28%, 23%, and 48%, respectively.
Formal Education on CVI
Reported Training Received on Cortical or Cerebral Visual Impairment.
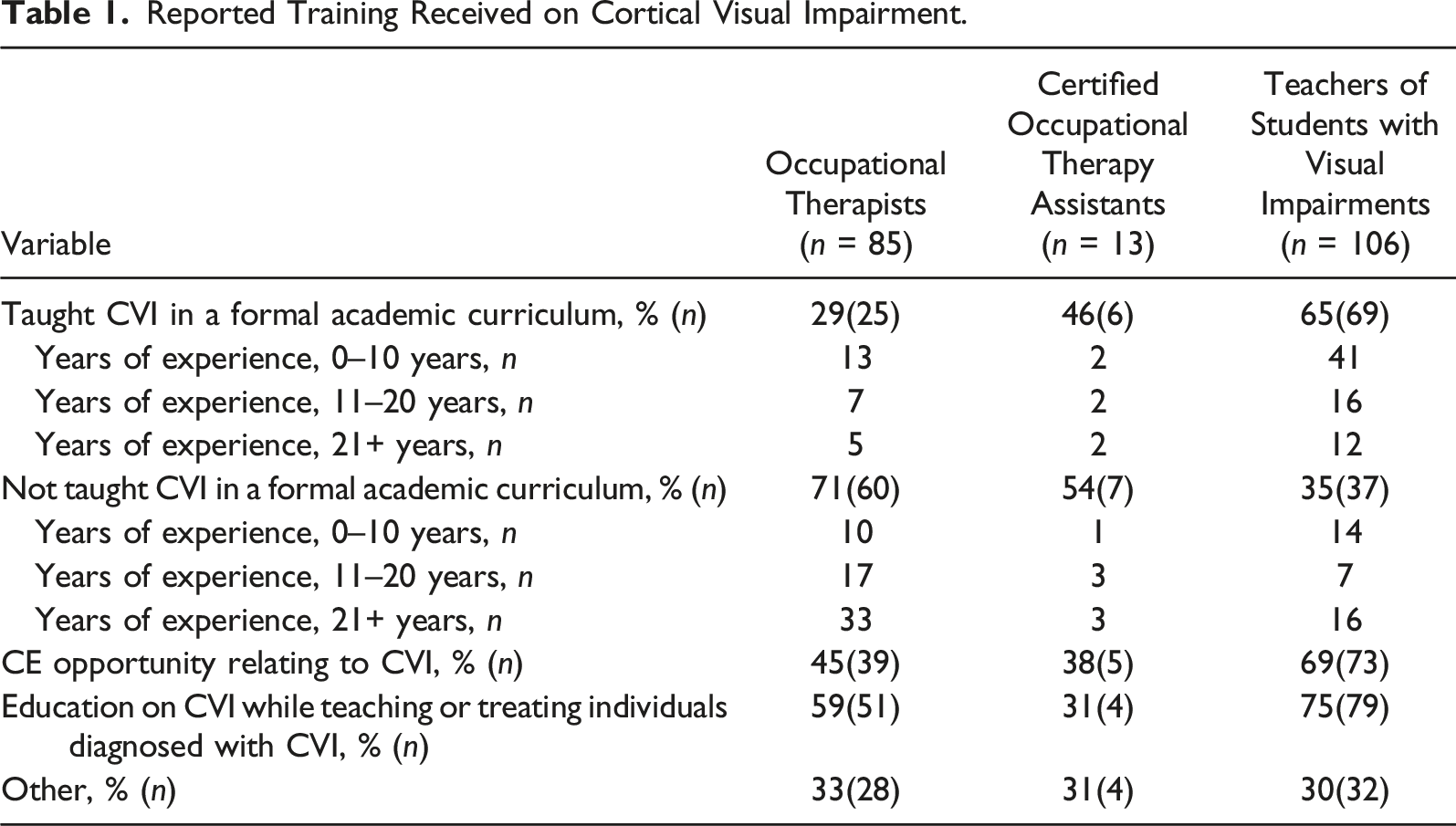
In the past two years, 34% of occupational therapists participated in CE opportunities related to CVI compared to 74% of teachers of students with visual impairments. Of the 107 professionals who have taken a CE course on CVI, 37% took an online course, 41% attended a CVI-specific conference, and 64% attended a CVI-specific presentation. A 5-point Likert scale was used to assess confidence and satisfaction with knowledge and skills in working with children with CVI. Occupational therapists, certified occupational therapy assistants, and teachers of students with visual impairments rated confidence in working with children with CVI as 3.5, 2.3, and 3.9, respectively and satisfaction with knowledge and skills in working with these children was rated 2.6, 1.6, and 3.3, respectively.
Experience or Training on CVI-Specific Evaluations and Interventions
Content Taught During Cortical or Cerebral Visual Impairment Experience and Training.

Accessibility to Medical Information
Average Rating of Accessibility to Medical Information on 5-point Likert Scale.
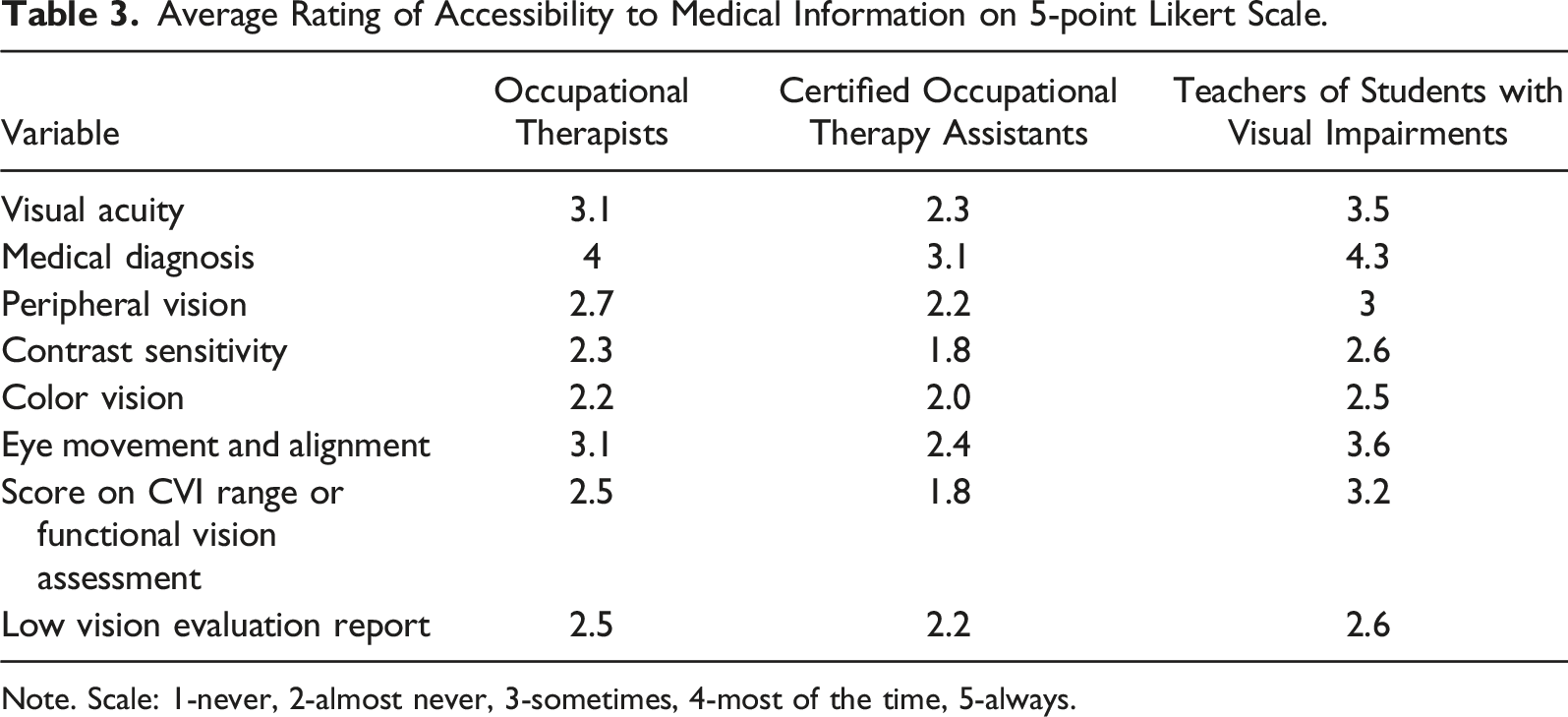
Note. Scale: 1-never, 2-almost never, 3-sometimes, 4-most of the time, 5-always.
Facilitators of Service Provision
To investigate materials needed to make it easier to work with children with CVI, participants rated a variety of materials on a 5-point Likert scale. All practitioners rated almost all the items as moderately or very important, with electronic video games and electronic magnification devices being an exception (average rating 3.5, lower than other items). Ratings among all practitioners indicated that materials explicitly designed for individuals with CVI and access to a multidisciplinary team would make intervention easier. They rated access to functional vision assessment scores, materials designed for children with visual impairments, and collaboration with other medical professionals and caregivers of children with CVI above a 4 on a 5-point scale. They rated access to optical devices, electronic video, and magnification devices on average a 3.5.
Discussion
Foundational education on specific medical conditions begins in formal academic training and continues after graduation in the form of CE and job-specific training. The results of the survey suggest a wide variation and less than optimal formal and informal training provided for teachers of students with visual impairments and even less training for occupational therapy practitioners. Variation in training is problematic, especially for occupational therapy practitioners who have the least amounts of training.
Cortical/cerebral visual impairment is a common pediatric condition and the possibility that occupational therapists and teachers of students with visual impairments will evaluate or treat or teach children with CVI is high. One factor to consider when evaluating the amount of formal academic education received is the number of years the practitioner has been out of school. One of the first papers to characterize CVI was published by Whiting and colleagues in 1985 (Whiting et al., 1985). Therefore, it makes sense that individuals who have been out of school longer received less education on CVI. The mean (range) number of years of experience for occupational therapists was 20.5 (3–49), certified occupational therapy assistants was 17 (3–27), and teachers of students with visual impairments was 14 (1–50). With such a wide range of years of experience, it is not surprising there is variability in the level of formal academic training.
Our survey results showed that a combined total of 1004 children with CVI were being served on the caseloads of the targeted practitioners in some capacity. This finding represents a large population of children who may be negatively affected by the lack of knowledge of CVI of the individuals who are providing them services. Most occupational therapists and teachers of students with visual impairments will likely encounter a child with CVI on their caseload. Therefore, adequate training on how to treat or teach individuals with CVI is essential.
Studies show that children with developmental conditions who receive evidence-based care at an early age have more successful outcomes in development and function (Odom, 2009). Thus, a lack of knowledge about how to work with children with CVI could lead to increased variation in care and decreased quality of care. As a result, potentially poorer outcomes such as minimal improvement in visual function following intervention, may occur. Results from this study suggest that variation in training provided to occupational therapy practitioners and teachers of students with visual impairments needs to be addressed. Occupational therapy practitioners and teachers of students with visual impairments could begin by contacting their licensure boards and formal academic education providers to advocate for curriculum addressing entry-level training for evaluating, treating, and teaching individuals with CVI. Having a training curriculum in which CVI is introduced could be helpful for new practitioners.
The results showed that 65% of teachers of students with visual impairments, 29% of occupational therapists, and 46% of certified occupational therapy assistants were trained on CVI during their formal educations. Additionally, the survey found that teachers of students with visual impairments participated in more formal and informal CVI CE opportunities following graduation. Although both occupational therapists and teachers of students with visual impairments work with children who have a wide range of needs and abilities, since such teachers work solely with students who have been diagnosed as having visual impairments, they may see students with CVI more frequently. However, the lack of training for occupational therapists is problematic because occupational therapy practitioners evaluate and treat many children with developmental conditions associated with CVI. Without proper training, it is unlikely the care provided is the highest quality.
Best practice is to provide evidence-based care to all children on a practitioner's caseload. According to the survey’s findings, only two occupational therapy respondents reported that they had attended a CVI conference; therefore, it appears that most occupational therapy practitioners do not participate in CE opportunities to further their CVI knowledge. A possible reason may be that conferences that are often attended by occupational therapy practitioners infrequently offer courses on CVI. Reading about CVI in research articles would be another way for practitioners to learn about best practices related to CVI. However, a cursory search of The American Journal of Occupational Therapy (AJOT), a key occupational therapy journal, using the keywords “CVI” and “cortical visual impairment” turned up fewer than 5 articles in the last 10 years, whereas a search using the same terms of articles published within the past 10 years in the Journal of Visual Impairment & Blindness, a key journal for teachers of students with visual impairments, revealed 54 articles. Therefore, if occupational therapists are only looking in occupational therapy journals such as AJOT, they may not have access to relevant information.
Clinicians and educators reported that their top three needs when working with children with CVI include access to medical information, access to materials designed for CVI, and working on a multidisciplinary team. Occupational therapy practitioners and teachers of students with visual impairments use available medical information to inform evaluation and intervention for children with CVI, which is essential to provide children with the best possible outcomes. The survey results showed that occupational therapy practitioners have less access than teachers of students with visual impairments to medical information, which could negatively affect the care they provide. Having access to visual exam information could enhance the child’s intervention plan. Advocacy for access to relevant external vision assessments may lead to better outcomes for the child.
Another vital consideration for practitioners who work with children with CVI is receiving adequate support for the interventions they offer. CVI is a complex diagnosis that requires an integrated approach from all members of the treatment team. A multidisciplinary treatment team that offers diverse expertise and collaboration on treatments and education would be ideal for giving children with CVI the opportunity to excel. In a school setting, a collaboration between the occupational therapy practitioner, teacher of students with visual impairments, and school psychologist would allow for the compilation of each discipline’s expertise leading to increased functional independence. As with any child who has a visual impairment, interventions and educational strategies may differ depending on each child’s individual needs. When working with children with CVI, professionals may employ techniques, including, but not limited to, eliminating background clutter or stimuli, dimming the lighting to make the environment more visually comfortable, and using simple high-contrast materials to draw the child’s attention to the work at hand. These types of strategies, combined with a team approach, may be useful in promoting the most effective learning environment for children with CVI.
The survey found that the majority (over 75%) of the practitioners working with children with CVI were utilizing methods and teachings that are disseminated by The Perkins School for the Blind (Perkins School for the Blind, 2022) and Roman-Lantzy for assessment of CVI (Roman-Lantzy, 2007). However, these two results could be influenced by sampling bias, since the sample was a volunteer sample, and thus, there was not equal representation from all parts of the United States and other countries.
The survey results also indicated that the primary assessment used was the CVI Range (Roman-Lantzy, 2007). The CVI Range is a tool that describes behaviors common in children with CVI and classifies the severity of the CVI impairment. The CVI Range was the first assessment method developed and distributed across the United States. Only one major study conducted by Newcomb (2010) has evaluated that reliability of the CVI Range (Newcomb, 2010). This study included 104 participants, and only 27 of those participants were tested by more than one practitioner for inter-rater reliability. Therefore, this study exhibits weak reliability and psychometric data.
Although new CVI assessments and screeners have been developed, the limited amount of research highlights the need for not only more formal education on other methods of evaluation for CVI and diversity in continuing education opportunities, but also more research to establish reliability and validity of assessments used for children with CVI. It is only through evidence-based practice that the treatment of CVI will be considered effective and credible to the medical community.
Limitations
Surveys were limited to online distribution, allowing only practitioners with Internet access to participate in the study. Only a few state occupational therapy associations allowed access to member databases that included digital addresses for their practicing occupational therapists. Therefore, another limitation was that the survey was distributed only to individuals in geographical locations that had access to the website or social media platform on which the survey was posted, and/or those whose e-mail addresses were included on professional lists to which access was granted.
Recall bias is a potential limitation, since the survey relied on a practitioner's accurate recall of their academic curriculum and CVI continuing educational opportunities that attended thereafter. To avoid participant bias, the survey was open to all occupational therapy practitioners and teachers of students with visual impairments in the United States and Canada. Consequently, the results may have been skewed by respondents who did not have children with CVI on their caseloads. A consideration for future research would be to conduct purposeful sampling to include more entry-level practitioners who may provide a more accurate representation of current curriculums and decrease the likelihood of recall bias.
Implications for Practice
A clear understanding of CVI and the common behavioral characteristics that are common in children with CVI is needed to provide high-quality care. It is possible that a child with CVI could be referred to services from occupational therapy practitioners or teachers of students with visual impairments prior to receiving a CVI diagnosis. It is imperative that these practitioners are trained to understand and identify CVI so that they can provide proper evaluation, treatment, and education, while also having an improved ability to refer these children appropriately for a proper diagnosis. This study is the first to identify an educational gap for professionals who treat or educate children with CVI. Including the topic of CVI in the standard occupational therapy and teacher of students with visual impairments curriculum would be beneficial to these future professionals, while also providing practitioners with a more extensive base of expertise for practice and increasing the credibility of the professions.
Conclusion
CVI is a highly prevalent condition and is the leading cause of visual impairment in children in high-income countries. Children with CVI require evaluation and intervention from occupational therapy practitioners and teachers of students with visual impairments for optimal functioning and learning. Only one-third of occupational therapy professionals and two-thirds of teachers of students with visual impairments reported being exposed to CVI in their formal academic coursework, supporting anecdotal evidence of an educational gap in CVI education. This educational gap is further supported by data showing decreased satisfaction in CVI knowledge and skills by both occupational therapy practitioners and teachers of students with visual impairments. Further research is needed to identify specific knowledge deficits that should be addressed in formal occupational therapy practitioner and teacher of students with visual impairments coursework, including the diversity of assessment techniques. Advocacy efforts are essential to encourage formal education programs in the states sampled to include CVI education in their curriculum if they do not currently do so. This encouragement could potentially lead to an increase in the percentage of new occupational therapy practitioners and teachers of students with visual impairments who feel confident to evaluate, treat, and educate individuals with CVI. Having knowledgeable and competent practitioners who treat and educate children with CVI may generate better outcomes for the children. Based on these study results, there is a clear gap and inconsistency in CVI education being provided across disciplines.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.