
Abstract
Parenting research is frequently conducted without a thorough examination of socio-economic characteristics. In this study, longitudinal observations of positive parenting were conducted across six time points. Participants were 219 mothers of children with and without developmental delays. Mothers’ positive parenting increased during early and middle childhood in children with and without developmental delays. Mothers who reported more education had significantly higher levels of positive parenting when their children were 3 years old. Mothers who reported more family income grew at a significantly faster rate in positive parenting. There was preliminary support that mothers with more income were more likely to be members of a class that started off and remained at a higher level of positive parenting over time. Implications are discussed.
A growing number of individuals are spending their childhood years in socio-economic adversity (Delamonica & Minujin, 2007; Emerson et al., 2009). However, parenting research is often conducted without a thorough examination of socio-economic characteristics (Emerson, Hatton, Llewellyn, Blacher, & Graham, 2006). Parenting practices also can be affected by the ethnicity (Blacher, 2001) and psychological adjustment (Baker, Blacher, & Olsson, 2005) of mothers. The purpose of this study was to examine mothers’ parenting behaviors and to investigate the relationship between parenting behaviors and socio-economic variables (education, income), status variables (Anglo, Latino; typical development [TD], developmental delays [DD]) and maternal psychological variables (depressive symptoms, optimism).
Positive parenting
Over 40 years ago, Baumrind (1966, 1971) described negative and positive aspects of parenting styles. Since these seminal articles, there has been an increased focus on the detrimental effects of negative parenting (Ritchie & Buchanan, 2011). However, with intervention efforts primarily aimed at enhancing positive interactions between parents and children, there has been a concomitant increase in interest in the association between positive parenting and children’s outcomes. For example, with typically-developing children, mothers who showed high levels of warm responsiveness and low levels of restrictiveness had children with more optimal social and cognitive outcomes (Smith, Landry, & Swank, 2000). A meta-analysis by Dyches, Smith, Korth, Roper, and Mandleco (2012) suggested a moderate association between positive parenting and outcomes for children with DD.
One definition of positive parenting used in the literature includes positive affect, sensitivity, cognitive stimulation, and lack of detachment. We were particularly interested in this broad definition because of its dual benefits: 1) It encompasses several aspects previously linked to children’s outcomes and 2) It has been used with families of children with and without DD. For example, Fenning, Baker, Baker, and Crnic (2007) reported that mothers of children with borderline intelligence were less likely to exhibit this style of positive parenting in comparison to mothers of children with and without DD. Recently, longitudinal observations (child ages 3–5 years) were conducted using this definition of positive parenting in 183 mothers of children with and without DD. The authors reported that positive parenting was higher during free play and especially higher for children with Down syndrome. Additionally, more educated mothers were more positive with their children during a teaching task regardless of diagnostic group (Blacher, Baker, & Kaladjian, 2012).
Correlates of parenting
Research suggests the importance of economic adversity in putting families at risk, even more so, than aspects of disability or ethnicity (Emerson & Hatton, 2007; Emerson et al., 2009). Indeed, unsafe living conditions and stress caused by economic hardship can lead to more insensitive parenting, which is in turn associated with less favorable emotional and academic outcomes for typically-developing children (McLoyd, 1990, 1998). According to Emerson et al. (2006), exposure to socio-economic disadvantage may account for most or all of the risk of poorer mental health among mothers of children with DD as well as among individuals with DD themselves.
SES interacts with a multitude of other socio-cultural and psychological variables to impact parenting practices. For example, some immigrant Latino families live in low-income working-class neighborhoods that are viewed as relatively dangerous by its inhabitants (Reese, 2002). As a result, low-income Latina mothers of typically-developing youth reported that strictness is a strategy for protecting their children from the harmful social influences that they may encounter in the US (Reese, 2002; Wagner et al., 2008). For Latina mothers of children with DD, SES may limit access and utilization of appropriate services because of financial, linguistic, or ethnic barriers (Eisenhower & Blacher, 2006). Without appropriate services, it may be more difficult for Latina mothers to cope with the day-to-day stressors of a child with DD.
Further, depressive symptoms may impact the parenting behaviors of Latina mothers of children with and without DD. For example with typically-developing pre-adolescent children, symptoms of depression were linked to higher levels of maternal and paternal hostile parenting (i.e., rejection, control, and withdrawal) in both European and Mexican American families (Parke et al., 2004). Studies have shown that Latina mothers of children with DD reported more depressive symptoms compared to their Anglo counterparts (Blacher & McIntyre, 2006; Eisenhower & Blacher, 2006). Indeed, Latina mothers who did not receive help from family members (perhaps due to having a child with DD) may have felt the additional caretaking burden, which in turn made them more vulnerable to depression (Blacher, Lopez, Shapiro, & Fusco, 1997).
Relative to depressive symptoms, optimism has received less attention in the literature, but may also be related to parenting practices. For example, Koenig, Barry, and Kochanska (2010) reported that having an optimistic outlook was a helpful trait when rearing typically-developing, but anger-prone children. Specifically, mothers’ optimism was related to positive parenting practices (i.e., responsiveness and affectively positive interactions). Additionally, findings from Baker et al. (2005) indicated that when children with DD had moderate to high levels of behavioral problems, mothers who were classified as high in optimism reported the least stress while mothers who were classified as low in optimism reported the most stress. Further, Mexican-origin mothers reported hopeful visions and personal growth, despite the burden of caring for a child with a disability (Larson, 1998). In Latino families, the tendency to view children as not being responsible for their behavioral problems may contribute to maternal optimism (Chavira, Lopez, Blacher, & Shapiro, 2000).
Limitations of previous research and contributions of present study
Economic adversity, particularly as it impacts parenting practices, has received limited attention in the parenting literature (Emerson et al., 2009). This study examines various approaches to how SES might impact parenting practices. It is necessary to examine various approaches because of the inconsistent way this complex variable is measured. For example, some authors proposed that mothers’ education and family income can have a direct impact on parenting and, therefore, measured these as continuous variables. For example, education is measured as the number of grades completed in Fenning et al. (2007). Other authors proposed that education and income are categorical (Pelchat, Bisson, Bois, & Saucier, 2003). Specifically, Pelchat et al. (2003) divided education into uncompleted secondary education or less, completed secondary education, or college degree or higher, whereas Ispa et al. (2004) divided education into less than high school, high school, or more than high school. However, imposing a category on education and income implies that these variables have an indirect impact on parenting (e.g. education impacts parenting via the categories of low, medium, or high). It is also possible that mothers’ education and family income can have both a direct and indirect impact.
Determining how to measure SES a priori may be associated with different outcomes. In Stoneman (2007), there was a Down syndrome advantage (i.e., parents of children with Down syndrome experienced greater well-being) when income was not considered. However after variance attributable to income was removed, the Down syndrome advantage disappeared. Although this study does not examine the direct vs. indirect effects of SES, it does suggest that the measurement of SES can be differentially associated with outcomes. Braveman, Cubbin, Marchi, Egerter, and Chavez (2001) further examined this differential impact by investigating racial/ethnic disparities in health indicators using various logistic models that incorporated continuous or categorical measurements of income and mother’s education. Their results indicated that Latino mothers were at significantly greater risk of delayed prenatal care than European/Middle Eastern women when income was measured as a continuous variable, but not when income was measured in categories. In contrast, the risk of delayed prenatal care was similar for Latino and European/Middle Eastern women when education was measured in categories, but Latino mothers were more likely than European/Middle Eastern women to have delayed prenatal care when education was measured as a continuous variable. Therefore, the measurement of SES as a continuous or categorical variable may be related to differential conclusions. To date, there are no studies to our knowledge that empirically examine direct vs. indirect vs. direct-indirect effects of SES. However, in the event that there is a direct-indirect impact, this would suggest that SES indicators directly impact the outcome, as well as impact the outcome through specified categories (Braveman et al., 2001).
Researchers have acknowledged the multifunctional nature of SES (Adler & Ostrove, 2006), urging the field to empirically test how conclusions may vary depending on how SES is measured. In response to this call, the goal of the present study was to examine direct, indirect and combined direct-indirect effects of SES on parenting practices. Parenting was assessed via observations of parenting behaviors during an unstructured task at home when children were 3, 4, 5, 6, 7, and 8 years old. Specifically, we examined the longitudinal trajectories of positive parenting behaviors and their relationship to socio-economic variables (education, income), status variables (Anglo, Latino; TD, DD) and maternal psychological variables (depressive symptoms, optimism).
Method
Participants
Participants were drawn from a larger study (N = 260) of young children aged 3–15 years old. Targets in the TD group were recruited from preschools and day care programs. Targets in the DD group were recruited through community agencies providing services for individuals with disabilities. Selection criteria were that children had to be between 30 and 40 months of age. In the TD group, targets were excluded if they had a disability of any kind or premature birth. In the DD group, targets were excluded if they could not walk, had autism, or an IQ below 40.
When the children were 3 years old, they were administered the Bayley II. Children classified as having DD had a cognitive assessment score of 84 or lower. Children categorized as TD had a cognitive assessment score of 85 or higher. There was a subsequent assessment when children were 5 years old, using both a cognitive assessment and an adaptive behavior assessment. A chi-square test determined no statistically significant difference between the frequency of children with TD or DD in the 3- and 5-year assessments (chi-square (1) = 2.01, p > .05). Therefore, disability status at age 3 was chosen to examine whether having a child with DD impacted mothers’ positive parenting behaviors.
This study consisted of 219 families (i.e., 84% of the original sample). There were no statistically significant differences between participants included and excluded from the present study. Of the 219 families, 112 families had a child with DD and 107 families had a child with TD. In the combined sample, 60% of the targets were boys and 40% of the targets were girls. Child age at intake averaged 35.09 months (SD = 2.89). The majority of children (93%) were in good or excellent health. Most mothers (84%) were married and averaged about 15 years of school; 56% of them reported working outside of the home. Many of the families (74%) reported having more than one child. Approximately 48% of families had an annual income of more than $50,000. There were 168 Anglo families and 51 Latino families. Table 1 shows that Anglo mothers reported completing more grades (15.3) than Latina mothers (13.5); t(217) = 4.54, p < .001. More Anglo families reported having an annual income of $50,000 or higher (52.9%) than Latino families (36.7%); chi-square (1) = 3.90, p < .05. Confidence intervals were also examined to confirm these differences.
Demographic characteristics.
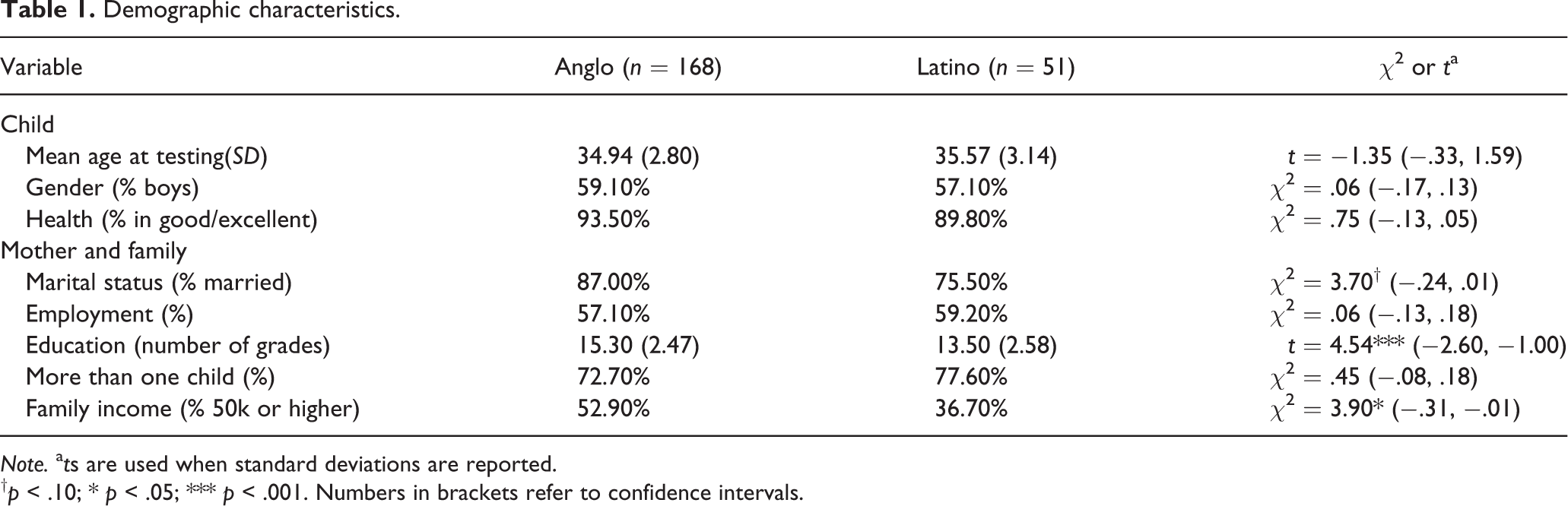
Note. a ts are used when standard deviations are reported.
Procedures
All procedures were approved by the Institutional Review Board. At the initial home assessment, research assistants visited the family to obtain consent and to administer the Bayley II. Subsequent home visits were scheduled around dinnertime. There were questionnaire packets completed by parents, which included a demographic form from which we determined ethnic status, mothers’ education, and family income.
Measures
Bayley scales of infant development second edition (Bayley II)
The Bayley II is a widely used measure of mental and motor development in children ages 1 to 42 months. Only the mental development items were administered when the child was 36 months old. Bayley reported high short-term test-retest reliability (0.91) for the MDI. With children aged 36–42 months, the MDI correlated well with the Full Scale IQ of the WPPSI-R, r = .73 (Bayley, 1993).
Center for epidemiologic studies depression scale (CES-D)
The CES-D is a 20-item self-report scale designed to measure depressive symptoms of mood, feelings, and perceptions. Participants were asked to rate each item based on how they felt or behaved during the past week. A Likert scale ranging from 0 (rarely or none of the time) to 3 (most or all of the time) is used. The scoring range is from 0 to 60, with higher scores indicating greater depressive symptoms. The CES-D has high internal consistency (.90) and acceptable test-retest reliability (.70), as well as convergent and divergent validity (Radloff, 1977). The CES-D was completed by mothers when their children were 3 years old. Cronbach’s alpha was .89.
Life orientation test-revised (LOT-R)
The LOT-R is a 10-item self-report measure of dispositional optimism. Participants were asked to rate each item on a Likert scale ranging from 0 (strongly disagree) to 4 (strongly agree). The scoring range is from 0 to 24, with higher scores indicating more optimism. The LOT-R has acceptable internal consistency (.78) and test-retest reliability (.79), as well as convergent and divergent validity (Scheier & Carver, 1985; Scheier, Carver, & Bridges, 1994). The LOT-R was completed by mothers when their children were 3 years old. Cronbach’s alpha was .81.
Parenting
Maternal parenting behaviors were coded using the Parent Child Interaction Rating System (Belsky, Crnic, & Gable, 1995), which evaluates six dimensions of parenting. Positive affect was observed in tone of voice, facial expressions, and affectionate acts. Sensitivity was reflected in mother’s awareness of what the child was doing and adjusting her behavior to take the child’s behavior into consideration. Cognitive stimulation was reflected by the extent to which the mother intellectually stimulated the child at his/her developmental level. Detachment was represented by the extent to which the mother was uninvolved/unresponsive toward the child. The dimensions were rated on a five-point scale ranging from 1 (not at all characteristic) to 5 (highly characteristic). The four aspects of parenting yield the broader dimension of positive parenting (Belsky et al., 1995; Fenning et al., 2007). Cronbach’s alpha for positive parenting was .90 (age 3), .89 (age 4), .85 (age 5), .86 (age 6), .82 (age 7), and .86 (age 8), with an average alpha of .86.
PCIRS coding (i.e., 10-minute observations separated by 5-minute ratings) was completed at six time-points and there was attrition across these time points. More specifically, the sample size at age 4 was 186, it was 199 at age 5 (more children were recruited at this age), 167 at age 6, 158 at age 7, and 152 at age 8. However, there was no relationship between the participants in each of the time points and the predictors of interest. The specific coding instructions remained constant across the time points. During the 3- and 4-year visits, the observation time was 90 minutes. During the 5-year visits, the observation time was 60 minutes. During the 6-, 7-, and 8-year visits, the observation time was 30 minutes. To increase reliability, the ratings were averaged for each visit. For each time point, there were different observers. Given the normal changes in graduate student research assistants over the 6 years of this study, the correlations for positive parenting across time were still moderate, ranging from .24 to .60. Reliability was established when there was 70% exact agreement with the primary coder from that time period and 95% agreement within one scale point.
Results
To what extent do mothers’ positive parenting behaviors change across early and middle childhood?
The models were fit to the data using Mplus via full information maximum likelihood to deal with missing data (Muthén & Muthén, 2006). Latent curve analysis was chosen to investigate the change over time. Specifically, the Level and Shape model was used because it does not a priori assume a particular change trajectory. The Level factor represented individuals’ scores of positive parenting at the beginning of the study. The Shape factor represented change in positive parenting across the repeated measurements. The loading on the first time point (age 3) was fixed to 0 and the loading on the last time point (age 8) was fixed to 1. The arrows indicating the rest of the loadings on the Shape factor represented the proportion of change relative to the total change occurring over all of the time points (Raykov & Marcoulides, 2006) (Figure 1).
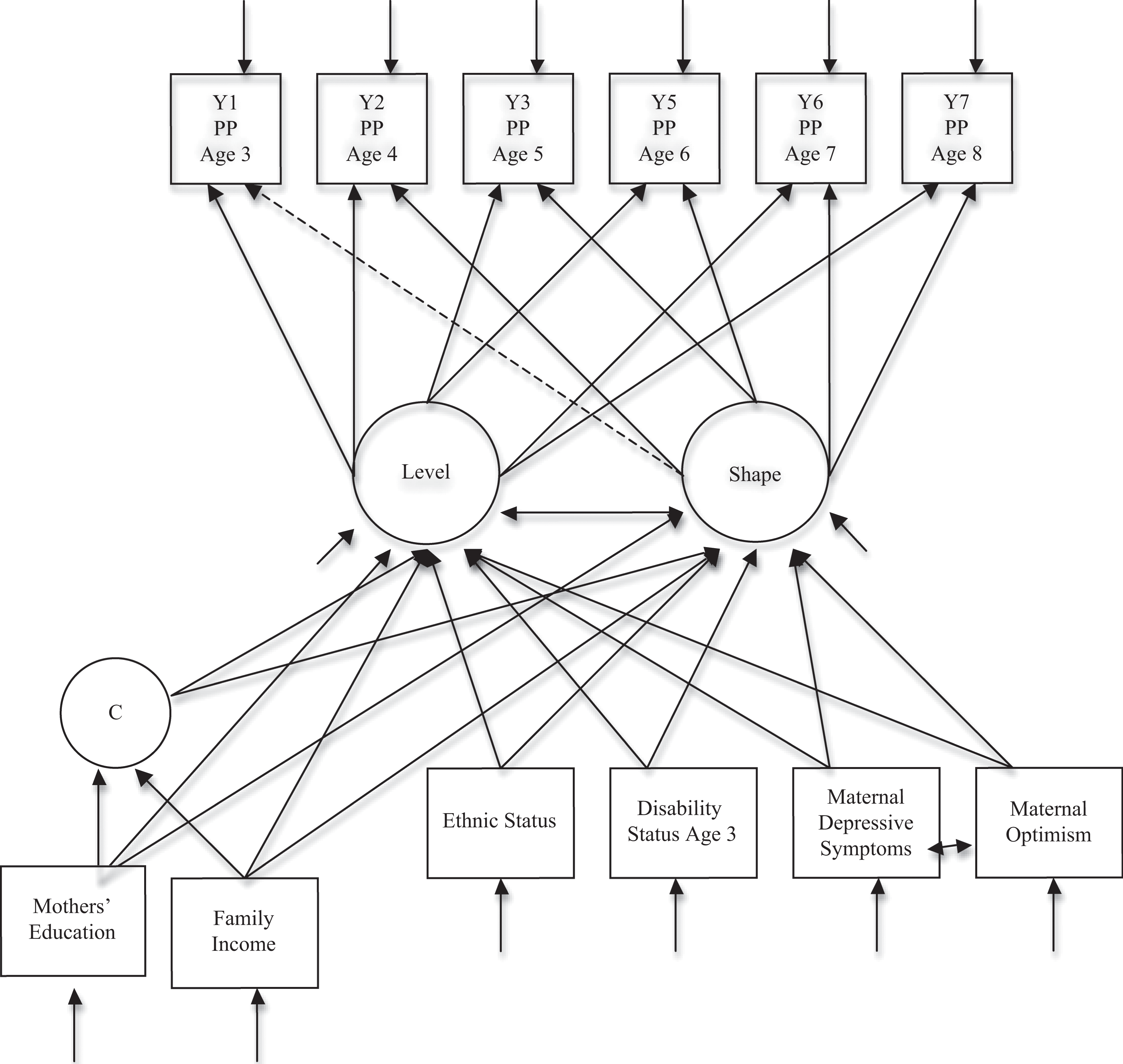
Latent growth mixture model with mothers' education and family income having direct and indirect effects on level shape of positive parenting (PP).
Models with good fit have: 1) a chi-square value that is not significant in order to not reject the model, 2) a comparative fit index (CFI) greater than .90, and 3) a root-mean-square error of approximation (RMSEA) below .05 with the left endpoint of its 90% confidence interval being smaller than .05. Since the chi-square test is sensitive to sample size, greater emphasis was placed on the other fit criteria (Raykov & Marcoulides, 2006). The unconditional model (i.e., no predictors) provided the following criteria: χ2 = (13, N = 219) = 26.74 p < .05; CFI = .96; and RMSEA = .07 (.03; .11), indicating model fit.
The mean value for the Level factor (i.e., the average initial starting position) was μαy= 10.67, t = 60.15, p < .001. The variance on the Level factor was s2 = 3.94, t = 8.23, p < .001, reflecting significant individual differences at the beginning of the study. The relationship between the Level and Shape factors was not significant (covariance = −.53, t = −1.35, p = .177; correlation = −.25, t = −1.47, p = .141) and indicated that an individual’s positive parenting score at the end of the study was not related to their initial parenting score. The estimated factor loadings representing the proportion of change relative to the total change occurring over all time points were 0, 0, −.22, −.31, .65, and 1. (Note that the first time point, age 3, and the second time point, age 4, were both fixed to 0, due to the lack of significant difference between these means.) Specifically, there was a significant decline in positive parenting from age 4 to age 5 (−.22, p = .024); significant decline in positive parenting from age 4 to age 6 (−.31, p = .008); and significant growth in positive parenting from age 4 to 7 (.65, p < .001). The mean value for the Shape factor was positive and significantly different from zero (μβy= 1.98, t = 8.32, p < .001), indicating that overall there was growth in mothers’ positive parenting from the initial mean value on the Level factor (μαy = 10.67). There was a trend for the variance on the Shape factor, s2 = 1.19, t = 1.71, p = .088 (Table 2).
Unconditional model results.
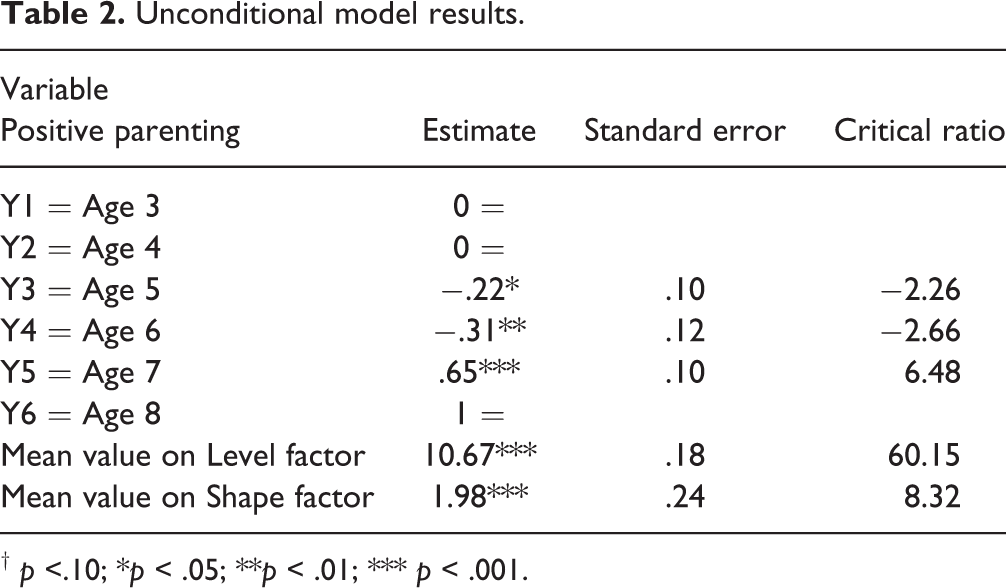
† p <.10; *p < .05; **p < .01; *** p < .001.
To what extent can positive parenting be directly predicted by socio-economic variables, status variables, or maternal psychological variables?
The conditional model includes predictors (Raykov & Marcoulides, 2006). Specifically, it included mother’s education, family income, ethnic status, disability status at age 3, depressive symptoms, and optimism. Mothers’ education was measured with the number of grades completed. Income was measured with the following groups: less than $35,000, $35,001 to $70,000, and over $75,001. Ethnic status was measured with 0 indicating Anglo mothers and 1 indicating Latina mothers. Disability status at age 3 was measured with 0 indicating children with TD and 1 indicating children with DD. The degree of depressive symptomatology was measured using the CES-D. Optimism was measured using the LOT-R.
The conditional model provided the following fit criteria: χ2 = (37, N = 219) = 74.29 p < .001; CFI = .91; and RMSEA = .07 (.05; .09), indicating good model fit. Mothers’ education significantly predicted the Level factor (γ = .20, p = .003), suggesting that mothers’ reporting more education had significantly higher initial values on positive parenting. Maternal depressive symptoms significantly predicted the Level factor (γ = −.04, p = .028), indicating mothers who reported more depressive symptoms had significantly lower initial values on positive parenting. Family income predicted the Shape factor (γ = .66, p = .006), suggesting that mothers who reported more family income made significantly more growth in positive parenting over time.
To what extent can positive parenting be indirectly predicted by socio-economic variables and directly predicted by status variables or maternal psychological variables?
Latent class analysis was used as a preliminary step because group membership on mothers’ education and family income was not known beforehand. When group membership is inferred from the data, the groups are referred to as latent classes. The Bayesian Information Criterion (BIC) index was used to examine model fit of two, three, etc. classes of education/income in comparison to the model fit of one education/income class. The BIC values were as follows: one-class model = 1557.06, two-class model = 1483.73, and three-class model = 1499.15. The model with two classes of education/income was the best fit to the data because it had the smallest BIC index (Marcoulides & Heck, 2009). The final classification of individuals was 48.4% in Class 1 and 51.6% in Class 2.
Latent growth mixture models (LGMM) posit that the Level and Shape factors are different for different classes. LGMM extends latent curve analysis to include latent class analysis (Marcoulides & Heck, 2009). The class invariant estimates suggested that maternal optimism significantly predicted the Level factor (γ = .10, p = .025), indicating that mothers who reported more optimism had significantly higher initial values on positive parenting. Maternal optimism predicted the Shape factor (γ = .08, p = .048), suggesting that mothers’ who reported more optimism made significantly more growth in positive parenting over time.
Regarding class membership, the log odds for mothers’ education was .07 (p = .457) and the log odds for income was .63 (p = .101). With respect to the reference group (Class 1), this suggested a trend such that mothers with more income were more likely to be members of Class 2. The odds of being in Class 2 based on the income variable was 1.88 times larger than the odds of being in Class 1; that is, they increased by 88%. For Class 1, the mean value for the Level factor was μαy = 9.17, t = 72.70, p < .001, and the mean value on the Shape factor was positive and significantly different from zero (μαy = 1.97, t = 28.14, p < .001). For Class 2, the mean value on the Level factor was μαy = 10.99, t = 86.54, p < .001, and the mean value on the Shape factor was positive and significantly different from zero (μαy = 1.92, t = 27.43, p < .001).
To what extent can the level and trajectories of positive parenting be directly and indirectly predicted by socio-economic variables and directly predicted by status variables or maternal psychological variables?
In this research question, mothers’ education and family income were allowed to directly impact the Level and Shape factors. The class invariant estimates suggested that mothers’ education significantly predicted the Level factor (γ = .21, p = .002), indicating that mothers’ who reported more education had significantly higher initial values on positive parenting. Family income significantly predicted the Shape factor (γ = .67, p = .006), suggesting that mothers’ who reported more family income had significantly more growth in positive parenting over time.
Regarding class membership, the log odds for mothers’ education was .06 (p = .544) and the log odds for income was .65 (p = .077). With respect to the reference group (Class 1), this suggested a trend such that mothers’ with more income were more likely to be members of Class 2. The odds of being in Class 2 based on the income variable was 1.92 times larger than the odds of being in Class 1; that is, they increased by 92%. For Class 1, the mean value for the Level factor was μαy = 9.16, t = 73.87, p < .001, and the mean value on the Shape factor was positive and significantly different from zero (μαy = 1.95, t = 29.10, p < .001). For Class 2, the mean value on the Level factor was μαy = 10.99, t = 88.92, p < .001, and the mean value on the Shape factor was positive and significantly different from zero (μαy= 1.91, t = 28.50, p < .001) (Table 3).
Direct-indirect latent growth mixture model results.

† p < .10; *p < .05; **p < .01; ***p < .001.
Which model of SES was the best fit to the data?
Akaike Information Criterion (AIC) was used to determine which model of SES was the best fit. Specifically, the smaller the AIC index, the better the fit of the model (Raykov & Marcoulides, 2006). The AIC values were as follows: direct impact = 9449.86, indirect impact = 7424.62, and direct–indirect impact = 7409.97. The LGMM model with mothers’ education and family income having a direct and indirect impact on the Level and Shape factors was the best fit because it had the smallest AIC index. Figure 1 displays the final direct-indirect model tested. Figure 2 displays the class means and growth trajectories, which show that the two classes had a similar trajectory; however, mothers in Class 2 started off and remained at a higher level on positive parenting than mothers in Class 1. Since disability status did not contribute to differences in parenting, we refer to parents of children with and without DD in our discussion of the findings.
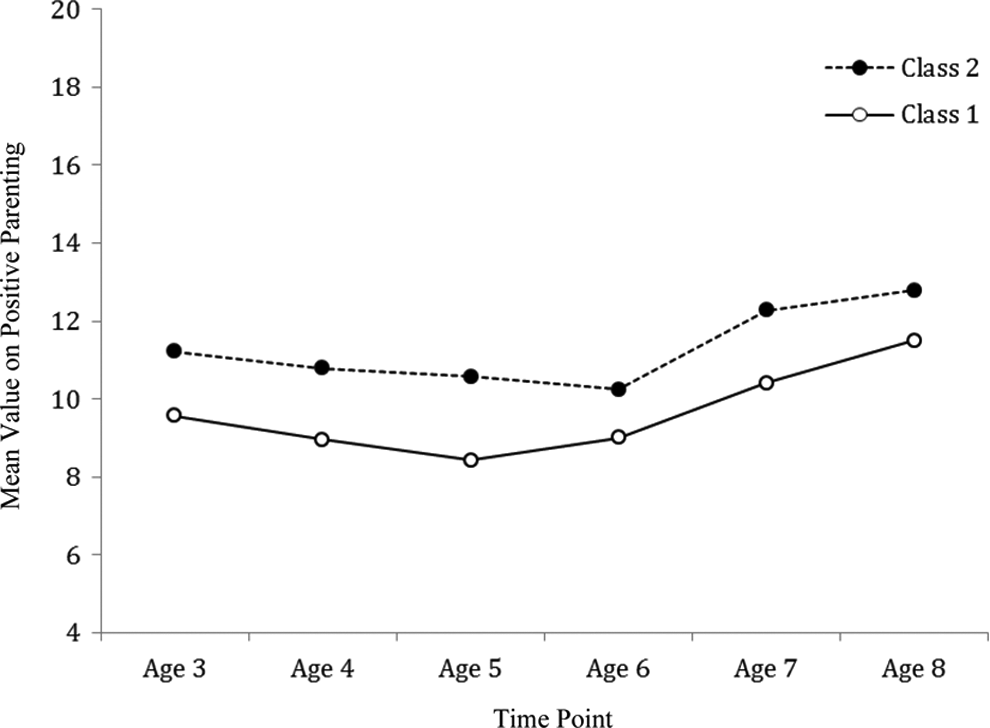
Estimated latent class means and growth trajectories for direct-indirect model
Discussion
The aim of the present study was to examine the longitudinal positive parenting behaviors of mothers, and to investigate the relationship between positive parenting and socio-economic variables (education, income), status variables (Anglo, Latino; TD, DD) and maternal psychological variables (depressive symptoms, optimism). Overall, the results indicated an increase in positive parenting over time, with particular emphasis on socio-economic characteristics. Our initial interest was to examine the extent to which mothers’ positive parenting changed across early and middle childhood. The results suggested that there was growth in mothers’ positive parenting across a 6-year period. When children were 3 years old, there were significant individual differences in the level of positive parenting. Subsequent analyses of three models of SES suggested that mothers’ education and family income had a direct and indirect impact on positive parenting. The results of the direct–indirect model suggested that mothers who reported more education had significantly higher initial values on positive parenting when their children were 3 years old. This finding is consistent with a longitudinal observational study of parenting with 1,041 mothers and their TD children, in which low SES (i.e., maternal education) was associated with poor parenting (defined using warmth, negativity, positive control, fairly similar to the present study) (Belsky et al., 2006).
This study also showed that education was related to the level (i.e., where mothers started off) in positive parenting. It is likely that mothers with more education were better able to understand the constellation and depth of factors that impacted their children’s development, especially from a young age (Eshbaugh et al., 2011), and therefore engaged in higher levels of positive parenting in early childhood. Another noteworthy finding from the direct–indirect model of SES was that mothers’ who reported more family income made significantly more growth in positive parenting over time. One probable explanation is that parents with higher income had more resources (e.g. opportunities to attend classes, read on the topic, hire a babysitter), and consequentially, were able to engage in positive parenting over time (Pelchat et al., 2003). Unfortunately, many families continue to live in income poverty (Delamonica & Minujin, 2007; Emerson et al., 2009). This is problematic considering that higher SES is related to more positive parenting at multiple ages throughout childhood (Smith et al., 2000).
The results of the present study are consistent with the literature on children with and without DD suggesting the powerful impact of socio-economic characteristics (Emerson et al., 2009; Emerson & Hatton, 2007; Halgunseth, Ispa, Rudy, 2006). Currently, the literature on parenting has either failed to address the nuanced effect of SES or controlled for the effects of SES (Emerson et al., 2006). However, failing to consider SES may mask or elevate findings, and consequentially, lead to faulty conclusions (Stoneman, 2007).
In the direct–indirect model of SES, there was a trend indicating that mothers with more income were more likely to be members of Class 2. Specifically with higher income, the odds of being in Class 2 were almost twice as likely as the odds of being in Class 1. Although the trajectories of positive parenting were similar in both classes, mothers in Class 2 started off and remained at a higher level of positive parenting than mothers in Class 1. The present study provided preliminary evidence that the socio-economic backgrounds of mothers, as measured by their educational attainment is important; however, it may be income poverty that has the powerful effect of differentiating groups (Emerson et al., 2009). Socio-economic characteristics function in a multifaceted and significant manner, and therefore, it is imperative for parenting researchers to take these attributes into consideration in order to provide ecologically and methodologically clear results.
The direct–indirect model of SES also suggested no association between the other variables of interest (i.e., ethnic status, disability status, depressive symptoms, and optimism) and positive parenting. The lack of association between ethnic status and positive parenting behaviors is consistent with prior studies that have indicated the loss of significant findings once SES is considered. For example, although there were significant differences between Anglo and Latino mothers with regard to the amount of modeling they used when teaching their 5-year-old typically-developing children, this difference disappeared when SES was controlled (Laosa, 1980). With regard to disability status, our lack of significant association between this construct and positive parenting behaviors is consistent with some studies and inconsistent with other studies. For example, research has shown that parents of children with intellectual disabilities display less positive affect than parents of children with typical development (Fenning et al., 2007). However, parents of children with intellectual disabilities also have been shown to adapt their interactions, language, and play (i.e., indicators of sensitivity) to match the developmental needs of their children (Childress, 2011). With regard to cognitive stimulation, there are inconsistent findings in the literature regarding whether parents of children with intellectual disabilities provide more cognitive stimulation than parents of children with typical development (Cuskelly, Jobling, Gilmore, & Glenn, 2006; Lambrechts, Leeuwen, Boonen, Maes, & Noens, 2011). It is difficult to draw general conclusions about positive parenting behaviors in families of children with intellectual disabilities because of the various findings reported. Given this variability, it is reasonable that our findings were consistent with some studies and inconsistent with others.
We did not find a significant relationship between mothers’ depressive symptoms and positive parenting behaviors or mother’s optimism and positive parenting behaviors. These findings are inconsistent with previous studies that have shown an association between mothers’ psychological states and parenting practices. For example, with typically-developing pre-adolescent children, symptoms of depression were linked to higher levels of maternal and paternal hostile parenting (i.e., rejection, control, and withdrawal) in both European and Mexican American families (Parke et al., 2004). In a sample of 119 mothers of children with autism spectrum disorders, Ekas, Lickenbrock and Whiteman (2010) reported that higher levels of optimism were associated with increased positive outcomes (increased positive affect, life satisfaction, and psychological well-being) and decreased negative outcomes (decreased depression, parenting stress, and negative affect). One probable reason for these inconsistent findings is the difference in methodology. Specifically, Parke et al. (2004) and Ekas et al. (2010) used questionnaires to examine mothers’ parenting behaviors, whereas the present study utilized direct observations to capture mothers’ behaviors. It is important to note that direct observations of parenting behaviors have been shown to have better psychometric properties than self-reported measures of parenting behaviors (Kochanska, Kuczynski, & Radke-Yarrow, 1989; McGuire & Earls, 1993; Zaslow et al., 2006).
As with any study, it is important to note the limitations. First, due to the complexity of the analyses, more in-depth investigations such as mediation or bi-direction, as well as the impact of SES on negative parenting, were not conducted. Promising areas of future research include examining a mediational model of parenting and investigating the transactional relationships between variables of interest on positive and negative parenting. Second, due to the sample size, it was not possible to examine within-group determinants of parenting practices. In the Latino population, cultural notions such as familismo, educacion, and respeto have been linked to parenting practices (Halgunseth et al, 2006). Another area of future research is to investigate whether cultural notions account for variance in parenting above and beyond SES. Third, we did not use comprehensive indicators to measure SES. Indicators of SES used in the literature include income, maternal/paternal education, maternal age, married vs. single parent, employment status, home ownership, housing quality, social activities, and the number of siblings in the household (Belsky et al., 2006; Chao & Kanatsu, 2008). It is likely that certain indicators of SES may be more salient for parenting than others (Chao & Kanatsu, 2008). In order to fully understand the impact of SES, future studies should measure it using multiple indicators.
Conclusion
Research has established the efficacy of treatment programs to increase positive parenting in families of children with and without DD (Feinfield & Baker, 2004; Landry, Smith, Swank, & Guttentag, 2008). Emerson and colleagues (Emerson et al., 2009) suggested that interventions must be accessible and effective for deprived families and communities. Otherwise, selective access and use of interventions will only increase the social inequalities already present. Ultimately, a more broad documentation of social context may lead to a better understanding of the complex associations between parenting, socio-economic characteristics, status variables, and maternal psychological well-being to design ecologically valid interventions.
Footnotes
*This article accepted during Marcel van Aken’s term as Editor-in-Chief.
Funding
This work was supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development [grant number: 34879-1459].