
Abstract
This longitudinal study explores differences between native Dutch and immigrant Moroccan adolescents in the relationship between internalizing and externalizing problems across time. By using generalized estimating equations (GEE), the strength and stability of associations between internalizing and externalizing problems in 159 Moroccan and 159 Dutch adolescents was studied over a period of 4 years. No differences in strength of co-occurring problems were found between Moroccan and Dutch adolescents. However, for Moroccan adolescents, associations between problems increased over time, whereas in Dutch adolescents, associations remained stable. The increase of co-occurring problems may be a result of undertreatment and increasing complexity of problems in Moroccans during adolescence. The results of this study imply that investigating processes leading to co-occurring problems in subgroups of adolescents, such as immigrant youths, is needed to optimize prevention and intervention efforts.
In both epidemiological and clinical samples, externalizing problems often co-occur with internalizing problems (Angold & Costello, 1993; Beyers & Loeber, 2003; Capaldi & Stoolmiller, 1999; Fergusson & Woodward, 2002; Ritakallio et al., 2008; Vermeiren, Deboutte, Ruchkin, & Schwab-Stone, 2002). Adolescents with co-occurring externalizing and internalizing problems comprise a highly vulnerable group being at extreme risk of demonstrating problems in various life domains, including school failure, violent behaviour, and adult psychiatric illness (Capaldi, 1992; Capaldi & Stoolmiller, 1999; McCarty, Stoep, Kuo, & McCauley, 2006). In addition, co-occurring problems may be related to poorer treatment success (Newman, Moffitt, Caspi, & Silva, 1998; Ollendick, Jarrett, Grills-Taquechel, Hovey, & Wolff, 2008).
In the past decades, ample research has provided important information about the mechanisms underlying the co-occurrence of internalizing and externalizing problems (for a review, see Boylan, Vaillancourt, Boyle, & Szatmari, 2007). With the development of advanced statistical techniques, the focus has mainly been on the causal relations between internalizing and externalizing problems in longitudinal study designs (e.g. Burt, Obradovic, Long, & Masten, 2008; Fanti & Henrich, 2010; Fergusson, Lynskey, & Horwood, 1996; Hutteman, Denissen, Asendorpf, & Van, 2009; Masten et al., 2005; Ritakallio et al., 2008). The development of the strength, and course of the associations itself, has received much less attention, and has been predominantly described in cross-sectional samples. However, it is known that adolescence as a developmental stage is marked by substantial fluctuation in both the expression and severity of problem behaviour (Angold & Costello, 1995; Costello, Mustillo, Erkanli, Keeler, & Angold, 2003; Hudziak, Achenbach, Althoff, & Pine, 2007). It is therefore not surprising that the level of problems, as well as the domains in which problems arise during adolescence, were found to vary (Burt et al., 2008; Denissen, Asendorpf, & van Aken, 2008; Hutteman et al., 2009). Accordingly, the strength and course of the co-occurring problems may also vary. Indeed, in the few studies that have been investigating the course and strength of the association of co-occurring internalizing and externalizing problems such variations have been found. Tolan and Henry (1996) found that rates of co-occurring problems among a sample of urban youth increased with age. Capaldi (1992) found that among a sample of at-risk boys, only 48% showed a stable pattern of co-occurring externalizing and internalizing problems during adolescence. Such variations over time may have implications for prevention and intervention efforts of co-occurring internalizing and externalizing problems, in that they need to be well timed and aimed at the appropriate risk groups.
Furthermore, it is likely that the prevalence of co-occurring internalizing and externalizing problems is not equally distributed across subgroups of adolescents: adolescents differ in the prevalence and impact of risk factors that are likely to influence mutual associations (e.g. Boylan et al., 2010; de Wit et al., 2008; Fergusson et al., 1996; Lee & Bukowski, 2011; Oland & Shaw, 2005; Ritakallio et al., 2008; Wiesner & Kim, 2006). For instance, immigrant youths are believed to be at an increased risk of developing both externalizing and internalizing problems (Anderson & Mayes, 2010; de Wit et al., 2008; McLaughlin, Hilt, & Nolen-Hoeksema, 2007; Reijneveld, Harland, Brugman, Verhulst, & Verloove-Vanhorick, 2005; G. W. J. M. Stevens & Vollebergh, 2008). Associations between internalizing and externalizing problems may therefore also differ in immigrant youths. Comparing the strength and course of associations between internalizing and externalizing problems in immigrant youths and native youths is therefore particularly interesting, because it is likely to enhance our knowledge on the possible variation of co-occurring internalizing and externalizing problems during adolescence. Gaining insight in differences in dynamics of co-occurring patterns between native and immigrant adolescents may provide a starting point for effective interventions that are well timed and directed at the appropriate risk groups.
In the Netherlands, adolescents with a Moroccan background (mostly second generation immigrants, further called Moroccan adolescents) are one of the largest and most disadvantaged immigrant groups (Dagevos, Gijsberts, & Van Praag, 2003). Therefore, associations across time between internalizing and externalizing problems among Moroccan immigrant adolescents compared to native Dutch adolescents are studied.
Since depression, generalized anxiety and social anxiety are the most common disorders in the general population and are likely to co-occur with externalizing problems (Bubier & Drabick, 2009; Costello et al., 2003; Rapee, Schniering, & Hudson, 2009; van Oort, Ormel, & Verhulst, 2012), we will compare strength of associations between depression, generalized anxiety and social anxiety with externalizing problems among Dutch and Moroccan adolescents.
The aim of this study was twofold: First, to compare the longitudinal associations over a 4-year period between internalizing and externalizing problems among Moroccan and Dutch adolescents. Second, to study the variation across time of these associations within both groups.
Methods
Participants and procedure
Participants were 159 Moroccan immigrant (75 boys, 84 girls, M age = 13.51 ± .55) and 159 native Dutch adolescents (75 boys, 84 girls, Mage = 13.02 ± .50). Participants were selected from the ongoing longitudinal RADAR study (Research on Adolescent Development And Relationships), a population based cohort study in the Netherlands. This study is designed to identify mechanisms of influence from the family and peer context on adolescent normal and abnormal behavioural development, including psychopathology. Participants were considered Moroccan if either the adolescent or one of the parents was born in Morocco. Young adolescents from the final year of elementary school were screened and selected to participate by means of the Teacher Report Form (TRF: Achenbach & Ruffle, 2000). Boys and girls at risk of developing externalizing behavioural problems (TRF borderline clinical cut-off t score ≥ 60) were over-sampled in the study. Assessments of participants began in 2006 when the adolescents were in the first grade of secondary school. Selected adolescents were visited at home by a trained interviewer. All participants and their parents provided informed consent, and were asked to fill in an annual battery of questionnaires during a home visit by trained interviewers. This procedure resulted in the inclusion of a total of 497 Dutch adolescents and 164 Moroccan adolescents. The RADAR study was approved by the medical ethical committee of Utrecht University.
For this study, Wave 1 to 4 were included (2006–2009). Participants with missing data on all waves concerning our measures of interest were excluded (Moroccan adolescents: n = 5). Adolescents from the Dutch sample with a foreign-born parent were excluded (n = 19). Furthermore, to increase socio-economic homogeneity between the Dutch and Moroccan sample, we matched the groups on socio-economic status (SES), accounting for the same proportions of high- and low-risk boys and girls in both samples. This resulted in the final sample of 159 Moroccan and 159 Dutch adolescents. Although we decreased the difference between SES of the Dutch and the Moroccan samples substantially, discrepancies were too large to fully match, and therefore we adjusted for SES in all analyses. Table 1 shows the descriptives of the final sample. Analyses revealed no differences in mean scores in outcome measures between those with complete data for the four waves and those who dropped out, suggesting that there was no selective attrition.
Sample descriptives.
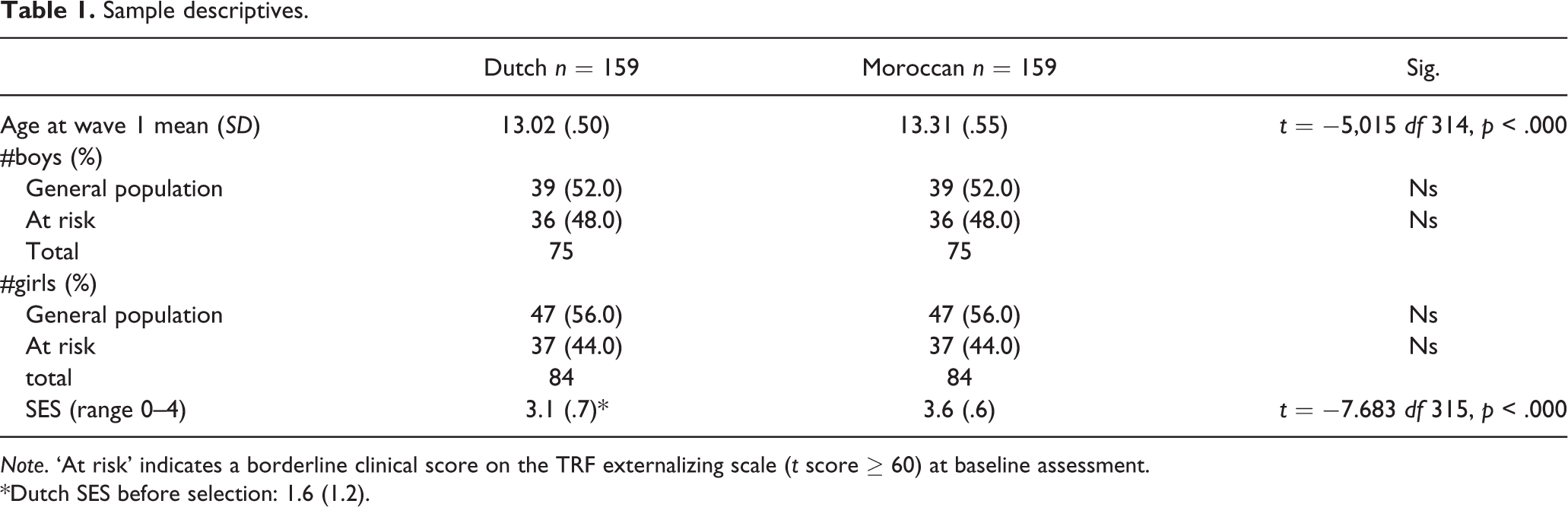
Note. ‘At risk’ indicates a borderline clinical score on the TRF externalizing scale (t score ≥ 60) at baseline assessment.
*Dutch SES before selection: 1.6 (1.2).
Measures
Externalizing problems
The externalizing problems scale of the Youth Self Report (YRS: Achenbach & Ruffle, 2000) was used to determine the adolescents’ externalizing behaviour problems. The externalizing problems scale of the YSR is based on the sum of the subscales Rule Breaking Behaviour (11 items) and Aggressive Behaviour (19 items). Items are scored on a 3-point scale (0 = not true, 1 = somewhat true, 2 = very true or often true). Good reliability and validity have been reported for the Dutch YSR version (Verhulst, Van der Ende, & Koot, 1996, 1997). Cronbach’s α’s in this sample were .86 for Dutch adolescents and .91 for Moroccan adolescents. To obtain a normal distribution of externalizing problems, t scores of the YSR were used in this study.
Internalizing problems
As for internalizing problems, the most common internalizing disorders—depression, generalized anxiety and social anxiety—were assessed. Depression was measured using the Reynolds Adolescent Depression Scale (RADS-2: Reynolds, 2002). This is a 30-item self-reported questionnaire containing four subscales: Dysphoric Mood (8 items), Anhedonia/Negative Affect (7 items), Negative Self Evaluation (8 items) and Somatic Complaints (7 items). Good validity and reliability have been reported in various international studies (Osman, Gutierrez, Bagge, Fang, & Emmerich, 2010). Items were scored on a 4-point scale, ranging from 1 = almost never to 4 = usually. Total scale scores were used in the analyses. Cronbach’s α’s in this sample were .88 for Dutch adolescents and .87 for Moroccan adolescents.
Information on anxiety was obtained by using the subscales Social Anxiety and Generalised Anxiety of the Screen for Child Anxiety Related Emotional Disorders (SCARED: Birmaher et al., 1997, 1999). The subscale Social Anxiety consists of 5 items with a Cronbach’s α of .72 for Dutch adolescents and .74 for Moroccan adolescents. The 8 item subscale Generalised Anxiety showed a Cronbach’s α of .82 for both Dutch and Moroccan adolescents.
Analyses
Mean scores of both internalizing and externalizing problems of all waves were compared between Dutch and Moroccan boys and between Dutch and Moroccan girls. Next, Generalised Estimating Equations (Zeger & Liang, 1986) were used to analyse the relation between internalizing and externalizing problems among Dutch and Moroccan adolescents during a 4-year period. This procedure fits the explorative and longitudinal character of our research aims and makes use of all available data (Ballinger, 2004). GEE is suitable to compare differences between groups, while Growth models are more suited to investigate individual trajectories. GEE takes into account the dependency of observations by specifying a “working correlation structure.” The correction for within subject correlations is carried out by assuming a priori correlation structure for the repeated measurements. Unlike mixed models, the correlation structure in GEE does not affect the marginal parameter estimates (Twisk, 2003). In general, the simplest structure which uses up the fewest degrees of freedom and reasonably fits the data is used. In this study, an exchangeable correlation structure was used for all analyses. GEE works as follows: first, a naive linear regression analysis is carried out, assuming the observations within subjects are independent. Then, residuals are calculated from the naive model (observed–predicted) and a working correlation matrix is estimated from these residuals. Then, the regression coefficients are refit, correcting for the correlation. In the case of continuous outcomes GEE with an exchangeable correlation structure result in the same parameter estimates as a mixed model where a random intercept is used to take into account intra-individual correlation. GEEs have the advantage of producing standard errors that are robust to misspecification of the correlation structure (Pan & Connett, 2002; Twisk, 2003).
For better interpretation, z scores of the RADS and both anxiety scales were used in the GEE analyses. Z scores of the internalizing measures were combined to a total internalizing problem scale.
First, main effects of the internalizing predictors of boys and girls on externalizing behaviour were calculated. The GEE approach pooled the repeated measures on the internalizing measures and on the externalizing measures to produce an estimate of the association between internalizing and externalizing problems for boys and girls during adolescence averaged over the four waves and the two ethnicities.
Next, an interaction term between ethnicity and the predictors was added to the models to investigate ethnic differences in the association between internalizing and externalizing problems in boys and girls.
The models considered up to this point, assume the association between internalizing and externalizing problems to be stable over time, which may not always be the case. Associations may increase or decrease over time. By adding a time interaction in the third, and last step of the model we can investigate whether associations are equal for each point in time (non-significant time interaction) or whether associations vary over time (significant time interaction), resulting in the three-ways interactions ethnicity × predictor × time. A significant time interaction therefore means that associations are not stable. Post-hoc analyses are presented to visualize differences in associations over time. To check the assumptions required for GEE analyses, we made separate QQ plots for the residuals for each of the six models fitted in step 3. We did this separately for each of the waves as residuals for the same subject are not independent in GEE analysis. Residuals were found to satisfy the normal assumption, indicating that any skewness of the outcome (if present at all) is explained by the predictors.
Gender interactions were also investigated. About a third of the analyses revealed gender interactions. Given the limitations of our sample size to test for four-way interactions (ethnicity × gender × predictor × time), our focus on ethnicity and to be able to present our results in a readable manner, we chose to report all results for boys and girls separately. We adjusted for SES by adding SES as a covariate in all our analyses.
Since power analyses for detecting interaction effects in longitudinal designs are not available and would require assumptions on the sizes of the regression coefficients and the correlation between them which are usually impossible to specify in advance, a standard rule of thumb for performing ordinary multiple linear regression—of which generalized estimating equations are an extension—is to include at least 10 observations per independent variable. Our sample sizes of 150 (boys) and 168 (girls) subjects with a total of 776 (boys) and 680 (girls) observations should therefore be more than sufficient to fit the largest models considered, containing a maximum of 8 variables. A significance level of p < .05 was used for all analyses. SPSS version 19 was used for all analyses.
Results
In Table 2, an overview of differences in mean scores on externalizing problems, depression, social and generalized anxiety for the four waves for both Dutch and Moroccan adolescents is presented separately for boys and girls. T tests revealed significant differences in externalizing problems between Dutch and Moroccan boys and between Dutch and Moroccan girls. Except for Moroccan girls at W2, lower levels of externalizing problems (YSR) were reported by the Moroccan adolescents. For depression (RADS), Moroccan boys reported lower levels of problems as compared to Dutch boys in W2 and W3, whereas no differences between Dutch and Moroccan boys were found regarding social and generalized anxiety (SCARED). Moroccan girls reported lower levels of depression (RADS) scores across waves than Dutch girls. Furthermore, as compared to Dutch girls, a lower mean score of social anxiety in W4 was reported by Moroccan girls, whereas no differences in generalized anxiety were found.
Ethnic differences in mean externalizing and internalizing problems scores for each wave for boys and girls.
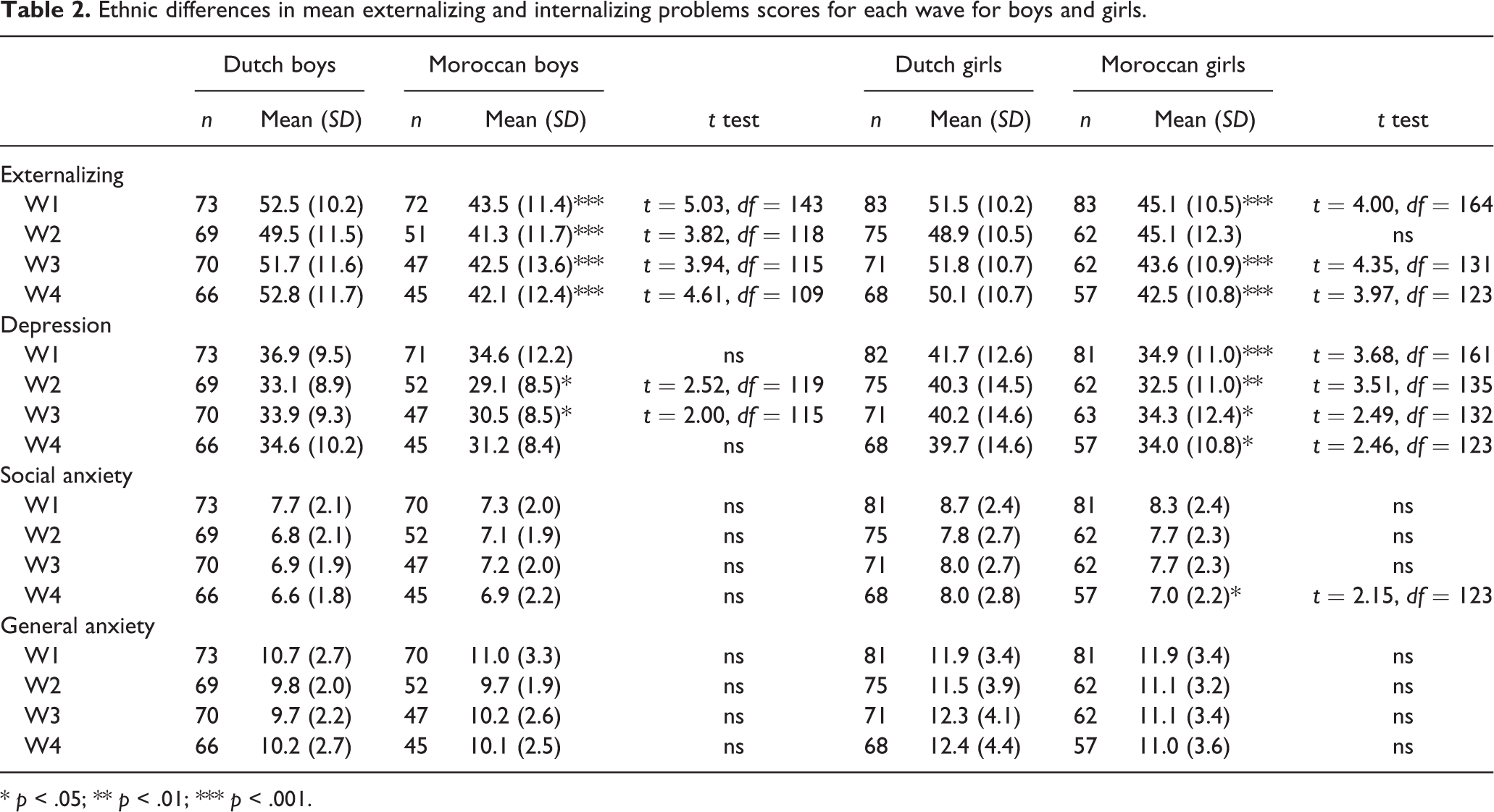
* p < .05; ** p < .01; *** p < .001.
Results from the GEE analyses of the longitudinal associations of internalizing and externalizing problems are shown in Table 3. Unstandardized beta coefficients and 95% confidence intervals are presented, adjusted for SES. In step 1 the main effects of total internalizing problems, depression, generalized anxiety and social anxiety associated with externalizing problems are presented for both boys and girls separately. Results showed longitudinal associations between all internalizing measures and externalizing behaviour in both boys and girls. The strongest association was found between depression and externalizing problems in both groups (boys: B = 4.2 CI 2.4–6.0; girls: B = 3.6, CI 2.6–4.6). This means that in boys, averaged over all time points, there is an average increase of 4.2 points and in girls of 3.6 points of the externalizing YSR score for every standard deviation increase of depression.
Linear GEE regression model for associations between internalizing and externalizing problems in boys and girls and interactions with ethnicity and time.
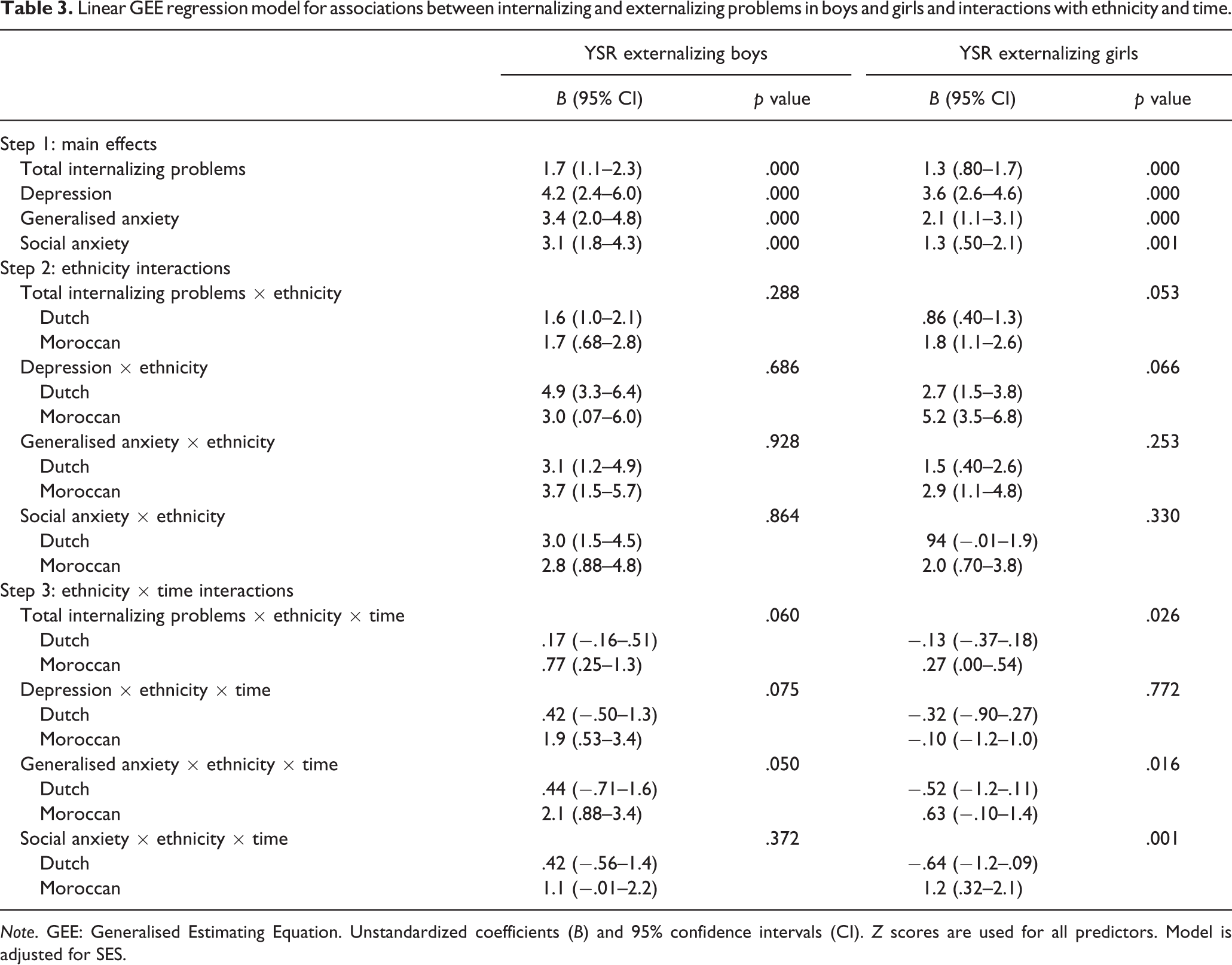
Note. GEE: Generalised Estimating Equation. Unstandardized coefficients (B) and 95% confidence intervals (CI). Z scores are used for all predictors. Model is adjusted for SES.
Then, ethnicity interactions were added to the model to investigate differences in associations between Dutch and Moroccan boys and between Dutch and Moroccan girls. Test statistics of these interactions are presented in the step 2 in Table 3. A visual presentation of these results of the separate internalizing measures is shown in Figure 1. Strength of the average associations over time was found to be similar across ethnicity, although the difference between Dutch and Moroccan girls total internalizing problems almost reached significance (p = .053) with stronger associations among Moroccan girls .
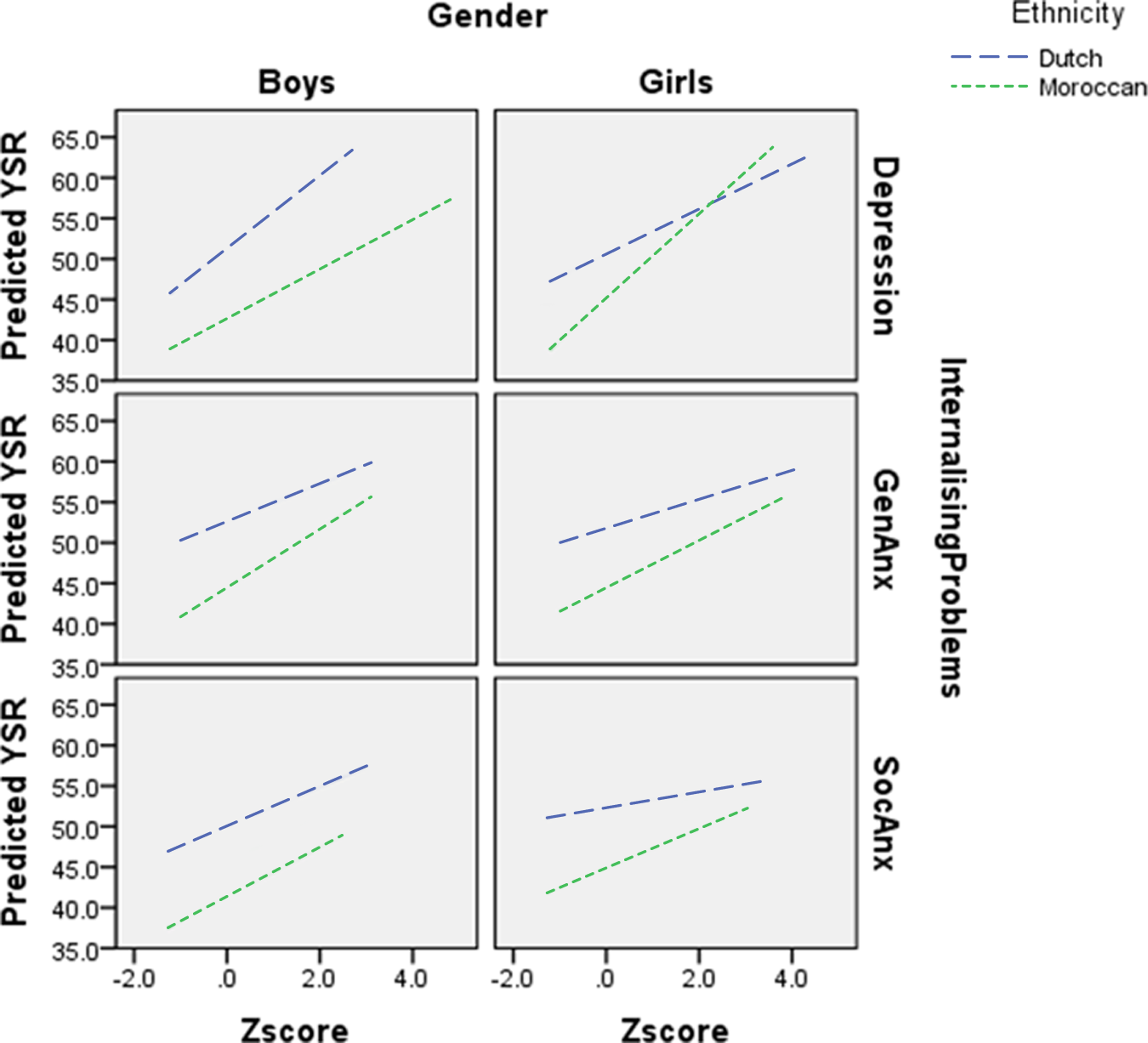
Linear GEE regression model for the associations between depression, generalized anxiety and social anxiety with and externalizing problems in Dutch and Moroccan adolescents.
Next, we added a time interaction to investigate whether the average associations that we found represented the association for each time point, indicating a stable association between internalizing and externalizing problems over time. Stable associations result in non-significant time interaction terms, whereas significant time interaction terms indicate increase or decrease of the strength of the association between internalizing and externalizing problems over time. This resulted in three-ways interactions between internalizing problems, time and ethnicity. Results are presented in step 3 of Table 3. A visual presentation of the results of the separate internalizing measures is shown in Figures 2 –4. No ethnic differences in course of co-occurring depression and externalizing problems were found for neither boys (p = .075) or girls (p = .772)
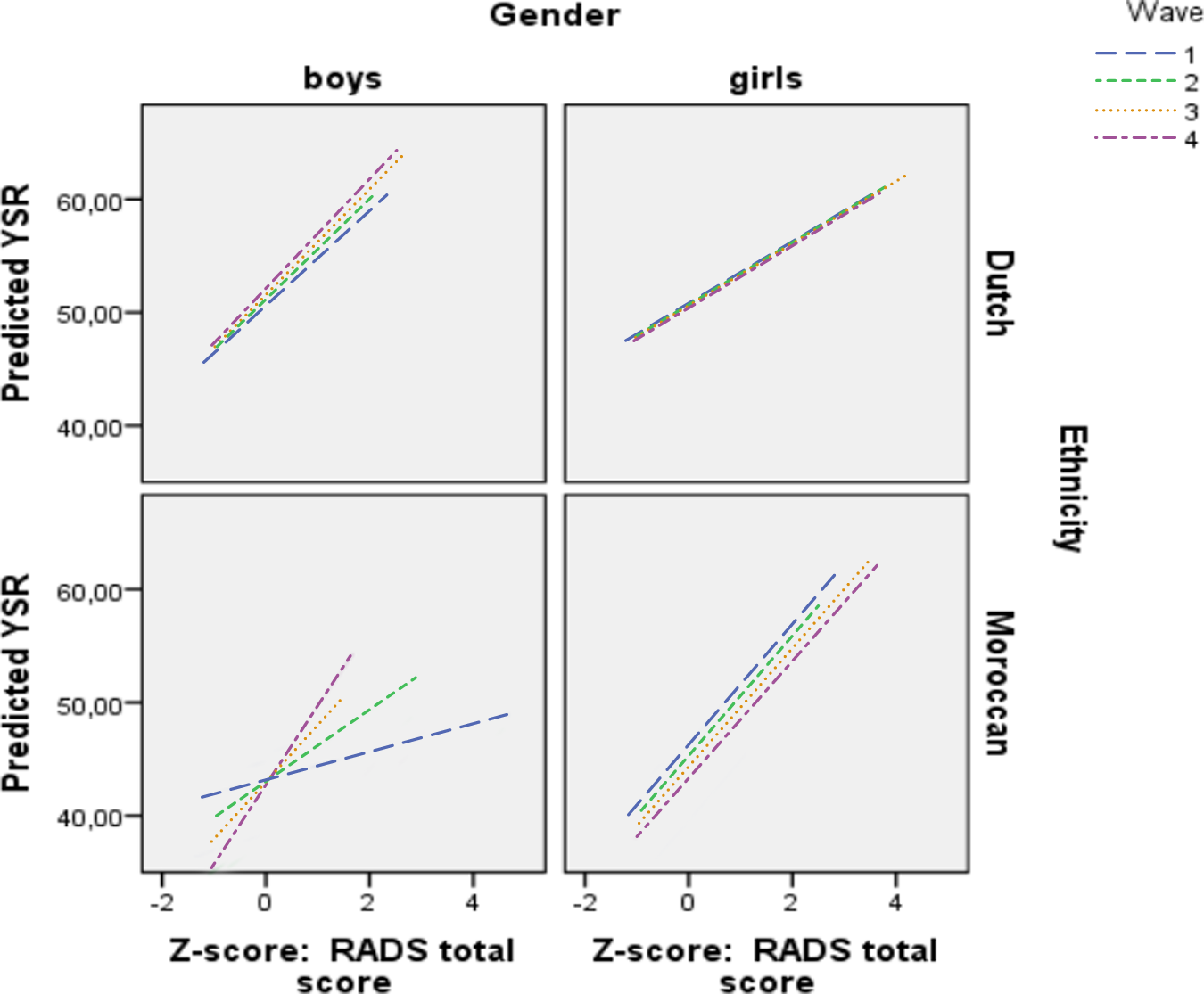
Linear GEE regression model for time interactions in the associations between depression and externalizing problems in Dutch and Moroccan boys and girls.
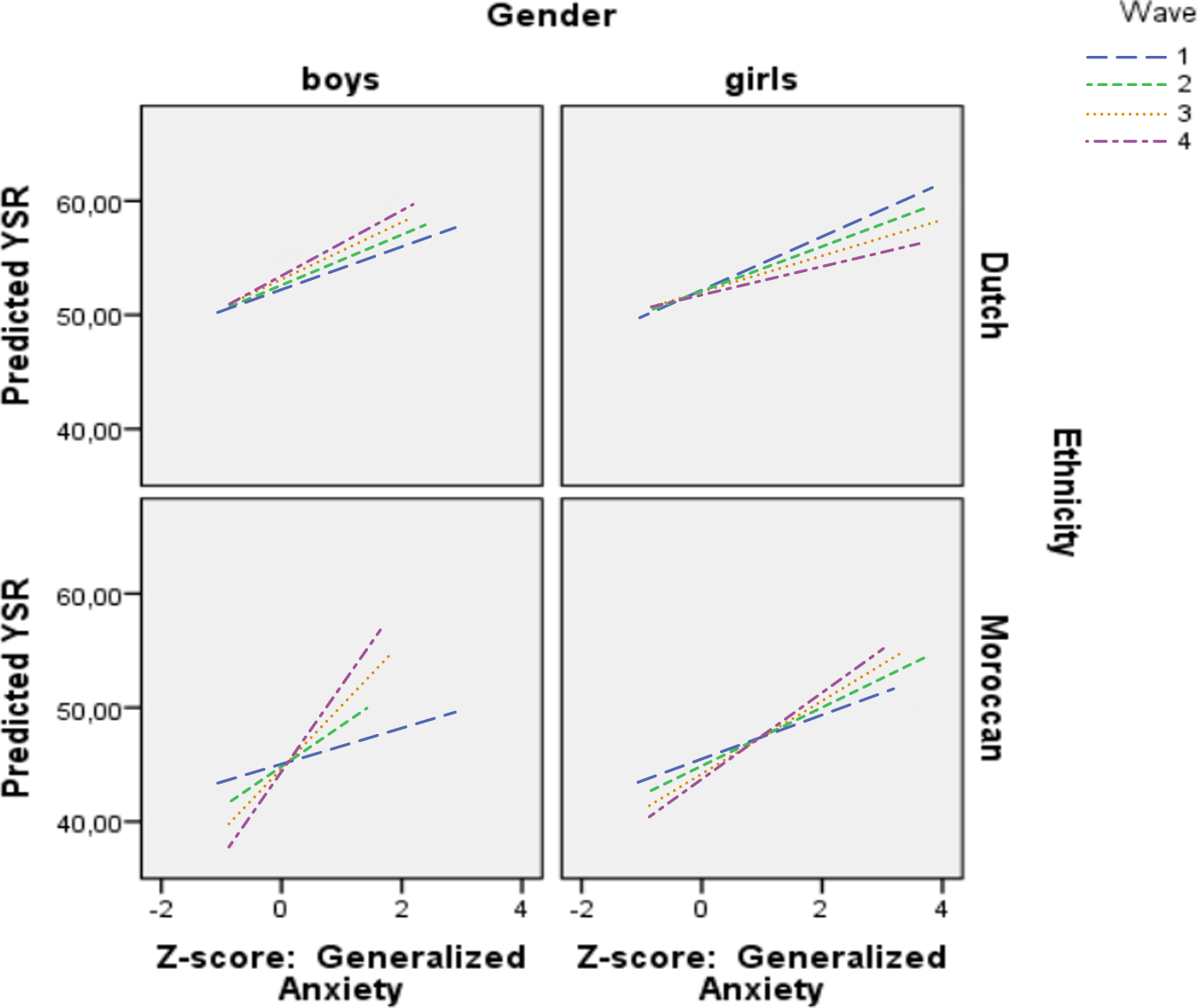
Linear GEE regression model for time interactions in the associations between generalized anxiety and externalizing problems in Dutch and Moroccan boys and girls.
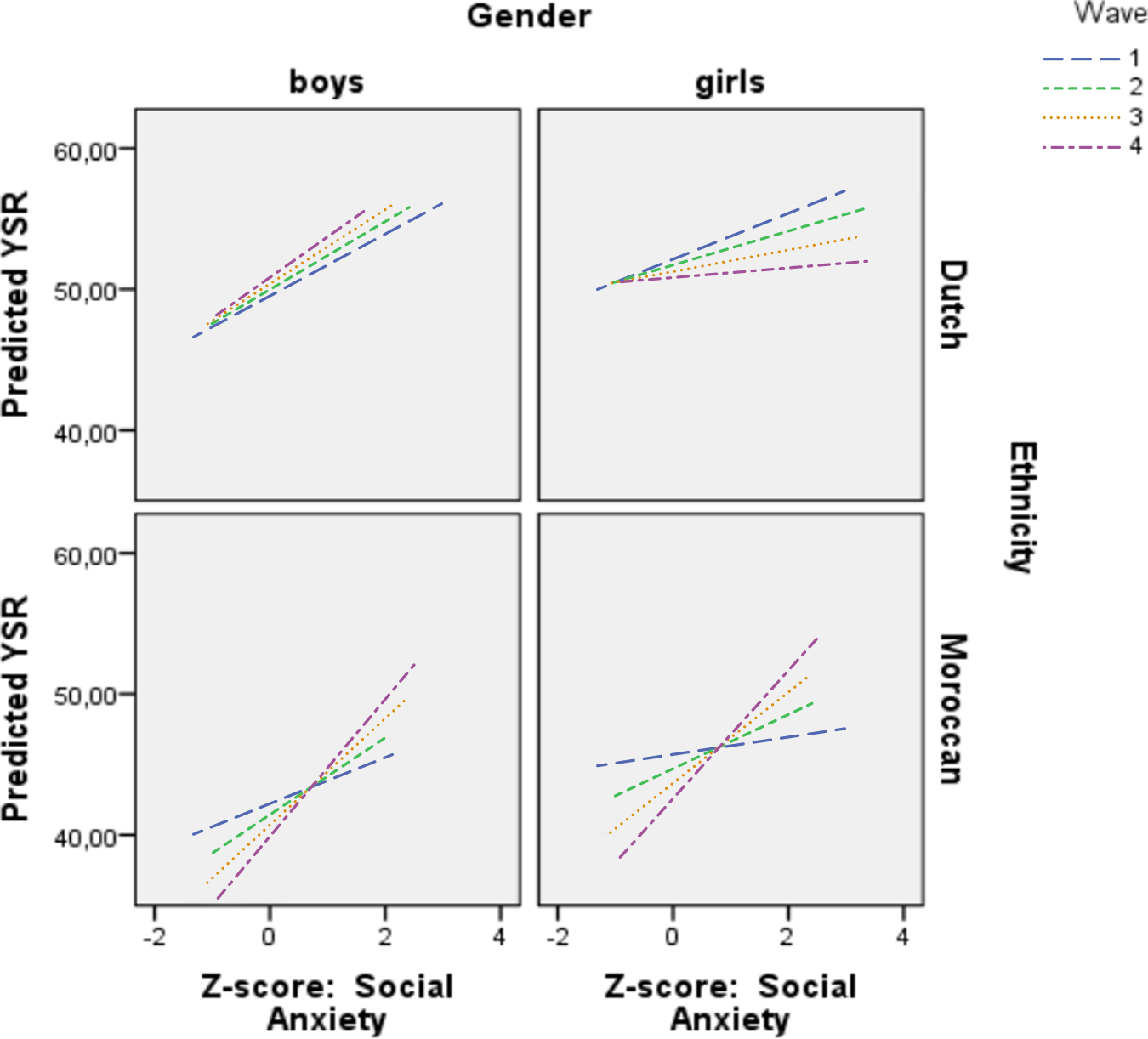
Linear GEE regression model for time interactions in the associations between social anxiety and externalizing problems in Dutch and Moroccan boys and girls.
Ethnic differences in the course of co-occurring generalized anxiety and externalizing problems course were found for both boys (p = .050) and girls (p = .016). Post-hoc analyses revealed that there was no time-interaction in Dutch boys (p = .458) and girls (p = .103), indicating a stable pattern of these co-occurring problems. However, the association in Moroccan boys was found to increase over time (p = .001). No time-interaction was found in Moroccan girls (p = .091). These results are visually presented in Figure 3.
No ethnic difference in course of co-occurring social anxiety and externalizing problems was found in boys (p = .372). In girls, ethnic differences concerning the course of co-occurring social anxiety and externalizing problems were found to be significant (p = .001). In both groups, associations varied over time. However, whereas associations between social anxiety and externalizing problems decreased in Dutch girls (B = −.64, CI −1.2–.09, p = .022), these associations in Moroccan girls increased (B = 1.2, CI 32 –2.1, p = .007). A visual presentation of these results in shown in Figure 4.
To investigate why mean levels did not increase, while associations became stronger among Moroccan adolescents, we performed post-hoc analyses in which we plotted the slopes of the internalizing and externalizing problems. Results revealed that the Moroccan group consisted of adolescents for whom internalizing problems more often lead to externalizing problems and/or vice versa during the course of adolescence, as well as adolescents with desisting internalizing or externalizing problems, explaining the stronger associations while mean levels did not increase.
Discussion
The aim of this study was to compare the strength and stability of associations between internalizing and externalizing problems among Moroccan and Dutch adolescents over a 4-year period. Adolescents taking part in this study predominantly originated from low-SES neighbourhoods and boys and girls at risk of developing externalizing problems were over-sampled. Lower levels of externalizing problems were reported by Moroccan adolescents as compared to Dutch adolescents. In contrast to what we expected, the average longitudinal co-occurrence between internalizing and externalizing problems did not differ between Dutch and Moroccan adolescents. However, ethnic differences were found in the course of the associations between internalizing and externalizing problems over time. Whereas associations were stable over time among Dutch adolescents, in Moroccan adolescents, associations between internalizing and externalizing problems increased as expected. These results may indicate an increasing complexity of problems in Moroccans during adolescence. The results of this explorative study indicate that the course of co-occurring problems may vary among different subgroups of adolescents.
The lower mean levels of self-reported externalizing behaviour in Moroccan adolescents as compared to Dutch adolescents are consistent with previous studies among Moroccan adolescents in the Netherlands (G. W. Stevens et al., 2003; Veen, Stevens, Doreleijers, Van der Ende, & Vollebergh, 2010; Zwirs, Burger, Buitelaar, & Schulpen, 2006). Several mechanisms have been put forward to explain these lower scores; they may be a result of social desirable answering, a different perspective of behaviour or may represent true lower levels of externalizing behaviour (G. W. Stevens et al., 2003; Veen et al., 2010). In our sample, the oversampling of at-risk adolescents was based on teacher reports. Results from several studies suggest that teachers attribute externalizing behaviour more easily to immigrant youths as compared to their native counterparts (e.g., Javo, Ronning, Handegard, & Rudmin, 2009; Lau et al., 2004; Sonugabarke, Minocha, Taylor, & Sandberg,1993; Youngstrom, Loeber, & Stouthamer-Loeber, 2000). If in our sample, teachers attributed unjust problems to Moroccan adolescents but not to Dutch adolescents, it is not surprising that Moroccan adolescents reported lower problems than Dutch adolescents on self-reports. Although studying levels of reported problems is an important topic for research, the focus of our study was on exploring associations between internalizing and externalizing problems. Interestingly, these lower levels of reported problems did not result in weaker associations between internalizing and externalizing problems.
Even though our study has an explorative character, the results are in line with some previous findings and theories and as such may provide possible directions of underlying mechanisms. We found that associations between internalizing and externalizing problems increased over time among Moroccan adolescents. Since mean problem scores did not increase in our study, this would imply that problems did not increase in severity but that more Moroccan boys and girls reported both types of problems to a relatively similar extend over the course of adolescence, which is reflected in increasing associations. Post-hoc analyses revealed that the Moroccan group consisted of adolescents who initially have co-occurring problems that decrease over time, as well as adolescents who persist in having problems. Due to a lack of treatment, problems may escalate (Capaldi & Stoolmiller, 1999; Chen & Simons-Morton, 2009). According theoretical frameworks, depressed or anxious adolescents may act out their internalizing problems in externalizing behaviour (acting-out model: Capaldi, 1992; Ritakallio et al., 2008), or due to continuous negative feed-back on their externalizing behaviour, adolescents with externalizing problems are also vulnerable for internalizing problems (failure model: Capaldi, 1992; Beyers & Loeber, 2003; Masten et al., 2005; Overbeek et al., 2006; Ritakallio et al., 2008; Vieno, Kiesner, Pastore, & Santinello, 2008). Regardless of the causal relation, the lower treatment rates of immigrants (Angold et al., 2002; Guevara, Mandell, Rostain, Zhao, & Hadley, 2006; Zwirs, Burger, Schulpen, & Buitelaar, 2006; Zwirs, Burger, Buitelaar et al., 2006), may possibly contribute to deteriorating problems and increasing associations between internalizing and externalizing problems in some Moroccan adolescents.
Furthermore, the shift in influence of the family to that of the environment outside the family (Arnett, 2000), may also result in a shift in impact of certain risk factors on the development of problems. Suggesting that risk factors related to the outside environment, such as living in a disadvantaged neighbourhood, or affiliation with delinquent peers, may grow in impact on the development of co-occurring problems during adolescence when the outside environment becomes increasingly important (Brown, 2004; Gardner and Steinberg, 2005). In the Netherlands, Moroccans belong to the most disadvantaged ethnic minority group and previous studies have found Moroccan adolescents to be over-represented in crime (Blom, Oudhof, Bijl, & Bakker, 2005; Junger-Tas, 2004; Gijsberts & Dagevos, 2009; Hoelling & Schlack, 2008; Veen, 2011; Wille, Bettge, & Ravens-Sieberer, 2008). It is possible that some factors that are more often found in Moroccan adolescents, affect the increasing level of co-occurring problems especially during adolescence. Furthermore, being part of an ethnic minority may complicate the typical identity issues associated with adolescence even more for migrant adolescents as compared to their native counterparts. During adolescence awareness of one’s ethnic identity is likely to occur when individuals grow to recognize that the surrounding society’s beliefs, values, and norms differ from their own (Matsunaga, Hecht, Elek, & Ndiaye, 2010). Throughout Europe, being part of Muslim culture is perceived as inferior to ‘Euro-American’ culture (Khanlou, Koh, & Mill, 2008). Such experiences of discrimination and social exclusion are likely to undermine an adolescent’s sense of worth (Fischer & Shaw, 1999; Romero & Roberts, 2003; Szalacha, Erkut, Coll Alarcón, Fields, & Ceder, 2003) and may contribute to increasing co-occurring problems. Such mechanisms would fit the theory that externalizing and internalizing problems are caused by shared risk factors. As a result, individuals faced with these risk factors may develop both problems simultaneously (e.g. Chen & Simons-Morton, 2009; Oland & Shaw, 2005).
However, no studies have yet longitudinally investigated time-varying risk factors such as (the development of) ethnic identity on co-occurring problems. Further research is needed to investigate the impact of risk factors in different developmental stages, and in different subgroups.
Irrespective of such possible explanatory mechanisms, the finding of an increase of co-occurring problems in Moroccan adolescents signals clinical relevance as co-occurring problems are related to poorer treatment outcomes and poorer overall functioning (Capaldi, 1992; Capaldi & Stoolmiller, 1999; McCarty et al., 2006; Newman et al., 1998; Ollendick et al., 2008). The more since findings from previous research indicated that, similar to other immigrant groups, Moroccan immigrants in the Netherlands face higher treatment thresholds and lower treatment rates of mental health disorders (Zwirs, Burger, Schulpen et al., 2006; Zwirs, Burger, Buitelaar et al., 2006). Our results indicate that a developmental perspective is necessary to identify Moroccan adolescents at risk of developing co-occurring problems: Differentiation between those with desisting problems and those developing co-occurring problems becomes clear during the course of adolescence. Future research should investigate underlying mechanisms and the impact of risk factors for co-occurring problems in different groups of adolescents across time. This information is needed for aiming intervention efforts at the appropriate risk factors among the appropriate risk groups.
Strengths and limitations
Several limitations to this study should be acknowledged. First, we did not investigate causal relations between internalizing and externalizing problems over time. Further research with larger groups is needed to investigate the mechanisms behind the associations between internalizing and externalizing problems in different subgroups. Second, replication of results in diverse ethnic-minority groups is needed to investigate generalizability of our results. Third, we solely relied on self-reports in our study. Using additional informants such as teachers and parents might have provided additional information. Although we used international validated instruments, the instruments used have not been validated for Moroccan immigrant samples. However, Stevens, Vollebergh, Pels, and Crijnen (2007), found a fair fit of the externalizing scale of the YSR in Moroccan youth in the Netherlands. Fourth, the focus of our study did not concern clinical problems, but the associations of the continuous measures of internalizing and externalizing problems. Therefore we can not draw conclusions regarding severity of problems. However, co-occurring internalizing and externalizing problems are a strong signal for future problems, irrespective of the mean scores of the separate problems.
Despite these limitations, findings indicate that co-occurring internalizing and externalizing problems during adolescence may be different for different ethnic groups. High risk groups, such as immigrant youths need our attention in order to prevent escalation of problems
Repeated screening may increase the chance to identify those immigrant adolescents at risk of developing co-occurring problems. Research on what factors result in differences between those with desisting problems and those with increasing co-occurring problems will provide valuable information for intervening.
Footnotes
Funding
Data from the RADAR study were used in this study. RADAR has been financially supported by main grants from the Netherlands Organization for Scientific Research (GB-MAGW 480-03-005, GB-MAGW 480-08-006), Stichting Achmea Slachtoffer en Samenleving (SASS), and various other grants from the Netherlands Organization for Scientific Research, VU University Amsterdam and Utrecht University.