
Abstract
Keywords
According to the World Health Organization (WHO), a person with low vision is defined as a “person who has impairment of visual functioning even after treatment and/or standard refractive correction, and has a visual acuity (VA) of <6/18 to the perception of light (PL) in the better eye, or a visual field of <10° from the point of fixation, but who uses, or is potentially able to use vision for the planning and/or execution of a task” (WHO, 1993). Globally, over 161 million people experience visual impairments, out of which 37 million are blind and 124 million are with low vision (Resnikoff et al., 2004). Around 90% of the global population of people who are blind reside in developing countries that have limited rehabilitation and vocational resources (Thylefors, 1998). In Pakistan, approximately 1.12 million people are blind, 1.09 million people have severe vision loss (3/60 ≤ VA), and 6.79 million people have moderate vision loss (6/60 ≤ VA) (Hassan et al., 2019).
Patients experiencing visual impairments have an increased risk of developing depression and anxiety due to poor quality of life caused by functional vision loss. Rehabilitation of individuals who have low vision is crucial since it enhances functional vision and quality of life in patients with low vision. There is an immense body of literature on improvement in quality of life and functional vision through proper low vision rehabilitation (Renieri et al., 2013; van Nispen et al., 2020). The necessary steps of low vision rehabilitation include dispensing and training individuals in how to use low vision devices, providing mobility training, such as assistive technology and adaptive vocational training, as well as long-term follow-up appointments and counseling sessions. However, despite the efforts to improve low vision rehabilitation, the uptake of low vision services continues to be low, even in the developed world, due to many barriers and prejudices around low vision rehabilitation (Owsley et al., 2009). The situation is worse in underprivileged communities, especially those in developing countries (Dandona et al., 2002). In the last two decades, low vision research has been focused on barriers to proper service provision, including those faced by eye care providers and patients. These barriers include a lack of awareness of proper vision rehabilitation, a lack of availability of low vision devices, and a lack of knowledge on service delivery among eye care providers (Hassan et al., 2019; Jose et al., 2016). As Pakistan is facing a large socioeconomic burden of disease because of visual impairment, which is expected to rise by 2025 (Hassan et al., 2019), all primary- and secondary-level eye care workers, especially optometrists, play an important role in catering to the growing need for patient care and to improve service delivery. The number of people in the optometry workforce in Pakistan is scarce—there are no more than 1,000 optometrists working in the whole country, with an optometrist versus population ratio of 1:21,2319. These figures indicate a need for at least 20,000 more trained optometrists to reach the global target of 1:10,000 ratio (Naidoo et al., 2022). Therefore, it is crucial to understand the regional barriers and challenges faced by optometrists in providing low vision rehabilitation. This study aimed to assess the level of understanding and knowledge and to determine the barriers to proper low vision rehabilitation among optometrists working at different levels of eye care services in Pakistan.
Methodology
A prospective cross-sectional survey-based study was conducted at the University of Faisalabad (TUF), Pakistan, between January 2021 and July 2021. Ethics approval was obtained from the institutional review board and ethics committee of TUF, Pakistan. The study protocol followed the tenets of the Declaration of Helsinki, revised in 2000. The study population included all optometrists practicing in Punjab province at various public and private sector eye hospitals. These optometrists were recruited through approved study advertisements on social media, professional platforms, and word of mouth. After verbal consent, informed written consent was taken, and all enrolled participants completed a self-administered pretested, standardized questionnaire (Jose et al., 2016; see Online Appendix A) in English using SurveyMonkey and Google Forms. The questionnaire contained closed-ended responses in sections including demographic information and qualification, assessment of knowledge regarding low vision, and perceived barriers to proper low vision rehabilitation. The specific questions regarding the awareness and barriers to low vision rehabilitation were modified to exclude the “not sure” option, making it simpler and more straightforward to avoid any anticipated selection bias from the study population. The question regarding the service delivery was categorized as “adequate” if the participants reported fulfilling all steps of rehabilitation including initial assessment and provision of low vision aids and training as well as referring the patient to a specialized unit for further management opportunities. The “inadequate” service included missed steps of rehabilitation and referral to other centers without initial assessment and counseling. All collected data was transferred to and stored in Microsoft Excel sheets. The questions regarding level of knowledge were scored and analyzed with “1” given to correct and “0” to incorrect identifications of answers. The Statistical Package for Social Science (SPSS) software was used for the tabulation and analysis of the collected data. Pearson's chi-square test was used to determine the association between the level of awareness and perceived barriers to low vision rehabilitation among optometrists with age, gender, number of years of working experience, and working place. A p value of less than .05 was considered statistically significant.
Results
A total of 100 participants completed the study questionnaire, including 59 male and 41 female eye care providers. The mean age of participants was 26 (±6.1 SD) years with a range of 21–55 years of age. Of these, 47 participants (47%) had more than 3 years of professional experience and 53 participants (53%) had less than or equal to 3 years of working experience. Fifty-six participants (56%) were working in a hospital setting (public or private), and 44 participants (44%) were working in a private practice setting. The majority of participants (84%) reported of being directly involved in patient management at their practice. Regarding low vision service provision, all participants reported that they worked with a person with low vision on a daily basis (zero participants reported “none”), 66 participants (66%) reported of daily patient load of three or fewer low vision patients, while 32 participants (32%) were seeing 3–10 low vision patients daily, and two participants (2%) reported of seeing more than 10 low vision cases as part of their daily routine. Regarding low vision rehabilitation services, 60 participants (60%) reported that they provided inadequate services either by providing spectacle correction and optical devices alone, without any further steps related to low vision rehabilitation, or that they simply referred their patients to other hospitals or health care centers without assessment and management with available low vision devices and counseling. Forty participants (40%) reported providing adequate services including all of the necessary steps for low vision rehabilitation. The majority of participants (59%) reported having no low vision clinical setup (including low vision charts or trial devices) at their practices. Those who were working in hospital settings (either public or private) had proper low vision clinical setups, as compared to those working in private practices (p = .004).
To assess the level of awareness regarding low vision rehabilitation, a list of structured, closed-ended questions was provided. Eighty-two participants (82%) reported of having an accurate understanding of WHO definition of low vision. Eighty-one participants (81%) correctly identified WHO's criteria for reduced visual acuity of 6/18 (20/63) or less and 76 participants (76%) correctly identified WHO's criteria for reduced visual field of 10° or less. However, when asked about the steps for low vision rehabilitation, 47 participants (47%) had no knowledge of all the necessary steps of low vision rehabilitation.
Most common barriers to proper low vision rehabilitation, as reported by participants were expense of rehabilitation (95%), time constraints (92%), lack of training (92%), lack of awareness (90%), lack of availability of low vision devices (90%), lack of manpower (82%), lack of interest (81%), difficulty in satisfying low vision patients (73%), and excessive workload (72%) (see Figure 1). When asked about future recommendations to improve low vision services in the country, 98% of participants suggested that awareness be raised among practitioners, patients, and the public, by creating more training programs for practitioners and increasing the availability of low-cost low vision devices (a detailed response rate for all questions is attached as Online Appendix B, Table 1).
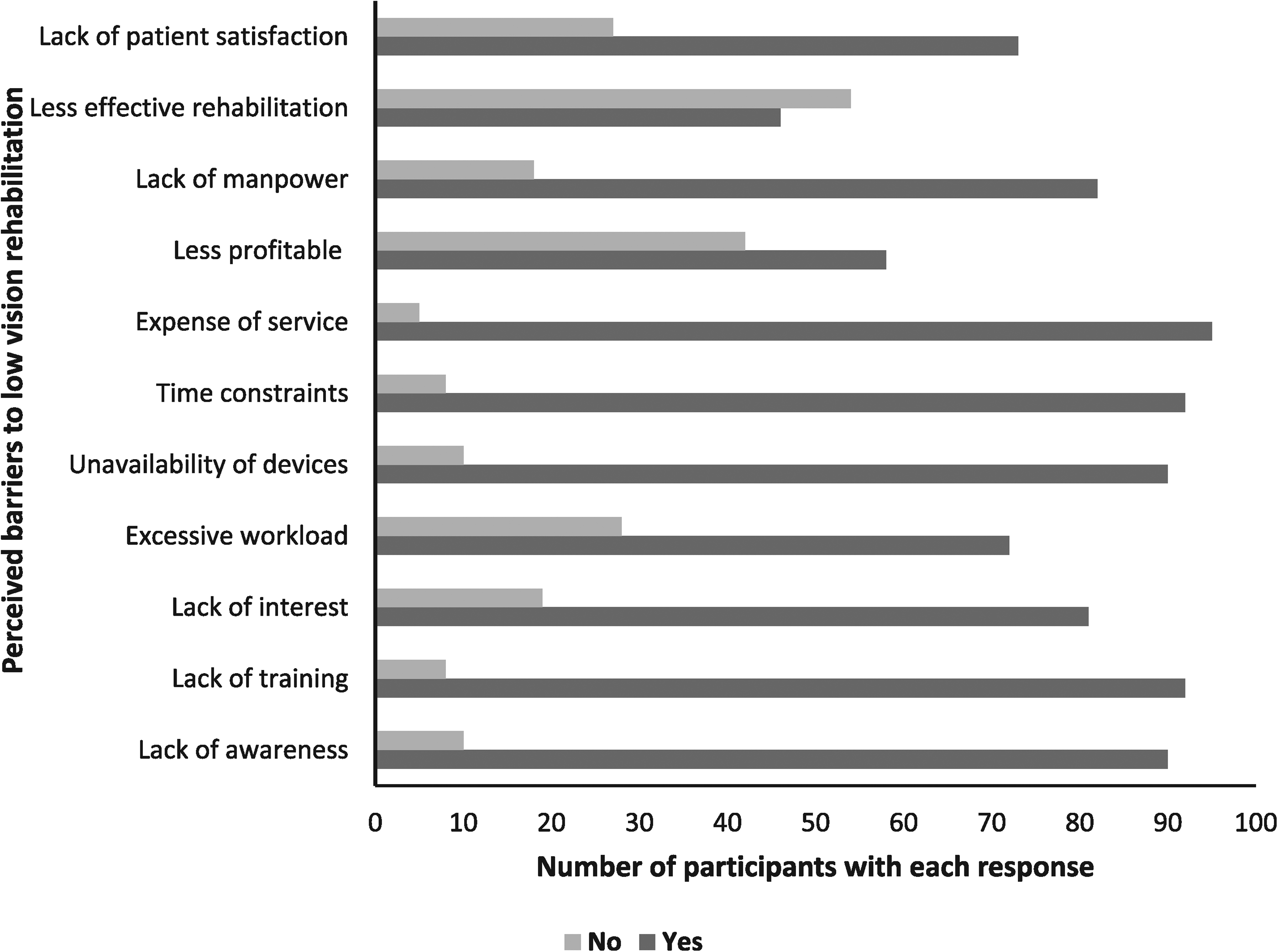
Perceived Barriers to Low Vision Rehabilitation as Reported by Study Population.
Association of Level of Knowledge and Barriers to Low Vision Rehabilitation With Working Experience of Study Population.
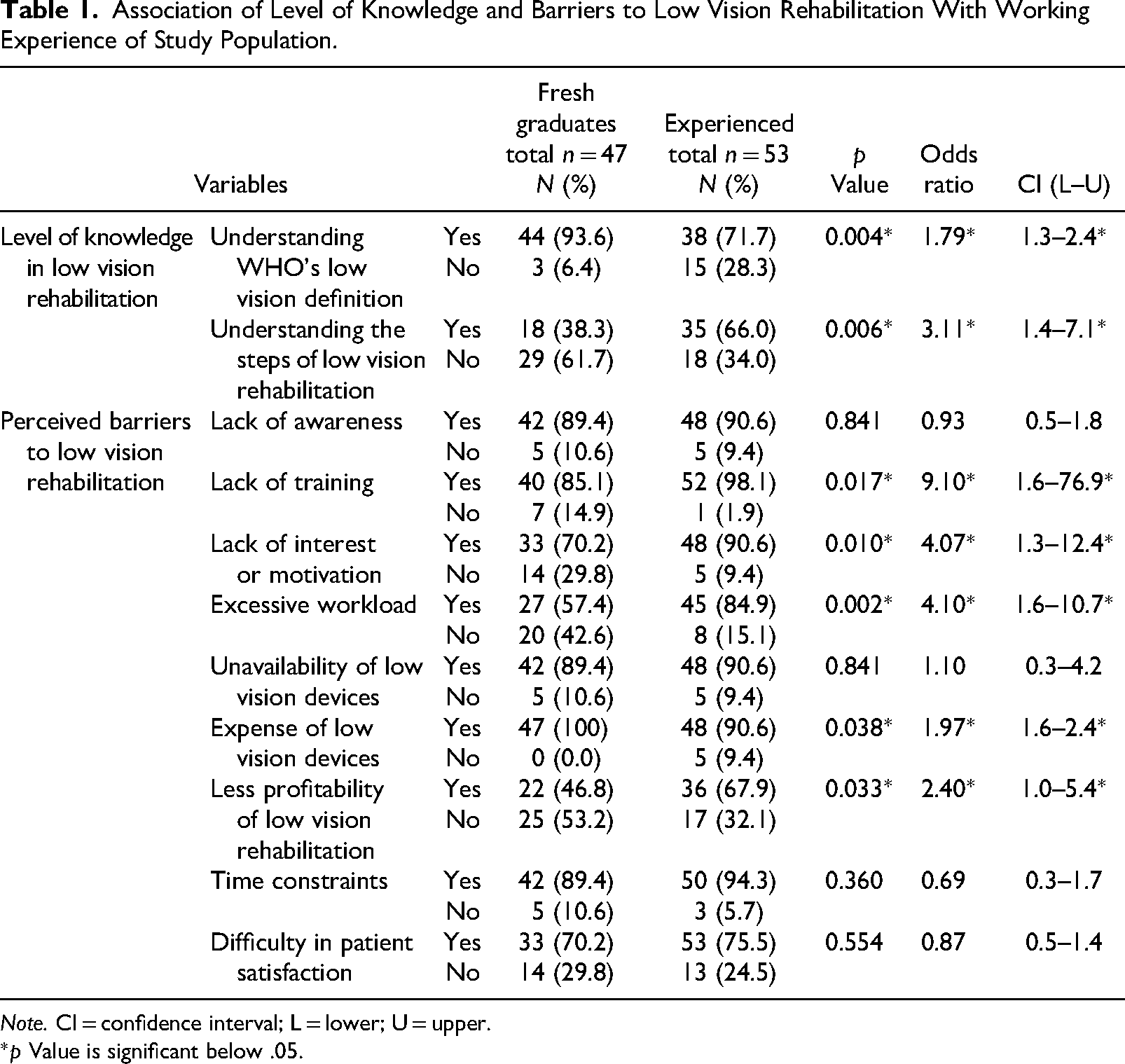
Note. CI = confidence interval; L = lower; U = upper.
*p Value is significant below .05.
Gender was insignificant when comparing the level of awareness and knowledge among the study population. However, recent graduates with less than 3 years of working experience as optometrists had a significantly better understanding of the definition of low vision (p = .004) and low vision rehabilitation steps (p = .006), as compared to more experienced optometrists (see Table 1).
There were no differences in the level of awareness and knowledge between those working in hospitals and private practices. However, those working in private practices were more likely to consider low vision rehabilitation as less profitable (p = .025, odds ratio = 2.56, CI = 1.1–5.8), compared to those working in hospitals (see Table 2).
Association of Level of Knowledge and Barriers to low Vision Rehabilitation With Place of Work of Study Population.

Note. CI = confidence interval; L = lower; U = upper.
*p Value is significant below.05.
Discussion
This study reported the level of knowledge and understanding of low vision rehabilitation among optometrists in Pakistan. The majority of participants had an adequate understanding of low vision definition and WHO's criteria for low vision inclusion. However, more than half of the study participants failed to correctly identify all steps of low vision rehabilitation, including best-corrected spectacle prescription, training to use low vision devices, mobility training, adaptive training for the job, and counseling. To the best of our knowledge, this is the first-ever reported data on the level of awareness and barriers to low vision rehabilitation among optometrists in Pakistan. These findings are particularly important due to the increasing global focus on low vision rehabilitation in middle- and low-income countries, to eradicate preventable blindness.
The level of low vision rehabilitation awareness and knowledge among the optometrists in this study is similar to that reported in other middle- and low-income countries (Jose et al., 2016; Marinoff, 2012). Interestingly, more experienced optometrists (i.e., those with more than 3 years of experience) had poorer levels of knowledge and awareness regarding low vision rehabilitation, compared to less-experienced optometrists (p < .05). These findings highlight the importance of continuous professional training and refresher courses for graduate practitioners to enhance their skills. Also, a significantly higher number of experienced optometrists reported a lack of training and lack of motivation or interest as barriers to low vision rehabilitation, compared to recent graduates (p < .05). Lack of awareness (90%), lack of training (92%), lack of interest and motivation (81%), excessive workload (72%) and unavailability of devices (90%) were other perceived barriers. Similar findings have been reported previously (Hassan et al., 2019; Jose et al., 2016; Okoye et al., 2007). Regardless of regional variations, low vision rehabilitation involves advanced diagnostic and management technology as well as highly motivated personnel to improve the quality of life in vulnerable low vision populations. The findings of the current study reflect that lack of proper training and awareness, which, considering the limited access to resources, may result in a loss of motivation or interest in proper low vision management. Therefore, it is highly significant to evaluate and overcome these challenges faced by low vision specialists including optometrists, to improve the delivery of service globally.
In this study, experienced optometrists (i.e., those with more than 3 years of working experience) considered low vision services more time consuming, expensive, and less profitable, compared to recent graduates (p < .05). In Pakistan, optometrists obtain clinical and subspecialty training during graduate degree programs with limited or no availability of post-graduate training. The country is also way behind other nations in regards of optometric authorization and organization with no licensing body or legislature to pursue experienced optometrists in uplifting their knowledge or continue professional development. The aim of an optometry governance board or legislature authority is to maintain the standards of practice and implement continuous professional development among practitioners. Having such legislative supervision at the national level in Pakistan or any other country facing similar challenges will be very helpful for enhancing optometrists’ level of understanding and low vision rehabilitation services across the country (Okoye et al., 2007; van Nispen et al., 2020).
In this study, no age or gender differences were reported in terms of the level of awareness and knowledge regarding low vision rehabilitation. Optometrists working in hospital settings had similar levels of knowledge to those working in private practices. However, a significantly higher number of optometrists working in private practices considered low vision rehabilitation as being less profitable, compared to those working in hospitals (p < .05). Although not significant, a higher number of private practitioners considered a lack of patient satisfaction as a barrier to low vision rehabilitation (p = .07). Improved communications between practitioners and patients and educating practitioners in psychosocial counseling of low vision patients may help to overcome this barrier and increase patients’ satisfaction during low vision rehabilitation (Markowitz, 2006; van Nispen et al., 2020).
Conclusion
In summary, the majority of the study population had adequate levels of knowledge regarding the definition of low vision and its criteria but lacked an adequate understanding of proper low vision rehabilitation. Lack of training and unavailability of low vision rehabilitative devices are major barriers, as perceived by optometrists. Rigorous attempts are needed to educate eye care practitioners—specifically optometrists—about the availability and usage of low-cost, improved-quality, and up-to-date low vision devices in the country. A basic low vision assessment kit should be a mandatory part of any ocular examination setup, including at hospitals and private clinics.
A limitation of this study was a limited sample size, which may not represent the whole country's optometry population—a larger study, with a bigger sample size, may further help researchers understand the level of knowledge and barriers to proper low vision rehabilitation. However, this preliminary study may help policymakers and health authorities to regulate and upgrade low vision services in Pakistan, which, in turn, may help a large number of people experiencing vision loss in the country.
Supplemental Material
sj-docx-1-jvb-10.1177_0145482X241248461 - Supplemental material for Assessment of Level of Awareness and Barriers to Low Vision Rehabilitation Among Optometrists in Pakistan
Supplemental material, sj-docx-1-jvb-10.1177_0145482X241248461 for Assessment of Level of Awareness and Barriers to Low Vision Rehabilitation Among Optometrists in Pakistan by Memoona Arshad, Aqsa Younas and Nida Amin in Journal of Visual Impairment & Blindness
Supplemental Material
sj-docx-2-jvb-10.1177_0145482X241248461 - Supplemental material for Assessment of Level of Awareness and Barriers to Low Vision Rehabilitation Among Optometrists in Pakistan
Supplemental material, sj-docx-2-jvb-10.1177_0145482X241248461 for Assessment of Level of Awareness and Barriers to Low Vision Rehabilitation Among Optometrists in Pakistan by Memoona Arshad, Aqsa Younas and Nida Amin in Journal of Visual Impairment & Blindness
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.