
Abstract
The National Institutes of Health human immunodeficiency virus (HIV) and Aging Working Group identified spirituality as a research emphasis. This qualitative study examines the importance of religion and spirituality among 30 HIV-positive older adults. Using modified grounded theory, adults 50+ were recruited in Ontario, Canada, through AIDS service organizations, clinics, and community agencies. Descriptions of religion and spirituality encapsulated the idea of a journey, which had two components: the long-term HIV survivor profile combined with the experience of aging itself. A final category of HIV as a spiritual journey was finalized through consensus and included the properties of (1) being rejected by as well as rejection of formalized religion, (2) differentiating spirituality from religion, (3) having a connection, (4) feeling grateful, and (5) mindfulness and learning new skills. Interventions fostering resilience and strengths in HIV-positive older adults using spirituality should be considered, including the promotion of person-centered spirituality and interventions that include mindfulness and skill building.
Advances in the clinical management of human immunodeficiency virus (HIV) disease, due largely to the effectiveness of highly active antiretroviral therapy (HAART), have altered the epidemiological landscape of HIV in the North America and globally (Palella et al., 2006). Due to the confluence of new HIV infections and increased longevity, there is a substantial and consistent growth in the number of people over the age of 50 living with HIV infection throughout North America. For example, in Canada, new HIV diagnoses among adults aged 50 years and over have grown consistently over time, increasing from 1 in 10 (10%) in 2007 to more than 1 in 5 (21%) in 2013 (National Coordinating Committee on HIV and Aging, 2015). Similarly in the United States, between 2010 and 2014, the number of people aged 50 years and over living with HIV infection in the United States increased from 301,647 to 428,724 between 2010 and 2014 (Centers For Disease Control and Prevention [CDC], 2016), an increase of approximately 40%.
Clinical advances notwithstanding, growing evidence suggests aging with HIV disease is uniquely challenging (High et al., 2012). Seropositive older adults must confront complex physiological and psychosocial issues (High et al., 2012) related to increased mortality (CDC, 2016), delayed or late diagnosis (CDC, 2016; National Coordinating Committee, 2015), as well as accelerated or accentuated aging (Pathai, Bajillan, Landay, & High, 2014). Stigma and ageism—related not only to the disease itself but to aging with it—have been implicated in the fragility of seropositive older adults’ informal social support networks and their relative isolation (Emlet, 2006; Fredriksen-Goldsen, 2011; Shippy, Cantor, & Brennan, 2004).
Interest in understanding successful aging in this population is growing despite the unique challenges confronting people aging with HIV. The HIV and Aging Working Group, in their report to the National Institute of Health, Office of AIDS Research, has identified understanding successful aging with HIV as a research priority (High et al., 2012). The working group acknowledges the importance of improving our understanding of this phenomenon—explaining that, through understanding what characteristics are associated with successful aging, we can subsequently “translate research findings for those not successfully aging” (S14). A variety of components may contribute to the concept of successful aging among those aging with HIV, including spirituality and mindfulness (High et al., 2012).
Religion and Spirituality
Before proceeding, it is important to clarify the distinction between religion and spirituality. Admittedly, both are multidimensional constructs and operationalized differently in the literature. In general, religion is typically perceived more narrowly—as a construct linked to dogma, to institution (Tarakeshwar, Khan, & Sikkema, 2006), and to worshipping a higher power, like God (Hill et al., 2000). Spirituality, on the other hand, is conceptualized as a broader concept, concerned with individuals’ functional experiences of personal transcendence, superconscious sensitivity, and meaningfulness (Hill et al., 2000).
Successful Aging, Religion, and Spirituality
Prevailing models of successful aging (Rowe & Kahn, 1998) have been criticized for their inconsideration of individual differences in aging (Rubinstein & de Medeiros, 2014) and for their failure to highlight association(s) between religion, spirituality, and health (Crowther, Parker, Achenbaum, Larimore, & Koenig, 2002). Neglecting religion and spirituality as central constructs in paradigms of successful aging handicaps their application—namely because research notes high levels of religious participation among older adults (Krause, 2008; McFadden 2013). Further, national surveys have consistently shown that the vast majority of older Americans report a religious or spiritual component to their lives (Crowther et al., 2002). In Rowe and Kahn’s (2015) recent “conceptual expansion” of successful aging, constructs associated with religion and/or spirituality were still absent.
This is notable—because, among the general adult population, religiosity and spiritual involvement have been associated with improvements in subjective states of well-being (Ellison, 1991), reductions in levels of depression, distress, and morbidity (Williams, Larson, Buckler, Heckmann, & Pyle, 1991); and among older adults specifically, spirituality may aid in addressing existential concerns regarding afterlife, which can contribute to one’s own subjective life review, and support gerotranscendence (Erikson, 1997). Stigma and ageism may hinder older adults living with HIV from the benefits of engagement in religious and spiritual support (Vance et al., 2011). However, in a study of older adults living with HIV, Brennan, Strauss and Karpiak (2010) found that about half of their study population had disclosed their HIV status to their religious congregation, while the other half remained engaged in their religious communities despite nondisclosure. Past research also highlights the benefits of religious and spiritual practice, broadly, in the context of coping with chronic disease (Dalmida, 2006; Vance, Struzick, & Masten, 2008), but significantly less is known about their benefits in the context of HIV disease.
Religion, Spirituality, and HIV
Because HIV has transitioned from a terminal to a chronic disease (Deeks, Lewin, & Havlir, 2013), the role of religious and spirituality among those living with HIV has also changed. For example, early qualitative work with HIV-positive individuals positioned religious and spiritual coping as a strategy through which adults found meaning in preparing for an impending death (Hall, 1998). Adults living with HIV are now surviving to ages similar to their seronegative counterparts (CDC, 2016) and thus, religion and spirituality may be examined as a means to promote healthy adaptation to HIV.
This body of research suggests religion and spirituality are associated with beneficial outcomes in individuals living with HIV infection (Trevino et al., 2010) including less psychological distress (Simoni, Martone, & Kerwin, 2002), pain (Ramer, Johnson, Chan, & Barrett, 2006), and depression (Coleman, 2004; Simoni & Ortiz, 2003). Higher levels of spirituality among seropositive individuals have been associated with fewer HIV symptoms and with feeling like life has improved since diagnosis (Szaflarski et al., 2006). Spirituality has also been linked to physiological indicators of HIV progression: Patients reporting an increase in spirituality following an HIV diagnosis had lower rates of CD4 cell loss and lower rates of viral load increase over 4 years than participants whose spirituality decreased post-diagnosis (Ironson, Stuetzle, & Fletcher, 2006). In a study following a cohort of persons living with HIV/AIDS for 17 years, researchers found that positive spiritual coping predicted greater survival rates (Ironson, Kremer & Lucette, 2016).
Mindfulness-based stress reduction (MBSR) practices—derived from ancient Buddhist teachings—(Hanh, 1987; Kabat-Zinn, 2003) have become appreciated for its contributions to living with HIV infection and improving outcomes (Robinson, Mathews, & Witek-Janusek, 2003). Studies show that MBSR programs are efficacious among people living with HIV (PLWHIV) on outcomes as diverse as improvements in levels of cortisol, CD4s, CD8s, cytokines, CD4 receptor expression, and natural killer cells, as well as psychological well-being and HIV prevention (Abell & Rutledge, 2009; Creswell, Myers, Cole, & Irwin, 2009; Jam et al., 2010; SeyedAlinaghi et al., 2012; Treloar, Laybutt, & Carruthers, 2010). In a preliminary systematic review of the 11 known studies that have been conducted on mindfulness and PLWHIV, Riley and Kalichman (2015) found that MBSR interventions decreased emotional distress and, in some cases, improved disease progression. A recent study found that the significance of spiritual and complementary and integrative health approaches are resources for older adults living with HIV/AIDS (Porter, Brennan-Ing, Burr, Dugan, & Karpiak, 2015). Combined, these studies position mindfulness and other spirituality-based practices as promising interventions for PLWHIV—but their (formal and informal) application(s) in the lives of older adults aging with HIV disease are unclear.
Religious participation among older adults is greater than in any other age-group (Kaplan & Berkman, 2011) and likely plays an adaptive role in how they cope with adverse life experiences, including chronic or terminal illness(es). Religious behaviors—such as prayer and church attendance—have also been linked to positive mental health outcomes (Krok, 2014), less emotional distress, better quality of life, medical adherence, and higher CD4 counts (Flannelly & Inouye, 2001; Parsons, Cruise, Davenport, & Jones, 2006; Szaflarski et al., 2006; Woods, Antoni, Ironson, & Kling, 1999).
However, participation in organized religion has also been associated with adverse psychological outcomes—like feelings of guilt or anxiety—as well as doctrines to adhere to personal austerities, denying sexuality, or refuse live-saving medical therapies (Kaplan & Berkman, 2011). Few studies have examined the unintended consequences of religious participation among PLWHIV. Early in the HIV/AIDS epidemic—when the mechanisms of transmission were unclear and largely tethered to homosexuality or drug use—many religious organizations considered the disease to be a punishment for sin (El-Bassel, Shaw, Dasgupta, & Strathdee, 2014). Given this history, it is conceivable that PLWHIV, particularly gay men, may be more likely to identify as being spiritual rather than religious (Tarakeshwar et al., 2006)—but how these identities are renegotiated, and to what extent religion in re-embraced with HIV in late adulthood, remains unclear.
Combined, these findings suggest religion and spirituality may have mixed linkages with health outcomes among individuals with HIV/AIDS. To date, few studies have used qualitative methods to describe and understand the place of religion and spirituality in successfully aging among HIV-positive older adults.
Religion, Spirituality, and Aging Successfully With HIV
Despite the noted positive effects of religion and spirituality on the psychological well-being of PLWHIV, few studies have described how these practices promote successful aging among older adults living with HIV/AIDS. Of the few studies that have examined this phenomenon, findings suggest that spirituality may be protective, with seropositive individuals incorporating their spirituality into their coping process (Cotton et al., 2006). It is noteworthy, for example, that 45% of a sample of adults with HIV reported an increase in their spirituality in response to their diagnosis (Ironson et al., 2006) and that this finding has been replicated across samples (Cotton et al., 2006).
Unfortunately, less is known about how religion/spirituality contribute to successful aging through the lived experiences of older adults living with HIV. Extant studies on the matter are also disproportionately quantitative. To address this gap in the literature, we conducted a qualitative study among older adults living with HIV, exploring their lived experiences of aging successfully. The purpose of this article is to report on qualitative results from 30 in-depth interviews with older adults who have self identified as aging successfully with HIV and to elucidate the role that religion and spirituality (including mindfulness) plays in that dynamic.
Method
Ethical Approval
This study was approved by the research ethics board at McMaster University. Written consent was obtained from all participants.
Study Sample
This study’s sample included 30 adults, aged 50 years or older, who are HIV positive, living in Ontario, Canada, and self-identifying as “aging successfully with HIV.” We interviewed participants in two different cities in the Greater Toronto/Hamilton area of Ontario, Canada. The first city is considered to be resource rich (i.e., residents have access to multiple AIDS service organizations [ASOs] and a large array of HIV specific as well as general health and social services). The second city is urban but has fewer resources particularly HIV-specific services. There is one ASO in the city and that organization has experienced organizational issues impacting their provision of services.
Sampling Strategy
Adults, 50 years and over, living in the Greater Toronto/Hamilton Area of Ontario, Canada, were recruited using purposive sampling strategies. Purposeful sampling techniques set the tone for in-depth qualitative analysis by systematically representing a variety of perspectives on the topic of the study, that is, successful aging with HIV (Palys, 2008). In order to maximize diversity in the data, specific efforts were made to recruit older women, people of color, and individuals who were older than 65 years of age.
Recruitment
Flyers concerning the study were placed at HIV clinics, ASOs, and notices were published in HIV consumer newsletters. We sought to recruit individuals who were aged 50 and over, were living with HIV, and felt they were aging well with HIV. The informed consent procedure asked individuals what it was about them personally that helped them age successfully with HIV? Potential participants were encouraged to call the principal investigator (PI) to determine eligibility. Participants were paid $25 CAD for their participation. After potential participants contacted the PI, an initial phone screening was completed to ensure participants met the study’s inclusion criteria. Individuals were considered if they were at least 50 years of age or older, HIV positive, considered themselves as aging successfully with HIV, and had the ability to provide informed consent. Research focusing on diverse elders living with disabilities found allowing participants to self define successful aging was a sound methodological approach (Romo et al., 2012). Eligible participants were then invited to schedule an in-person interview.
Data Collection
Two researchers (C.A.E. and C.F.) conducted the qualitative interviews, which lasted approximately 45–120 min, between February and May 2013. After interviews were completed, they were professionally transcribed and returned to the PI for analysis. No participants who contacted the PI refused to participate. One interviewee was eliminated from the analysis when it was learned he did not meet the age criteria for inclusion.
Participants were asked their age, gender, sexual orientation, racial and ethnic background, time since first HIV diagnosis, living arrangements, education, marital status, income, employment status, and whether they had ever been diagnosed with AIDS. We used nine semistructured interview questions based upon the Late Life Resilience Framework (Cruttenden, 2016), through a collaborative interview process whereby researchers and participants are coconstructors of knowledge (Holstein & Gubrium, 1995). Participants were asked to describe their lived experience of having with HIV and the individual characteristics, interpersonal relationships, and environmental resources they considered central to their experiences of aging successfully.
Using constructivist grounded theory techniques (Charmaz, 2014), the authors explored strategies that participants employed to engage in successful aging within their own personal context. Religious and spiritual coping in the context of successful aging with HIV emerged from our data for the majority of our participants (N = 21), and therefore we began the process of developing the beginnings of a substantive resilience theory explaining some of the strategies involving religion and spirituality associated with successful aging.
As the research progressed, the idea of “HIV as a spiritual journey” emerged from the interview data. For example, after the interviews were underway, it became clear that successful aging with HIV was influenced by dimensions of religion and spirituality. In the subsequent interviews, we asked specific questions to explore how religion and/or spirituality was seen as a component of successful aging.
Data Analysis
Interview transcripts were first read by all researchers with notations made in reference to emerging categories. Transcripts were managed using NVivo (Version 10) (QSR International, 2012) software that facilitates qualitative data analysis and management. Four researchers trained in qualitative methods conducted the analysis using constructivist grounded theory techniques (Charmaz, 2014) to complete open and focused coding.
Using peer debriefing and consensus building (Erlandson, 1993), researchers came together to build a codebook comprised of 21 codes which were collapsed into 11 code families with definitions. After the codebook was established, two researchers separately coded all 30 interviews and conferred after all transcripts had been coded. This iterative process identified segments in which codes did not agree, so that the researchers could address and edit code segments and move forward with more accurately coded material (Guest & MacQueen, 2007).
After all of the interview transcripts were coded, an interrater reliability test was performed to ensure that agreement was reached among coders. After obtaining a pooled Cohen’s κ statistic of 83% (Cohen, 1960; De Vries, Elliott, Kanouse, & Teleki, 2008), two of the coders (C.A.E. and L.H.) met as a team to discuss and adjudicate each excerpt where agreement was not obtained. Cohen’s κ statistic is a widely used measure to evaluate intercoder agreement as compared to the rate of agreement expected by chance. According to Landis and Koch (1977), the κ-statistic achieved was considered to be “very good agreement.” After the adjudication process was complete, and 100% agreement was reached, the authors conducted a more focused analysis aimed at uncovering the possible dimensions related to religion and spirituality and developed the category of HIV as a spiritual journey. The analysis focused around discovering the relationship between properties and dimensions while we continued to explore other categories found in the data. In order to further develop the category of HIV as a spiritual journey, we used memoing (Bowers, 1989; Charmaz, 2014; Strauss & Corbin, 1998) and developed a matrix as the analysis progressed to illustrate and support the development of the category. We used techniques described by Charmaz (2014) and Strauss and Corbin (1998) to show the relationship(s) that exist(s) among properties and dimensions supporting the category of HIV as a spiritual journey (see Figure 1).
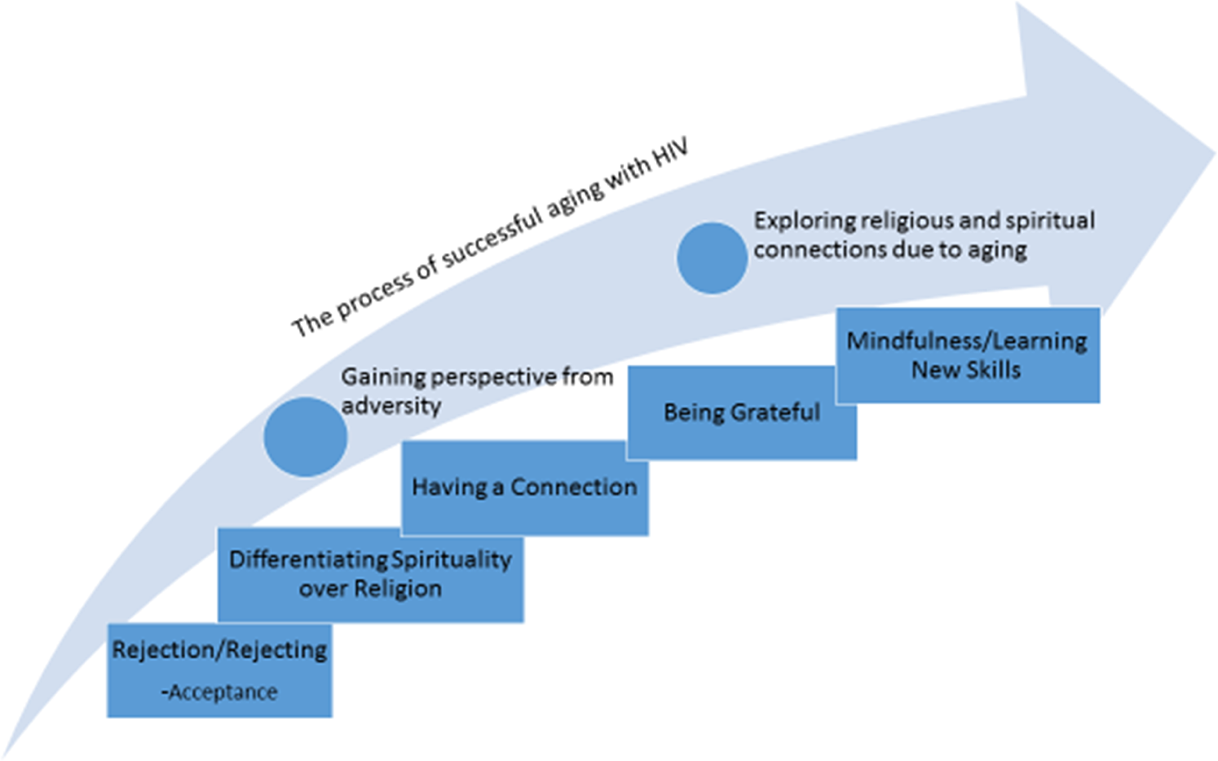
HIV as a spiritual journey.
Results
Sample Characteristics
Participants ranged in age from 50 to 73 years (M = 58, standard deviation [SD] = 6.1) were predominantly male (66.7%) and White (66.7%). Thirteen percent were Black Canadians, some of whom were immigrants to Canada from endemic African countries. Eighteen individuals identified as gay, 10 as heterosexual and 2 as bisexual. No one recruited into the study identified as transgender. The mean time since the first HIV diagnosis was 18 years (range = 4–30, SD = 7.6). Over half (56.6%) were diagnosed before HAART became available in 1996. Slightly less than two thirds of participants had education that equaled high school or less and had annual incomes of $30,000 CAD or less (at the time, the average annual income in Ontario is $49,000). Seventy percent were currently unemployed, retired, or receiving disability benefits. Sixty percent lived alone; one third were married or in a partnered relationship. Sample characteristics are shown in Table 1.
Sample Characteristics.

Note. SD = standard deviation; HIV = human immunodeficiency virus, HS = high school.
Qualitative Findings
Our analysis of the qualitative findings resulted in one major category supported by five properties (Figure 1). The main category or overarching social process was that of spirituality and religion being part of a spiritual journey set within the context of aging with HIV. Descriptions of religion and spirituality encapsulated the idea of a journey which had two components: (1) the long-term HIV survivor profile combined with (2) the experience of aging itself. The long-term survivor experiences incorporated ideas about HIV being a catalyst for a journey in which participants gained perspective from and found meaning in adversity. For example, George (a 70-year-old gay male) stated “all sorts of things get shoved at you…your ability to find meaning in that.” Participants spoke about how the experience of living with HIV, and having their life threatened by illness, inspired thankfulness and increased engagement with spiritual practices. Pinky, a 57-year-old female stated, “I went to bed and prayed and then I woke up and realized, yay I’m still alive and my mind is still functioning and I’m still in this world. I said, thank you Lord for one more day.”
The second component (the experience of aging itself) of the overall category of journey was associated with how aging shifted participants’ views, causing reflection similar to their experiences of adversity and creating more curiosity about spirituality. Participants explained that aging was a catalyst for examination of life which led to spiritual questions and increased interest in a connection to a higher power. Matia (54-year-old female) noted the change the aging process brings as altering their spiritual view saying “growing older, you appreciate stuff, the creation of it, people animals and plants.”
The category of HIV and aging as a spiritual journey was supported by five properties including (1) being rejected by as well as rejecting formalized religion, (2) differentiating religion from spirituality, (3) having or making a connection, (4) gratitude, and finally (5) mindfulness and the learning of new skills. What follows is a more complete description of these properties, supporting quotes placing them into the context of successful aging, and how those properties fit together to support the category of HIV as a spiritual journey.
Being Rejected by as well as Rejecting Formalized Religion
Participants in the study discussed the separation from organized religion was a two-way street. Many individuals had been rejected by churches or more formalized methods of worship based on “moral” grounds. As an example, Bob (male 64 years old) explained: “being a gay male, you were taught that you did not belong there.” Another described the environment where he was raised. Gregory, a 55-year-old male who emigrated from Jamaica, stated, I grew up in a highly religious society…I say religious, and not spiritual, a religious society and, in addition to that, a highly homophobic society. My being gay, I always had difficulties around whether God really loves gay men, or gays and lesbians.
Differentiating Religion From Spirituality
For many participants, particularly those who rejected formalized religion, it was important to distinguish religion from spirituality. Participants often identified as being spiritual, but not religious. They often noted the importance of connection in their spiritual practices. Some believed that religion separates people instead of forming those needed connections. For instance, one participant noted that he believed that “Religion disconnects.” While another stated “I don’t like the idea of formal attendance. I don’t get connected there.”
Some participants voiced feelings that were antireligion and/or anti-institutionalized religion, and instead sought opportunities for spiritual connection, either privately or within spiritual communities. Gregory simply said, “I’m strong spiritually, not religious.” For some, it was not so much an antireligion stance but rather needing a freer, more open way to explore meaning. Herb (age 59) described this as, “I don’t belong to any denomination…I don’t like to say religion…spirituality for me is open.” Some found a more spiritual view evolved out of previous religious involvement. For example, George stated that he “had a spiritual base” which was grounded in a highly religious upbringing. Although he no longer practiced formal religion due to “intellectual objections,” this spiritual home was very much a part of his “psyche.”
Having a Connection
A substantial number of individuals identified being connected to other people, beings, and even the earth as an essential part of their spirituality. Here the importance of spirituality went beyond a connection to God—which also occurred—but included a deep connection to something outside of themselves, something bigger, whether sentient or not. Participants talked about connections to people, music, animals, and plants in addition to what they perceived as God. For example, Gregory said, “I have a very personal relationship with God, who I consider my higher power.” Alexander, a 66-year-old male, discussed his connection to something outside himself that had importance, “I believe in something, I don’t know really what it is, but I talk to something. It’s not somebody, it’s something I talk to.” Mar, a 54-year-old immigrant from Asia, talked about a broad spiritual connection to various parts of the physical world. She said, “I’m loving the animals, I love the flowers, I love the people. I’m always thinking I am a mother.” Another individual found their spiritual connection through music. Herb said, “And music has also a lot of spirituality too because it connects with my emotions and it fills my spirit and it makes me feel good.” As spirituality is defined as a universal and fundamental quality that involves the search for meaning, purpose, morality, and a relationship with ourselves, others, and ultimate reality (Canda & Furman, 2010), we can see how the importance of connection to others, nature, and “something” is for these individuals. It also speaks to the importance of seeing and allowing diversity within the context of what any individual may identify as spiritual.
Feeling Grateful
A number of participants voiced what we ultimately termed feeling grateful or the expression of gratitude. This property included feelings of optimism, giving back to others, and seeing life through a positive lens. This feeling was grounded in their ability to survive for many years in the face of HIV infection. Alexander noted, “I thank God for the day that I’ve had, and say, I’m thankful for surviving this day, and I hope that I survive another day.”
Gratitude also came in the form of serving others as a means of paying back for what participants had received. Pinky stated, For me, it’s a personal spiritual journey and my belief that I was born a spiritual being but there are certain things that God has been doing for me and in return I have to really give back, I have to show God that yeah I am grateful for what he has done for me.
Mindfulness Practices—Learning New Skills
Many commented on practicing meditation in general and mindfulness specifically. Participants discussed mindfulness as a new, learned skill that helped them to cope with body changes and psychosocial issues associated with HIV disease. Mindfulness was said to assist in dealing with physical issues (insomnia and lipodystrophy), negative emotions, and internalized homophobia. For some, mindfulness was a new skill participants sought out, which aided them in learning to live in the moment. The use and integration of mindfulness (meditation) practice was useful in dealing with physical manifestations of health issues. Boulos (55-year-old gay male) said, “The lipoatrophy caused me tremendous grief, and it was through mindfulness meditation that I was able to find the relief that I was seeking just to be able to be in the world.” Mindfulness practice was also described as an effective strategy for dealing with side effects of HIV medication and age-related changes such as sleep disturbance. Neil (age 52) said, I don’t know if it’s my age, but something has changed, and I don’t sleep as well as I used to. I use mindfulness techniques now to help me relax and get back to sleep again so that’s how I use it. He’s a gay Buddhist, and he’s the one who taught this mindfulness meditation to a group of HIV positive men. I think that was really a turning point for me because I was tremendously weighed down by the anxiety caused by the changes in my appearance, and increased homophobia, etcetera. That I think has really been a saving grace for me so that’s one place where I would say.
Discussion
The HIV and Aging Working Group (High et al., 2012) has identified successful aging with HIV as an important research agenda, emphasizing how spirituality and mindfulness contribute to the processes of successful aging. In this study, we have obtained qualitative data from 30 individuals aging with HIV to help elucidate the importance of spirituality from an emic perspective. This study addressed how religion and spirituality fit into the process of successful aging with HIV and unearthed a deeper understanding of the processes and considerations that researchers and practitioners should consider when approaching individuals aging with HIV.
A substantial number of participants viewed the relationship with religion and spirituality as a journey, suggesting it takes place over time and is an evolving process. This is clearly seen in the negotiation of self that individuals experienced when addressing religion, sexual orientation, and/or HIV status in their own lives. As we found, the rejection that existed between religion and these individuals went both ways, ultimately leading to some type of recalibration of the relationship. This finding reinforces Siegel and Scrimshaw (2002) when they caution us not to assume that gay and bisexual men living with HIV will reject religion. What we found was that the relationship between the individual and organized religion had fluidity and transformation. Some found a balance with organized religion, such as a more accepting faith community, while others moved to a more open and loosely defined sense of spirituality. In addition, our study found that a parting between organized religion and the individual does not negate the need for spiritual nourishment that may be found in other ways. There appeared to be a dynamic interplay between the rejection of organized religion, the acceptance of the self, and newfound ways of being spiritual and finding community. As suggested by Brennan (2008), continued involvement in religion and spirituality after an HIV diagnosis may require a reformulation of one’s spiritual identity.
The importance of creating connections for the person living with HIV was an important element and one that is consistent with the concepts of spirituality. As Canda and Furman (2010) note, an important element of spirituality is creating relationships with ourselves, others, and ultimate reality, and this does not presuppose that relationship is with a higher power or God. Our informants discussed the importance of relationships with others, music, plants, and animals as well as what some termed their “higher power.” A number of our respondents had significant substance use histories and were currently in recovery. Therefore, it is important to recognize the influence that the recovery movement may have on their development of spiritual ideals.
A number of the participants in this study spoke of a sense of gratitude and thankfulness for their lives, including their HIV infection. Siegel and Scrimshaw (2002) identified that older adults in their study felt acceptance and affirmation of their self-worth through their belief system. Our participants felt gratitude for the opportunity to age (a process they did not expect to experience) but also noted the importance of giving back to others. This need to give back is consistent with a component of what Crowther, Parker, Achenbaum, Larimore, and Koenig (2002) referred to as positive spirituality in the model of successful aging. Other studies of successful aging among older adults with HIV point to the importance of giving back to the community (Siegel & Scrimshaw, 2002; Vance et al., 2008), but these studies have not framed it in the context of spirituality.
Although much aging literature has, historically, focused on decline and deterioration, emerging research has focused on gains later in life, particularly among those living with chronic or life-threatening illnesses (Romo et al., 2012). Explorations of gratitude in the face of HIV illness may be notable among older adults, particularly in long-term survivors who have seen many of their peers die during the height of the HIV crisis in North America. Studies on gratitude and aging have shown that gratitude has both physical and mental health benefits for older adults (Emmons & McCullough, 2004). Studies on older adults have emphasized that health can be perceived more of a “state of mind” as one ages, with less emphasis placed on the aging body and physical health conditions presented by health-care providers (Van Maanen, 2006).
Many of our participants focused on spiritual practices as a way of learning new skills and coping with stress. Studies on stress and aging have shown that daily stress is lessened in the lives of older adults who show gratitude toward God (Krause, 2006). Recent research has examined the effects of a multicomponent intervention that increases positive affect through learning new skills, such as noticing positive events, capitalizing, and gratitude. Participants living with HIV in one study were able to achieve important increases in their reported positive affect and decrease their reported negative affect (Moskowitz et al., 2011). Similar studies have been conducted on testing the impact of a gratitude intervention to enhance well-being among older adults and have found similar positive results (Killen& Macaskill, 2015). However, studies examining the efficacy of gratitude interventions among older adults living with HIV are scarce and require further development.
Participants in this study called upon practical tools for everyday life that were grounded in spirituality—mindfulness practice and meditation. The individuals in our study had gained experience and oftentimes new skills related to these practices and applied them to aid in their adjustment to physical and emotional aspects of aging with HIV infection. Numerous studies point to the importance of prayer and meditation in adjusting and coping with HIV infection (Krok, 2014; Siegel & Scrimshaw, 2002; Trevino et al., 2010); however, these often focuses on the frequency with which the sample uses those techniques. In our study, participants shared specific benefits of learning meditation and mindfulness practice and how specifically they implemented it into their disease management. It is important to note that the participants in this study used these techniques to deal with both physical changes associated with HIV, physical changes associated with aging, and physical changes associated with emotional and psychosocial issues.
The findings from this research study have potential implications for both practice and policy with older adults living with HIV infection. First, it is clear that religion and spirituality is important to this population but uniquely individual. Attention and openness should be utilized when conducting assessments, being inclusive of various approaches to spirituality. The important and utility of mindfulness practice emerged from these interviews and should be considered as a potential source for improving coping and adjustment to HIV and age-related changes. Finally, on a more macro-level, efforts to encourage churches of all denominations to be more inclusive and affirming of PLWHIV infection and those of differing sexual orientations and gender identities continues to be important. Future research can examine the effectiveness of religious and spiritual practices on adjustment to life changes associated with HIV infection.
Limitations
This study provides important insight into the value of religion and spirituality in the process of aging well with HIV infection. The majority of the participants in this study specifically discussed the value of spirituality and religion in their personal process of attempting to age well with HIV. Despite the richness of these emic views and qualitative data, the study has important limitations. First, the study, being framed in the qualitative paradigm, makes no attempt to suggest our findings are generalizable or are representative of older adults living with HIV. The notion of generalizability is contrary to qualitative research. All participants were recruited in the Greater Toronto/Hamilton area of Ontario, Canada, and may not reflect the views or experiences of those outside that area. The overall lack of diversity (particularly racial and ethnic diversity) should be noted as an additional limitation. Additionally, as one of the inclusion criteria for the study was that participants’ view that they are aging well, these data do not necessarily reflect the experiences of those struggling to age with HIV infection.
Conclusions
Overall, the present study reinforces the importance of both organized religion and spirituality in the lives of older adults living with HIV infection and elucidates the complexity of the relationship between those living with HIV infection and organized religion. Our findings underscore the importance of these domains in the lives of these individuals and reinforce the need for sensitive, thorough assessments of how spirituality and religion may play a role in the lives of older, HIV-positive adults. We need not only to engage individuals to share with researchers and practitioners how this helps or hinders their health but to do so openly without preconceived ideas of how that might look. Additionally, as we learned from these informants, techniques grounded in a spiritual tradition such as meditation and mindfulness practice can have an important place in interventions that may assist in the adjustment and coping with HIV in physical, emotional, and spiritual domains. Continued research is needed to unravel the complexity of the roles—both positive and negative—spirituality and religion play in the lives of older HIV-positive adults in general and more specifically how those realms can aid in successful aging.
Footnotes
Authors’ Note
During the data collection phase, the PI (CAE) was a Fulbright Visiting Research Chair at McMaster University, Hamilton, Ontario, Canada, and Visiting Faculty at the Factor-Inwentash Faculty of Social Work, University of Toronto.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a Fulbright Scholars grant from Fulbright Canada and a grant from the University of Washington Tacoma to C.A.E., principal investigator (PI).