
Abstract
The deleterious effects of maternal depression on child emotional and behavioral development are well documented, yet many children exposed to maternal depression experience positive outcomes. The aim of this study was to identify psychosocial factors associated with the emotional–behavioral resilience of four-year-old children of first-time mothers experiencing depressive symptoms across the early childhood period. Data were from 1085 mother–child dyads in the Maternal Health Study collected prospectively at five time-points from pregnancy to child age four. Longitudinal trajectories of maternal depressive symptoms were identified, and children were regarded as resilient or competent if they scored in the normal range on the Total Difficulties subscale of the Strengths and Difficulties Questionnaire. We found that 22% of women had a pattern of moderate to high depressive symptoms, and within this group 78% of their children were identified as resilient. Maternal tertiary education and maternal involvement in home learning activities were unique predictors of children’s resilience. Higher maternal age at the time of pregnancy and financial security were factors associated with positive outcomes for all children. The findings highlight the importance of policy and intervention efforts to strengthen the quality of maternal–child interactions and the home learning environment to promote the emotional and behavioral functioning of children whose mothers are experiencing mental health difficulties in the early years of parenting.
Introduction
The impact of maternal mental health on children’s development is a global health concern (Paschetta et al., 2014). Depression affects approximately 25% of women during pregnancy (Priest et al., 2008) and 10–15% in the first postnatal year (Gavin et al., 2005). Depressive symptoms often persist beyond the first postnatal year for up to 40% of women (Giallo, Cooklin, & Nicholson, 2014; Giallo, Woolhouse, Gartland, Hiscock, & Brown, 2015; Woolhouse, Gartland, Mensah, & Brown, 2015), and are associated with a past history of mental health problems, stressful life events, relationship difficulties, and limited social support (Giallo et al., 2014; Woolhouse et al., 2015). Many studies have investigated the negative impacts of maternal depression on children. Two systematic reviews have reported increased risks of asthma, language problems, cognitive difficulties, and emotional–behavioral difficulties from infancy through to adolescence (Kingston & Tough, 2013; Kingston, Tough, & Whitfield, 2012). Most recently, data from 1085 mother–child dyads participating in the Maternal Health Study (MHS) (also used in the present study) found that 24% of children with mothers reporting persistently high depressive symptoms across the early childhood period had emotional–behavioral difficulties in the “at risk” or “clinical” ranges on the Strengths and Difficulties Questionnaire at four years (Giallo et al., 2015). Children of mothers reporting subclinical depressive symptoms were also at risk, with 19% having difficulties in the “at-risk” or “clinical” ranges. Children may be at risk of poor outcomes due to the potential impact of maternal depressive symptoms on parenting behavior, parenting self-efficacy, and maternal sensitivity (Lovejoy, Graczyk, O’Hare, & Neuman, 2000).
Few studies have sought to understand why many children who grow up within a context of adversity associated with maternal depression have similar emotional–behavioral functioning to unexposed children. The current study seeks to identify factors associated with positive or competent emotional–behavioral functioning for children exposed to maternal depression across the early childhood period using longitudinal data from the Maternal Health Study.
Resilience Theory and Research
Understanding why some children do well in the face of adversity is the key focus of resilience theory and research. “Resilient outcomes” are broadly defined as evidence of positive adaptation and functioning despite exposure to significant risk or adversity (Luthar, Cicchetti, & Becker, 2000), while “competent outcomes” refer to similar positive outcomes but in the absence of risk or adversity. Resilient outcomes may be evident in one or multiple domains of development such as cognitive, emotional, behavioral, social, or academic functioning (Luthar et al., 2000).
Resilience research seeks to identify factors or processes that disrupt or buffer the effects of adversity, resulting in more favorable outcomes for children. Protective factors uniquely enable positive adaption for children in high-risk contexts, but have little influence in low-risk contexts (Luthar et al., 2000). Resource factors, on the other hand, promote positive outcomes for children in both high- and low-risk contexts. Protective and resource factors can be characteristics of an individual or aspects of their environment, and may vary considerably across the lifespan. Given that children are embedded in their caregivers’ everyday contexts, an ecological or systemic theoretical approach to identifying protective and resource factors for children is needed. Drawing upon Bronfenbrenner’s (1986) ecological theory of development, protective and resource factors can operate and interact at various levels including the child (i.e., temperament, coping behaviors), the family (i.e., parental warmth, family communication), the community (i.e., social support), and the broader socio-political environment (i.e., policy initiatives promoting child and family health).
Factors Associated with Resilience in Children of Mothers with Depressive Symptoms
Studies identifying factors associated with resilient outcomes for children exposed to maternal depression are scarce. To the best of our knowledge, only one study has examined emotional–behavioral resilience in 1009 children of mothers reporting depressive symptoms in the first year postpartum (Savage-McGlynn et al., 2015). The study showed that 32% of children were emotionally and behaviorally resilient on the Strengths and Difficulties Questionnaire at age 11 years, and that maternal positive feelings about parenting at 18 months postpartum and children’s good non-verbal communication at 15 months were associated with resilient outcomes. Whilst important, this study did not include children not exposed to maternal depression in the analyses; therefore, it was not possible to distinguish between protective and resource factors as per resilience theory.
Previous studies have focused on exposure to maternal depression during childhood, adolescence, and early adulthood. For instance, in a study of school-aged children of mothers with and without unipolar depression, bipolar disorder, and medical illness, positive self-concept, academic success, social competence, and positive perceptions of their mother were identified as resource factors associated with positive outcomes (defined as not having a diagnosis of a mental health disorder) for all children (Conrad & Hammen, 1993). Maternal social competence and having a father without mental health problems were protective factors specifically for children of mothers with unipolar depression. In an Australian cross-sectional study of 816 adolescents, maternal warmth and low maternal over-involvement and parental control were associated with resilient outcomes (defined as no past or current psychiatric diagnoses, internalizing, or social difficulties) for adolescents of depressed mothers (Brennan, Le Brocque, & Hammen, 2003). More recently, Lewandowski and colleagues (2014) identified predictors of positive mental health outcomes in 235 children (aged 5–25 years at baseline) of depressed and non-depressed parents across a 20-year period. Resilient outcomes for children of depressed parents and competent outcomes for offspring of non-depressed parents were defined as absence of psychiatric disorder and good emotional–behavioral functioning at two, 10, and 20 years after baseline. The study identified both protective factors (i.e., present for at-risk children only: higher IQ and lower maternal overprotection) and resource factors (i.e., present for non-risk or both groups: easier temperament, higher self-esteem, maternal affection, family cohesion).
Whilst these studies contribute to the evidence about potential factors associated with positive outcomes for children of mothers experiencing mental health difficulties, they are limited on several counts. First, with the exception Savage-McGlynn et al. (2015), the focus has been on exposure for school age children and adolescents, with limited attention to the antenatal and early childhood periods. Early life adversity can impact fetal and infant neuro-development, increasing the risk of poor outcomes across the lifespan (Shonkoff, 2010). Therefore, identifying the protective factors in the early years on children’s emotional–behavioral functioning is critical. Second, all studies examined exposure to maternal depression at a single time point, with no assessment of the chronicity of depressive symptoms. This is important given recent research showing that children of mothers experiencing subclinical or high depressive symptoms across pregnancy and early childhood were twice as likely to have emotional–behavioral difficulties than children of mothers reporting minimal symptoms (Giallo et al., 2015). Finally, with few exceptions (Brennan et al., 2003), the sample sizes were small, limiting the generalizability and utility of findings to inform policy and practice.
Aims of the Current Study
The current study addresses these limitations and builds on previous work drawing upon data from a large Australian prospective pregnancy cohort of over 1000 first-time mothers and their children. The aim of the study was to identify the perinatal and concurrent psychosocial protective factors associated with emotional–behavioral resilience (as demonstrated by functioning in the normative range on a well-established measure of children’s mental health) among four-year-old children of mothers who reported depressive symptoms across the perinatal and early childhood period. We also sought to identify psychosocial factors associated with positive emotional–behavioral outcomes for children not exposed to maternal depressive symptoms over time. Given the importance of the early caregiving environment to children’s development, we were particularly interested in maternal self-care behavior, partner relationship quality, and emotional satisfaction (Krishnakumar & Buehler, 2000), partner contribution to caregiving (Sarkadi, Kristiansson, Oberklaid, & Bremberg, 2008), and maternal involvement in home activities that foster children’s learning and development (Wake et al., 2008). We hypothesized that these would be associated with resilient outcomes for children exposed to maternal depression.
Method
Study Design
Data were drawn from the Maternal Health Study, a prospective longitudinal study of women’s health during pregnancy and after childbirth. Ethics approvals were obtained from participating hospitals, La Trobe University, and the Royal Children’s Hospital. Study design, sampling, and field methods are published in the study protocol (Brown, Lumley, McDonald, & Krastev, 2006). Briefly, women registered to give birth at six metropolitan public hospitals in Melbourne, Australia, between April 2003 and December 2005 were invited to participate. Eligibility criteria were: (a) 18 years or older; (b) nulliparity; (c) gestation of up to 24 weeks at time of enrolment; and (d) proficiency in English to complete written questionnaires.
Approximately 6000 invitation packages were distributed to women attending the six study hospitals for maternity care, shortly after their booking visit between 10 and 20 weeks’ gestation. Invitation packages were distributed to women during clinic visits, at antenatal education classes, and mailed to women at their home address. Mailed invitations and invitation packs given to women at clinic visits were followed up by a single reminder postcard. It is not possible to determine precisely how many: (a) women received more than one invitation via different pathways; (b) ineligible women received an invitation; and (c) invitations were incorrectly addressed. Assuming that 80–90% of invitations reached eligible women, we conservatively estimate that the final response rate was 28–31%.
Women were followed up during pregnancy and after childbirth with mailed self-administered questionnaires. This paper draws on data collected in early pregnancy (10–24 weeks’ gestation), and at three, six, 12, and 18 months postpartum, and four years postpartum.
Participants
There were 1507 women who met the eligibility criteria and returned a baseline questionnaire. Over the course of the study, 126 participants dropped out or were lost to follow-up. Reasons include: participant declined further participation (n = 58); participant unable to be contacted (n = 29); participant too busy (n = 21); undisclosed reason (n = 7); stillbirth (n = 6); infant death (n = 2); infant ill health (n = 2); and maternal ill health (n = 1). The number of surveys returned following the three-, six-, 12-, and 18-months and the four-year follow-ups were 1431, 1400, 1357, 1327, and 1102, respectively. Selective attrition was observed between six months and four years, whereby women completing the four-year follow-up were more likely to be older, Australian-born, tertiary educated, and less likely to have reported depressive symptoms in the first year following birth than women at baseline.
It is important to note that 17 women completed the four-year follow-up survey but did not provide information on the Strengths and Difficulties Questionnaire (SDQ). Three of these women had stillbirths and two experienced a child death during the course of the study, but chose to remain in the study. Cases with missing data on the SDQ were excluded as we were unable to correctly classify children’s emotional–behavioral resilience status (see more information about missing data in the Results section).
The final analysis sample for the present study was 1085 mothers. Their demographic characteristics at enrolment were compared with routinely collected Victorian data for nulliparous women giving birth as public patients in Victoria during the recruitment period (see Table 1). The majority of women were aged between 30 and 34 years at the time of enrolment (range 18–46 years), born in Australia, and in a relationship.
Characteristics of Study Participants at Enrolment and Nulliparous Women Giving Birth in Victoria as Public Patients During the Study Recruitment Period.
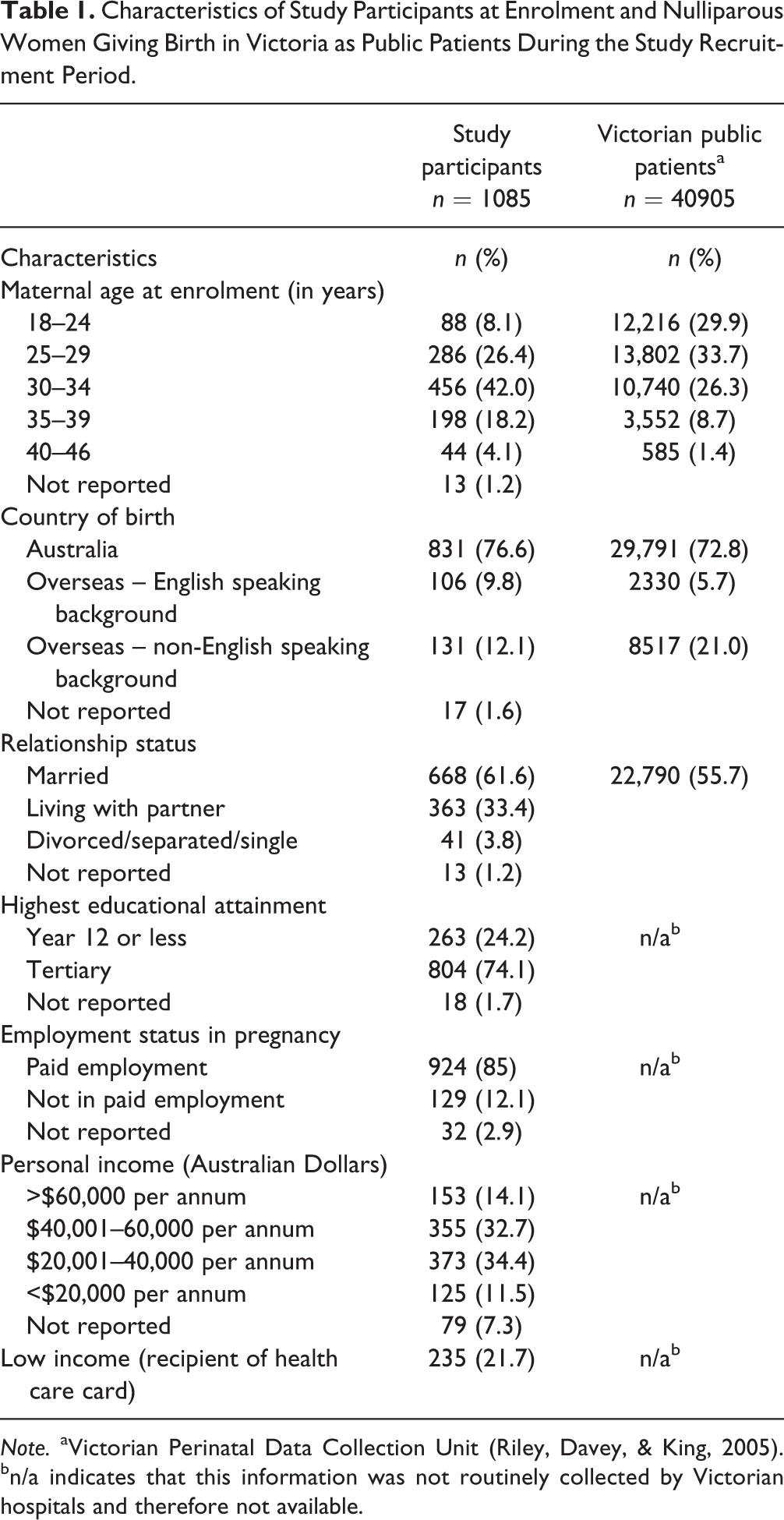
Note. aVictorian Perinatal Data Collection Unit (Riley, Davey, & King, 2005). bn/a indicates that this information was not routinely collected by Victorian hospitals and therefore not available.
Measures
Children’s emotional–behavioral functioning at four years of age was assessed using the parent-report on the SDQ (Goodman, 2001). The SDQ comprises 25 items rated on a three-point scale (0 = not true to 2 = certainly true) assessing symptoms such as sadness, worries, attention difficulties, fighting, and problems with peers. The four problem subscales (emotional symptoms, conduct problems, hyperactivity/inattention, peer problems) are summed to give a total difficulties score, with higher scores indicating more difficulties. Pre-defined cut-off scores based on Australian norms were used to identify children in the normal (0–13), at risk (14–16), and clinical (17–40) ranges (see www.sdqinfo.com). The SDQ has had extensive psychometric evaluation with Australian samples, with moderate to strong internal consistency and test–retest reliability reported (Hawes & Dadds, 2004). Cronbach’s alpha for the total difficulties scale for the current sample was .79.
Maternal depressive symptoms were assessed using the 10-item self-report Edinburgh Postnatal Depression Scale (EPDS) at each time point. Designed to identify women at risk for depression in the postnatal period (Cox, Holden, & Sagovsky, 1987), the EPDS was later validated for use in pregnancy (Murray & Cox, 1990) and outside the perinatal period (Cox, Chapman, Murray, & Jones, 1996). Women indicated the extent to which they had experienced a range of symptoms such as depressed mood, crying, difficulty sleeping, feeling anxious, and thoughts of self-harm in the previous week on a four-point scale. A cut-off score of ≥13 is recommended when screening for probable major depression in community samples (Murray & Cox, 1990). Cronbach’s alphas for the current sample at each time point ranged from .87 during pregnancy to .90 at four years postpartum.
Potential Resource or Protective Factors
Demographic variables were child gender, maternal age at enrolment (in years), maternal education (categorized into high school education year 12 or less/tertiary or university education), and being a recipient of an Australian Government Health Care Concession Card (yes/no) as a marker of low income and eligibility for cheaper medicines and other concessions. At six months and four years postpartum, a range of maternal factors were examined. Having time to oneself when someone else looked after their child (1 = at least once/week, 2 = less than once/week) and maternal changes in relationship status (0 = no relationship transitions, 1 = at least one relationship transition) were assessed. Perceived emotional satisfaction in their couple relationship was assessed at six months and four years postpartum using a single item (0 = high emotional satisfaction, 1 = high emotional dissatisfaction). Perceptions of partners’ involvement in parenting were also assessed at six months and four years postpartum using a single item (0 = limited involvement, 1 = high involvement). Some women who indicated that they were not currently in a relationship (i.e., single, divorced, or widowed) completed these items referring to their child’s father. For those women not in a relationship who did not complete these items, we created a category “Did not have a partner.”
Maternal involvement in home activities was assessed at four years using a five-item scale from the Growing up in Australia: Longitudinal study of Australian children (National Center for Education Statistics, 2002). Mothers were asked to indicate how many days in the past week (1 = none, 2 = 1–2 days, 3 = 3–5 days, 4 = 6–7 days) they had engaged in a range of activities with their children, including read from a book, told a story, played music, sang or danced, played toys or indoor games, or involved them in everyday activities. Items were summed, with higher scores indicating greater involvement. Cronbach’s alpha for this scale was .71. Presence of more than one child and the number of adults living in the household at four years postpartum were also included.
Data Analysis
Analyses were conducted in three stages: (1) describe and classify maternal depressive symptoms across the early parenting period; (2) establish a derived variable of child emotional–behavioral resilience status; and (3) address the study aims to identify perinatal and concurrent psychosocial factors associated with positive emotional–behavioral functioning for children whose mothers report high depressive symptoms across the early childhood period and those who do not.
First, latent growth class modeling was conducted to describe the course of maternal depressive symptoms across six time-points across the early parenting period. A two-factor latent growth model was estimated prior to identifying latent classes in MPlus Version 7.11 (Muthen & Muthen, 1998–2013). Latent factors to represent the initial levels of the variable (intercept) and the change in that variable over time (slope) were estimated using robust maximum likelihood estimation. The model was assessed using the chi-square test (χ2), Tucker–Lewis index (TLI), the comparative fit index (CFI), and root mean square error of approximation (RMSEA). Indices for the TLI and CFI should exceed 0.90 for an acceptable fit (Bentler, 1990), and values close to or below 0.05 for the RMSEA were considered acceptable (Hu & Bentler, 1999).
Having established sufficient variability in the intercept and slope factors, latent class growth mixture modeling was conducted to identify distinct subgroups of women based on their trajectory of depressive symptoms. This involves identifying the smallest number of classes, starting with a parsimonious 1-class model and fitting successive models with increasing numbers of classes. Model solutions were evaluated based on several criteria including: (a) model fit indices; (b) relative entropy; (c) the Vuong–Lo–Mendell–Rubin likelihood ratio test; and (d) final class counts and proportions for the latent classes for each solution. Better fitting models have a lower likelihood-ratio statistic (L 2), Bayesian information criterion (BIC), and Akaike information criterion (AIC), whilst entropy is an index for assessing the precision of assigning latent class membership, where higher probability values indicate greater precisions of classification. The Vuong–Lo–Mendell–Rubin likelihood ratio test was also used to test for significant differences between the models. The resulting class counts and proportion in each latent class for each solution were also considered to ensure that latent class sizes were meaningful. Class membership for all cases in the accepted model was saved and used in the logistic regression analyses.
Second, a derived variable of children’s emotional–behavioral resilience status was constructed. Children’s emotional–behavioral functioning (normal range vs cut-off scores at the “at-risk” and “clinical” ranges on the SDQ) were cross-classified with exposure to the trajectories of maternal depressive symptoms in the previous phase. This resulted in four groups of children: (1) those exposed to low-risk environments (minimal depressive symptoms), with scores in the normal range (few emotional–behavioral difficulties); (2) those exposed to low-risk environments (minimal maternal depressive symptoms), with scores in the at-risk or clinical ranges (high emotional–behavioral difficulties); (3) those exposed to high-risk environments (moderate to high maternal depressive symptoms), with scores in the at-risk or clinical ranges (high emotional–behavioral difficulties); and (4) those exposed to high-risk environments (high to moderate maternal depressive symptoms), with scores in the normal range (few emotional–behavioral difficulties).
Finally, to identify protective and resource factors, two sets of univariable and multivariable logistic regression models were estimated to assess the relationship between a range of psychosocial factors associated with positive outcomes (few emotional–behavioral difficulties) for children with exposure to moderate to high maternal depressive symptoms (Model 1) and low maternal depressive symptoms (Model 2). Separate models were estimated to assess the similarities and differences in significant predictor variables in the different contexts. Variables significantly associated with positive outcomes (p < .05) in one or both contexts in the univariate models were entered in the multivariable models. Reported associations between the predictor and outcome variables are expressed as odds ratios with 95% confidence intervals. Odds ratios of less than 1.0 denote a reduced likelihood of positive psychological functioning relative to the reference category, and odds ratios of greater than 1.0 an increased likelihood of positive emotional–behavioral functioning relative to the reference category.
To address missing data on the EPDS, we used full information maximum likelihood in MPlus Version 7.11 for the latent class growth modeling. We used multiple imputation to handle incomplete data in remaining analyses, which were conducted in SPSS (Lee & Simpson, 2014; Sterne et al., 2009). Ten complete datasets under a multivariate normal model incorporating all analysis variables were imputed. Maternal age and maternal involvement in home activities were included in the imputation model as continuous variables, whilst all other variables were imputed as binary variables. We obtained pooled estimates for all proportions and model parameter estimates generated by SPSS, which averages results using Rubin’s rules.
Results
Descriptive Statistics and Missing Data
Of the 1507 women who completed a baseline survey, there were 422 women who had missing data at four years postpartum (due to the reasons described above). Consequently, missing data was approximately 28% across all study variables at four years postpartum. Little’s MCAR test with continuous variables was significant, χ 2(8) = 17.69, p = .024, suggesting that missing data were not missing completely at random. Women who were lost to follow-up, those who did not have a four-year-old child due to stillbirth or child death, or those who had no data on the key analysis variables were excluded from the analyses.
Missing data on some of the key analysis variables for the remaining 1085 cases was minimal ( < 8%), and missing completely at random, as evidenced by Little’s MCAR χ 2(8) = 1.78, p = .411, and these were handled using multiple imputation described above. Descriptive statistics for the study variables are presented in Table 2.
Descriptive statistics for Study Variables (n = 1085).
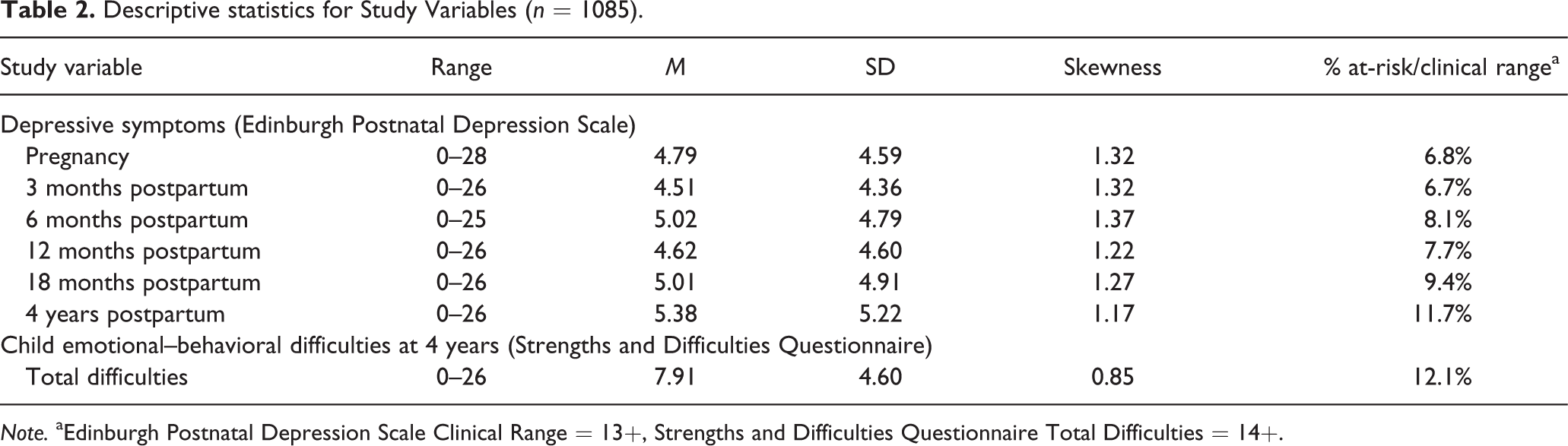
Note. aEdinburgh Postnatal Depression Scale Clinical Range = 13+, Strengths and Difficulties Questionnaire Total Difficulties = 14+.
Trajectories of Maternal Depressive Symptoms
The two-factor latent growth model of maternal depressive symptoms was a good fit to the data, χ2 (16) = 133.32, p < .001, CFI = .95, TLI = .95, RMSEA = .08 (90% CI, .07–.10). The mean for the intercept was positive and significantly different from zero (Intercept = 4.68, p < .001), indicating that the average depressive score at baseline during pregnancy was 4.68. Although the estimate of the slope was significantly different from zero, it was very small (Slope = 0.01, p < .001), indicating that depressive symptom scores increased at a rate of .01 points each wave. The variance components indicated significant individual differences in the initial levels of depressive symptoms during pregnancy (11.07, p < .001) and in change over time (0.002, p = .0.15), providing support for conducting latent class growth mixture modeling. Finally, the correlation between the intercept and the slope factor was not significant (r = –.05, p = .630).
Next, to identify distinct trajectories of maternal depressive symptoms over time, latent class growth mixture models specifying 1–4 trajectories were estimated (see Table 3). Although the three-class model had the lowest L 2, BIC, AIC values, and the Vuong–Lo–Mendell–Rubin Likelihood Ratio Test indicating a significant difference between the two- and three-class model, we chose the two-class model solution as the final counts and proportions for one of the classes was low (n = 87; 8%). We considered whether a class of this size would be meaningful to conduct the subsequent analyses with. A three-class solution would have yielded two classes representing women with low depressive symptoms (EPDS scores less than 13) and one class representing women with high depressive symptoms (EPDS scores greater than 13). We chose to accept the parsimonious two-class model (representing a similar pattern of women with high and low depressive symptoms) with the highest relative entropy value (.91) and high average posterior probabilities (class 1: .98; class 2: .94), indicating acceptable precision in assigning individual cases to their appropriate class.
Model Fit Indexes for Latent Growth Class Models of Depressive Symptoms from Pregnancy to Four Years Postpartum (n = 1085).

Note. L 2: Likelihood-ratio statistic; BIC: Bayesian information criterion; AIC: Akaike information criterion
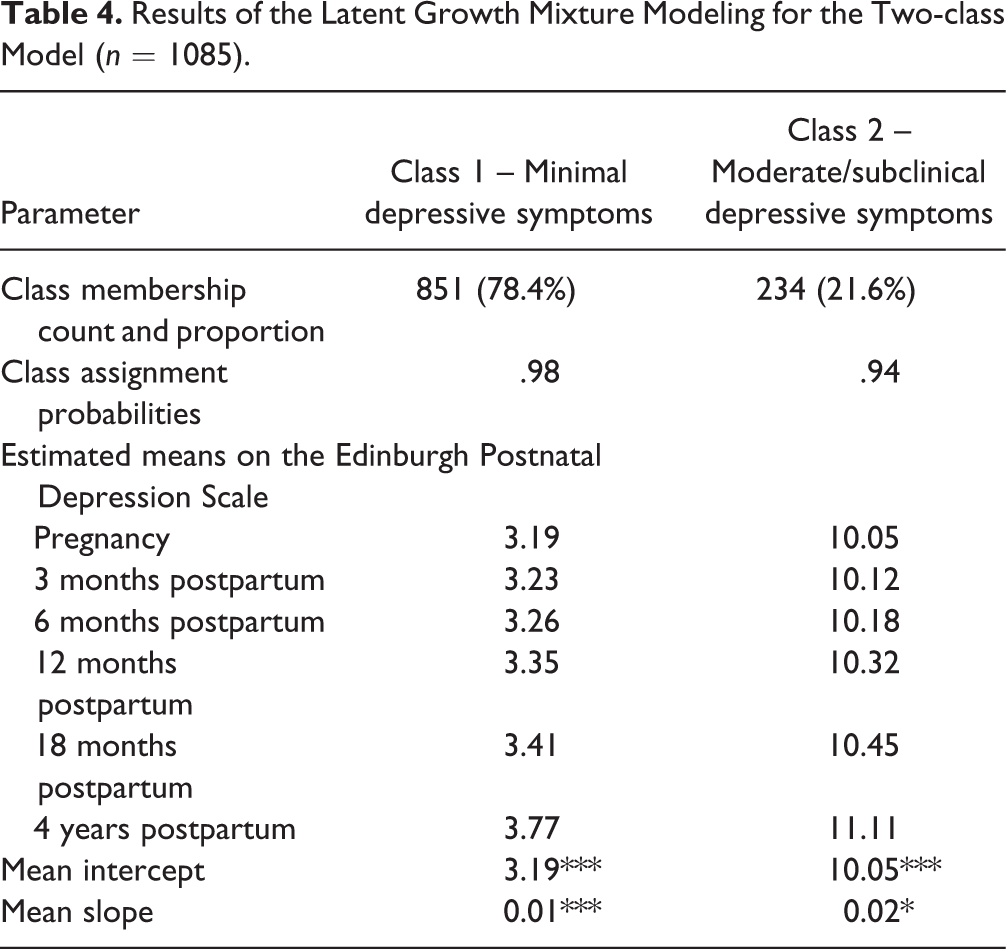
Table 4 summarizes the two-class model and Figure 1 illustrates the two trajectory classes of maternal depressive symptoms. The larger class consisted of women who reported low EPDS scores from pregnancy to four years postpartum (n = 851, 78.4%), and therefore were referred to as the “minimal depressive symptoms” class. The average EPDS score at baseline for this class was 3.19 (intercept) and in the normal range. The very small increase of .01 points each wave (slope) indicates stability of low depressive symptoms over time for this class.
Results of the Latent Growth Mixture Modeling for the Two-class Model (n = 1085).
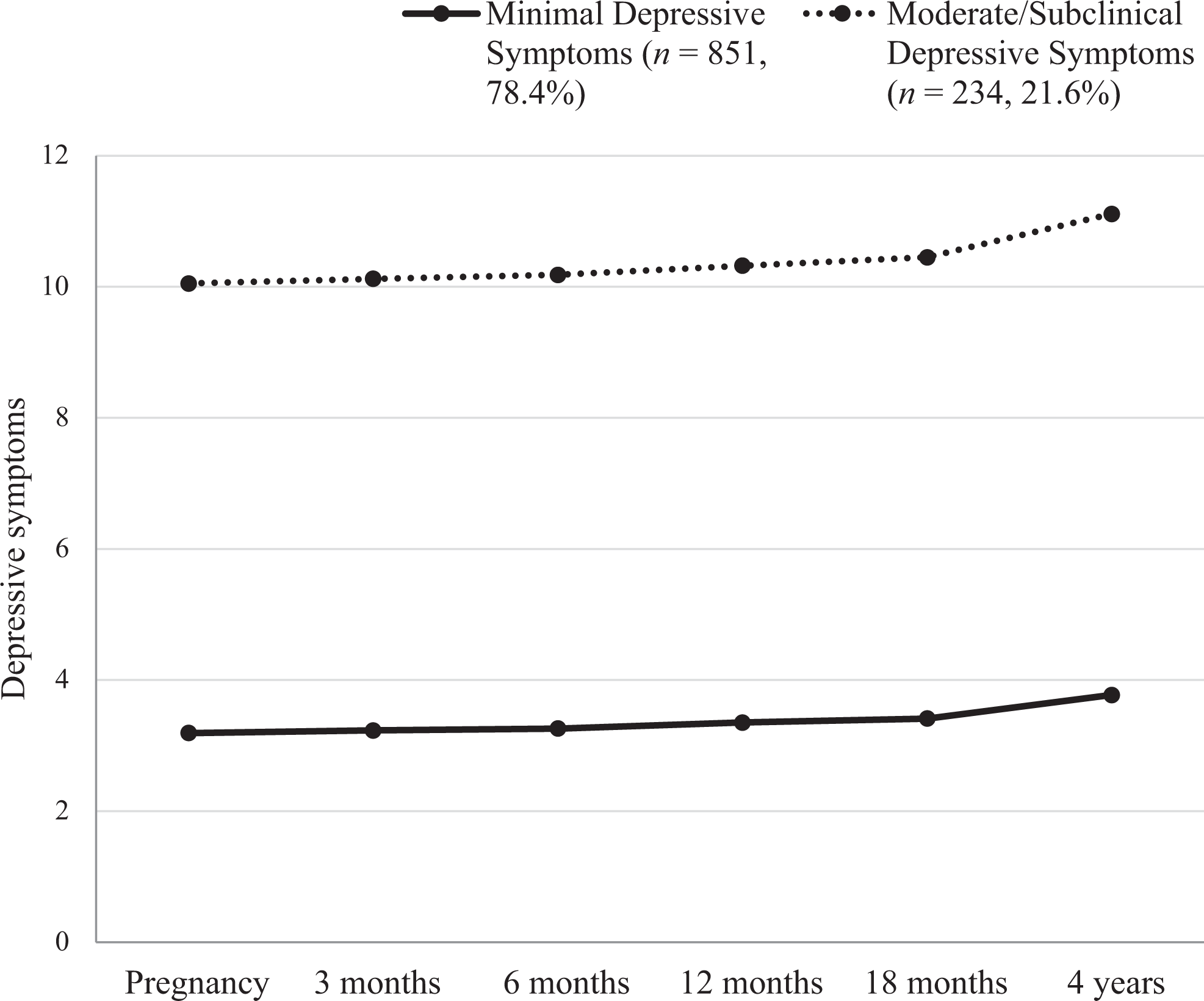
Estimated means on the Edinburgh Postnatal Depression Scale for the trajectories of maternal depressive symptoms from pregnancy to four years postpartum (n = 1085).
The smaller class consisted of women who reported scores approaching the clinical cut point of 13 on the EPDS over time, and therefore were referred to as the “moderate/subclinical depressive symptoms” class (n = 234, 21.6%). The average EPDS score at baseline for this class was 10.05 (intercept). The small increase of .02 points each wave (slope) indicates stability of moderate/subclinical depressive symptoms over time for this class.
Children’s Emotional–Behavioral Resilience Status
Classification of emotional–behavioral resilience status revealed that: 70.1% (n = 761) of children were exposed to minimal maternal depressive symptoms and had good emotional–behavioral functioning (i.e., “competent outcomes”); 7.2% (n = 78) were exposed to minimal maternal depressive symptoms and had poor emotional–behavioral functioning; 6.1% (n = 66) were exposed to moderate to high maternal depressive symptoms and had poor emotional–behavioral functioning; and finally, 16.6% (n = 180) of children had been exposed to mothers with moderate to high maternal depressive symptoms and experienced good emotional–behavioral functioning (i.e. “resilient outcomes”). Of the 246 children exposed to moderate to high maternal depressive symptoms, 26.8% had poor emotional–behavioral functioning, and 73.2% had good emotional–behavioral functioning. Descriptive statistics for potential predictor variables by each status classification are shown in Table 5.
Descriptive Statistics for Potential Predictor Variables by Each Resilience Status Classification (n = 1085).

Table 6 presents the univariate and multivariable logistic regression models predicting the likelihood of emotional–behavioral resilience within the context of exposure to moderate to high maternal depressive symptoms (Model 1) and minimal maternal depressive symptoms (Model 2).
Bivariate and Multivariable Logistic Regression Models Predicting Children’s Positive Emotional–Behavioral Functioning in High- and Low-risk Exposure Environments (n = 1085).

Results in bold indicate significant odds ratios at p<.05. aAll participants completed this item regardless of partner status. bCell size too small.
Model 1: Moderate–High Maternal Depressive Symptoms – Modeling the Likelihood of Emotional–Behavioral Resilience
The univariate models (Table 6 – Model 1) revealed that the following maternal factors were significantly associated with children’s emotional–behavioral resilience: higher age at birth; being tertiary-educated; having a high income; perceived practical support from partner at six months postpartum; and high level of involvement in home activities at four years postpartum. The following variables were close to significance and were included in the multivariable model: high emotional satisfaction in the couple relationship at six months postpartum; being in a household headed by more than one adult; and mother not having experienced any relationship transitions by four years postpartum. In the multivariable model, higher maternal age, having a tertiary-educated mother, and high level of maternal involvement in home activities with the child were associated with emotional–behavioral resilience.
Model 2: Minimal Maternal Depressive Symptoms – Modeling the Likelihood of Competent Emotional–Behavioral Functioning
The univariate results (Table 6 – Model 2) revealed that the factors significantly associated with positive emotional–behavioral functioning were: being a female child; higher maternal age; having a tertiary-educated mother; having a high income; mother having time to self at least once a week at six months and four years postpartum; high emotional satisfaction in the couple relationship at six months and four years postpartum; and perceived partner contribution to caregiving at six months postpartum. Perceived practical support from partner at six months postpartum approached significance. In the multivariable model the factors that remained significant were being a female child, higher maternal age, mother having time to self at least once a week at six months and four years postpartum, and perception of high emotional satisfaction in the couple relationship at six months and four years postpartum.
Factors Uniquely Associated with Children’s Emotional–Behavioral Resilience in High-Risk Exposure Environments
Models 1 and 2 were compared to identify variables that were significant in high- but not low-risk exposure contexts. Two variables were uniquely associated with emotional–behavioral resilience for children exposed to moderate to high maternal depressive symptoms in the multivariable models: maternal education at a tertiary level and maternal involvement in activities with their child.
Discussion
We explored emotional–behavioral resilience among four-year-old children whose mothers reported maternal depressive symptoms during pregnancy and the early parenting period. We found that 21.6% of first-time mothers had a pattern of moderate to high depressive symptoms over time. This is slightly higher than previously reported estimates of maternal depression in the first and second postnatal years (Matthey et al., 2000; O’Hara and Swain, 1996), and the course of depression across six to seven years postpartum (Giallo et al., 2014). Of the 246 children whose mothers had this persistent pattern of symptoms, approximately three quarters (73.2%) were identified as emotionally and behaviorally resilient as evidenced by functioning in the normal range on the SDQ. Although maternal depression is a well-established risk factor for poor child health and wellbeing (Kingston & Tough, 2013; Kingston et al., 2012), the vast majority of children whose mothers were experiencing depressive symptoms in this study were functioning well.
Protective Factors for Children of Mothers Experiencing Depressive Symptoms
We also identified the perinatal and concurrent psychosocial factors uniquely associated with emotional–behavioral resilience among children whose mothers reported depressive symptoms (i.e., variables significant in the multivariable Model 1 but not in Model 2). We focused on characteristics in the early caregiving environment important to children’s wellbeing. The pattern of results was complex, but it was clear that maternal involvement in activities that included reading or talking with their child at four years was uniquely associated with emotional and behavioral resilience for these children. Although depressive symptoms can make it harder for parents to engage in and enjoy activities with their children (Giallo et al., 2013), our findings suggest that when mothers maintain a high level of engagement and interaction with their child, the child is more likely to experience better outcomes. Reading stories, playing together, and involving children in everyday routines can provide mothers and children with an opportunity to share positive times with one another, talk about their experiences, and strengthen connection and warmth in their relationships. It can also provide mothers with an opportunity to create a caregiving environment that is sensitive and responsive to their children’s needs. Although it is not possible to infer directionality, it is also plausible that children with emotional and behavioral difficulties are less likely to benefit from maternal involvement, or that mothers who experience depression may be more overwhelmed by their children’s problems and are less able to maintain high involvement. Notwithstanding issues pertaining to directionality, other research indicates that these experiences are important for all children’s emotional and behavioral development (Bradley et al., 2001), and our findings suggest they might be particularly important for children whose mothers are experiencing depression.
Two protective factors identified at the univariate level were maternal education and partner support. Low education is a well-established risk factor associated with poor outcomes for children (Bradley & Corwyn, 2002). Grounded in Conger’s Family Resource Model (Conger et al., 1992), we propose that compared to depressed mothers with limited education, more educated depressed mothers may have greater access to economic and social resources that enable them to provide an enriching caregiving environment for their child. Similarly, having a partner who provides a high level of practical support can be an important resource to women experiencing depression. A positive contribution to practical aspects of caring for children and running households may enable women to engage in responsive and sensitive interactions with their children, and be consistent in their interactions. Involved and supportive partners may also help to maintain family routines and provide extra support to children during periods of maternal depression. Partner support and involvement can also have direct effects on child wellbeing, which is in line with other studies reporting that fathers’ social support for their depressed partner is associated with positive outcomes for children (Letourneau, Duffett-Leger, & Salmani, 2009; Tannenbaum & Forehand, 1994).
Resource Factors Important for All Children
This study also identified resource factors associated with competent outcomes for all children regardless of whether they had been exposed to maternal depression or not (i.e., variables that were significant in both multivariate Models 1 and 2). Older maternal age and not experiencing significant financial hardship (as indicated by not having a Health Care Concession Card) were associated with positive emotional–behavioral outcomes for all children. It is likely that older mothers and those not experiencing significant financial hardship have greater economic and social resources to provide a supportive early caregiving environment. This is consistent with research indicating that children of young mothers have poorer outcomes, likely due to the educational, economic, and social disadvantages (i.e., limited opportunities to pursue education or employment) that younger mothers often experience (Harden, 2009).
Factors Unique to Children of Mothers Experiencing No or Minimal Depressive Symptoms
Several factors were unique to competent outcomes for children of mothers experiencing no or minimal depressive symptoms (i.e., variables significant in multivariate Model 2 but not in Model 1), including high emotional satisfaction in the couple relationship, having time to themself at least once per week at both six months and four years postpartum, and partner contribution to caregiving at six months postpartum. Whilst these factors are likely to have played an important role in promoting the mental health of women in this group, our findings also highlight their direct importance to children. Although relationship conflict was not assessed in this study, healthy couple relationships with low conflict are associated with positive emotional and behavioral functioning among children (Krishnakumar & Buehler, 2000).
Study Strengths, Limitations, and Future Research
This is one of the first prospective pregnancy cohort studies to examine the relationships between childhood emotional and behavioral resilience and exposure to maternal depression from a life course perspective spanning pregnancy and early childhood. This study builds on previous work primarily focused on poor outcomes for children, to provide a broader picture of children’s functioning that will help facilitate positive outcomes for children whose mothers are experiencing depressive symptoms. Strengths included the use of longitudinal analyses to identify different levels of maternal depression across the childhood period. This person-centered analytic approach enabled the identification of a group of resilient children who were functioning well within the context of adversity, and the factors uniquely associated with their outcomes. This is in contrast to a variable-centered approach which examines the interaction or moderating effects between variables, where a protective factor is identified if it reduces the effect of adversity on functioning (Miller-Lewis, Searle, Sawyer, Baghurt, & Hedley, 2013). Despite the different approaches available, evidence suggests that they yield similar findings. For instance, Miller-Lewis et al. (2013) identified the factors associated with positive mental health outcomes for preschool-aged children experiencing both low and high family adversity (poverty, parental separation, psychological distress, and stressful life events) using four approaches to conceptualize resilience and analyze data. All methodologies yielded similar results, and therefore strengthen confidence in the robustness of the approach we have taken in our study.
There are, however, several study limitations to note, along with key directions for future research. First, we assessed one domain of children’s functioning at a single time point during early childhood. Although we used the SDQ, a psychometrically sound and widely used measure of emotional–behavioral functioning, resilient outcomes can be evident in other domains, such as cognitive or academic functioning, and resilient status can also change across the lifespan (Luthar et al., 2000). Future research drawing upon life course approaches to examine trajectories of resilience in multiple domains will provide a more comprehensive profile of childhood resilience within the context of maternal depression.
Second, our investigation of protective and resource factors was limited to the variables available in the MHS, a study designed to investigate maternal health during pregnancy and postpartum. The measures were necessarily brief, and our capacity to examine issues such as the quality of couple relationships was constrained. Other resources and protective factors (e.g., child temperament; warm, sensitive, and responsive parenting behavior; father mental health; the provision of high quality childcare; and access to and adequacy of professional support for women with depressive symptoms) may play an important protective function, but were not a primary measurement focus in early waves of the MHS. Third, while we explored a broad range of contextual factors associated with resilient child outcomes, and provide confidence intervals for estimated associations to support the strength of the evidence, we acknowledge that multiple comparisons can increase the risk of chance findings. Future research may focus on a more comprehensive investigation of fewer factors that were identified as important predictors of resilience outcomes for children, such as economic resources and couple relationship functioning.
Fourth, data for this study were all based on maternal self-report, which may have introduced some self-report measurement bias. Finally, the majority of the sample were Australian-born, married, and tertiary educated, and selective attrition was observed whereby women completing the four-year follow-up were more likely to be older, Australian-born, tertiary educated, and less likely to have reported depressive symptoms in the first year following birth. Therefore, the sample was under-representative of women who were single parents and those from vulnerable backgrounds (i.e., non-English speaking, Aboriginal or Torres Strait Islander, low socio-economic background), limiting generalizability of the findings to these groups. It is also important to note that this study was of first-time mothers, and results may vary for mothers who have had a broader range of parenting experiences.
Conclusion
This study has important implications for policy and practice efforts focused on promoting outcomes for mothers, children, and families in the postnatal and early parenting period. Our findings highlight that despite growing up in high-risk contexts associated with maternal depression, many children do well, experiencing good emotional and behavioral functioning. We found that the home learning environment, practical support from a partner, and adequate economic resources are particularly important protective factors that may buffer children from the potential adverse effects of maternal depression. These findings suggest that targeted interventions focused on strengthening co-parenting relationships (Feinberg & Kan, 2008), parent–child interactions, and the early home learning and play environment (Barlow et al., 2010) are important for mothers experiencing depression. Information, resources, and support to strengthen the quality of day-to-day interactions, fostering play and communication between mothers, fathers, and children, are important targets for policy and prevention efforts to promote the health and wellbeing of children and their families in the early years and beyond.
Footnotes
Acknowledgments
We are grateful to the women who participated in the study; to members of the Maternal Health Study Collaborative Group who contributed to the study design; and to members of the Maternal Health Study research team who contributed to data collection and coding.
Funding
The work was supported by the National Health and Medical Research Council (NHMRC), VicHealth, and the Victorian Government’s Operational Infrastructure Support Program. RG and SB were supported by an NHMRC Career Development Fellowship and an NHMRC Research Fellowship, respectively.